
Abstract
Despite the growing recognition of mental health concerns within Asian American populations, significant barriers exist in accessing and receiving adequate mental health care. This study seeks to examine the current mental health needs of Asian/Asian American (AAA) Christians to promote future efforts in addressing the mental health treatment gap. Participants (N = 98) who identified as AAA Christians living in Los Angeles and Orange Counties were recruited using purposive and snowball sampling. The needs assessment battery administered consisted of quantitative and qualitative questions that examined mental health needs, types of mental health service needed, and factors that impact mental health service seeking. Using a mixed-methods program evaluation approach with the Pillar Integration Process, this study found there continues to exist unmet mental health needs, with respondents indicating factors such as finances, lack of information, and time constraints as barriers toward seeking help. Participants indicated a preference toward receiving mental health care through individual therapy and psychoeducation workshops. Recommendations and implications for responding to the unmet mental health needs in AAA Christian communities are discussed.
Among all racial and ethnic groups, Asian Americans are the least likely to seek mental health care (Alegria et al., 2008; CBHSQ [Center for Behavioral Health Statistics and Quality], 2021; Derr, 2016). The low utilization rate is evident even when Asian Americans endorse mental health needs (Balaraman et al., 2023; J. J. Kim et al., 2018; McGarity-Palmer et al., 2023; Shih et al., 2023), have serious psychological distress and experience a major depressive episode (Yang et al., 2020). In fact, between 2015 and 2019, only one out of five Asian adults with a mental illness received mental health care (CBHSQ, 2021). The American Psychiatric Association (APA, 2020) points to structural and cultural barriers in explaining mental health disparity. Structural barriers include cost, language barriers, and lack of cultural competency from providers, and cultural barriers include stigma and shame associated with seeking mental health care and the model minority myth (APA, 2020; Cheng et al., 2017; D. K. Eng & TenElshof, 2020; S. Lee et al., 2008). In addition, Asians are more likely to endorse not knowing where to go for mental health treatment compared with non-Hispanic Whites (Wang et al., 2019; Yang et al., 2020). These problems point to the need for culturally specific outreach and mental health services tailored to Asian American communities.
At the same time, the Pew Research Center (2023) reports that Christianity is the largest (34%) faith group among Asian Americans. Furthermore, a previous survey by the Pew Research Center (2013) found that Asian American Christians have a higher level of religious commitments compared with the general U.S. Christian adults. Specifically, among Evangelical Protestants, Asian Americans are more likely to attend weekly religious service (76%) than their White counterparts (64%). In addition, 72% of U.S. Asian evangelicals endorse that their religion is the one true faith that leads to eternal life, compared with 49% of U.S. White evangelicals (with 42% endorsing that other religions can also lead to eternal life). Finally, more Asian Americans (37%) state that living a very religious life is one of their most important goals compared with the general U.S. adults (24%). In light of the importance of religiosity among Asian Christians, church is often a significant source of support. In addition, individuals who endorse higher religiosity and spirituality tend to seek mental health care from religious leaders (Boateng et al., 2024) and appear to benefit from mental health treatments that incorporate religious and spiritual adaptations (Smith et al., 2007). The purpose of this mixed-method study is to assess mental health needs among Asian American Christians, the types of services that would meet the needs in this community, and factors that are related to mental health help-seeking.
Background
Mental health care utilization
Mental health care utilization is a complex and multidimensional process (Andersen & Davidson, 2007; Radhamony et al., 2024). Andersen and Davidson (2007) present a theoretical model of health service use, which has been applied to mental health service utilization (Radhamony et al., 2024), and highlight the need to examine both contextual and individual factors. The extant literature has documented a number of contextual factors that contribute to mental health disparities among Asian Americans. Among others, contextual factors include limited availability of professionals who are able to provide culturally congruent care (M. Lee et al., 2021; Nagayama Hall & Yee, 2012; Sorkin & Ngo-Metzger, 2014; Wang et al., 2019). On a broader, more systemic level, service providers and institutions that train providers tend to conceptualize mental health and idioms of distress in Eurocentric terms, marginalizing communities of color, including Asian Americans (Maru et al., 2024). These are just a few of the contextual factors that underscore the fact that mental health care utilization is a social process and must be understood within relational and sociopolitical contexts, in addition to examining individual factors (Radhamony et al., 2024).
The role of Christian communities
Notwithstanding the aforementioned barriers to help-seeking, religious spaces have historically been a place for meeting the health needs of communities of color (Whitt-Glover et al., 2014), including counseling resources for its congregants (Campbell & Winchester, 2020; Min, 1992). This is true for Korean Americans (I. J. Kim et al., 2006), with some preferring to receive their health information from church as opposed to resources in the community, including hospitals (Bastani et al., 2007; Jo et al., 2008; K. Kim et al., 1999). A broader review of the literature indicates that there has been research pointing toward bridging mental health service utilization disparities within religious organizations (Campbell & Winchester, 2020; Hays, 2015; McLaughlin et al., 2022). Because mental health care utilization is a social process (Radhamony et al., 2024), referrals and education from within the church may help destigmatize some barriers and encourage seeking support for mental health care needs for Asian American congregants (D. K. Eng & TenElshof, 2020).
While studies have examined factors associated with mental health disparity among religious individuals (Abu-Ras et al., 2008; McLaughlin et al., 2022), Christians (Campbell & Winchester, 2020; Lefover et al., 2021), and Asian Americans (e.g., Balaraman et al., 2023; McGarity-Palmer et al., 2023; Yang et al., 2020), few have examined how faith-based communities may improve mental health care utilization among Asian Americans. For example, a systematic review (S. B. Kim & Lee, 2022) of 34 studies on mental health help-seeking among Asian Americans reveals that only two studies included measures of religiosity and spirituality (R/S). In light of the high level of religiosity endorsed among Asian Americans (Pew Research Center, 2023), more studies are needed to examine factors associated with help-seeking at the intersection of spiritual/religious and racial social identities. The results from these types of studies will inform how mental health professionals can work more effectively with clergy to improve mental health well-being in their respective communities. To the authors’ knowledge, no study has examined the mental health needs of Asian American Christians in particular.
Present study
This study seeks to investigate current mental health needs and perspectives of Asian American Christians, in efforts to further understand factors associated with mental health service utilization. A mixed-method program evaluation approach was used to increase the emphasis on the local impact of results (Fitzpatrick et al., 2023). Specifically, a needs assessment framework was used to establish whether a problem or need exists, to describe the nature of the problem, and to make recommendations for ways to reduce the problem (Royse & Badger, 2015). The following questions were used to guide the needs assessment: Among Asian American Christians, (1) What are the felt mental health needs? (2) What are the types of preferred supports or services? And, (3) what are the barriers and facilitators to seeking mental health support or services? Identifying these factors will further the understanding of the current needs and promote future efforts to bridge the gap between mental health service utilization for Asian American Christians.
Method
Research design overview
The study adopted a mixed-methods program evaluation approach to answer the aforementioned needs assessment questions. Moseholm and Fetters (2017) describe integration in mixed-methods research at the (1) philosophical, (2) design, (3) methods, and (4) interpretation and reporting levels. See the Supplemental Materials for further elaboration on this approach.
Participants
Study protocols were approved by the institutional review board (IRB) according to ethical principles as described in the Belmont Report. Participants were recruited through purposive and snowball sampling, with outreach focused on churches in Los Angeles County and Orange County among Asian American Christians. Flyers and emails were disseminated widely, such as through contacts and leaders in organizations and churches focusing on Asian/Asian American Christians. Flyers were also posted on social media and listserv. Participants were eligible for the survey if they self-identified as (1) Asian/Asian-American, (2) identified as Christians, (3) lived in LA or Orange County, and (4) were older than 18. A screening survey was included as part of the survey protocol to screen only for participants who met these demographics and to limit the possibility of fraudulent bot responses. A total of 111 unique responses were collected. Eight responses were removed from the analysis due to the completion of less than half of the survey, reducing the number of participants to 103. Literature suggests using multiple criteria along with validity questions/attention checks to remove data while not eliminating complete responses on the basis of one validity question (Berinsky et al., 2013; Muszyński, 2023; Ward & Meade, 2023). As this study contains qualitative components as well as four validity/attention check questions, the determined threshold of elimination of data was set to participant responses that missed more than one validity question (n = 5). The final sample of participants included in the quantitative and qualitative data analysis was 98 respondents. Table 1 provides further demographic information based on gender, immigrant generation, ethnicity, education level, marital status, household income, employment status, and language proficiency.
Participant Demographics.
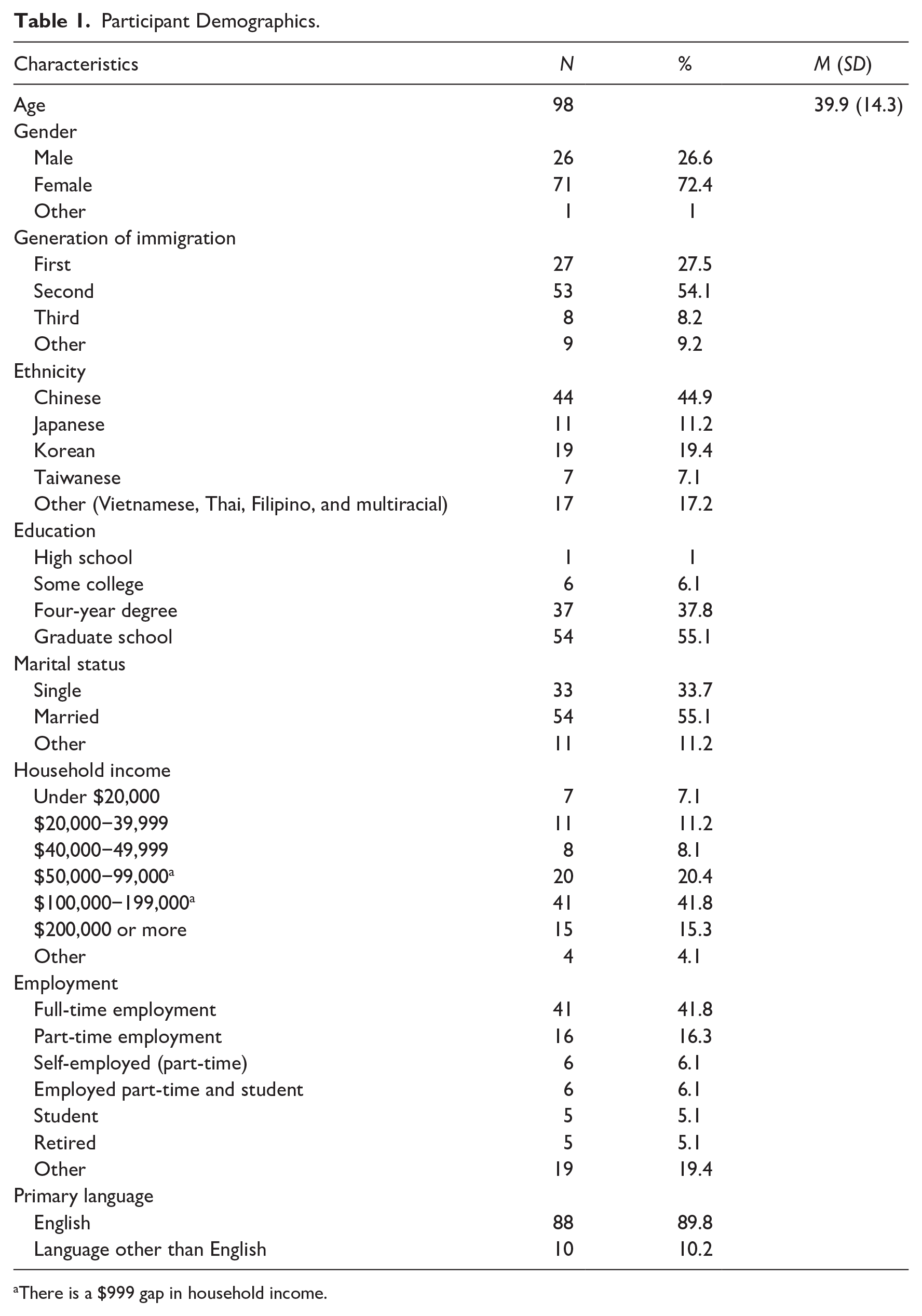
There is a $999 gap in household income.
Data collection measures
Close-ended self-report questions were utilized to provide quantitative data, while open-ended self-report questions were utilized to provide qualitative data. A matching approach was used to align the domains covered by the qualitative interview questions and quantitative instruments (Moseholm & Fetters, 2017). Supplemental Table 1 depicts how the aforementioned questions matched with the following three domains: (1) level of felt mental health needs, (2) desired types of services and supports, and (3) factors that could increase the likelihood of seeking mental health care. Including demographic information, the quantitative portion of the assessment included items from the Depression, Anxiety, and Stress Scale−21 (DASS-21; Lovibond & Lovibond, 1995) and a series of forced option questions adapted from Jang et al. (2019). In addition, participants responded to items pertaining to the likelihood of seeking out various mental health services (e.g., individual therapy, family therapy), factors that may impede (e.g., finances) or facilitate mental health help-seeking (e.g., desire to improve spiritual health), preferences for mental health providers’ characteristics (e.g., same gender), and attitudes regarding various referral sources (e.g., referral from clergy). Finally, five short answer questions adapted from the Cultural Formation Interview (CFI; APA, 2022) were included to assess stressors that might worsen their mental health, supports that may improve their mental health, facilitators and barriers to seeking mental health services, and aspects of identity that may impact mental health care seeking. The Supplemental Materials provide further psychometric information for the DASS-21, binary questions from Jang et al. (2019), and open-ended questions from the CFI (APA, 2022).
Data analytic plan
Quantitative data analysis
Data were analyzed using R Studio (R Core Team, 2024). Data were cleaned by removing duplicate responses, possible bots, and those who did not pass two or more of the four validity questions. For the survey items that provided quantitative results, missing data patterns were as follows: three participants had 1.59% missing items, and two participants had 11.11% missing items. For analysis of Domain 1, to assess mental health needs, DASS-21 scores were compared according to interpretive thresholds recommended in the DASS-21 manual (Lovibond & Lovibond, 1995) and thresholds described by Ronk and colleagues (2013) in a study with an outpatient and inpatient sample. In addition, percentages for a one-item question adapted from Jang et al. (2019) regarding mental health needs will be reported. For analysis of Domain 2, to assess participants’ mental health service needs, descriptive statistics are reported for participants’ responses to questions regarding services they might utilize. For analysis of Domain 3, to examine predictors of mental health service utilization, descriptive statistics were reported on participants’ responses to questions regarding factors that may impact service utilization.
Qualitative data analysis
The qualitative data were analyzed using a Consensual Qualitative Research−Modified (CQR-M) method. CQR-M utilizes a bottom-up approach where researchers collaboratively discuss data to discover domains and subcategories and code the data accordingly to each category (Spangler et al., 2012). This discovery-oriented and exploratory approach makes CQR-M particularly useful for investigating novel and unprecedented topics through simple data (Spangler et al., 2012). The four-person coding team conducted four 90-minute meetings to discuss domains and subcategories based on the open-ended data.
Researcher bias
CQR-M requires the researchers to reflect on their personal biases related to the research topic and facilitates collaborative discussions among the researchers to reach an objective and highly agreed-upon consensus (Spangler et al., 2012). The qualitative research group consisted of four female doctoral-level students in a clinical psychology program in a Christian institution located in Southern California. The researchers came from diverse cultural backgrounds, including third to fourth generation to first-generation immigrants, and various standings in the program. When reflecting on the cultural, personal, and clinical experience relevant to the research topic, common themes that emerged included generational differences in the perception of mental health, how mental health is perceived in religious contexts, and the generalization of Asian culture by the mainstream media.
Coding of domains
Following the guidelines from Spangler et al. (2012), the qualitative data coding team first retrieved domains from the data independently and then finalized the list of nine domains through collaborative discussion. The team discussed whether the wording of the domains sufficiently captured the content of the data and addressed the questions it pertained to. When inconsistencies in labeling arose, the team reviewed their reasoning for naming the domains and subcategories until they reached a consensus. In addition, the team selected a quote(s) from the data for each domain that accurately represents its content. After consolidating the domains, the team individually calculated the frequencies for each domain and then divided into groups to compare the results across domains. For domains with inconsistent numbers, the groups reviewed the domain together to reach an agreement on the final count. After the final count was reached, the draft of domains was reviewed by the two faculty members (second and fourth authors), who provided oversight over the research study. Specifically, these faculty members provided feedback on parsimony and readability of the domains. First, the second author suggested consolidating Domains 1 through 6 into a single domain (Factors Impacting Mental Health-Seeking) and reclassifying them as categories due to their relevance and to make it coherent with the other two domains. After discussing these recommendations, the team agreed that the change would enhance readability and decided to incorporate the suggestion. The modified draft was again reviewed by the second and fourth authors, who suggested collapsing two subcategories (professional support, support from mental health professionals). The team collaboratively decided that the two subcategories were similar enough to be combined and incorporated the suggestion. See Supplemental Table 2 for the finalized results that emerged from the CQR-M analysis.
Mixed-methods analysis
The Pillar Integration Process (Johnson et al., 2019), a mixed-methods approach that incorporates an integration of quantitative and qualitative data into a joint visual display, was utilized. This approach was utilized due to its rigorous, transparent approach to integrating quantitative and qualitative data and conveying simultaneously through a visual representation of the data. First, initial quantitative (i.e., descriptive statistics) and qualitative analyses (CQR-M) were conducted separately. Then, the Pillar Integration Process (Johnson et al., 2019) was completed sequentially in four stages: (1) listing, (2) matching, (3) checking, and (4) pillar building. Each stage of the integration process is described in the Supplemental Materials.
Results
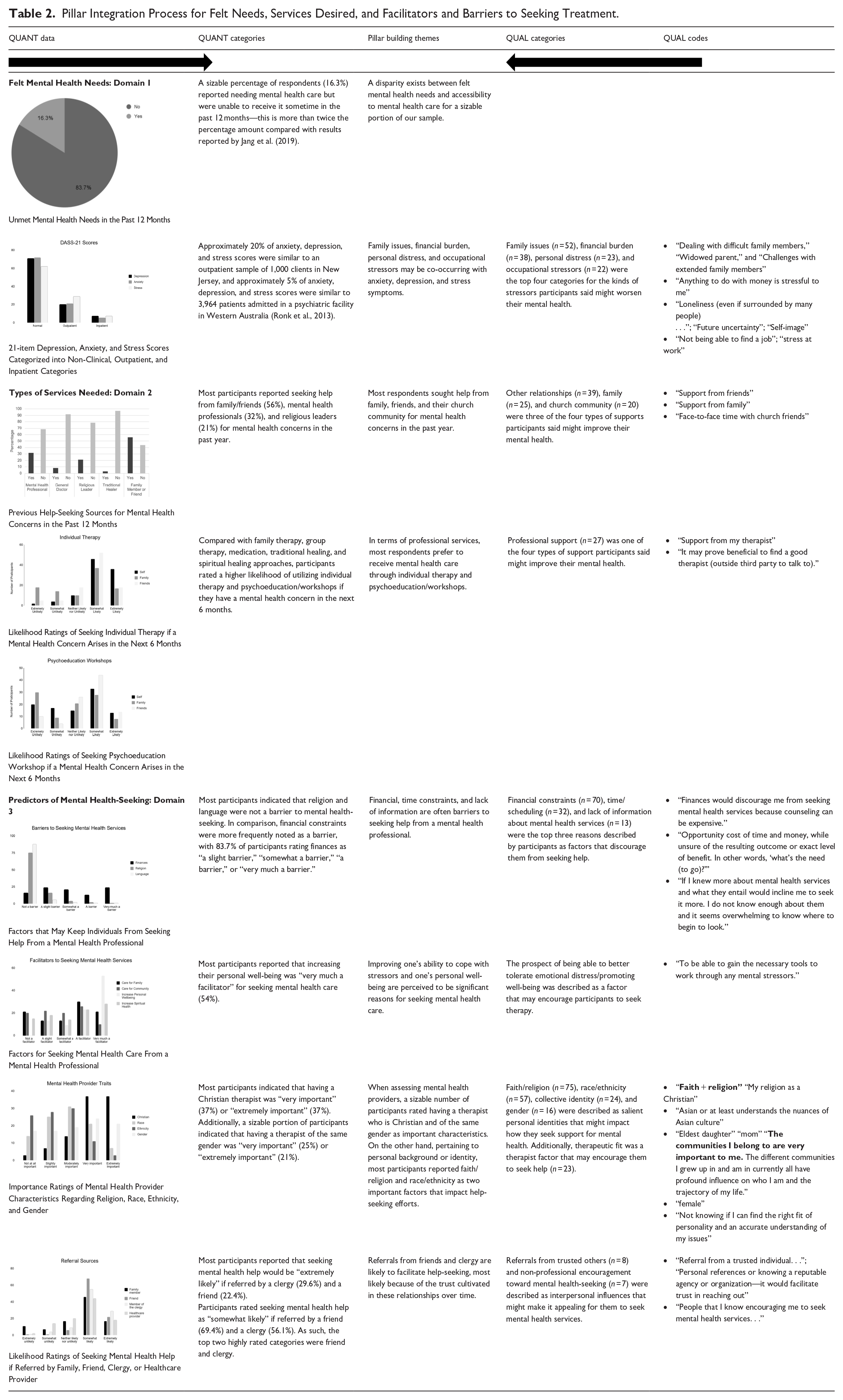
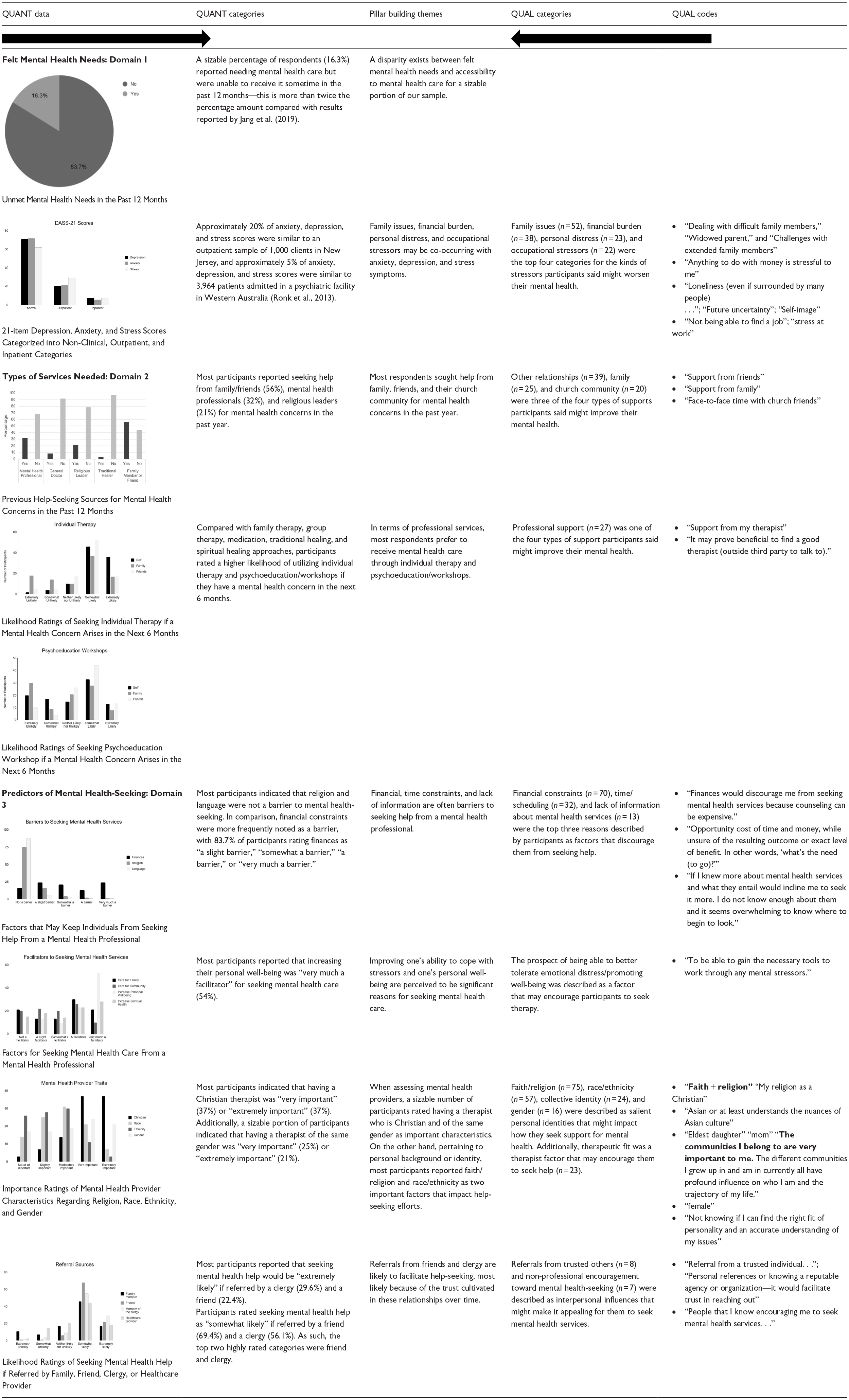
The following themes, organized according to our three broad research questions, emerged from the pillar integration process (see Table 2):
Domain 1: What is the level of felt mental health needs? A disparity exists between felt mental health needs and accessibility to mental health care for a sizable portion of our sample. Family issues, financial burden, personal distress, and occupational stressors may be co-occurring with anxiety, depression, and stress symptoms.
Domain 2: What are the desired types of services and supports? Most respondents sought help from family, friends, and their church community for mental health concerns in the past year. In terms of professional services, most respondents prefer to receive mental health care through individual therapy and psychoeducation/workshops.
Domain 3: What factors could increase the likelihood of seeking mental health treatment? Financial, time constraints, and lack of information are often barriers to seeking help from a mental health professional. Improving one’s ability to cope with stressors and one’s personal well-being are perceived to be significant reasons for seeking mental health care. When assessing mental health providers, a sizable number of participants rated having a therapist who is Christian and of the same gender as important characteristics. On the other hand, pertaining to personal background or identity, most participants reported faith/religion and race/ethnicity as two important factors that impact help-seeking efforts. Referrals from clergy members and friends are likely to facilitate help-seeking, most likely because of the trust cultivated in these relationships over time.
Pillar Integration Process for Felt Needs, Services Desired, and Facilitators and Barriers to Seeking Treatment.
Discussion
This study provides a snapshot of the current mental health needs of Asian American Christians in Los Angeles County and Orange County. Specifically, the study analyzed findings in three domains: (1) felt mental health needs, (2) desired types of support and services, and (3) facilitators or barriers to seeking formal mental health assistance. The mixed-methods program evaluation approach provided complementary insights from qualitative and quantitative strands of data to contribute to extant literature and guide the design of the Asian American Specialty Clinic. Findings are discussed according to the three domains, including clinical implications and suggestions for future research.
Felt mental health needs: Domain 1
Approximately 16% of the participants in this study reported an unmet mental health need, which is more than twice as much as was reported in Jang et al.’s (2019) study, where 7% of the participants in the study indicated an unmet mental health need. This finding suggests that there are barriers that continue to prevent individuals from accessing mental health care, which is a similar conclusion reported in other studies on mental health service utilization for Asian Americans (Balaraman et al., 2023; McGarity-Palmer et al., 2023; Shih et al., 2023). In addition, family issues, financial burden, personal distress, and occupational stressors may be co-occurring with anxiety, depression, and stress symptoms. Mental health providers who desire to work effectively with Christian Asian American clergy and congregants could consider how these needs are defined and articulated in their community outreach and clinical-related activities.
Types of services needed: Domain 2
In examining where individuals had sought support for mental health concerns in the past year, more than half of the participants had sought help from a friend or family member regarding a mental health concern. This majority preference is consistent with studies that found that Asian Americans tend to seek informal support from friends, relatives, religious communities, or significant others rather than mental health professionals (S. Lee et al., 2008; Leung et al., 2012). However, contrary to results reported in other studies (S. Lee et al., 2008; Leung et al., 2012; Spencer & Chen, 2004), mental health professionals were sought out more frequently than clergy, as around 31% of the participants in our sample had sought support from a mental health professional in the past year, and 21.4% had sought support from a member of the clergy in the past year for mental health concerns. This discrepancy could be attributed to immigrant generational differences. In a recent systematic review, S. B. Kim and Lee (2022) outlined a conceptual model that describes how predisposing factors (e.g., lack of familiarity with mainstream American culture) could contribute to structural barriers (e.g., experiences of discrimination) to mental health help-seeking behaviors. Similarly, Spencer and Chen (2004) reported that Chinese Americans who have experienced language-based discrimination (e.g., recent immigrants being treated poorly because of language or accent) tend to utilize informal services for mental health assistance rather than formal services. Indeed, M. Lee et al. (2020) reported that English proficiency is related to higher receptiveness to formal mental health services. Because our sample was predominantly English speaking (89.8% with English as primary language), the results of our study may be more relevant to Asian American individuals who may be second generation or above in terms of immigrant generation.
Predictors of mental health-seeking: Domain 3
Pertaining to barriers, financial constraints were identified as a top barrier (in both quantitative and qualitative strands) to seeking mental health care in our study. Cost and affordability have consistently been recognized as significant barriers within Asian American communities (S. B. Kim & Lee, 2022; Shih et al., 2023; Yang et al., 2020). To address this barrier, researchers have highlighted the importance of structural changes in mental health access, such as increased government funding for Asian American mental health and the restructuring of insurance coverage to expand access to mental health services (Obra et al., 2021; Yang et al., 2020). Furthermore, countries such as the U.S. have been implementing a task-sharing approach of collaborating with a wide range of community-based resources such as Mental Health First Aid (MHFA) to improve accessibility of mental health treatment to underserved populations (Mongelli et al., 2020). Additional solutions include students seeking specific support, such as utilizing institutional resources from universities and implementing prevention programs, which have proven to be more cost-effective than actual treatment (Gee et al., 2020; Obra et al., 2021).
Readers may notice that more than half of our participants earned over $100,000, which may raise questions regarding financial barriers. Our study was conducted in the Los Angeles Metro Area, which has one of the highest living costs in the United States. For example, in Los Angeles County in 2024−2025, $110,950 is considered low income for a household of four (Los Angeles Almanac, n.d.). One of the limitations in our study is that we did not combine income information with household size to examine the question of financial barrier vis-à-vis income. Even among those who can afford therapy, there may be a barrier in valuing psychotherapy as a service to pay for when considering other competing demands, especially in light of the structural barriers identified above. Future studies may explore these variables in addition to the extent to which model minority myth-related beliefs may contribute to undervaluing psychological well-being when making financial decisions (D. L. Eng & Han, 2018). In addition, the potential benefit of a trauma-informed approach to financial decision making among Asian American Christians may be useful to explore as well (Ross & Coambs, 2018). A recent needs assessment conducted with Asian Americans (AA) and Native Hawaiians and Pacific Islanders (NHPI) in Orange County highlighted the socioeconomic diversity present in this population (Vo & Hom, 2018), which is a crucial consideration when considering financial barriers faced by various ethnic groups represented in the Asian American population.
In addition, lack of information about mental health was one of the top three barriers to seeking mental health services. One participant, for example, noted, “If I knew more about mental health services and what they entail would incline me to seek it more. I do not know enough about them and it seems overwhelming to know where to begin to look.” Knowledge of conditions (Cheon et al., 2016; H. J. Kim et al., 2019) and options to mental health care (Kung, 2004) are frequently cited factors in various help-seeking studies. Compared with other reasons for seeking formal mental health support (e.g., increased ability to care for family members, to improve spiritual health), our sample reported that improving personal well-being was the most compelling reason for seeking help from a mental health professional. Nagayama Hall et al. (2019) emphasized the cultural relevance of receiving immediate, tangible benefits in psychotherapy when working with Asian American clients.
Pertaining to mental health provider characteristics, the integrated mixed-methods results demonstrated that faith/religion was a significant factor that affected their help-seeking behaviors. As our study indicated, Christian Asian American clients prefer to have therapists who are Christian and may feel that they will be better understood by a provider who shares their religious beliefs (Boateng et al., 2024). Similar to having a therapist of the same faith, Asian American Christians appear to prefer a therapist of the same gender because of a perceived mutual understanding of experiences and a sense of safety and comfort. On the other hand, pertaining to themselves (i.e., not the therapist), respondents cited race/ethnicity as the second most important social identity that affects how they seek support for their mental health. It is possible that one’s social identity affects other factors that influence help-seeking behaviors (Arnault, 2009), but the Asian American preference for matching for gender over and above race/ethnicity appears to be consistent with extant literature. Compared with Black/African participants, for example, Asian/Asian American participants had higher gender matching preferences over and above racial matching preferences (Ilagan & Heatherington, 2021). Collectively, these findings suggest the importance of paying attention to gender dynamics in therapy (ChenFeng et al., 2017), especially if dealing with sensitive issues such as sexuality, sexual trauma, and/or sexual conditions.
Clinical implications and suggestions for future research
Based on the mixed-method findings from the pillar integration analysis and the review of literature above, the following recommendations are suggested for clinical service provision among Asian American Christians. Providers may benefit from reviewing cross-cultural best practices and Asian American culture-specific guidelines (Benuto et al., 2014) when collaboratively deciding on personalized treatment targets with their clients, such as anxiety, depression, or other change goals derived from the client’s values. Participants indicate that individual therapy and psychoeducation/workshops are preferable over other services (e.g., family therapy, group therapy). The provision of psychoeducation/workshops could be seen as a less stigmatizing way to engage with resources and may further provide Asian Americans with increased mental health literacy, training, and knowledge of mental health conditions. Given that cost was consistently reported as a significant barrier, providers may benefit from exploring alternative funding mechanisms such as federal, state grants, or donors. In addition, clinic administrators could collaborate with church communities or parachurch organizations to generate funds to offset the cost of seeing a mental health professional, such as subsidies for seeking mental health services for clergy (Koh, 2023). Given that our results indicated a strong preference for a Christian therapist, church (compared with same race, ethnicity, or gender), church and Christian mental health service partnerships may increase access to care within the Christian faith community while destigmatizing mental health-seeking (D. K. Eng & TenElshof, 2020). In addition, clinicians should consider gender dynamics when working with Asian American clergy and congregants (ChenFeng et al., 2017), as this appears to be the second most important factor when it comes to choosing a mental health provider among our respondents.
Future research could implement community-engaged research (Dubois et al., 2011) or empowerment program evaluation (Fitzpatrick et al., 2023) to give voice to and understand the explanatory models of mental health among Christian Asian American communities. A variety of engagement levels is possible, ranging from recruiting community members in surveys, interviews, and focus groups, assembling community advisory boards where advisors meet regularly with the clinic administrators or researchers, or hiring community members as part of the research/program evaluation team. Cultivating trust in these relationships over time may be key to increasing the relevance and appeal of services to Christian Asian American congregants. Specifically, sustained, meaningful partnerships based on mutual attunement and influence (ChenFeng et al., 2017) have the potential to shed light on how local theologies, embodied integration, as well as generational and cultural wisdom (Dwiwardani & Whitney, 2024) embedded in Christian Asian American communities influence the perceptions and adoption of mental health services. Future types of community-engaged research should consider how various social identities (such as age, gender, education, disability, national origin) may covary with the abovementioned factors, especially when dealing with diverse Christian Asian American groups.
Limitations
Some limitations of this study include the small sample size, which limits the generalizability of this study. As the category of Asian/Asian Americans encompasses many different countries with different cultures, the limited sample size also does not allow for disaggregation of the many different ethnicities that make up the population of Asian Americans in Los Angeles and Orange Counties. There is a need to understand the nuances and cultural differences of different Asian backgrounds, and the blanket term “Asian American” does not adequately capture the nuances (Okazaki et al., 2022; Shivaram, 2021). Additional studies with greater sample sizes and ethnicities would provide greater insight into the diverse perspectives toward mental health in different Asian cultures. In addition, the survey battery was only available in English, and all the participants of this study self-reported their fluency in English as “well” or “very well.” The results of this needs assessment also found that language was not generally reported as a barrier to seeking mental health care, with a total of 4.1% of the participants indicating that language is “somewhat a barrier,” “a barrier,” or “very much a barrier.” Thus, due to sampling bias, the results of this study may not generalize to Asian/Asian Americans whose primary language is not English.
Another consideration to take into account is the negatively skewed distribution of attitudes toward mental health-seeking, with greater than 93% indicating positive attitudes toward seeking mental health care. In other words, the results of this study may not capture the thoughts and perspectives of those who view mental health-seeking with higher amounts of stigma. Notwithstanding the favorable attitudes endorsed by our participants, nonetheless, results of our needs assessment still point to the presence of other barriers and facilitators to seeking care, such as financial constraints and fit with the therapist’s religiosity and/or spiritual beliefs.
Conclusion
The findings of this needs assessment are consistent with literature indicating that there continues to be a mental health treatment gap for Asian Americans, and services are not being accessed at the same rate as the mental health needs (Balaraman et al., 2023; Jang et al., 2019). Family issues, financial burden, personal distress, and occupational stressors may be co-occurring with anxiety, depression, and stress symptoms. Most respondents sought help from family, friends, and their church community for mental health concerns in the past year. To that end, referrals from clergy members and friends appeared to weigh heavily on decisions on mental health help-seeking. In terms of mental health services, however, most respondents indicated a preference to receive mental health care through individual therapy and psychoeducation/workshops. In addition, most participants rated having a therapist who is Christian and of the same gender as important mental health provider characteristics, while personal identification of race/ethnicity may be an important background or identity that impacts other aspects of help-seeking efforts.
Many of the above conclusions are consistent with findings reported from other studies and systematic reviews. To the authors’ knowledge, however, our study may be the first to systematically report integration at various levels (i.e., philosophical, design, methods, and interpretation and reporting levels) and use a transparent and rigorous four-stage technique (Johnson et al., 2019) for integrating and presenting findings in a joint display. The program evaluation approach also placed emphasis on having local impact in terms of utility, accuracy, and feasibility of findings (Fitzpatrick et al., 2023)—over and above its contribution to the literature on mental health help-seeking among Asian American Christians. It is hoped that this study could be a concrete demonstration of how other researchers, program evaluators, and/or clinic administrators could explore diverse methods of research or program evaluation methods to exert local impact and contribute to the broader conversation on Asian American mental health.
Supplemental Material
sj-docx-1-ptj-10.1177_00916471251343396 – Supplemental material for Mixed-Methods Needs Assessment of Mental Health Among Asian American Christians: A Pilot Study
Supplemental material, sj-docx-1-ptj-10.1177_00916471251343396 for Mixed-Methods Needs Assessment of Mental Health Among Asian American Christians: A Pilot Study by Priscilla Kwong, Carissa Dwiwardani, Grace Y. Kim, Eu Gene Chin, Nicole Chang and Lydia Cho in Journal of Psychology and Theology
Footnotes
Authors’ Note
The authors would like to express their gratitude to Biola University’s Office of the Provost and Office of Innovation for the Innovation Grant and Research and Development (R&D) Grant, as well as private donors who made this work possible. The opinions expressed in this publication are those of the authors and do not necessarily reflect the views of Biola University or the donors who supported this work. A large portion of this paper was based on the first author’s master’s thesis. In addition, a portion of the introduction section has appeared on previous grant proposals for this and projects on Asian American mental health. The authors would also like to thank Sydni Wong for her contributions to the qualitative analysis process.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by Biola University’s Office of Innovation (through the Innovation Grant), Provost’s Office (through the Research and Development Grant), and Office of University Advancement (through Private Donor Grants).
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.