
Abstract
Recent research has shown Mainline Protestant clergy evidence poor mental health. In accounting for this, research has focused on occupational factors that impact health, with less attention paid to the role of selection into ministry as it relates to health. We investigate one possible selection characteristic, adverse childhood experiences (ACEs), among a sample of 535 seminarians attending a Mainline seminary. Compared with a demographically matched national sample, these seminarians reported higher prevalence of the childhood experiences of emotional abuse, of living with someone with mental illness, and of sexual abuse. These seminarians also reported lower prevalence of parental separation/divorce and of familial incarceration. Furthermore, we found demographic variations in the prevalence of certain ACEs among the sample of seminarians. In addition to informing the scholarly discussion regarding mechanisms associated with clergy well-being, this work highlights the need for seminaries to attend to the ministerial formation of students with these experiences.
Introduction
The mental health and well-being of the clergy has been of interest to scholars of religion, religious organizations, and occupations for many years (Carroll, 2006; Ellison et al., 2010; Fichter, 1987; Holleman, 2023; Holleman & Eagle, 2023; Meisenhelder & Chandler, 2001; Miles et al., 2011; Rossetti, 2011; Wells, 2013). Mainline Protestant clergy, in particular, evidence higher rates of elevated anxiety and depressive symptoms compared with the general population (Edwards et al., 2020; Holleman & Eagle, 2023; Proeschold-Bell & Byassee, 2018). Similar patterns may exist among the Roman Catholic clergy (Edwards et al., 2020; Knox et al., 2005). Past studies have proposed that these patterns exist because of the unique occupational conditions of the pastorate. The clergy profession is typically portrayed as inherently difficult and stressful, involving long hours, role overload, and lack of social support (Bloom, 2019; Knox et al., 2005; Lee, 1999; Miner, 2007; Rowatt, 2001; Virginia, 1998). These factors, coupled with the aging clergy population and the loss of occupational prestige (Chaves, 2017), are thought to place the clergy at an elevated risk for developing poor mental health.
Altogether, past research has focused on the factors that affect pastors’ mental health after they enter the profession. However, no prior study has focused on understanding how the patterns of selection into the pastorate may correlate with mental health and well-being. It is possible that early life adversity, which has been shown to place people at a higher risk for developing symptoms of poor mental health later in life (Felitti et al., 1998), may be a catalyst for entering into ministry. The focus of this study is to understand one potential factor in the selection process into a career in ministry: adverse childhood experiences (ACEs). ACEs are traumatic events experienced prior to age 18 years, including both household dysfunction and direct experiences of abuse (Felitti et al., 1998). ACEs are typically divided into eight specific domains. Household dysfunction is divided into five categories: household mental illness, household substance abuse, parental separation or divorce, incarceration of a family member, and witnessing interpersonal violence. Direct experiences of abuse are divided into three categories: emotional abuse, physical abuse, and sexual abuse.
Past research has found a strong association between ACEs and adulthood experiences of depressive symptoms, anxiety symptoms, suicidality, alcoholism, substance use disorder, and low life satisfaction (Brodsky & Stanley, 2008; Chapman et al., 2004; Danese et al., 2009; Dasgupta et al., 2018; Dube et al., 2001; Felitti et al., 1998; Hughes et al., 2017; Merrick et al., 2017; Pilowsky et al., 2009; Sareen et al., 2013). Furthermore, individuals with ACEs may be more vulnerable to further experiences of trauma during adulthood, both through direct experiences and through vicarious and secondary trauma (Figley, 1995; Pearlman, 1999; Slattery & Goodman, 2009).
A significant body of research has examined the relationship between ACEs and career choice in adulthood. This work suggests that those entering helping professions, such as therapists, counselors, social workers, and police officers, experienced more ACEs than other professions (Black et al., 1993; Branson et al., 2019; Bryce et al., 2023; Elliott & Guy, 1993; Follette et al., 1994; Pope & Feldman-Summers, 1992; Racusin et al., 1981; Rompf & Royse, 1994). As the clergy frequently serve in roles analogous to helping professions, including as ad hoc mental health counselors, crisis responders, and spiritual directors (Carroll, 2006; Chatters et al., 2011; Kuhne & Donaldson, 1995; Lee, 1999; Morris & Blanton, 1994; Pickard & Guo, 2008), the process of selection into the clergy profession as it relates to ACEs may be similar to that of other helping professions.
In addition to the occupational similarities between the clergy and other helping professions, the life course perspective offers a useful frame as to why the clergy may demonstrate a greater prevalence of ACEs. The life course perspective emphasizes that the events, transitions, and turning points that comprise life trajectories—including religious life—may be shaped by childhood experiences (Ben-Shlomo & Kuh, 2002; Manglos, 2013). Some research suggests that early life adversity is associated with greater spiritual openness and spiritual growth (Harris et al., 2015; Reinert & Smith, 1997; Santoro et al., 2016; Schafer, 2014). Furthermore, religion may be a source of comfort in crisis and can help people derive meaning from adversity, including childhood emotional and physical abuse (Park, 2005; Upenieks, 2021; Walker et al., 2009). Individuals seeking comfort through their faith may be more likely to interpret the events of their lives as part of a greater divine plan, of which the call to ministry may be a part.
Despite this, there have been very few scholarly investigations of experiences of childhood trauma among pastoral leaders. The studies that do exist have relied on small convenience samples, ranging in size from 84 to 182 participants, and they have produced mixed results. Regarding studies of ACEs prevalence, Wilkins et al. (2017) found that a sample of American Christian international missionaries reported an average ACEs score of 1.49, while Whipple (2020) found that a sample of primarily evangelical ministry workers (including active congregational leaders, chaplains, and church planters) reported an average ACEs score of 2.07. During this period, the average ACEs score in the United States was 1.56 (Giano et al., 2020). However, as neither Wilkins et al. (2017) nor Whipple (2020) conducted a demographically matched comparison between their samples and the general population, it is hard to accurately interpret what their findings indicate about the prevalence of ACEs among those working in ministry. In addition, though not an ACEs domain, Burton and Topham (1997) studied the prevalence of experiencing the death of an important adult during childhood among individuals from various professions in the United Kingdom. They found that, while 47% of the clergy experienced the loss of an important adult in their childhood, only 27% of therapists and 4% of engineers had this experience (Burton & Topham, 1997). Taken as a whole, past research does not offer an easily interpretable or uniform picture of the rates of childhood trauma among those in ministry. As a result of these mixed results, more research is needed to better understand experiences of childhood trauma among those selecting the pastorate.
Method
We used data from the Seminary-to-Early Ministry (SEM) study: a mixed-methods, longitudinal cohort study of seminary students at a Mainline Protestant Divinity School (Eagle et al., 2023). This Divinity School is founded and supported by the United Methodist Church (UMC). While predominantly United Methodist, the school also attracts students from other religious traditions. We used survey data collected from students entering a master’s program in the fall of 2019–2022. Surveys were administered online, and response rates ranged from 73% to 83%. Aggregated, the total number of students was 535. Table 1 gives the basic demographic information about our sample of seminary students. All students provided informed consent and study procedures were approved by the [Duke] Campus Institutional Review Board.
Seminarian Sample Characteristics (Total Sample N = 535).
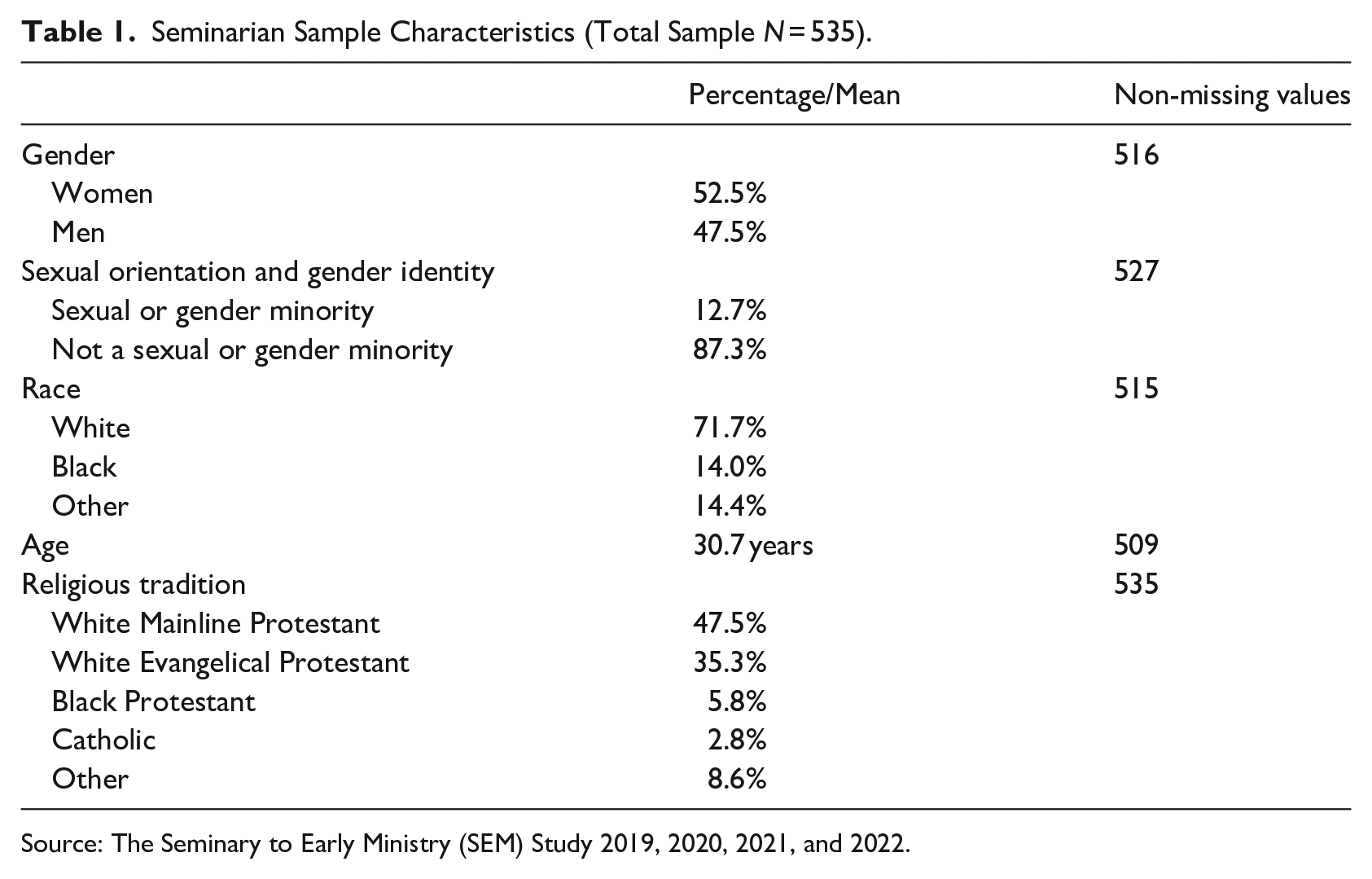
Source: The Seminary to Early Ministry (SEM) Study 2019, 2020, 2021, and 2022.
We also used data from the Behavioral Risk Factor Surveillance System (BRFSS) study to compare our sample with the general U.S. population (Centers for Disease Control and Prevention, 2021). The BRFSS is a state-based surveillance system that collects data on behaviors and conditions that place non-institutionalized adults at risk for chronic disease. Interviewers collect data monthly using an independent probability sample of households with telephones. We used data from the 2019–2021 BRFSS. Not all states collect data on ACEs and our analysis includes only those states with an ACEs module. 1 The aggregate sample size for the 3 years of BRFSS data with relevant measures was 401,958.
When comparing the seminarian sample with the U.S. population, we limited the age of BRFSS respondents to between 21 and 74 years (the youngest and oldest respondents in the SEM study). We also removed any BRFSS respondents who did not have at least a bachelor’s degree (all students in the SEM study have a bachelor’s degree). We then used raking, or sample balancing (Battaglia et al., 2009; Lumley, 2004), to adjust the survey weights in the BRFSS based on age and race. Once the samples were balanced based on education, age, and race, we confirmed that the gender distribution and distribution of sexual or gender minority status were also balanced. Raking was done via the survey package in R (Lumley, 2004). Conducting this demographically matched comparison between our sample of seminarians and the BRFSS data allows us to accurately compare the findings from our study with the national prevalence of ACEs.
Our outcome of interest is ACEs. There are eight central ACE domains, all of which must have occurred prior to age 18 years (Giano et al., 2020): living with someone with a mental illness, living with someone who abused alcohol or drugs, having an incarcerated family member, having separated or divorced parents, experiencing adults in the home physically harm one another, personally experiencing physical abuse, personally experiencing emotional abuse, and personally experiencing sexual abuse. In addition, respondents were given a composite ACEs score, calculated by summing the number of ACEs experienced, with values from 0 to 8. In the SEM and BRFSS data, ACEs domains and total scores were calculated in the same way, though there were slight wording differences in some ACE domains—mostly notably the sexual abuse item. 2 Details of question wording can be seen in Table 2.
Wording of Each ACE Domain in the BRFSS and SEM Studies.
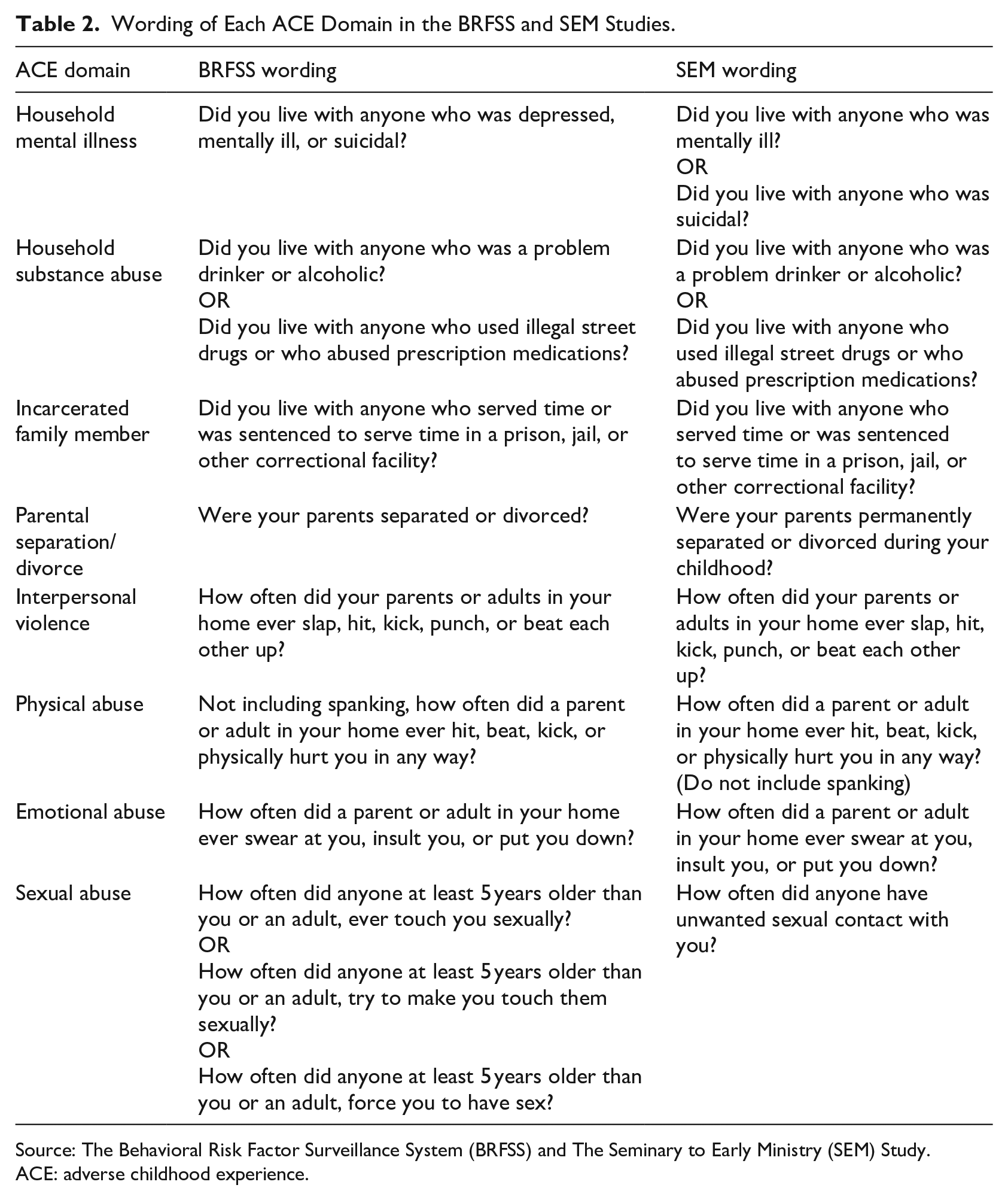
Source: The Behavioral Risk Factor Surveillance System (BRFSS) and The Seminary to Early Ministry (SEM) Study.
ACE: adverse childhood experience.
We account for a variety of demographic factors that could confound observed relationships: age, gender, sexual and gender minority (SGM) status, and race (in the BRFSS and SEM data). For the bivariate analysis, age was coded into a binary variable indicating respondents <30 years. Age was kept as a continuous variable in the multivariate analysis. Gender was coded as “male” or “female.” We coded respondents as SGM if they indicated they had any sexual orientation other than heterosexual, if they indicated their gender identity was an identity other than “male” or “female,” or if they indicated their current gender identity was different than their sex assigned at birth. We coded race into three categories: White and non-Hispanic, Black and non-Hispanic, and other. Although the SEM sample contains individuals from other racial and ethnic backgrounds, sample size was not sufficient to separate out other groups for analysis. In the multivariate analysis, we collapse this to White and non-White.
Results
Figure 1 shows the unadjusted prevalence of ACEs among our sample of seminarians, as well as the comparison to national estimates of ACEs prevalence among a demographically similar population. We found that the average seminarian in our sample reported an average of 1.8 ACEs (95% CI = [1.7, 2.0]), which is approximately the same as the average in the matched U.S. sample (1.8 ACEs, [1.7, 1.8]). However, we did find significant differences among five of the eight ACEs between our sample of seminarians and the matched U.S. sample. Seminarians in our sample were significantly more likely to have experienced emotional abuse during childhood, with 52.6% (95% CI = [48.1%, 57.1%]) of seminarians having this experience, compared with 39.4% (95% CI = [37.9%, 40.9%]) of the matched U.S. sample. Seminarians in our sample were also significantly more likely to have lived during their childhood with someone experiencing mental illness, with 35.8% (95% CI = [31.5%, 40.1%]) of seminarians compared with 24.8% (95% CI = [23.6%, 26.1%]) of the matched U.S. sample. In addition, seminarians in our sample seem to be somewhat more likely to have experienced sexual abuse during childhood than the matched U.S. sample: 20.2% (95% CI = [16.6%, 23.8%]) of seminarians, compared with 9.2% (95% [8.4%, 9.9%]) of the matched U.S. sample. 3
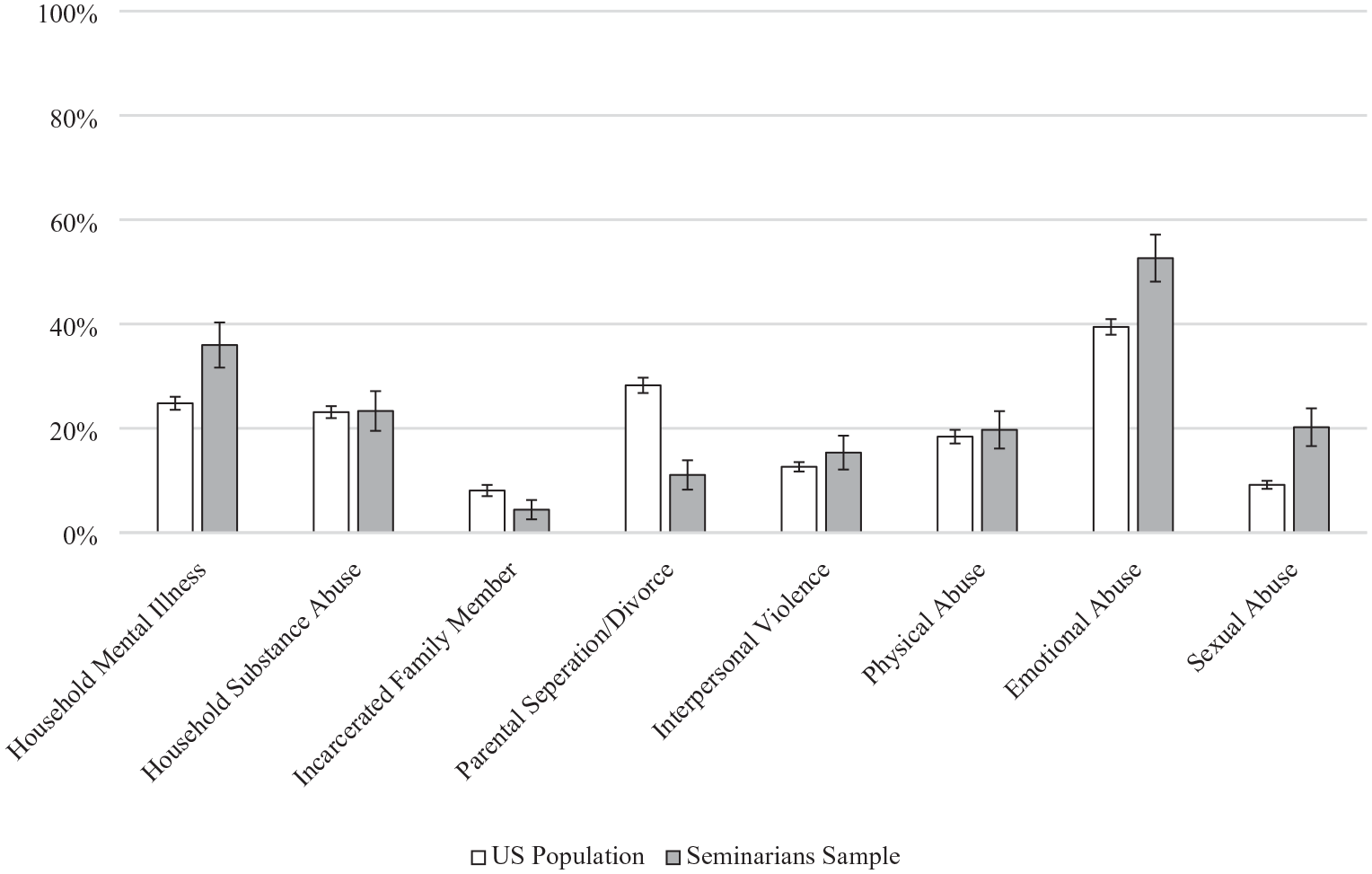
Comparison of demographically matched U.S. population ACEs prevalence to sample of seminarians.
We also found that the seminarians in our sample experienced both parental separation or divorce and living with an incarcerated family member less often than the matched U.S. sample. Only 11.1% (95% CI = [8.3%, 13.9%]) of seminarians had parents that separated or divorced, while the matched U.S. sample had a prevalence of parental separation or divorce of 28.2% (95% CI = [26.8%, 29.7%]). Also, while only 4.4% (95% CI = [2.6%, 6.3%]) of our sample lived during childhood with an incarcerated family member, the matched U.S sample had a prevalence of living with an incarcerated family member of 8.1% (95% CI = [7.0%, 9.1%]). We did not find any significant differences between the seminarian sample and the matched U.S. sample in the prevalence of household substance abuse, interpersonal violence, or physical abuse.
Within our sample of seminarians, we also found that the prevalence of ACEs varied by seminarians’ demographic characteristics, as seen in Table 3. Women as compared with men seminarians were significantly more likely to have experienced living before the age of 18 years with someone who was mentally ill (41.4% vs. 29.7%; p < .01), and women seminarians were >2.5 times more likely to have experienced childhood sexual abuse (28.2% vs. 11.5%; p < .001). SGM seminarians had higher composite ACEs scores compared with non-SGM seminarians (2.4 vs. 1.7; p < .01). SGM students also had a higher prevalence of household mental illness (50.0% vs. 33.7%, p < .05), higher prevalence of physical abuse (33.9% vs. 17.6%, p < .01), and higher prevalence of sexual abuse (32.3% vs. 18.4%, p < .05).
Prevalence and Bivariate Comparisons of ACE Domains and Mean ACE Score by Sociodemographic Characteristics Among Seminarians.
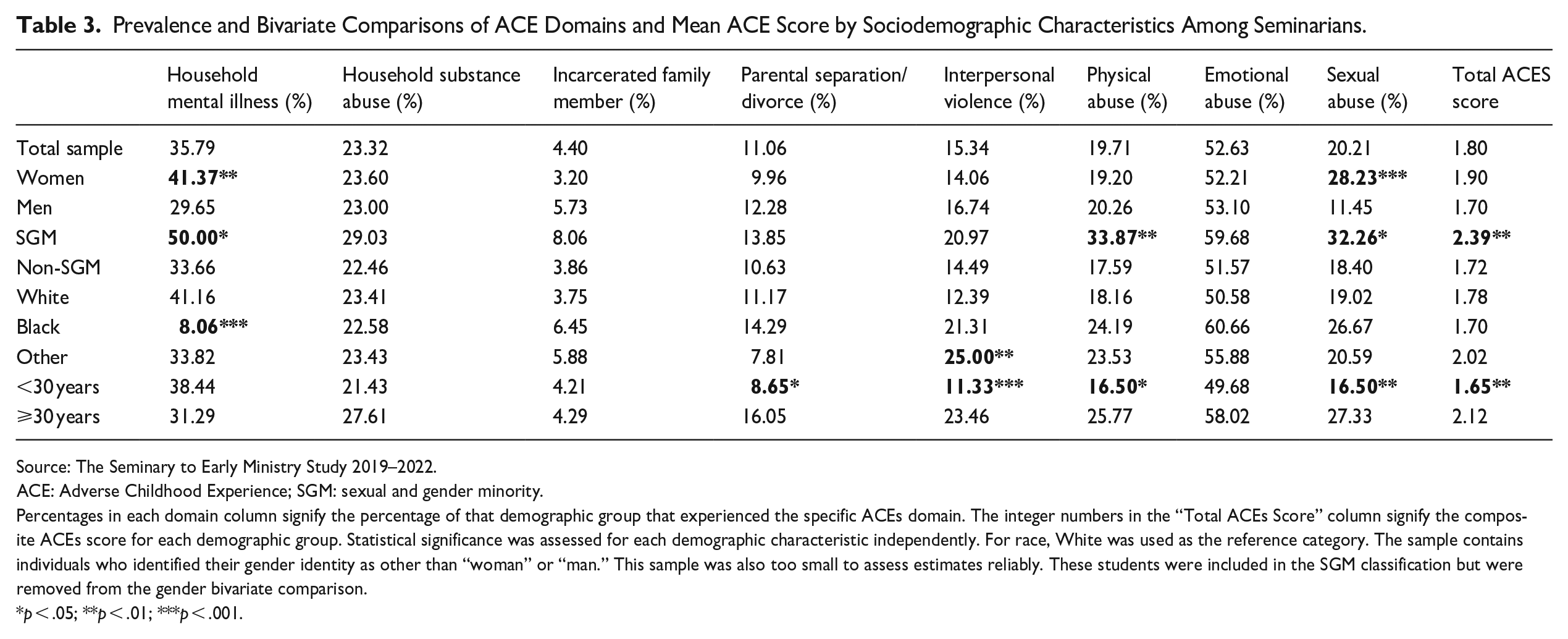
Source: The Seminary to Early Ministry Study 2019–2022.
ACE: Adverse Childhood Experience; SGM: sexual and gender minority.
Percentages in each domain column signify the percentage of that demographic group that experienced the specific ACEs domain. The integer numbers in the “Total ACEs Score” column signify the composite ACEs score for each demographic group. Statistical significance was assessed for each demographic characteristic independently. For race, White was used as the reference category. The sample contains individuals who identified their gender identity as other than “woman” or “man.” This sample was also too small to assess estimates reliably. These students were included in the SGM classification but were removed from the gender bivariate comparison.
p < .05; **p < .01; ***p < .001.
Compared with White students, Black students were less likely to have experienced household mental illness (41.2% of White students, 8.1% of Black students, p < .001), and White students were less likely to have experienced interpersonal violence (12.4% of White students and 25.0% of non-White and non-Black students; p < .01). Seminary students aged ⩾30 years had significantly higher composite ACEs scores than students <30 years (2.1 vs. 1.7; p < .001); had higher rates of parental separation or divorce than students younger than 30 years (16.1% vs. 8.7%; p < .05); were more likely to have experienced interpersonal violence (23.5% vs. 11.3%; p < .001); were more likely to have experienced physical abuse (25.8% vs. 16.5%; p < .05); and were more likely to have experienced sexual abuse (27.3% vs. 16.5%; p < .001).
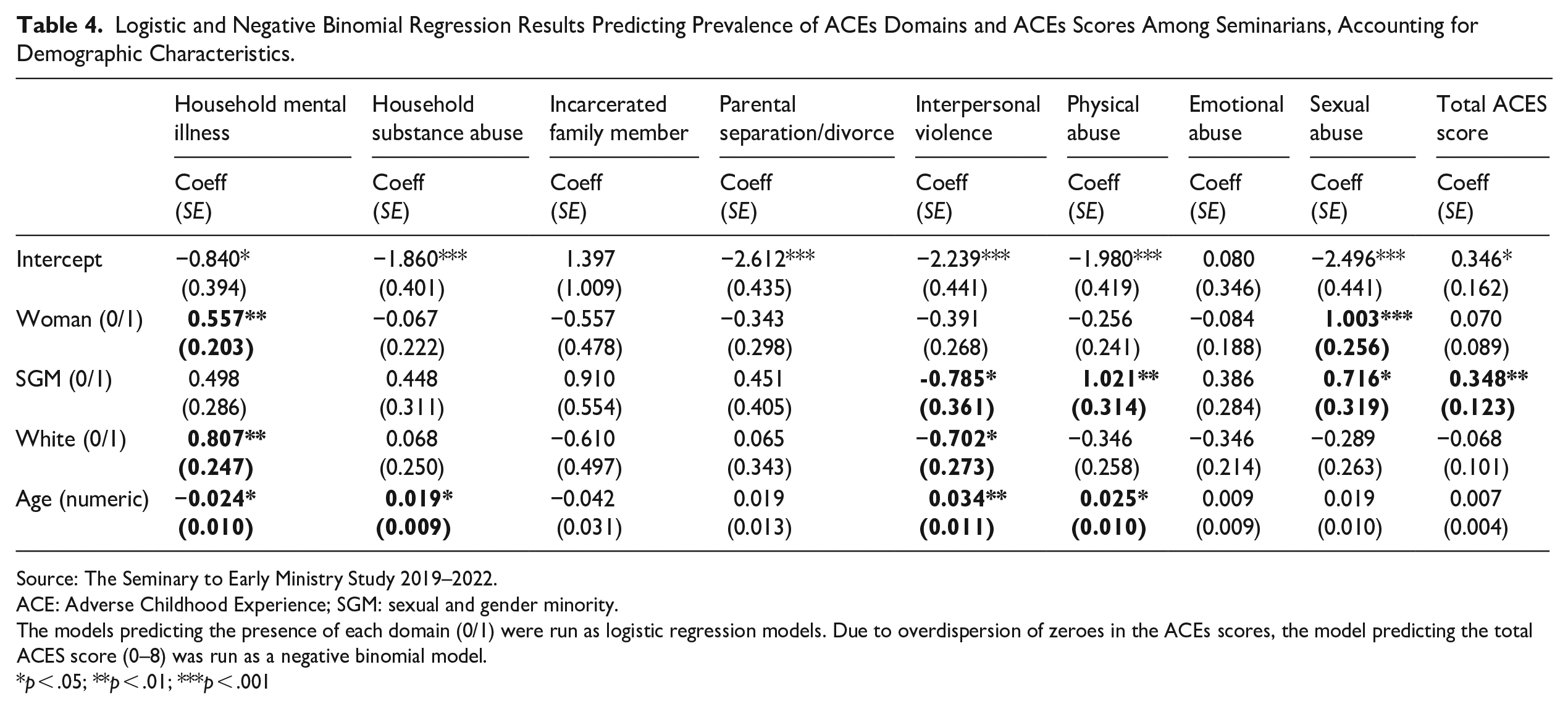
Table 4 reports the results of multivariable models, in which the outcomes are the occurrence of each ACE domain and the composite ACE score. When controlling for other factors, we found that women demonstrated a higher prevalence of household mental illness (p < .01) and a higher prevalence of childhood sexual abuse (p < .001). We also found that when accounting for other demographic characteristics, SGM seminarians demonstrated a higher prevalence of household interpersonal violence (p < .05), higher prevalence of childhood physical abuse (p < .01), higher prevalence of childhood sexual abuse (p < .05), and higher composite ACEs score (p < .01).
Logistic and Negative Binomial Regression Results Predicting Prevalence of ACEs Domains and ACEs Scores Among Seminarians, Accounting for Demographic Characteristics.
Source: The Seminary to Early Ministry Study 2019–2022.
ACE: Adverse Childhood Experience; SGM: sexual and gender minority.
The models predicting the presence of each domain (0/1) were run as logistic regression models. Due to overdispersion of zeroes in the ACEs scores, the model predicting the total ACES score (0–8) was run as a negative binomial model.
p < .05; **p < .01; ***p < .001
The race and age patterns were more complex. Even when controlling for other demographic factors, White students were significantly more likely to have experienced household mental illness (p < .01), but significantly less likely to have experienced household interpersonal violence (p < .05). Also, even when controlling for other factors, as age increased among our sample of seminarians, students were more likely to have experienced household substance abuse (p < .01), household interpersonal violence (p < .01), and childhood physical abuse (p < .05), but less likely to have experienced household mental illness (p < .05).
Discussion
The goal of this study was to examine how the prevalence of ACEs may differ between individuals selecting into ministry (in this case, those currently attending seminary) and the general population. We found that, in a sample of seminarians at a Mainline Protestant divinity, overall levels of ACEs were not statistically different than a demographically matched sample of U.S. individuals. However, seminarians in this sample were more likely than the matched population to have experienced childhood emotional abuse and more likely to have lived during childhood with someone with mental illness. Seminarians in our sample also were slightly more likely to have experienced childhood sexual abuse, though we interpret that difference with caution, as the wording of the sexual abuse question differed between the seminarian sample and the national sample. Seminarians in our sample were less likely to have experienced parental separation or divorce during childhood, or to have a family member be incarcerated.
The three ACE domains which seminarians showed a marked increase relative to the general population is notable. In various studies researching the relationship between individual ACE domains and mental health outcomes, childhood experience of emotional abuse was the ACE domain that bore the strongest relationship with elevated depressive and anxiety symptoms, suicide attempts, substance use, symptoms of post-traumatic stress disorder, and aggression later in life (Dube et al., 2001; Merrick et al., 2017; Negriff, 2020; Nurius et al., 2012). Other studies have found that growing up in a household with an adult experiencing mental illness bears the strongest association with having elevated depressive and anxiety symptoms and low life satisfaction later in life (Giano et al., 2021; Hughes et al., 2016; Lanier et al., 2018; Nurius et al., 2012). Still other studies found that experiencing childhood sexual abuse was the most strongly associated with elevated depression symptoms and low life satisfaction later in life (Hughes et al., 2016; Schilling et al., 2007). Although there is not yet a scholarly consensus on the ACE domain that is most predictive of poor mental health symptoms, it is clear that the three ACE domains for which our sample shows a higher prevalence of relativity to the general population are especially important predictors of poor mental health later in life.
We also found that women seminarians and seminarians who identified as sexual or gender minorities demonstrated especially high prevalence of some ACE domains, compared with men and non-SGM seminarians in our sample. This mirrors past research among the general population (Giano et al., 2020) and strongly suggests that institutions should target these students for additional support, as research has shown that students in these demographic categories already face significant barriers in seminary (Adams, 2007; Kleinman, 1984; Stevens, 1989). In addition, despite past findings that younger individuals typically report a higher prevalence of ACEs (Giano et al., 2020), we found that older individuals reported higher ACEs prevalence in our sample of seminarians. This may simply be a result of our sample being relatively young overall (with an average age of 31 years), but it may also be an indication of the process of selection into ministry, especially among older individuals.
Two important implications follow from our findings. First, this work suggests that considering potential “upstream” causes of clergy mental health, especially among Mainline clergy, will be important for understanding the mechanisms by which the clergy demonstrate poor mental health. As past research has focused primarily on occupational conditions, rather than selection into the occupation, further research is needed. Importantly, in this analysis we did not empirically test for the relationship between ACE domains and mental health symptoms among our respondents at the start of seminary or throughout their seminary or ministry careers. In documenting the prevalence of ACEs and specific ACE domains among our respondents, we have sought to demonstrate the potential theoretical link between ACEs and mental health among the clergy, and to urge future research on this topic.
Second, this work suggests that seminaries and divinity schools may have student bodies with above-average prevalence of traumatic experiences during childhood. Theological schools should consider providing targeted programs and services to those with a history of ACEs, to best equip those students to enter pastoral ministry while maintaining mental wellness. There are several major classes of interventions that have shown promise for people suffering from stress symptoms related to childhood trauma (Karatekin, 2019; Kirlic et al., 2020; Lorenc et al., 2020). Many people with complex trauma histories require specialized care from trained mental health professionals. Confidentially screening incoming seminary students for ACEs and associated problems with mood symptoms, emotional regulation, and managing interpersonal interactions is a potential first step for seminaries to understand their students’ backgrounds and potential mental healthcare needs. This screening data could be used to connect students to professionals who specialize in treating people with experiences of childhood trauma. Specific manualized therapeutic programs could also be offered in group settings with trained professionals, such as Skills Training in Affective and Interpersonal Regulation Skills and Mindfulness-Based Stress Reduction. These programs have been shown to be effective in improving mood, emotional regulation, anxiety, and interpersonal stress in people suffering from the adverse effects of trauma (Kirlic et al., 2020).
This work is particularly important for the aspiring clergy, as being exposed to vicarious and secondary trauma occurs frequently in the context of pastoral ministry (Hendron et al., 2012; Roggenbaum et al., 2023). These experiences are an unavoidable part of a clergyperson’s occupational responsibilities, and they have been shown to be particularly emotionally difficult for individuals with ACEs (Figley, 1995; Pearlman, 1999; Slattery & Goodman, 2009; Morgan et al., 2022). As unresolved trauma histories are often associated with difficulties managing interpersonal relationships, often via emotional dysregulation (Poole et al., 2018), this could pose major challenges for clergy who work in an emotionally demanding and interpersonally complex job. Seminaries have a responsibility to prepare students for the theological, spiritual, and emotional demands of ministry.
This study is not without limitations. First, this sample of seminarians comes from four entering cohorts at a single Mainline Protestant divinity school. We were not able to make significant comparisons on the basis of religious tradition or race, as this group of students was overwhelmingly Mainline Protestant and White. Past research has demonstrated that Black and Hispanic/Latinx individuals in the United States report a higher aggregate ACEs score compared with White individuals, and that there are marked differences in the prevalence of specific ACE domains among different racial groups (Giano et al., 2020). Further research is needed to understand how the patterns found in this analysis may replicate in other seminary contexts, especially in seminary contexts with a greater percentage of seminarians of color. Second, in this analysis, we only establish the prevalence of ACEs in our sample, and we cannot yet speak of how individuals with a high number of ACEs or who have experienced certain ACE domains will fare over the course of seminary or as they enter their careers in ministry. Third, as already noted, the comparison between our data and the BRFSS sample cannot be perfectly aligned on the ACE domain regarding sexual abuse. We believe that these measures are close enough to approximate a comparison, with caution, but future research will need to be done to confirm this finding.
In her work concerning childhood trauma among social work interns, Sharon Lyter wrote that these “wounds can serve as a risk factor as well as a protective factor that promotes one’s ability to perform” (Lyter, 2008, p. 35). We echo these sentiments in our conclusions concerning ACEs among seminarians as future pastoral leaders. Although we assert that the prevalence of ACEs—and especially the elevated rates of emotional abuse, household mental illness, and sexual abuse—among this sample of seminarians is important to address, elevated ACE scores should not disqualify someone from pastoral ministry. If seminarians and pastors understand the impact of ACEs on their lives and adopt successful emotional management strategies, they can use their experiences to connect with others with similar backgrounds. The findings presented in this analysis highlight the need for seminaries and divinity schools to provide resources for students with these experiences. It should also draw attention to the need to better understand “upstream” causes of poor pastoral mental health.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is funded by a grant from the Rural Church Area of The Duke Endowment.
1.
In 2019, the following states included the ACEs module: AL, DE, FL, IN, IA, KS, MI, MS, MO, NM, NY, ND, OH, OK, PA, RI, SC, TN, VA, WV, WI. In 2020: AL, AZ, CA, DC, FL, GA, HI, ID, IA, KS, KY, MD, MA, MS, MO, MT, NV, NJ, ND, OK, RI, SD, SC, TX, UT, VA, WI, WY. In 2021: AL, AR, IA, KS, ME, MS, NV, NH, NJ, NY, ND, OH, OR, SC, VA, WI.
2.
The Seminary-to-Early Ministry (SEM) and Behavioral Risk Factor Surveillance System (BRFSS) questionnaires inquire about sexual abuse slightly differently. In the SEM questionnaire, only one item measured experience of sexual abuse prior to age 18: “How often did anyone have unwanted sexual contact with you?” The BRFSS questionnaire uses three items, and qualifies that the sexual abuse was enacted by an individual at least 5 years older than the respondent (Regarding experiences prior to age 18: “How often did anyone at least 5 years older than you or an adult, ever touch you sexually?”; “How often did anyone at least 5 years older than you or an adult, try to make you touch them sexually?”; “How often did anyone at least 5 years older than you or an adult, force you to have sex?”). Therefore, we cannot make a perfectly accurate comparison between the rates of sexual abuse between the SEM data and BRFSS data. However, past research has demonstrated that, among instances of sexual abuse during childhood, the average age difference between perpetrator and victim of childhood abuse is close to 10 years (Hassan et al., 2015; McKillop et al., 2015). Therefore, though the BRFSS data likely slightly underestimates the prevalence of childhood sexual abuse compared with the SEM data, we believe the measures are close enough to make approximate comparisons, with caution in our conclusions.
3.
We say “somewhat more likely” here to indicate to the reader that we interpret this finding with some caution. As mentioned in the “Method” section, the SEM and BRFSS questionnaires inquire about sexual abuse slightly differently, such that the BRFSS data likely slightly underestimates the prevalence of childhood sexual abuse relative to the SEM data. See “Method” for more details.