
Abstract
Police-led drug diversion (PDD) schemes can divert individuals caught in possession of controlled substances away from the harms associated with criminal justice pathways and toward treatment, education, or welfare support. As an alternative to prosecution, it has been established that the use of well-implemented diversion schemes may lead to reductions in reoffending, efficiencies in police time, and reductions in costs for the wider criminal justice system. However, there has been insufficient evidence to draw conclusions about the role that needs assessments play in achieving the desired aims of PDD. This paper analyzes how three PDD schemes in England provide opportunities for individuals to make life-improving changes, focusing on the role of needs assessments. Adopting a realist framework to evaluate diversion schemes in three police forces, we carried out semistructured interviews with police officers, diversion staff, individuals who had been diverted, and other stakeholders. We identified multiple opportunities to assess the needs of people who use drugs. This included the initial interaction with the police, subsequent screening processes (often referred to as “triage”), and at other points of interaction with the diversion service provider. While all schemes provided opportunities for the diverted individual to receive relevant support, there was considerable variation in how this was made available. PDD scheme components included: the duration of the program; the process of referrals to other services; the nature of support; the level of handholding and signposting; and how the support matched the individual's specific needs. Despite variation across police forces, PDD schemes can provide opportunities which enable people who use drugs to begin to recognize, communicate, or acknowledge their own needs. Our findings suggest that the breadth of harm reduction claims—which are central to many PDD scheme aims—can be better realized when assessment of individual needs leads to tailored support and meaningful engagement with health and wider social services.
Introduction
A growing evidence base demonstrates how the “war on drugs” has proved ineffective (Coyne & Hall, 2017; Global Commission on Drug Policy, 2011), with claims that it has contributed to harmful drug policy that disproportionately impacts certain ethnic groups (Rosino & Hughey, 2018) and the marginalized in society (Zampini & Stengel, 2025). Globally, over recent decades, there has been a trend toward decriminalization of low-level drug possession, to the extent that this has been referred to as a “quiet revolution” (Eastwood et al., 2016). Despite this, however, enforcement-led prohibition, which has proved neither a deterrent nor a solution, has continued unabated in the UK, where no Class A-C drug has been decriminalized or legalized (other than for medical use) and where police and criminal justice resources are stretched. In this context, the policy debate regarding the punishment of people who use drugs has heightened. It highlights the harmful impact on the future life chances of those who are charged and prosecuted (Ward, 2013). In addition to the established physical and mental harms associated with drug use for the individual (Degenhardt & Hall, 2012), Bacon and Spicer (2023) draw on a broad evidence base to advocate “harm reduction policing” (HRP). This mitigates the wider harms caused by ineffective, punitive interventions associated with drug use, including stigma, marginalization, and longer-lasting consequences that might lead to further vulnerability and discrimination, such as unemployment and lack of secure housing.
Preventing harm through changes to drug policy (Walcott, 2023) was a compelling rationale for the emergence of out-of-court drug diversion policies in the UK, which are akin to those already applied in other European jurisdictions (Stevens et al., 2019). Out-of-court resolutions (OOCRs) are primarily used for low-level or first-time offending and are intended to provide proportionate, efficient, and rehabilitative responses. Administered by police discretion using preset eligibility criteria, officers have a number of different conditional and unconditional out-of-court options (the number of options is currently under NPCC review to simplify diversion outcomes (Grant & Heydari, 2022). Such policies, as a substitute for prison sentences, could also prevent net-widening (Kantorowicz-Reznichenko, 2013) and further reduce demands on already overburdened police and criminal justice resources (The Law Society, 2024).
There is increasing evidence that the provision of pre or postarrest diversion programs can reduce recidivism, improve public health through education and support, and improve life chances by addressing the root causes of drug-related issues and by avoiding the harms and stigma of criminalization (Collins et al., 2015a; 2015b; Scher et al., 2023; Stevens et al., 2019). One of the most notable alternatives to prosecution is Seattle's Law Enforcement Assisted Diversion (LEAD) program, launched in 2011. LEAD seeks to divert individuals engaged in low-level offenses away from the criminal justice system (CJS) and into supportive, community-based services. The program is grounded in three core components: diversion from prosecution, harm-reduction oriented case management that does not require abstinence, and coordinated support for managing legal and social challenges.
Although such diversion away from criminalization is not a new phenomenon (Bacon, 2024), there is a new wave of diversion schemes in England and Wales, which we refer to as police-led drug diversion (PDD). Initiated by the police, examples include West Midlands’ DIVERT (Jones & Twomey, 2023), Avon and Somerset's Drug Education Programme (De Viggiani, 2022), Thames Valley's Drug Diversion Pilot (Spyt & Kew, 2023), and Durham's Checkpoint (Weir et al., 2021). Holding a more centralized position in the police's response to drug use, these schemes aim to redirect people who use drugs away from harmful involvement with the CJS and into education or treatment (Stevens et al., 2023). Considered a more proportionate response than criminal sanctions, PDD schemes have gained increased political support following recommendations proposed by Dame Carol Black in the second part of her commissioned review on drugs (Black, 2021), which focuses on prevention, treatment, and recovery.
Political, police, and public perceptions of people who use drugs are complex and emphasize the tension between criminal justice and public health approaches. Adoption of a public health, HRP, trauma-led approach promotes care and understanding rather than punishment. Bacon and Spicer (2023) position out-of-court diversion as a mix of care and control. This demonstrates how diversion can offer support, treatment, and wider welfare-oriented interventions, while still operating within a criminal justice framework that can monitor compliance, impose conditions, and retain the threat of prosecution for nonengagement. However, tensions between the aims of different drug diversion schemes can arise due to the complexity of competing priorities within the justice and health systems. In their systematic review of 27 articles addressing harm reduction through diversion programs, Blais et al. (2022) found that some schemes prioritize reducing reoffending and easing pressure on courts and prisons, focusing on swift case resolution and cost efficiency. Others emphasize public health goals, such as harm reduction (including reduced health risks and fewer overdoses), treatment engagement, and addressing underlying causes of substance use. Some schemes aim to secure complete abstinence and crime reduction enforced through punitive measures. Although reduction of drug use might be an outcome of PDD, it is not a primary aim. This highlights a tension with the then UK Government's aim to reduce drug-related offending, drug deaths and drug use through Project ADDER (Addiction, Diversion, Disruption, Enforcement, and Recovery), launched in 2020 (Home Office, 2025), and their 10-year strategy to cut crime and save lives by reducing the supply and demand for drugs and delivering a high-quality treatment and recovery system (HM Government, 2021). Such welfare-first approaches understand that some people who use drugs—particularly those with substance use disorders—are often victims whose drug use is a symptom of underlying factors such as poor physical or mental health, often caused by abuse and trauma (Butler et al., 2022; Ullman et al., 2013).
Paradoxically, public health approaches also frame the individual within libertarian views of human rights—that, despite the harms associated with drug use, they are free to make choices and therefore informed and safe choices are deemed preferable. PDD is based on choice where an individual's options are clearly explained, their response is voluntary—with no coercion or control—and they are offered support even when they do not wish to stop using drugs (Bacon, 2024). However, this apparent choice could be questioned when the offer of diversion (with or without conditions attached) is the sole alternative to criminalization.
Those who do choose diversion are not a homogeneous group. While some people who use drugs may have substance use disorders, many who are caught in the net of the CJS do not have such a treatable disorder, even if they regularly—or occasionally—use illicit drugs. The challenge for PDD interventions, then, is how to tailor effective service provision to this diverse group of service users. We argue that understanding the circumstances, needs, and motivations of this group of users is a necessary function to support the success of PDD schemes—even when definitions of success are sometimes ambiguous, difficult to measure and vary across different devolved Parliaments in the UK and across police forces in England and Wales (House of Commons Home Affairs Committee, 2023).
This article draws on existing literature and new empirical research to examine how individual needs are assessed across three PDD schemes in England. Its central contribution is to foreground the lived experiences, health vulnerabilities and structural barriers faced by people who use drugs as integral to the design and delivery of effective diversion policy. The analysis demonstrates how needs assessments can shape diversion pathways and inform the development of personalized interventions—including treatment, education, and broader social support—not solely to alleviate pressures on policing or to prevent harms associated with the CJS, but to facilitate meaningful behavioral and social change. Crucially, it highlights the importance of incorporating individual voice and autonomy within assessment processes, ensuring that people who use drugs are not positioned merely as subjects of risk management but as active participants in identifying their own priorities, capacities, and support needs. By examining whether and how assessment mechanisms are embedded within each scheme, this article highlights the significance of incorporating a structured understanding of individual circumstances into diversion practice. This reframes diversion beyond a narrow emphasis on enforcement outcomes or arrest metrics, positioning it instead as a mechanism for responding to complex health and social needs. The variation in aims, resources, and operational models across PDD schemes accentuates the importance of robust assessment processes to ensure that individuals are directed toward the most appropriate forms of support.
The Role of Needs Assessments in Police-led Diversion Schemes
Diversion programs may struggle to simultaneously satisfy demands for justice, measurable performance outcomes, and long-term therapeutic change if there is a conflict between standardized diversion program content and the need for flexible, individualized support (Sutton et al., 2025). A potential response to the complex and heterogeneous needs of divertees is the introduction of a formalized “triage” stage within diversion processes, explicitly designed to assess individual circumstances and levels of need. Such an approach would enable systematic identification of health, social and criminogenic factors at an early point of contact, thereby supporting more proportionate and appropriately tailored interventions.
When conducted in custody settings (typically postarrest), triage has played a crucial role in identifying the wider welfare needs of detained individuals (Skinns, 2019). Typically carried out by Liaison and Diversion teams, which comprise health and social care professionals with specific expertise and experience in criminal justice settings, these assessments not only inform immediate responses but can also lead to referrals to services addressing mental health, substance use, housing, and trauma (Annison et al., 2018; McKinnon et al., 2016). In England, this model has been evaluated by stakeholders as overwhelmingly positive; it provides useful information about vulnerabilities and has led to closer working between the CJS, mental health services, other professionals, and the police and courts (Disley et al., 2016). Although the focus of this article is on needs assessments conducted within PDD schemes, it is important to note that some individuals may undergo concurrent vulnerability or risk assessments in police custody where a formal PDD triage process exists. Processes may therefore overlap informally, with Liaison and Diversion practitioners and custody officers sharing information that contributes to a broader, though variable, understanding of an individual's circumstances. Conversely, individuals may miss out on comprehensive needs assessments and the supportive referrals that often follow if they are diverted away from the assessment processes that are in place in custody—especially through brief, nonclinical diversion interventions by police officers on the streets.
Research commissioned by the Ministry of Justice on how police in England and Wales use out-of-court options to support adults with health-related vulnerabilities identified how training of police officers and staff, particularly in relation to conducting vulnerability assessments, was generally conducted on an ad-hoc basis rather than through structured training programs (Strang et al., 2024). Furthermore, staff turnover and inexperienced officers contributed to a lack of understanding of the needs of people who use drugs. Strang et al. (2024) found that most forces did not have a policy requiring a health vulnerability screening and assessment during the OOCR decision-making process. This reveals the necessity of incorporating such assessments at a subsequent stage within the diversion pathway, particularly where PDD initiatives seek to enhance health and welfare outcomes.
Triage has proved effective for the evaluation of patients with substance use disorders when deciding to divert to hospital admission or to appropriate outpatient interventions (Penzenstadler et al., 2023) and to assign people who use drugs to relevant interventions based on their risk-and-need profile (Marlowe et al., 2011). Moving away from language associated with medicalized treatment models, we use the term “needs assessment” (rather than triage) to describe any stage in the diversion process that is designed to understand an individual's specific circumstances—including their physical and mental health and wider welfare needs (Breslin et al., 2003)—to facilitate better matching of diversion interventions.
Although not all PDD schemes include a formal needs assessment stage, the benefits of doing so have been suggested by previous research. These benefits include more tailored and effective interventions, better health and criminal justice outcomes, and reduced rates of reoffending (Hayhurst et al., 2017; Nyland et al., 2024; Zgierska et al., 2021). A well-designed needs assessment can provide an understanding of substance use patterns, capturing the type, duration, frequency, and severity of use as well as contextual factors such as mental or physical health, trauma history, or co-existing medication use—for example, the full behavioral-health assessment and creation of a personal intervention plan in Leon County's diversion program (Blais et al., 2022). This understanding can help to determine appropriate interventions, such as screening for addiction severity to decide if clinical treatment is necessary and what type of support might be most effective (Marlowe et al., 2011; Mee-Lee et al., 2013). Marlowe et al.'s (2011) Risk and Needs Triage (RANT) model differentiates between individuals who require clinical treatment and those who may not, highlighting the importance of tailored responses based on a person's criminogenic and clinical needs (Andrews & Bonta, 2010; Belenko, 2006; Simpson & Knight, 2007). Done well, a needs assessment can help people who use drugs and who come into contact with the CJS to engage with services which may include drug treatment services (Wong & Horan, 2020) and might reduce their offending.
In the absence of effective assessment of need, there is a danger that not enough is done to address the underlying causes of an individual's use of drugs. There is also a risk that people are exposed to too much intervention, to treatment that does not meet their needs and may not align with their motivation to change (Hiller et al., 2002). The risk of over- or under-treatment highlights the need to balance the intervention with the level of need. Not all individuals who use drugs are dependent or addicted with many individuals reporting that they engage in functional or recreational use “alongside otherwise conforming lives” (Askew, 2016, p. 116). Over-medicalization of low-level drug use can lead to unintended harms, such as stigma, unnecessary exposure to clinical settings, or disruption to work and family life (Ginn & Clark, 2017).
Even where drug treatment is not deemed relevant for people who use drugs, assessment of individual needs can be an effective tool to explore physical and mental health, housing instability, family relationships, educational background, employment status, and other personal circumstances such as bereavement, which may influence substance use. Assessments can be used to inform wider service referrals, including mental health services, housing support, education, or employment services—even if these are not covered directly in the diversion scheme content (Clifasefi et al., 2017). Postarrest schemes such as the Together Women Project have demonstrated the value of such assessments for women in contact with the justice system (Brennan et al., 2016). Needs assessments also offer a crucial baseline for tracking outcomes, enabling evaluation of program effectiveness and supporting accountability to funders and stakeholders. However, accountability demands and bureaucratic oversight can inadvertently reproduce surveillance practices and punitive rationalities, contributing to processes of net-widening. Drawing on five years of ethnographic research across multiple sites, Schaible and Gant (2025) emphasize the importance of safeguarding individual autonomy within diversion programs and offer recommendations to ensure closer alignment with foundational harm reduction principles. Questions concerning individual autonomy, the pathologization of social problems and coercion (rather than care) highlight ethical concerns when an assessment of individual needs and participation in a diversion program is presented as the only alternative to criminalization (Caplan, 2006).
Despite evidence supporting the effectiveness of assessment tools, brief screenings are often favored over full assessments due to cost and time considerations (Spooner et al., 2001). This may be based on findings which demonstrate how light-touch drug education programs are sufficient to trigger change for individuals who are already contemplating behavioral change and are motivated to change (De Viggiani, 2022). However, there is recognition that those resistant to change, or those facing difficult personal and social contexts—particularly those from disadvantaged backgrounds—need a greater degree of support to engage with an intervention and for whom change may be much harder (Smith et al., forthcoming). For these individuals, educational courses are unlikely to be effective. This highlights the need for some preintervention assessment and the opportunity to discuss with people who use drugs the nature of meaningful support. There is growing recognition that interventions should be collaborative, involving the individual in identifying their goals and support needs (Åkerblom & Ness, 2023; Madden et al., 2020). Assessments should not only determine eligibility but also empower the person to co-produce a plan that reflects their lived experience and aspirations (Weir et al., 2021).
We argue that assessment of individual needs in the diversion process plays a central role in understanding and addressing the complex factors that may drive, exacerbate, or maintain problematic drug use. While the implementation of needs assessments can be resource-intensive, the potential benefits for individuals, communities, and public systems is substantial. Although there is some evidence supporting the value of triaging the needs of people who use drugs (Marlowe et al., 2011), there remains limited empirical research substantiating the broader claim that embedding structured, trauma-informed, and context-sensitive assessments within diversion schemes constitutes a critical mechanism for understanding individual need and tailoring proportionate responses. In particular, the extent to which such integrated assessment frameworks contribute to sustained reductions in harm, improved individual outcomes, enhanced public health and greater community safety has yet to be demonstrated.
Methodology and Methods
This article draws on data from a realist and quasiexperimental evaluation of PDD schemes in England. The study protocol outlines the overall design, work packages, and methods (Stevens et al., 2023). Here, we focus specifically on findings from the qualitative process evaluation of adult PDD schemes implemented across three police service areas. To protect participant confidentiality, these forces are anonymized and referred to as A, B, and C.
Realist evaluation, developed by Pawson and Tilley (1997), is grounded in realist ontology and epistemology (Bhaskar, 1975) and adopts a generative model of causation. Rather than asking simply whether an intervention works, realist approaches seek to explain what works, for whom, in what circumstances, and why. The aim is to understand how outcomes are produced through the interaction of mechanisms and contexts, recognizing that any intervention may generate multiple and variable outcomes.
A realist methodological approach is well-suited to exploring the needs of individuals who use illicit drugs because it foregrounds the interaction between context, mechanism, and outcome within decision-making processes. An assessment of needs is not a neutral or purely procedural act; it is shaped by organizational priorities, legal frameworks, resource constraints, practitioner discretion, and assumptions about risk, responsibility, and deservingness. Realist inquiry allows analysis of how these contextual conditions trigger different mechanisms—such as perceptions of vulnerability, assessments of compliance, or beliefs about deterrence—which in turn influence whether an individual is diverted, sanctioned, or referred to support. By asking what forms of needs assessments work (for whom, in what circumstances, and why), realist methodology can illuminate how similar individuals experience markedly different pathways depending on how drug use is interpreted at the point of intervention. This approach also makes visible how assessment practices negotiate the tension between care and control, revealing when they enhance agency and harm reduction, and when they reproduce exclusion, net-widening, or coercive forms of intervention.
Desk-based research and workshops with local and national stakeholders informed the development of a preliminary theory of change and PDD program manuals. These manuals were structured using the Template for Intervention Description and Replication (TIDieR) checklist (Hoffmann et al., 2014) and provided a reference point for examining whether any assessment of needs was included in a diversion scheme's processes.
Qualitative fieldwork for the process evaluation was conducted between April 2023 and May 2024. Data collection comprised semistructured interviews with practitioners and individuals diverted through PDD schemes. Interview numbers and participant roles are summarized in Table 1. Sampling continued until data saturation and inductive thematic saturation were reached (Saunders et al., 2018). Practitioner participants included those involved in the design, governance, and delivery of PDD schemes, such as police leads for drug policy and out-of-court disposals, staff from Offices of the Police and Crime Commissioner (OPCCs), scheme managers, and frontline officers. Purposive sampling ensured diversity among frontline officers in terms of role, district, gender, ethnicity, and length of service. Interviews were also conducted with staff from commissioned services delivering diversion and related support, including drug treatment, housing, and employment services.
Interview and Focus Group Participants.
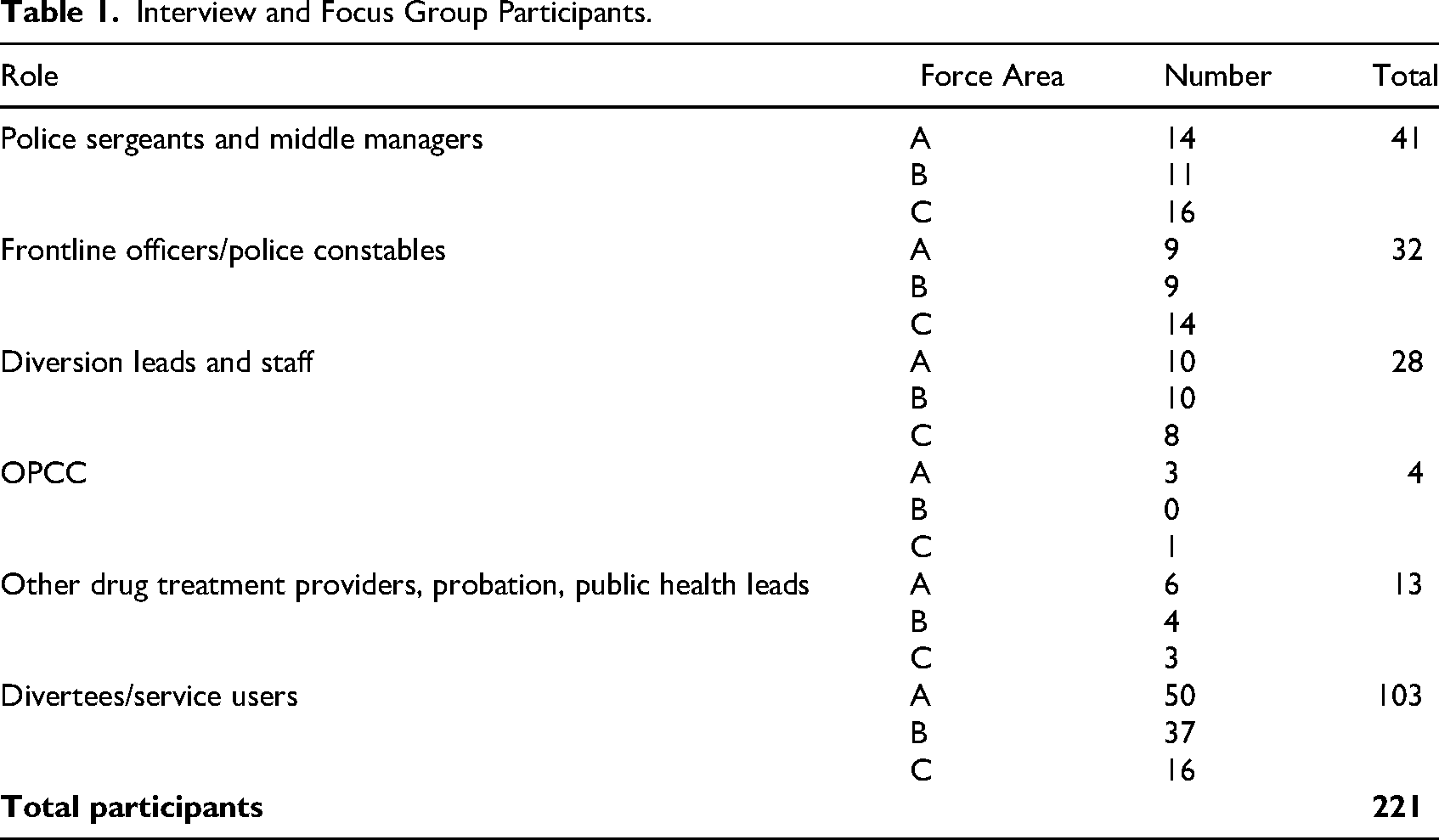
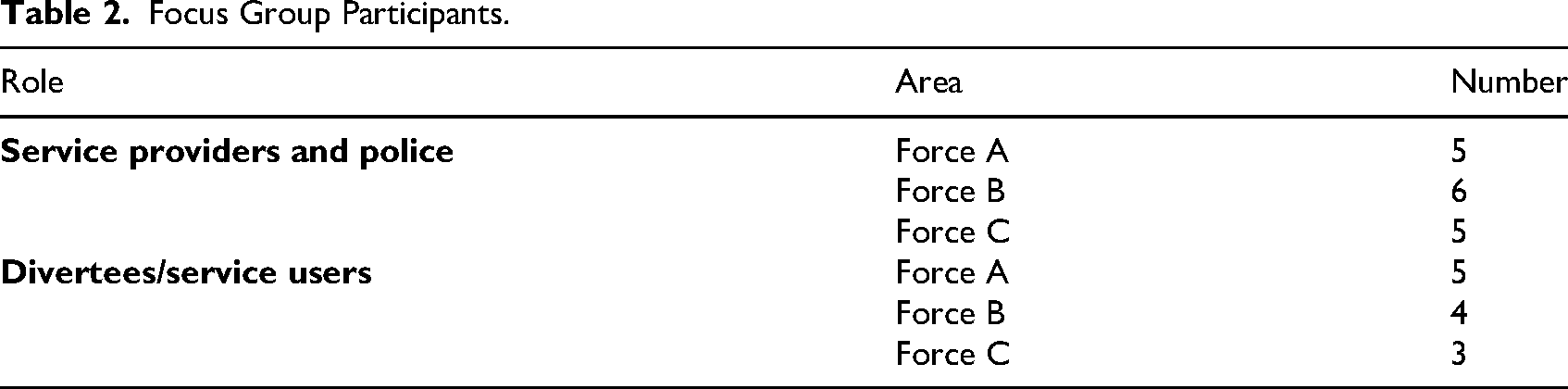
Interviews with individuals eligible for diversion were conducted by peer researchers with lived experience of drug use and criminal justice involvement. These peer researchers were recruited, trained, and remunerated by the partner organization User Voice, drawing on their experiential knowledge and capacity to build rapport. Toward the end of fieldwork, interim findings were discussed in six focus groups composed of interview participants—three with practitioners and three with diverted individuals, as shown in Table 2.
Focus Group Participants.
NVivo qualitative data analysis software was used to support the systematic management, coding, and analysis of interview and focus group data (Dalkin et al., 2020). All transcripts were imported into NVivo to facilitate consistent data organization and transparent analytic processes. Coding was conducted iteratively, combining inductive and theoretically informed approaches, and enabled the research team to compare patterns across participant groups, sites, and stages of implementation. NVivo was used to support abductive analysis (Danermark et al., 2019) by allowing the constant movement between empirical data and conceptual frameworks such as EMMIE (Johnson et al., 2015) as well as retroductive reasoning through the exploration of relationships between codes, contexts, and outcomes. While NVivo did not determine analytic interpretations, it provided a structured environment through which complex qualitative data could be systematically interrogated, supporting the development of explanatory insights into practices associated with needs assessments and how they were implemented in the three schemes.
Regular online meetings and three in-person, day-long workshops (which included peer researchers) enhanced our interpretations during data collection, the analytical phase, and into the writing process.
Findings
Each of the three PDD schemes offered individuals several temporal opportunities to reflect on their relationship with drugs, some of which included questioning the underlying reasons for drug use. However, there was considerable variation in the ways in which individual needs were identified.
First, we outline the nature of any specific “needs assessment” process in each scheme, detailing how individual needs were assessed, where and when it took place and who conducted the assessment. Contextualized by their overarching aims, we then compare the schemes, considering how any assessment of individual needs shaped an intervention to offer more tailored support to promote positive outcomes (Smith et al., 2025). We conclude our findings with examples of missed opportunities for change due to the lack of a specific assessment of needs.
The Nature and Purpose of an Assessment of Individual Needs
Specific Assessment of Needs
The purpose of an assessment of needs in a diversion scheme is to shape how an intervention could be best matched to the individual to offer more tailored support to promote better outcomes. We present our findings of specific needs assessments identified in each scheme.
Force A
The aim of PDD in Force A was to improve the life chances of those who participate through providing information and support to access a wide range of rehabilitative, educational, or other intervention activities in the local community—with the objective that this will reduce or stop offending. PDD operated internally through a dedicated diversion team of police employed civilian staff with health, CJS, or lived experience backgrounds. There had been little change to its model of operation since its implementation in 2015 due to the internalized nature of PDD that negated the need for external PDD delivery providers—as seen in Forces B and C (Smith et al., forthcoming). We identified the emphasis that diversion practitioners placed on the need for individualization across both types of PDD needs assessment and intervention offered in this force (Groups 1 and 2). Staff emphasized the importance of a specific stage of any diversion process where an individual's needs could be assessed to identify the most appropriate pathways that would make up the diversion measure.
The nature of the intervention was moderated, however, by which group divertees were eligible for. Group 1 divertees are those who were caught in possession of cannabis, whether through a standalone possession offense or as a disposal method where other offenses had been committed, for example, someone was arrested for another offense and during police contact, cannabis was also found. Where no other offense was suspected, Group 1 divertees avoided arrest and formal processing in custody, much like the prearrest schemes in Forces B and C. Group 1 was a short, one-off, in-person measure, which comprised a needs assessment process and a one-to-one intervention with the opportunity for onward referrals during the intervention based upon individual need.
Eligibility for Group 2 included other low-level offenses (domestic violence or sex offenses are excluded) where drug use or possession was not necessarily a contributory factor to the offense. This scheme is for adults who are not on probation, have not been detained under the Mental Health Act (Department for Health, 1983), are not already subject to a court order, suspended sentence or conditional caution, and who have not committed an offense or received a caution in the last six months. As the Group 2 PDD scheme was longer in duration (four months of one-to-one meetings with a practitioner), the first session was more formally designated as being a needs assessment, though there was significant overlap in content and substance of the process of assessing needs across both groups:
We’ll do the same assessment as we would [for Group 2]. So, we cover things like housing, mental health, substance abuse, alcohol, relationships, finances, employment, so we’ll cover all of that, but it's a very brief intervention (Abbie, Diversion Practitioner).
The needs assessment process was therefore very similar for both groups, with the key difference being the outcome received and the duration. For both PDD schemes, divertees were given an appointment to meet with a diversion practitioner at a police station voluntarily, usually within a week of the offense. This consisted of a comprehensive assessment using psychological tools, including questions about why they were offending and what might have triggered this. Questioning focused on individuals’ current circumstances (e.g., housing and employment) and a psychological assessment to understand any mental health needs, including whether they had experienced trauma. For Group 1, the outcome of the assessment could lead to referrals to other services that could be made on their behalf during the session. For Group 2, the assessment led to a four-month intervention tailored to the individual's needs, allowing prolonged and more intensive support to access services.
Practitioners reported that both groups required time that was devoted to identifying individual needs. Divertees who could remember the assessment phase of the process reported it as positive and that it was “friendly,” giving examples of what they talked about, including their mental health, home life, relationships, and “how I felt in myself.” One divertee (Callum) remembered it as “basically talking, seeing how I was doing, dealing with things, if I was doing anything else like, or if I was coping with being off drugs, if I needed any more help or assistance.” The in-person sessions enabled practitioners to build rapport with divertees, “to then challenge, explore and unpick” the information disclosed to them during the session. The needs assessment was viewed by practitioners as a vital component of PDD to maximize the benefits to the divertee. Practitioners reported that allowing time for a detailed needs assessment allowed them to take individuals on a “case-by-case” approach, tailoring what they did next.
Force B
The stated aims of Force B's scheme were to break the cycle of drugs and offending and to help people change their lives and behavior. This force worked with an external diversion partner with national reach whose aims were to prevent reoffending and harm through education and training.
Needs assessment by a diversion partner organization was a central component of the pilot of this PDD scheme (analysis of this informed the current scheme). When it was introduced, this was a one-to-one telephone assessment carried out by someone with lived experience and an in-depth knowledge of drugs to “destigmatize and de-police” the offense. The purpose of the assessment was to identify those who needed support and divert them to a specific pathway, including treatment, a diversion course, referral to other services or decide that no further action was necessary. To ensure inequalities were not exacerbated, the scheme was free of charge to the individual. John (Force B, Diversion staff) reflected on the initial model:
One of the things that we really liked with the [pilot diversion scheme] was this ability to triage. So, when people ring us, we can say to them, actually—we have the long conversation with them and then say—actually, it's housing that's your issue or it's mental health services that are your issue. The presenting issue is drug taking or the alcoholism. But actually, you need to sort out your housing first. And having that ability to refer people into other, local services is really, really good.
Although the scheme reported positive health outcomes in its early stage, funding for the triage process was not maintained after the first year. Instead, the scheme moved to a user-paid model where the intervention was determined by the type of drug found and whether the individual had engaged with the scheme for any previous diversions. Force B was the only scheme with a user-paid model. On the whole, divertees did not question this with one individual likening it to paying for a speed awareness course instead of getting points on a driving license. As the diversion had no conditions, there was no follow-up for the divertees who did not comply; this included one individual who told us that they did not have the money to complete the course.
All classes of drugs were eligible, and the scheme was available for adults who agreed to engage with the intervention. For first-time divertees and for individuals who had engaged with previous diversion requirements, police officers referred the individual for a community resolution. Depending on the drug found, the individual was diverted by the police to an online education course for either cannabis only, or to a course which addressed issues associated with all other drugs. Once the divertee had paid the set fee to the diversion partner, they were sent a link to access the e-learning course. Compliance data was returned by the diversion partner to the police force.
If a reoffender did not engage with a previously imposed community resolution for drug possession, they were given a conditional caution. The condition was a requirement for the individual to attend—and engage with—a three-hour online or in-person group education session covering all drug use. The fee was higher than for the e-learning course. The individual could choose which of the national centers to attend for this session or whether to undertake the session online.
The only specific reference to assessment of needs in Force B was noted by a police officer who outlined the process of referring individuals to the multiagency safeguarding hub (MASH) if they were concerned about a divertee's welfare during the initial interaction. This was separate from the force's PDD scheme and might be linked to a specific vulnerability that required immediate attention or a need that would not get picked up through the PDD scheme. This referral was in addition to a referral for diversion. Once diverted, there was no needs assessment stage built into the process for diversion to e-learning or to an in-person or online group session.
Force C
Force C modeled their PDD scheme on the pilot version established by Force B. The stated aims of the scheme were to educate and support individuals to make informed choices about drug use. Eligibility criteria for the scheme include individuals found in possession of any controlled drugs, and/or the cultivation of cannabis, for personal use. The offender must agree that they were responsible for the offense and to engage with the intervention. The diversion was officially reported as a community resolution.
Force C offered diversion interventions free of charge. Their funding model enabled them to keep a triage stage where an individual's needs were assessed during a phone call carried out by the diversion partner. Shaped by this assessment, individuals were then referred to one-to-one treatment, another one-to-one intervention, or to an online facilitated group course for either cannabis or general drug use.
The inclusion of the phone call in Force C enabled the diversion partner to identify individuals for whom the group course would not be suitable, either because of their vulnerability or because they needed treatment. Ross (police staff) emphasized the importance of this stage:
Making sure we’re identifying underlying vulnerabilities and needs and ensuring we’re plugging them in - so very much a social prescribing element to it…and that's why that initial intervention to me is almost the most important part of [the diversion scheme]. Intervention with that individual about their holistic needs, looking at why they use drugs, looking at how it affects them, and ensuring that where it is drifting into that to cope with life, that the most important part of that is working with them to see if extra support can be given, if they want it (Force C).
The nature, duration, and frequency of drug use by those diverted to the group sessions varied widely.
Comparisons Across Forces
The output from the first phase of our research included the production of manuals, which outlined the aims and details of each diversion scheme. Findings were used to update our working theory of change (Stevens & Glasspoole-Bird, 2023). Table 3 maps the elements of each scheme from the first interaction with the police to the exit point and any subsequent follow-up.
Comparison of Diversion Processes Across the Three Focus Forces.
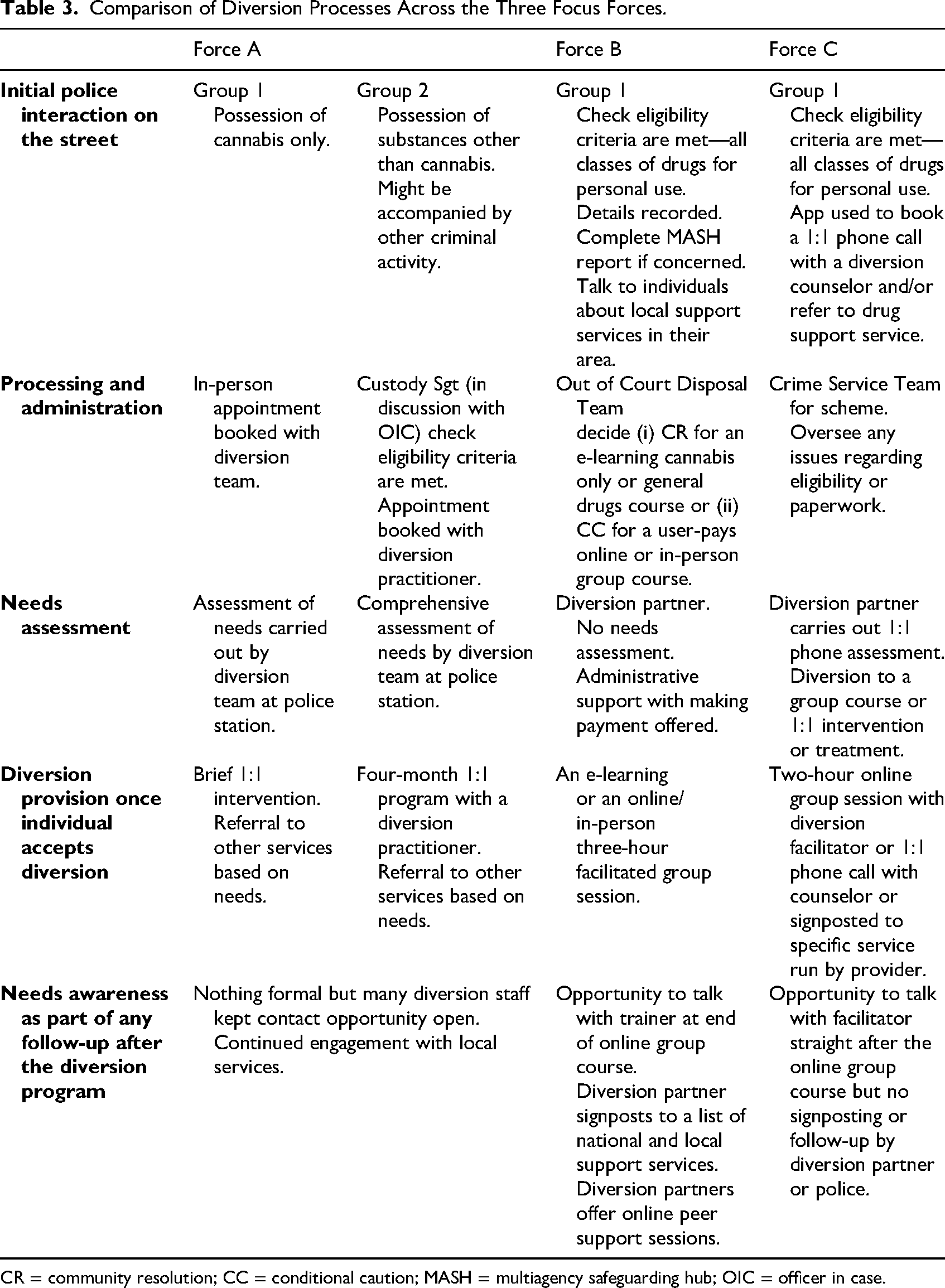
CR = community resolution; CC = conditional caution; MASH = multiagency safeguarding hub; OIC = officer in case.
Shaped by the aims and funding structure, we identified clear differences between the schemes, including whether individual needs were identified and how the flexibility and timing of the intervention supported these needs. It is also important to note that the schemes are not directly comparing like-for-like and that the more comprehensive offering for Force A Group 2 included individuals whose offenses were not solely drug possession or use. All schemes adopted a harm-reduction approach, diverting individuals away from potential harms associated with the CJS and toward opportunities to engage with health-related support.
Flexibility
Although the eligibility criteria were set for each of the three schemes, we found varying degrees of flexibility in the nature and content of the intervention. This included the ways in which the content was designed and communicated to divertees and how it could be adapted to respond to need.
Based on the outcome of the needs assessment process, Force A practitioners could assign Group 1 divertees to receive Group 2 support. Where this occurred, it was reported that it was undertaken voluntarily by the divertee who had expressed a genuine desire to receive the more intensive support of Group 2. This assessment of needs enabled the diversion team to understand an individual's circumstances and how these might trigger, maintain, or exacerbate drug use. Understanding an individual's context led to a tailored four-month intervention. The intervention supported individuals with a referral or handholding to other national or local agencies including: mental health services; NHS Liaison and diversion; drug and alcohol services; housing services; community support groups which include local food banks; Citizens Advice Bureau; local financial support services; Age UK; the Veterans Society; women's charities; sexual health services; support groups for males; and employability organizations. Individuals who were identified as having an addiction (to opiates or crack cocaine) could be referred to medical treatment as part of their intervention.
The intervention for Force B was limited in terms of flexibility as the content was preset. The design of both the e-learning course and the PowerPoint slides for the online or in-person group courses was informed by research and statistical data and included education about the effects of drugs, reducing harm, identifying risks, and legal penalties. During our evaluation, the content of both courses was updated and subsequently accredited by a third party. Interactive tasks were embedded in the e-learning course to promote engagement, but largely the course was passive but informative. Although divertees rated the courses as somewhat useful, their feedback included statements that the course was too generic. Their most frequent criticism was that it was “impersonal,” with “no opportunity to ask questions,” and not aimed at anyone in particular. The limitations of e-learning courses were recognized by the diversion partner. Although the content has since been updated, there was acknowledgment that e-learning lacked engagement and was “not the most impactful.”
The group course offered greater flexibility than the e-learning, as the trainers could respond to comments and questions from the group. A few of the trainers reported that they were not required to cover every slide in the session and could devote more time to topics that engaged a group, which may or may not have been linked to specific needs. One of the trainers explained that the group was “more around having those open and honest conversations, but also looking at the positive behavioral change, and how you can make those changes. So, identifying where the triggers might be.” Some trainers reported that they engaged the group in discussion about their motivations for drug use, which sometimes identified underlying needs.
Although we did not have access to the questions asked during the telephone call in the diversion program for Force C, those identified with substance use disorder were diverted to treatment and one-to-one interventions which were tailored to the individual's needs. Most individuals were diverted to an educational group session which included information about drugs and their effects, using drugs safely and the associated risks.
The content was preset and had been updated to focus mainly on cannabis, as this was the most frequent offense. Although there was no formal signposting to other services, one diversion partner noted that if there is “problematic use coming through,” they “try and support that person to find out what's available locally.”
Timing and Duration of the Intervention
The duration of the intervention varied from about an hour (Force B's e-learning) to two to three hours (Force B's group course) to four months (Force A program for Group 2), thus offering different windows of time to engage the individual, identify needs and provide support. We discuss elsewhere (Sutton et al., 2025) the importance of understanding how an individual's motivation can determine their engagement in a diversion program. This highlights the need to design interventions relevant to the participant's stage of change. Diversion partners across all three schemes questioned whether the intervention was delivered at the right time, expressing doubts about its effectiveness when other aspects of a person's life were unstable.
It is very much a personal journey that the offender has to have the motivation. So, we can provide the support, navigate, but actually if some of the drug users, if they’re not able, they’re not in that position yet where they’re emotionally and physically able to actively take some responsibility, then it may not work. So, it's less about the offense type for me and maybe more about where the offender is on that journey (Catherine, Force A, Police).
Force B and C required divertees to complete the one-off course within a given time frame, regardless of what other issues they might have been facing. The lack of a needs assessment (Force B) and the inclusion of a brief phone call (Force C) did not provide a clear understanding of the individual's relationship with drugs or the frequency or duration of use. This led police and diversion partners to question how effective the intervention would be in terms of cognitive or behavioral change if underlying triggers for drug use were not addressed. This was echoed by many divertees who did not find the course useful and only completed it to avoid more punitive outcomes. The diversion partner for Force B explained that the scheme recognized that many individuals needed more than one attempt to change their thinking and behavior associated with drug use. It also provided multiple opportunities to align the intervention with the “teachable moment” when an individual was ready to reflect honestly on their drug use. Therefore, if the individual was stopped again in Force B and C and met eligibility criteria, they would be offered another opportunity to engage with a PDD intervention.
The group intervention for Force B and C lasted for a maximum of three hours, offering a limited time for group trainers to support change. Although referrals were specifically tailored to individual needs, some of Force A's diversion staff questioned whether all individuals needed the full four months, with one referring to it as “a bit of a stretch.” Adam (Force A, Diversion staff) commented that there could be greater flexibility in the length of the contract:
What we really need is some science behind a prescribing tool, so actually if you come into us with a criminal damage type offense or an assault offense that's fuelled by alcohol, you might only need two months of the work or you might only need one month of work and actually we can make better use of our time with the other three months on somebody else and I think that's a challenge.
The Need for Tailored Interventions to Trigger Change
Across all schemes, we identified how the intervention led to enhanced lives, including positive cognitive or behavioral change associated with drug use for some divertees. Some of these outcomes were not linked to a specific assessment of needs but rather triggered by a different stage of the diversion process. This included the initial interaction with police, the content of e-learning or group courses and peer interaction during group sessions. Depending on the individual's context, the one-off, educative intervention for many Group 1 divertees was a sufficient nudge to trigger change. For many individuals who had been diverted, however, the intervention was not relevant, their reasons for drug use were not identified, and opportunities to support change were missed. In this section, we first present examples of where an initial assessment of needs led to a tailored intervention that triggered change. We then present perceptions of missed opportunities where divertees engaged with the intervention but left the process unchanged, as it was not deemed relevant or helpful.
Positive Outcomes by Recognizing Individual Need
In Force A, we found many examples of how the aim to improve life chances and stop offending had been realized. Divertees recognized the holistic nature of the needs assessment and most accepted that the intervention could be an opportunity for support.
Informed by the initial assessment, many individuals’ needs in Group 2 were met through this tailored scheme. Outcomes included better knowledge and understanding about the effects and harms of drugs, reduction in the amount or frequency of drug use and cessation of drug use. Other outcomes included the prescription of medication for health needs and help managing this. Wider needs were met, including anger management, better self-esteem, help with housing, finding employment, access to financial benefits, and referral to food banks.
In Force B and C, we identified cases of positive change due to the intervention providing a nudge to action. This included reduced, safer, or no further drug use. As a result of this, some individuals commented that their lives were more ordered, their children attended school more regularly, and they could better hold down a job.
We also identified opportunities in Force B and C's intervention where an individual's needs could be noticed or expressed through opportunities offered for further support. At the end of the online or in-person sessions, trainers made themselves available to speak with divertees. Although it was time-limited and not private, it was an opportunity for people to ask specific questions or explore further support with someone they had begun to build a relationship with.
When divertees had completed Force B's e-learning course or group session, they were provided with information about local drug support services, which signposted them to more tailored support. During our evaluation, the drug diversion partner began to contact these local services to consider whether a direct referral could be made for divertees who did not feel confident or motivated to self-refer. The diversion partner also introduced facilitated, online peer-support groups for divertees. Recognizing that the e-learning or group courses might have helped individuals to begin to engage with their drug use, the peer support offered a voluntary next step with an organization they had already connected with, and that was separate from any police diversion requirements. Several individuals had started to attend these sessions.
These interventions contributed to the scheme's aims of “helping people change their lives and behavior” (Force B) and “supporting individuals to make informed choices about drug use” (Force C).
Missed Opportunities due to the Lack of a Needs Assessment
Police and diversion staff identified how schemes could be enhanced to better meet needs. Interviews with those diverted to e-learning or group sessions provided insight into their circumstances, the extent to which they found the intervention relevant and what they would have included in the intervention if given the opportunity.
When Force C's telephone assessment identified individuals with complex needs and addiction, they were diverted to treatment and other tailored interventions. Some trainers in Force B commented that greater screening was required before being diverted to a group session, as people were turning up who “should never have been put on that course.” Trainers reported “addicts,” “dealers,” and “a guy – it was quite obvious he was withdrawing from heroin,” had turned up to their sessions. As the needs of the individuals in the group were diverse, and as the content was generic, the scheme lacked any targeted support for those with vulnerabilities and more complex issues.
Beth, a police officer in Force B, recognized that the diversion was a limited tool, “We can send this one on a drugs diversion course. If they’ve got a real problem, that's not going to help them do anything.” This was echoed by Jesse, a divertee, who said: “It's an addiction isn't it? So, it's hard to, like, stop an addiction based on just going for a course.”
Through our interviews with divertees, we found that some individuals were using controlled drugs for reasons associated with different underlying needs. These included specific situational factors, self-diagnosis, and wider personal circumstances. Situational factors included smoking cannabis to fit in with certain friends or at specific events such as football matches, with one divertee from Force B claiming that he only used drugs when there. He completed the e-learning course, which did not provide any help with managing the triggers associated with his use.
Self-diagnosis included cocaine use to manage neurodiversity, with autism named by several divertees from all schemes. There was also a reference to cannabis use to help with Attention Deficit Hyperactivity Disorder (ADHD) and mental health difficulties, such as anxiety, for example, to “just calm myself down.” Divertees reported that using drugs helped to alleviate symptoms and “made life better.” Some felt they had no other options to get help while on a long waiting list to see specialists to get an official diagnosis. Stacey, who had been self-medicating for undiagnosed chronic ADHD, commented that:
There's no hint or suspicion or nothing about the course was aimed at somebody like me… I found it sort of very lacking in that area…if I were pointed toward some help that was specific to me, then then you know that's certainly something that I probably would have engaged in at the time (Force B, Divertee).
Given the complexity of needs and the potential vulnerability of some divertees, staff across all schemes recognized the limitation of one-off e-learning or group courses, which “isn’t going to touch the sides.” Aaron, a trainer from Force B, explained that “I don't expect that I'm going to change their life as they walk away from that course.” Similarly, a police officer from Force C reflected that “while I appreciate something is better than nothing, I can understand why these places are out there, but for us, giving [an out of court diversion for a group session] to a certain person is never going to have an effect.” Some police and diversion staff expressed frustration that, although eligible for the scheme, it was not set up to help those divertees with more complex issues.
Wider personal circumstances were recognized by police and diversion staff across all three schemes as factors closely linked to drug use. Some divertees required support with other issues that were maintaining or exacerbating their drug use, noted by Force C's diversion staff as needing to get “support to those root causes,” in order to make a difference. Specific named issues by police, diversion staff, or divertees included: domestic abuse, alcoholism, exploitation (including control and “cuckooing”), poverty, grief, unemployment, neurodiversity, broken relationships and separation from children. An increase of mental health issues, more complex needs, and chaotic housing or homelessness were the most commonly mentioned. Diversion staff spoke of the need to “understand people's stories” and the trauma they have experienced, whether from childhood or linked to more recent events. They referred to the need for trauma-informed approaches throughout the diversion process.
Police and diversion staff agreed that for some individuals, a needs assessment could be very effective when tailoring support. John (Force B diversion staff) identified the triage stage in the current scheme as “the bit that's been missing.” The needs assessment would inform which specialist services the individual might benefit from. This was an integral part of Force A's design. Particularly for those with complex needs, police and diversion staff from Force B and C talked about the need for practical holistic support that extended beyond what could be offered by the diversion course. This included housing, education, employment, and access to food banks and other help. Some of the police involved in shaping Force B's diversion policy aimed to bring back a needs assessment to tailor the intervention to the individual; however, funding for this had not been agreed.
Toward the end of the Force A Group 2 intervention, PDD practitioners could choose to re-take the needs assessment paperwork as a means to measure the impact of PDD, primarily as a method for divertees to appreciate the positive outcomes they had achieved through undertaking the scheme. Practitioners did report, however, that due to the duration of Group 2, it was sometimes challenging for them to “wean” their intensive support away from the divertee.
Some divertees chose to keep in touch with their diversion provider after the intervention had ended, and many continued to engage with local services. Although several divertees reported that they wanted no further contact, some felt that contact by their practitioner would have been helpful to maintain change, especially for those who had begun to rely on their relationship with diversion staff for support, accountability, and encouragement:
Once you’ve completed the program, it ends quite abruptly. I think maybe if they were to potentially give a check-up maybe for the first month and then potentially three months down the line just another check-up, see how you’re doing, I think that could benefit a lot of people (Bradley, Force A Group 2, divertee).
This missed opportunity for support was echoed by many divertees in Force B who reported that they would have welcomed some form of follow-up after completing the intervention to provide ongoing support and to help sustain behavioral changes. Force B's diversion staff also recognized that meaningful follow-up after the diversion could be beneficial. Ideas included phone calls, sending information, and an additional intervention after a number of months. Key to all suggestions was having, “somebody there who could actually have that real conversation with them,” highlighting the limitations of existing provision.
The potential impact of missed opportunities to understand an individual's drug-related health and welfare issues highlights the value of a needs assessment in the intervention process.
Discussion
Suitability of Needs Assessment
The suitability and role of needs assessments in PDD schemes emerge as central to both the effectiveness and ethical foundations of the intervention. A critical question is whether the inclusion of an assessment of needs is necessary to meet the aims of the diversion scheme. For many individuals diverted to Force B and C's group interventions, the educational content, interaction with diversion partners, or the initial shock of being caught by police was enough of a nudge to trigger change. The rationale for a comprehensive assessment is therefore less compelling; a brief, light-touch educational intervention may be sufficient to prompt behavior change (De Viggiani, 2022), and in such cases, expending resources on holistic assessments may be unnecessary.
However, when the stated aim is to improve the life chances of those who participate through providing information and support to access a wide range of rehabilitative diversionary, educational or intervention activities in the local community (Force A), or to support individuals in changing their lives and addressing patterns of drug use (Force B), a needs assessment becomes not only relevant but essential for those with problematic drug use, vulnerabilities, and ongoing complex situations. Missed opportunities to identify and tailor support included the one-size-fits-all e-learning and group content, lack of trusted relationship building, limited opportunities for an individual to shape the support they needed, no follow-up, a lack of holistic care, and too much emphasis on an individual's drug use, which was often a symptom, rather than a cause, of other issues. Without understanding the social, psychological, and structural factors underpinning drug use, interventions lack the tailored response to trigger change (Clifasefi et al., 2017; Collins et al., 2015a).
Ethical concerns further complicate the landscape. Diverting vulnerable individuals—many of whom experience multiple forms of disadvantage—into schemes without offering appropriate support raises questions about the justice and integrity of such interventions. If diversion schemes are designed primarily to avoid harm associated with criminal sanctions, a needs assessment may not be required. However, when schemes claim to address drug-related harms and improve lives, the absence of assessment and support may result in missed opportunities and unintended harms. While some divertees do experience positive outcomes without formal assessment, our findings indicate that many fall through the cracks, particularly in Forces B and C. This is further exacerbated for divertees in Force B if they cannot afford to engage with the user-pays model. Spooner et al. (2001) cautioned that by using discretion to divert people at the earliest stage, officers might inadvertently deny them access to services that would otherwise be available later in the justice process. Some participants may, therefore, receive more thorough support if processed through the traditional CJS (Dickson-Gomez et al., 2022). If needs are not assessed, police and diversion partners cannot know who may benefit from further support or tailored intervention. Conversely, it could be argued that such health and social needs should be identified and met by health and social services, not the police.
Our findings emphasize the importance of finding a tool to promote the effectiveness and cost-efficiency of matching intervention to need (Marlowe et al., 2011). To avoid under- or over-treatment and missed opportunities, further evaluation of the nature of a screening, triage, or needs assessment stage is required to identify how the aims of PDD can be met while promoting criminal justice and public health priorities.
Challenges for Needs Assessments
Our evaluation identified several challenges for the assessment of individual needs, including who carries this out and where, how it is funded, and the depth required to support the aims of the diversion scheme. The complexity of individual contexts and motivation interacting with the diversion process is threaded through the results and discussion. For some divertees, no assessment of needs was necessary to trigger positive change (see our wider findings on divertee motivation to change; Sutton et al., 2025). There were multiple opportunities throughout the diversion process for some form of needs assessment for those who did not benefit from the “one size fits all” intervention. In the absence of an assessment in Force B and C, it is not clear from our findings which of the opportunities for needs assessment (see Table 3) would best suit an individual's readiness to reflect on their drug use and the possible underlying causes or situational factors that maintain this. Challenges concerning funding, data sharing, and capacity for multiagency working are addressed in our paper which demonstrates how partnership is both a necessary condition and a contingent cause of effective practice in PDD (Smith et al., 2025). Here, we identify two challenges that emerged from our findings on the purpose and effectiveness of assessing individual needs: balancing health and criminal justice issues, and individual autonomy.
Balancing Health and Criminal Justice Issues
Determining the police's proportionate response to drug-related offenses involves navigating the complex intersection between criminal justice objectives and public health imperatives. We identified how diversion schemes offer a mechanism through which this balance can be struck, particularly where the aim is framed around harm reduction, education, and promoting informed choices.
A key challenge lies in understanding the function and value of the needs assessment stage. While often presented as a gateway to identifying support needs, the purpose of this assessment is not always clearly articulated or consistently applied. Some schemes lack a clear rationale for when and why a needs assessment is conducted (or not conducted), raising concerns about whether such assessments are effectively supporting the wider aims of police-led diversion. This raises questions about who is best placed to carry out the assessment and oversee subsequent tailored support—especially given the limited resources of publicly funded multiagency partnerships.
Although one of the commonly stated benefits of police-led diversion is the avoidance of harm associated with formal criminal justice processing—such as criminalization, stigma, or disruption to employment or housing (Bacon & Spicer, 2023; Spyt & Kew, 2023)—we found that interventions undertaken by Group 1 divertees provided limited support to address physical or mental health needs. The effectiveness of diversion in improving health outcomes is largely contingent on whether the individual is supported to access appropriate support (Clifasefi et al., 2017). This highlights the need for police officers to fully understand the vision of the scheme and how their actions contribute to broader health and social outcomes, even if they are not directly responsible for providing the intervention. Our inclusion of focus groups with police and diversion partners gave us insight into differing perceptions and tensions between the schemes’ aims and operational challenges.
The delivery of needs assessments by nonpolice actors, such as health or social care professionals, can also influence how these are received. In Force A, for instance, needs assessments conducted within the police station context were sometimes perceived as punitive rather than supportive, underlining the significance of how and by whom such assessments are delivered. It is also critical to recognize that not all individuals who use drugs require treatment. As identified in Marlowe et al.’s (2011) study, many people use substances recreationally or in a controlled manner without meeting criteria for dependency. Yet, a better-matched intervention based on assessed needs could be vital for those at risk of escalation—whether in the severity of their drug use or in associated criminal behavior. This could play an important preventative role in reducing the “revolving door” effect, where individuals cycle through low-level criminal justice interactions without addressing underlying issues.
Individual Autonomy
The role of individual autonomy emerged through our evaluation as an important aspect of diversion—both ethically and practically. Central to this is the importance of giving individuals a voice in the process—particularly in relation to how their needs are assessed, when their needs are assessed, how interventions are designed, and how they engage with subsequent support (Åkerblom & Ness, 2023; Madden et al., 2020). We found that those diverted to the intervention in Force A had some say in which services they were referred to, although they could not determine the duration of the intervention, as this was set at four months.
Schemes that impose a binary choice—participate in the intervention or face criminal charges—raise significant ethical concerns (Bacon, 2024), particularly when diversion away from criminalization means diversion away from support available in custody and when diversion interventions incur financial costs, as in Force B. Funding models across the schemes emphasize difference in police priorities. A user-paid model (Force B), particularly for vulnerable divertees, could be considered as unfair and regressive, placing financial burdens on those least able to bear them, thereby exacerbating existing social and economic inequalities. Charging for support can deter individuals from seeking help, undermining intervention aims and potentially increasing long-term harm and public costs. It also raises ethical concerns where user-pays diversion interventions are the only alternative option to criminal sanctions. For many participants, the program content was viewed as irrelevant, and many individuals did not see the value or relevance of the intervention. While given an apparent choice to avoid the CJS, there was only one option, and they had no voice in the nature of the intervention that they were required to engage with. This potential for coercion risks undermining both the legitimacy of the scheme and the individual's motivation to engage in a meaningful way.
Outcomes appeared to be more positive when divertees interacted with a supportive and responsive facilitator—someone who not only listened and contextualized the experience but also held individuals accountable. This suggests that autonomy does not simply mean having choices but being engaged in a relational process where support was personalized and responsive. Force B relied heavily on e-learning (for first-time divertees and for previously compliant repeat divertees) and lacked a human connection. The absence of interpersonal engagement may significantly reduce the impact of the intervention, particularly for individuals facing complex or entrenched challenges.
We question the extent to which individuals could be involved in the assessment of their own needs at a relevant point in the process and in the co-design of their intervention pathway aligned with their sense of readiness. This approach emphasizes that a needs assessment should not be a one-off process “done to” the individual. It highlights the importance of “teachable moments”—periods of heightened receptivity to change that may follow significant life events or encounters with the CJS (Graham et al., 2019; McDaniel et al., 2024). Embedding individual autonomy into the diversion process—through tailored support, relational accountability, and the opportunity for self-directed engagement—may better align interventions with the underlying social and emotional drivers of drug use and ultimately enhance outcomes. We suggest this is particularly important for those with disadvantages, complex needs, vulnerabilities, and experience of trauma.
Conclusion
This study highlights the potential of PDD to foster meaningful change among some individuals who use drugs, even in the absence of formal needs assessments. Across all models, we found that some divertees made cognitive and behavioral shifts triggered by relatively low-intensity interventions, including initial police contact and peer or facilitator interactions. In each scheme, there were multiple points where support was offered with varying degrees of signposting and handholding. These findings emphasize the potential for diversion to act as a critical intervention point, particularly for those who were self-motivated and whose lives were relatively stable.
However, the absence of an assessment of needs at any point in the process, lack of tailored interventions, and limited or no individual autonomy in the process, reflect missed opportunities to identify and address complex needs and vulnerabilities that may perpetuate or intensify drug-related harms. Realizing the broader harm-reduction goals of PDD schemes depends on ensuring that all individuals are meaningfully supported to access health and social services if required. Central to this is the need for targeted, evaluated, affordable, and needs-responsive approaches, embedded in robust multiagency partnerships which have adequate capacity. Promoting individual autonomy as part of diversion practice strengthens engagement, enhances the legitimacy of interventions, and aligns personalized support with the lived realities and motivations of those it seeks to assist.
These findings raise critical questions concerning the appropriate scope of police responsibilities—particularly in relation to the allocation of time and resources—and the extent to which law enforcement agencies can reasonably be expected to deliver improved health and social outcomes that extend beyond mitigating harms directly associated with involvement in the CJS. We propose that future design and evaluation of PDD schemes developed in partnership with external services should prioritize greater conceptual and operational clarity. In particular, attention should be directed toward: refining the purpose, timing, effectiveness, and funding of needs assessments; ensuring the appropriate tailoring of interventions; and systematically identifying service gaps. Such an approach would strengthen both individual-level outcomes and the broader system-level impact on crime reduction and public health improvement.
Footnotes
Acknowledgments
The authors gratefully acknowledge the support of the User Voice research team in carrying out interviews and focus groups with people who were eligible for diversion. Thanks also go to the wider PDD team for their contributions to the project and for reading earlier drafts of this article. For the purpose of open access, the authors have applied a Creative Commons Attribution (CC BY) license to any Author Accepted Manuscript version arising from this submission.
ORCID iDs
Ethical Considerations
This research received ethical approval from the University of Kent Staff Review Committee (REF0780b) on 07/03/2023 and abides by the University of Kent Ethics Code.
Consent to Participate
Informed consent was obtained from all research participants in writing, where data was collected in-person. Informed consent was verbally obtained and documented at the commencement of each audio-recorded telephone interview, in accordance with approved ethical protocols.
Consent for Publication
All individual data has been anonymized. Participants were aware of the intention to submit when they gave their consent to participate.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Evaluation Accelerator Fund—Cabinet Office [award number EAF-COP-PDD, scheme number: G2-SCH-2022-07-11481].
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that supported this article are not publicly available because they contained information that could compromise the privacy of research participants and forces.