
Abstract
The rising demand for substance-related treatments results in a persistent increase in human, social, health, and economic costs that affect not only people but also reverberates across families, communities, and societies. Social environment plays a crucial role in substance use as it influences recovery pathways either by fostering drug-free behaviors or hindering them. This review aims to synthesize existing scientific evidence on the social-environmental factors that influence recovery from substance use disorders, excluding alcohol and tobacco. Following the methodological framework proposed by Arksey and O’Malley and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews, a comprehensive search was conducted in 19 databases and other sources from inception to 2024. Forty-five studies met the inclusion criteria. A multitude of social-environmental factors were shown to influence recovery such as support networks, socioeconomic conditions (i.e., housing, education, employment), spirituality, drug availability in the substance milieu, stigmatization, and the therapeutic setting. The various support networks play a key role in facilitating recovery pathways, with dysfunctional relationships and substance availability hindering recovery progress. Factors that appear to play a protective role under some circumstances could also prove to be risk factors generating feelings of loneliness and alienation. A general lack of evidence directed at post-treatment integration failed to allow an exploration of results akin to other factors. This review highlights that not a single solution appears to apply to everyone's recovery, and continued disregard for varying intersectionalities could result in the support provided being subpar to what is expected by the person involved in a change process. Therapeutic approaches to recovery should seek to be holistic and inclusive of every network by recognizing and mitigating the systemic barriers that surround those in a process of change as a means to sustain treatment's success and facilitate post-treatment integration.
Introduction
Worldwide, most substance use disorders are associated with cannabis and opioids, with an approximate estimate of 228 million cannabis and 60 million opioid users in 2024 (United Nations Office on Drugs and Crime, 2024). The recurrence and rising number of people who use substances result in increasing human, social, health, and economic costs, escalating demands for specialized healthcare and rehabilitation services (Cartwright, 2008; Peacock et al., 2018).
Substance use disorders (SUD) can be characterized not only by cognitive, behavioral, or physiological features, but also by their contextual and dynamic nature, driven by intense activation of the reward system, where drug use continues despite possible negative consequences (American Psychological Association, 2015). Concurrently, standardized diagnostic thresholds for SUD are comparatively low and polythetic, where in the Diagnostic and Statistical Manual of Mental Disorders, 5th Edition (DSM-5) “substance abuse” requires 2 of 11 criteria, thus risking diagnostic “bracket creep” by conflating heterogeneous practices into a single disorder category (Race et al., 2025). Moreover, several items, namely risky use, failure to fulfil major role obligations, or withdrawal from family activities, are normative and can re-individualize what may be contextual dynamics, recommending greater specificity with respect to substance-setting-function when interpreting SUD prevalence (Race et al., 2025). Other perspectives view SUD as a response to life conditions, impacting individuals physically, emotionally, and relationally (Rothschild, 2010; Tatarsky & Marlatt, 2010), with effects rippling through families, communities, and societies (Daley, 2013).
The 2024 European Drug Report states that the impact of illicit drugs is seen almost everywhere in society, as nearly everything with psychoactive properties has the potential to be used as a drug, and everyone, directly or indirectly, can be affected by illicit drug use (European Monitoring Centre for Drugs and Drug Addiction [EMCDDA], 2024). This may lead to increased rates of social vulnerabilities and healthcare burdens, which often intertwine with societal challenges such as systemic inequities that exacerbate the complexity of recovery (Daley, 2013), highlighting the need for different solutions, better policies, and best practices (European Commission: Directorate General for Justice, Freedom and Security et al., 2009). More broadly, methodological critiques caution that when frameworks linking stress and health disparities are translated into standardized clinical routines, they can unintentionally shift attention away from structural causes of harm and reinforce individual-level explanations. This highlights the need to include broader environmental perspectives, such as the socioecological model and Rhodes’ risk environment (Rhodes, 2002), to better capture the structural and contextual dimensions of risk and recovery.
Socioecological Approach to Substance Use and Recovery
The social environment includes the groups we belong to, the neighborhoods we live in, our workplaces, the policies we create to organize our lives (Yen & Syme, 1999), and the experience of substance use is deeply engraved in this environment (Spooner & Hetherington, 2005). A diverse set of factors in the social environment is indeed responsible for encouraging or discouraging drug use, not in a deterministic, but rather in a probabilistic manner (Thomas, 2007). Thus, approaching drug use recovery through a socioecological lens allows one to seamlessly move through the ecological dimensions that may influence recovery pathways.
Building on ecological systems theory and social epidemiology, the socioecological model synthesizes intrapersonal, interpersonal, community/organizational, and societal/policy determinants that jointly shape risk, treatment access, and recovery trajectories (Witkiewitz & Tucker, 2024). Intrapersonal factors include determinants that influence exposure to substances, initiation, treatment engagement, and relapse risk over time. Factors like sociodemographic are dynamic and often bidirectional, such as financial strain posing as both cause and consequence, underscoring the need to look at these dimensions across time rather than as static covariates. At the interpersonal level, family, peers, and recovery networks may provide reinforcement and meaning that can either hinder or accelerate engagement and sustain recovery (Davis et al., 2016). Nonetheless, maintaining affiliation with drug-using networks may result in substance involvement and delays in treatment entry (Davis et al., 2016). At the community level, we encounter formal support settings that configure access, intensity, continuity, and cultural responsiveness of care. Within a socioecological approach, the organizational policies, healthcare professionals, and other dimensions of this support mediate interpersonal processes and individual change (Vest et al., 2023). Lastly, at the societal level, the regulatory frameworks, stigma cultures, and macroeconomic conditions may structure the availability and quality of formal support and the distribution of risk (Jalali et al., 2020). Socioecological analyses of the opioid crisis make clear that macro-level shifts reshape local overdose risk and the effectiveness of downstream interventions; as single-component strategies are insufficient absent integrated policy action (Jalali et al., 2020).
Consistent with social stress traditions, Meyer's Minority Stress Theory explains inequalities among stigmatized populations as arising from excess exposure to stressors that are social in origin, additive to general life stress. It distinguishes distal stressors (e.g., discriminatory policies, prejudicial events, structural disadvantages) from proximal stress processes (e.g., expectations of rejection, identity concealment, internalized stigma), with coping and community resources moderating these effects (Meyer, 1995). This distal-proximal architecture maps onto socioecological levels, and its premises generalize to several minoritized statuses when stressors are produced by institutions and cultures rather than individual pathology (Frost & Meyer, 2023; Meyer, 1995). Although the Minority Stress Theory has been criticized for its overemphasis on stigma and stress pathways, and neglect for cultural, identity-based, and community mechanisms of disinhibition and agency (Race et al., 2025), this theory remains useful to explain SUD across diverse populations, as long as its findings are interpreted through community-level dynamics, cultural meaning, identity affirmation, and collective agency lenses.
Rhodes’ risk environment framework offers another operational framework for locating drug-related harm in the patterned relations between people and context rather than in individual choice alone (Rhodes, 2002). Risk environment is defined as the social or physical space in which multiple factors interact to increase the probability of harm and posits it as a crossing between types of environments (physical, social, economic, policy), levels of environmental influence (micro, macro), and mechanisms of environmental influence (susceptibility and vulnerability) (Rhodes, 2002). By shifting the unit and locus of responsibility from individuals to environments and institutions, the framework both critiques the limits of individualistic behavior-change models and names the structural levers through which harms are produced and reduced, including the creation of what are defined as “enabling environments” (Rhodes, 2002). In practical terms, adopting the risk environment within a socioecological approach directs evaluation and action beyond “risk factors” toward “enabling environments,” removing constraints and building protections across levels so that individual motivation can translate into sustained recovery. (Rhodes, 2002; Rhodes, 2009).
Some patterns tend to be simple and direct in the manner through which they exert their influence, though the interactions between the different levels increase the complexity and the range of pathways that may be involved. As such, the different social interactions that can influence recovery might also foster and reinforce drug-free behaviors, or pose as mechanisms of control that might hinder recovery (Randle et al., 2014). The individual is neither fully autonomous nor passively shaped by external forces but actively engages in constructing meaning and behavior through social participation (Adom et al., 2016). People with SUD do not merely adapt to preexisting social realities but actively co-construct them through interaction and participation in social contexts (Vigdal et al., 2022), which underscores the dynamic and reciprocal relationship between individuals and their social environments. Thus, the patterns of substance use are not solely personal or biologically driven but embedded within and shaped by the meanings, norms, and behaviors prevalent in social groups (Burrel, 1999; Rhodes, 2002; Rhodes, 2009).
Recovery: Contested Meanings and Plural Pathways
The concept of recovery in substance use research has undergone a profound historical transformation. In its earliest framings during the mid-twentieth century, recovery was heavily influenced by the rise of Alcoholics Anonymous and other 12-step traditions, where abstinence was the defining criterion and spirituality was foregrounded as the path to change (Laudet, 2007; Witkiewitz & Tucker, 2024). In clinical and psychiatric settings, recovery was further tied to rehabilitation programs and institutional treatment, reinforcing a biomedical model that equated recovery with the cessation of substance use, successful treatment completion, and reintegration into socially sanctioned roles (Laudet, 2007). While useful for structuring treatment systems, this narrow understanding failed to capture the complexity of lived experiences and the broader processes of personal growth and social reintegration (Inanlou et al., 2020).
By the 1980s and 1990s, psychiatric rehabilitation and the mental health recovery movement began to challenge these biomedical framings, emphasizing person-centered care, empowerment, and quality of life as central components of recovery (Inanlou et al., 2020). Later, the introduction of the concept of recovery capital expanded this shift further, underlining the role of social, cultural, and community resources in enabling sustainable long-term recovery (Cloud & Granfield, 2008). These developments illustrate that recovery has never been static, but instead a contested and evolving construct that reflects the priorities of different historical moments.
Despite these advances, no consensual definition of recovery has emerged. Professionals continue to hold divergent views regarding whether abstinence or sobriety should be considered a necessary criterion and how recovery should be measured, indicating that the concept remains under debate (Cloud & Granfield, 2008; Inanlou et al., 2020).
More recent perspectives have positioned recovery as a dynamic and multifaceted process. This reconceptualization emphasizes not only behavioral change but also psychological resilience, social connectedness, and spiritual well-being, alongside broader improvements in quality of life (Laudet, 2007). Importantly, when the perspectives of people who use drugs are included, recovery is often described as a process of becoming one's “true self” or achieving personal potential (Tiburcio & Baker, 2023). Such perspectives resist externally imposed definitions and highlight the plurality of recovery experiences. This historical trajectory reflects a paradigmatic shift toward holistic and multidimensional frameworks that accommodate diverse pathways (Cloud & Granfield, 2008; Inanlou et al., 2020).
The constructivist paradigm offers a particularly valuable lens for interpreting these developments (Adom et al., 2016; Puddy & Wilkins, 2011; White, 2008). Constructivism emphasizes that recovery is always situated within specific social, cultural, and structural contexts. It rejects universalist definitions and instead situates recovery as a subjective and contextualized process, co-constructed through lived experience and narrative. By privileging personal perspectives and acknowledging structural constraints, constructivism aligns with contemporary approaches that frame recovery as plural, situated, and deeply contextual (Adom et al., 2016; El-Guebaly, 2012)
A concept analysis further clarifies four defining attributes of recovery (Brophy et al., 2023). First, recovery is non-linear, often involving relapse, which can be reframed as an element of growth rather than failure (Brophy et al., 2023). Second, recovery is more than regulating substance use, since a sole focus on consumption neglects the structural factors—such as poverty, stigma, and discrimination—that perpetuate harm. Third, recovery is holistic, encompassing improvements across mental, physical, emotional, spiritual, and social domains, where supportive networks play a protective role. Finally, recovery is person-centered, meaning that individuals themselves define their recovery targets, whether abstinence or broader personal change (Brophy et al., 2023).
It is also important to acknowledge that recovery does not exhaust the continuum of care for substance use disorders. Broader systems of care may involve processes that extend beyond recovery, reflecting the diversity of individual needs (Puddy & Wilkins, 2011; White, 2008).
Reintegration, though overlapping with recovery, may encompass distinct elements. The European Monitoring Centre for Drugs and Drug Addiction (EMCDDA) identifies three pillars: housing, education, and employment (Dale-Perera, 2017), along with supportive networks and freedom from stigma. Integration after leaving treatment supports recovery by fostering human, social, economic, and institutional capital, promoting social integration (Brophy et al., 2023). It aims to enhance health, wellness, and self-directed lives (Tiburcio & Baker, 2023), focusing on relationships, identity reshaping, substance use understanding, boundaries, and emotional regulation (Flora, 2023).
Understanding SUD requires engagement with both positivist and constructivist foundations. A positivist perspective, grounded in the notion that reality can be systematically observed and measured, provides the basis for mapping socioenvironmental determinants such as housing, employment, and education, which are essential to a scoping review analysis. Yet recovery extends beyond linear or quantifiable outcomes. From a constructivist standpoint, it is recognized as a socially embedded and individually constructed process, in which meaning is shaped through cultural and interpersonal contexts (Berger & Luckmann, 1967). This perspective situates recovery not merely as the cessation of substance use, but as a dynamic, person-centered trajectory defined by identity reconstruction, agency, and lived social experience.
Aims and Objectives
Previous efforts have provided a comprehensive overview regarding the role played by socioenvironmental factors in SUD recovery, providing relevant insights from qualitative evidence (Vigdal et al., 2022) or observational data (Johannessen et al., 2019), with literature signaling an influence from social factors in recovery, specifically directed at alcohol (Bryden et al., 2013; Groh et al., 2008; Kelly et al., 2009) and tobacco (Al-Qashoti et al., 2022; Obieche et al., 2021; Shruti et al., 2017). However, these overlook the challenges of drugs deemed illegal or illicit at the community and societal levels, as the type of substance has a differential effect on the likelihood of recovery (Cunningham et al., 1993).
Considering the multifaceted nature of SUD and the substantial impact of social surroundings on recovery (EMCCDA, 2022; Galea et al., 2004), this scoping review aims to map the socioenvironmental factors that contribute to recovery of people with SUD, other than alcohol and/or tobacco, by answering: “Which socioenvironmental factors can be associated with the recovery of people with SUD?”. We aim to provide a comprehensive overview that enriches the current understanding of recovery beyond the individual level and highlights areas for future research and intervention to address knowledge gaps and improve outcomes for people with SUD.
Method
This review follows the methodological framework proposed by Arksey and O’Malley. (2005) and reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (Tricco et al., 2018). According to the methodology that underpins the process of a scoping review, this methodological approach guarantees transparency and rigor in the scoping process thus divided into five stages: (1) identification of the research questions; (2) identification of relevant studies; (3) study selection; (4) data charting, and (5) collating, summarizing and reporting of the results (Arksey & O’Malley, 2005).
Identifying Relevant Studies
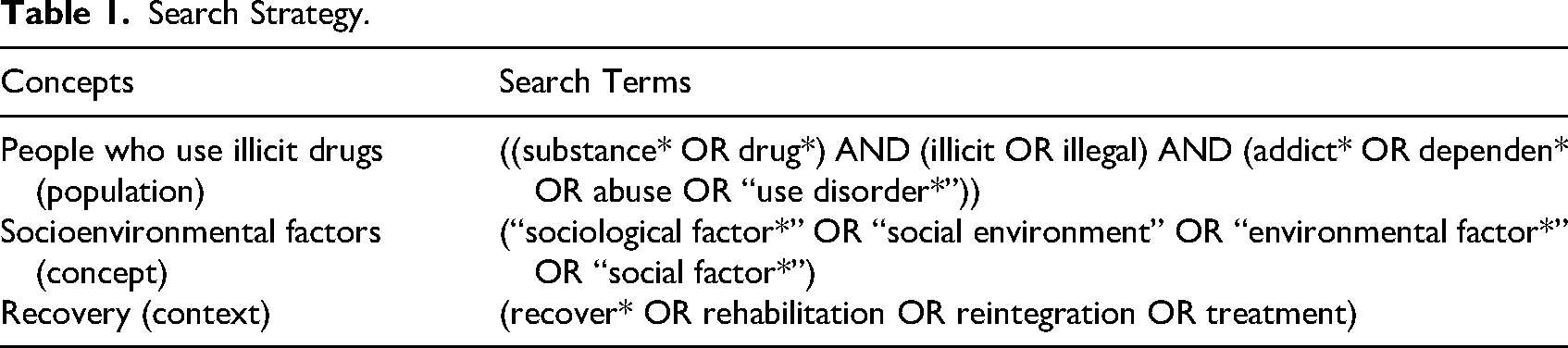
A preliminary search was conducted in Medline and APA PsycInfo (via EBSCO) to assess terminology and keywords most commonly used in this topic. The final search strategy (see Table 1), upon agreement by all authors, was introduced in nineteen electronic databases and other sources, including gray literature repositories (see Appendix 1), from inception to February 2024. This search strategy comprised an arrangement of terminology associated with substance use disorders, socioenvironmental factors, and recovery.
Search Strategy.
Eligibility Criteria
The eligible population was defined as people with SUD, problematic use, addiction, or dependency on one or more substances, other than alcohol and/or tobacco. Inclusion criteria stipulated the absence of psychiatric or somatic comorbidities to mitigate potential confounding. Participants were not to belong to highly specific subpopulations, such as pregnant women or people with mental disorders, as this would pose challenges in discerning the influence of the social environment beyond existing intersectionalities. The key concept was the socioenvironmental factors, including social environment and its specific dimensions, for people on a pathway to recovery, excluding processes of spontaneous or “natural” recovery, as they occur without treatment or support groups (Burman, 1997).
In this review, we chose to include only studies addressing recovery from the use of illicit substances. This decision reflects the substantial differences in social acceptance, legal regulation, and structural conditions between illicit drugs and legal substances such as alcohol and tobacco. For example, research consistently shows that dependence on illicit substances is associated with significantly higher levels of stigma, both at the public and structural levels, compared to alcohol and use disorders and tobacco use (Corrigan et al., 2009; Room, 2005). The criminalization of drug use generates barriers to healthcare, employment, housing, and social reintegration and other structures, all of which critically shape recovery trajectories (Csete et al., 2016). In contrast, alcohol and tobacco consumption are embedded in culturally normative practices, with legal frameworks and social networks that generally facilitate greater acceptance and more accessible recovery pathways (Room, 2005). Including alcohol and tobacco alongside illicit substances would therefore risk conflating contexts with fundamentally different socioenvironmental dynamics. Recovery from illicit drug use is particularly conditioned by punitive policies, stigma, and marginalization, while alcohol and tobacco use disorders operate within systems that more readily provide social legitimacy and medicalized responses (Room, 2005; Yang et al., 2017).
Broader inclusion criteria were determined for publication type and study design, which allowed the inclusion of dissertations, gray literature, and policy papers, with diverse study designs, including qualitative, quantitative, or mixed-methods. Reviews were preserved for citation searching. No restrictions were placed on the geographical location, timing of the intervention, language, or based on participants’ gender or ethnicity.
Screening Approach
Records were imported into EndNote for organization. The screening process was carried out in three stages. Firstly, duplicates were removed using EndNote software. Next, text and abstracts were screened, followed by a full text review, both conducted independently by two reviewers (João Pedro Ramos and Mariana Vieira) with the assistance of a literature review software (DistillerSR). In case of disagreements, a senior researcher (Marta Pinto) was consulted to resolve them. Backwards and forward citation searching was conducted on included studies through Google Scholar, PubMed, and Web of Science Core Collection (via Clarivate).
Collating, Summarizing, and Reporting the Results
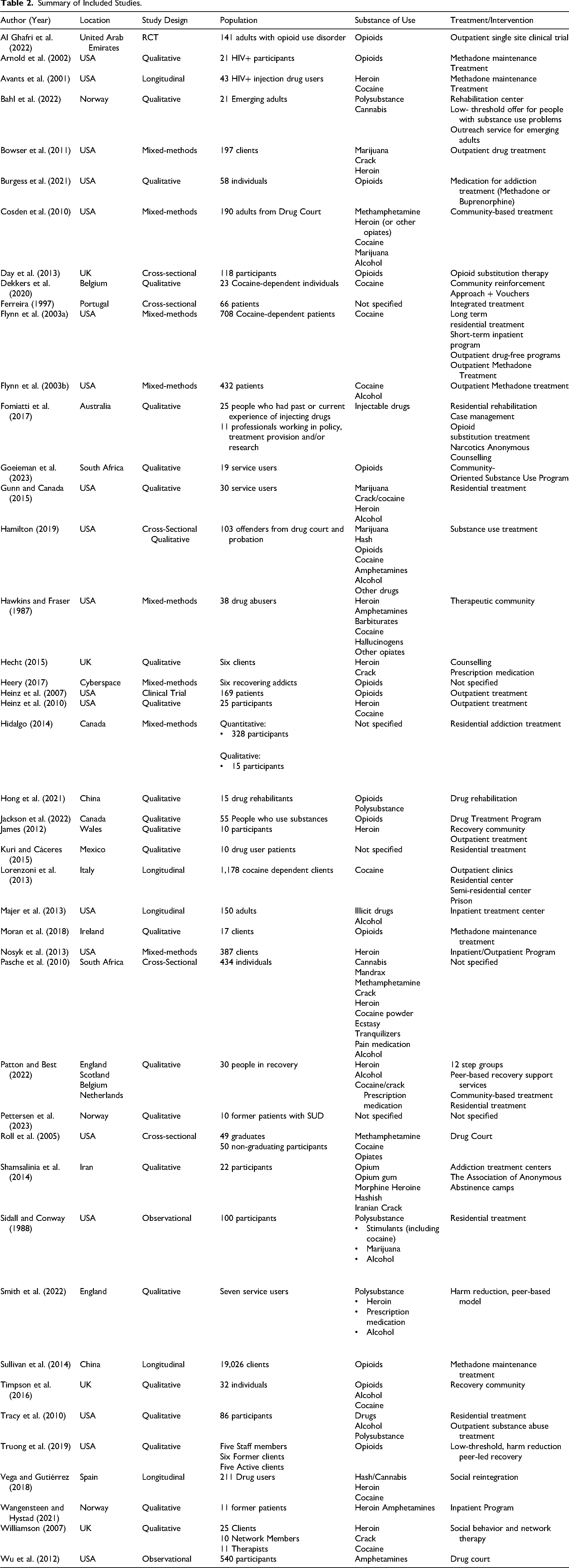
Data from each included record were extracted using a structured form developed by the authors, designed to capture key study characteristics reported in Table 2, under the following categories: author and year, study location, study design, population, sample, participants’ substance of choice, typology of treatment or intervention, and socioenvironmental factors considered. In addition, an inductive thematic analysis was conducted following Braun and Clarke's (2021) to identify patterns in how socioenvironmental factors were presented in the included studies. Although the full texts were reviewed for initial data extraction, only the primary findings were subject to thematic analysis, as these sections reflect the data derived from empirical investigation. In the familiarization phase, two researchers (João Pedro Ramos and Mariana Vieira) independently and manually conducted open coding, with codes assigned to units of meaning within the text (e.g., phrases, sentences, or short passages). All studies were independently coded by both researchers, who then compared their initial coding outputs to construct a preliminary thematic analysis grid. This iterative grid included emerging categories based on the recurring patterns observed in the data.
Summary of Included Studies.
Following this, the researchers engaged in a consensus-building process to define and refine the categories of analysis. Once an initial set of themes and categories had been agreed upon, the studies were re-read in light of this revised analytical framework, allowing for further refinement and confirmation of the coding structure. Discrepancies in coding or interpretation were resolved through discussion between the two researchers, and the thematic grid was presented to the research team for further review and validation. The analysis remained grounded in the original data, and care was taken to preserve the contextual integrity of findings while enabling abstraction at the thematic level.
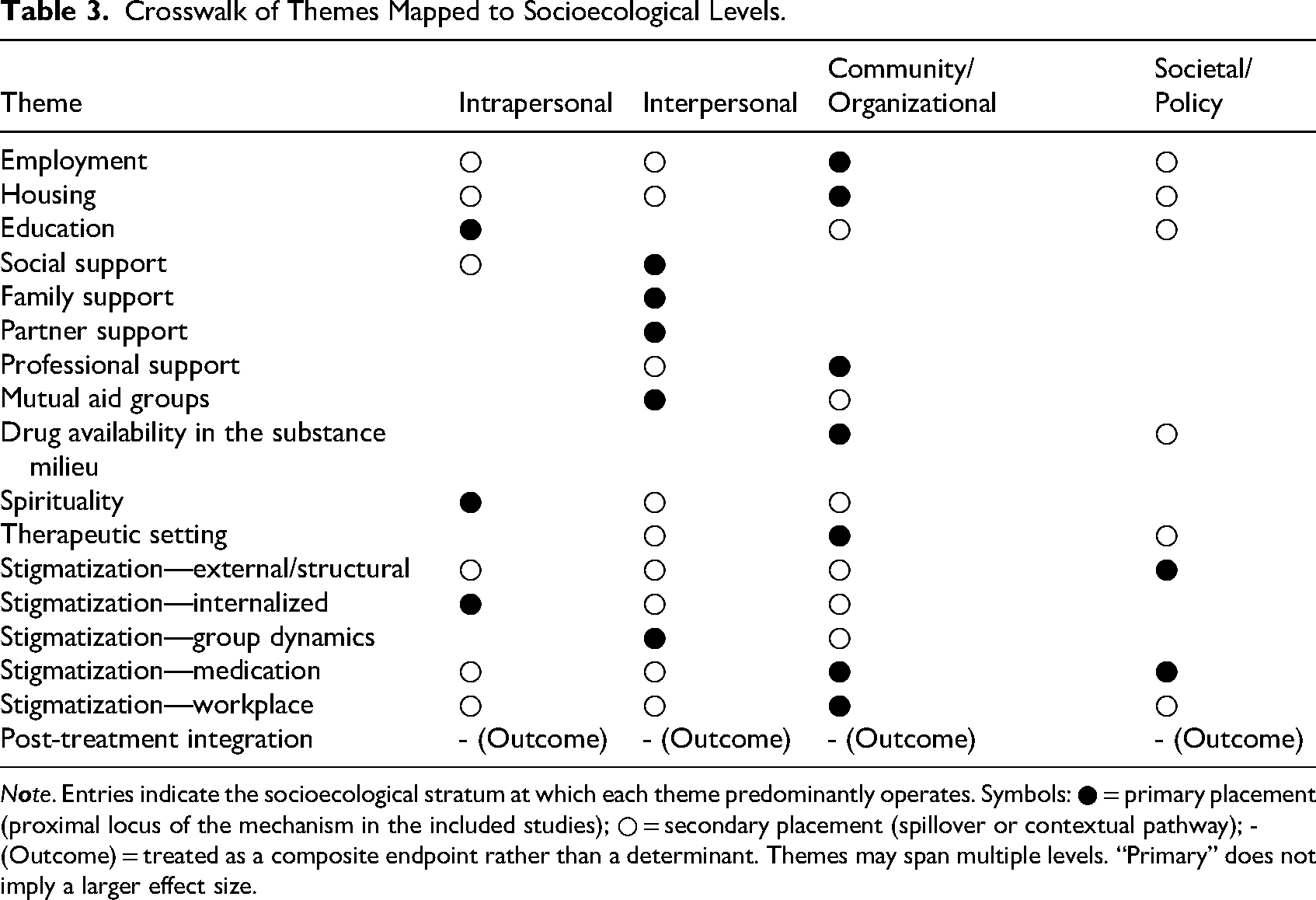
To preserve cross-level mechanisms, themes were allowed multiple socioecological placements. We coded a primary level when the included studies located the proximal mechanism there and a secondary level when effects were contextual. Where a theme functioned mainly as an endpoint, it was marked as an outcome.
Results
A total of 4,482 records were identified. After the removal of 1,467 duplicates, 3,017 titles and abstracts were screened, resulting in the removal of 2,721 records, as they did not answer the eligibility criteria. Full text screening of 295 studies was conducted, resulting in 24 records included. Retrieval from other sources coupled with backward and forward citation searching resulted in 21 included records (see Figure 1). Therefore, a total of 45 studies were included for thematic analysis.
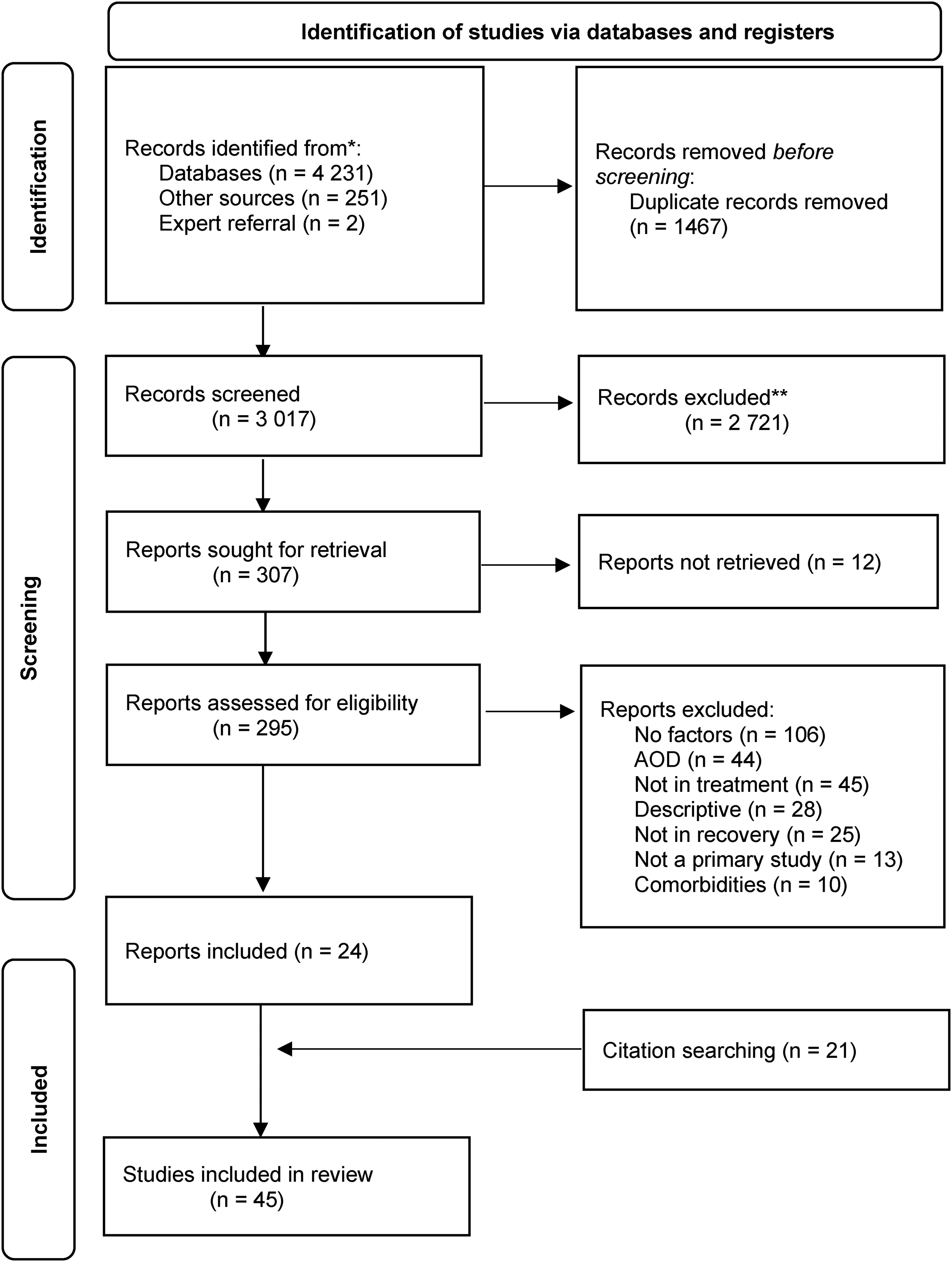
Flow diagram of review process (adapted from Page et al., 2021).
Descriptive Overview
Most included studies followed a qualitative methodology (n = 25), eight followed a mixed methods design, six longitudinal, four cross-sectional, two observational, and two clinical trials (see Table 2). This referred to a total of 25,264 participants, with the sample size of one study (Sullivan et al., 2014) amounting to 75% of the total number of included participants. The majority of the included studies resulted from research conducted in the United States (n = 19), followed by the United Kingdom (n = 4) and Norway (n = 3). Substances used were framed under opioids, cannabis, cocaine and methamphetamines, with five articles referring to polysubstance use.
Content Organization and Thematic Structuring
Following thematic analysis, identified themes were systematically organized to ensure coherence and alignment with the objectives of this review. The synthesis is presented in key areas addressing critical aspects of recovery of people with SUD. We begin by exploring Participants’ Perspectives on Recovery, where the lived experiences and personal constructions of recovery are discussed, providing foundational insights into their journey. Next, we examine the Social Determinants of Recovery, stratified into Employment, Housing, and Education, to understand their influence, barriers, and facilitators on recovery.
When investigating Support Systems, we adopted a comprehensive approach. Based on the framework proposed by Heaney and Israel (2008), we explore various dimensions of Social Support and the roles of Family, Partners, and Professional Support Systems. The analysis delves into the impact of intergenerational responsibilities within families, the influence of partner dynamics, and the support provided by healthcare professionals, further exploring the potential of Mutual Aid Groups for its transformative potential. When analyzing Drug Availability in the Substance Milieu, we emphasize the role of Network Renewal in disrupting pre-existing patterns and fostering change. The role of Spirituality is also explored, focusing on its dual function as both a protective and an altruistic factor in recovery. The analysis also considers the impact of the Therapeutic Setting, highlighting how different dimensions, such as interpersonal dynamics within therapeutic contexts, can alter the recovery pathway. Stigmatization is examined as a pervasive barrier to recovery, analyzed across multiple dimensions: External Stigma, Internalized Stigma, Group Dynamics of Stigma, and contextual stigma, such as Medication and Workplace. Finally, findings on Post-treatment Integration focus on the interplay of the aforementioned aspects as people navigate the challenges of reestablishing themselves within their communities and society.
Because several determinants operate across levels, we provide an overview in Table 3, which maps each theme to intrapersonal, interpersonal, community/organizational, and societal/policy strata.
Crosswalk of Themes Mapped to Socioecological Levels.
N
Participants’ Perspectives on Recovery
Six studies explored participants’ interpretations of recovery. According to participants in these studies, early recovery often involves overcoming substance-related hurdles, such as maintaining abstinence. As the recovery progresses, additional psychological and social challenges arise, including the consequences and underlying reasons for the SUD and cultivating positive social networks (James, 2012).
Participants described recovery as not merely a physical process but may imply a cognitive change (James, 2012), a different perspective on life, relaxation, and prioritizing positive experiences. Some participants see recovery as becoming a new person, shedding their previous identity and realizing their full potential (Dekkers et al., 2020; Timpson et al., 2016). Recovery could also imply leaving an old identity as a user and pursuing a new identity, which may require a “reset” in thinking and attitudes (Pettersen et al., 2023) and participants recognize the need to impart distance from dysfunctional thinking, destructive behaviors, or impaired control (Heery, 2017; James, 2012), along with a possible re-evaluation of life choices (Hecht, 2015).
Participants characterized recovery as a unique long-term arduous journey (Hecht, 2015; James, 2012; Pettersen et al., 2023), where the physical struggles can, at times, be anticipated but not its psychological and social impact (Hecht, 2015; James, 2012). They reported experiencing multiple emotions from fear, loss, unworthiness, anger, shame, and stigma, to hope, acceptance, faith, happiness, responsibility, resilience (Heery, 2017; Timpson et al., 2016), appreciation, and love of oneself and others (Heery, 2017).
For some participants, recovery appears to involve abstaining from substance use and harboring the determination to never use again, which they identified as fundamental for recovery (Dekkers et al., 2020; James, 2012; Timpson et al., 2016). They also emphasized the importance of acknowledging the necessity for change (Dekkers et al., 2020; Pettersen et al., 2023; Timpson et al., 2016). Adapting communication to convey and receive feedback from others aligns with the new identity as a non-user and helps manage daily stressors and confront challenges (Pettersen et al., 2023).
Social Determinants of Recovery
Employment
Employment emerges as a critical factor in the recovery pathway for people with SUD across 13 studies. Work serves as a protective element against substance use, but also a stimulus for recovery, fostering personal growth and acting as a base for support from coworkers (Dekkers et al., 2020; Nosyk et al., 2013; Pettersen et al., 2023; Roll et al., 2005; Sidall & Conway, 1988; Truong et al., 2019; Wu et al., 2012).
Balancing work and recovery present a nuanced challenge (Dekkers et al., 2020; Hamilton, 2019; Truong et al., 2019). Employment can be a stress inducer leading to substance use or a motivator for positive change (Dekkers et al., 2020; Truong et al., 2019). While some view employment as a hindrance, others emphasize its importance in providing for themselves and their families (Truong et al., 2019). Participants reported job losses due to treatment conflicts and legal concerns for missing sessions due to work commitments (Hamilton, 2019).
Unemployment strongly correlates with difficulties in treatment access and success, with employment status at discharge emerging as a predictor of treatment retention (Ferreira, 1997; Lorenzoni et al., 2013; Williamson et al., 2007) and longer periods of abstinence (James, 2012; Patton & Best, 2022; Sidall & Conway, 1988; Timpson et al., 2016; Wu et al., 2012). Additionally, employed people, particularly those engaged in amphetamine use, show higher graduation rates from treatment programs, indicating that employment provides opportunities and exposure to activities inconsistent with substance use (Truong et al., 2019; Wu et al., 2012).
Some differences by gender were observed in relation to employment and its perceived role in recovery (Vega & Gutiérrez, 2018). Men in particular reported placing greater emphasis on finding purpose, noting that taking on responsibilities in the workplace was experienced as helpful in addressing a perceived lack of purpose and responsibilities during their SUD phase (Patton & Best, 2022).
Housing
Housing came across as a factor in five studies. Living conditions play a pivotal role in substance use patterns and treatment outcomes, as homelessness, unstable housing, and specific living environments seem to impact the likelihood of continued substance use, treatment success, and relapse (Bahl et al., 2022; Day et al., 2013; Lorenzoni et al., 2013; Majer et al., 2013; Truong et al., 2019). The lack of motivation and satisfaction of basic needs among people in specific unstable living conditions highlights how the environment may foster a continuous need for substance use (Lorenzoni et al., 2013; Majer et al., 2013), while people in more regulated living conditions, such as prisons, hospitals, or drug-free apartments, have a greater likelihood of remaining substance free (Bowser et al., 2011; Majer et al., 2013). Although legal issues often disrupt access to medication for people with SUD (Truong et al., 2019), there are cases of people intentionally committing crimes to access this recovery opportunity (Majer et al., 2013).
Education
A total of five studies explored the influence of education on recovery. Education serves as a transformative tool in the recovery process, as acquiring new qualifications not only correlates with an enhanced employment rate (Patton & Best, 2022), but also elevates self-esteem and plays a crucial role in the formation of new, legitimate identities (James, 2012; Patton & Best, 2022). Improving the educational level appears to be a key turning point in recovery as it facilitates the development of new friendships and social networks, raises community capital, and offers employment and career pathways (James, 2012; Pasche et al., 2010; Patton & Best, 2022).
Spirituality
Nine studies explored spirituality's role in SUD recovery, highlighting its protective and altruistic dimensions. Spirituality can act as a guiding force (Arnold et al., 2002; Hidalgo, 2014; Shamsalinia et al., 2014), preventing cravings (Arnold et al., 2002), offering empowerment (Arnold et al., 2002; Heinz et al., 2010; Shamsalinia et al., 2014), and providing inner strength through faith in a higher power to ease the recovery burden (Arnold et al., 2002; Heinz et al., 2010; Shamsalinia et al., 2014). For some, helping others through an altruistic sense tied to spirituality also supports recovery (Heery, 2017; Hidalgo, 2014). However, it may occasionally hinder emotional or behavioral change (Flynn et al., 2003b; Shamsalinia et al., 2014).
Though some link spirituality to organized religion, some associate it with belief systems within support networks (Arnold et al., 2002). Prayer and belief can be coping mechanisms for recovery (Arnold et al., 2002), with greater spiritual support associated with more drug-free weeks (Arnold et al., 2002; Avants et al., 2001; Heinz et al., 2007). Spirituality plays a key role in motivating change (Flynn et al., 2003a; Flynn et al., 2003b; Heinz et al., 2007; Shamsalinia et al., 2014) and may emerge as a byproduct of recovery, as some seek spiritual comfort post treatment (Shamsalinia et al., 2014).
Support Systems
Recovery appears to be closely tied to multiple support systems that accompany people during their recovery pathway, including social, family, partner, professional, and mutual aid groups.
Social Support
Eleven studies explored the role of social networks, highlighting the role of friends and other members of the social network during recovery (Bahl et al., 2022; Day et al., 2013; Ferreira, 1997; Flynn et al., 2003a; Hecht, 2015; James, 2012; Pasche et al., 2010). People in recovery turn to these networks to share experiences (Flynn et al., 2003a; Hecht, 2015), seek encouragement (Flynn et al., 2003a; Hecht, 2015; Hidalgo, 2014; James, 2012), and for general or emergency help (Flynn et al., 2003a; Hecht, 2015). However, some may be non-supportive, judgmental of one's behavior, either towards drug use or recovery, or simply not available (Hidalgo, 2014).
Family Support
Family support was highlighted as an important facet of recovery throughout 25 studies, being improved family relationships considered crucial for, and sometimes a result of, successful recovery (Dekkers et al., 2020; Smith et al., 2022). Different family members were identified as supportive actors providing tangible and emotional support (Dekkers et al., 2020), through concrete actions, such as financial support (Dekkers et al., 2019), childcare provision (Dekkers et al., 2019; James, 2012), management of agendas and appointments (Pettersen et al., 2023) and material support (Ferreira, 1997). Positive family experiences such as increasing motivation (Dekkers et al., 2020; Flynn et al., 2003b; James, 2012; Pettersen et al., 2023), spiritual support (Heinz et al., 2010), and emotional encouragement (Dekkers et al., 2020) were reported as motivational factors in recovery, helping to avoid relapse and establishing a new life (Bahl et al., 2022; Smith et al., 2022; Williamson et al., 2007).
The degree of family engagement in treatment seems to be associated with treatment retention (Al Ghafri et al., 2022; Sidall & Conway, 1988), with positive relationships with mothers and frequent contact with the birth family, acting as protective factors (Ferreira, 1997; Flynn et al., 2003b). Those with parents with more external resources were generally more successful, while those with difficult family relationships were more prone to continued drug use (Al Ghafri et al., 2022; Ferreira, 1997; Wangensteen & Hystad, 2021).
Family members seem to actively facilitate recovery (Al Ghafri et al., 2022; Bahl et al., 2022; Dekkers et al., 2020; James, 2012; Moran et al., 2018; Pettersen et al., 2023; Sullivan et al., 2014) by ensuring attendance at counselling sessions, providing ongoing support (Moran et al., 2018; Smith et al., 2022), and as a source of pressure to stop drug use (Williamson et al., 2007), forming an important set of reasons given for change (Flynn et al., 2003a; Flynn et al., 2003b). Challenges may arise from a lack of understanding about substance use (Bahl et al., 2022; Moran et al., 2018), insufficient support (Bahl et al., 2022; Ferreira, 1997; Hidalgo, 2014), trauma (Bahl et al., 2022), and dysfunctional family relationships (Bahl et al., 2022; Sullivan et al., 2014; Williamson et al., 2007). Limited family support was noted in some cases, often attributed to distrust or distant relationships (Dekkers et al., 2020), while secrecy and hidden struggles were mentioned due to concerns about family members’ stress or lack of effective support (Bahl et al., 2022; Heinz et al., 2010; Hidalgo, 2014).
People in recovery who reported growing up with other family members, including stable caregivers or both parents, tended to describe smoother recovery processes, whereas those raised in institutions or single-parent families often reported facing greater challenges (Vega & Gutiérrez, 2018).
However, a secure emotional and relational environment seems to be more decisive than the specific family structure (Vega & Gutiérrez, 2018). Resilience, shaped by positive experiences and family support, is crucial, with the single mother's role emphasized as a catalyst for change (Vega & Gutiérrez, 2018). Additionally, the negative impact of maternal addiction, mental health issues, and the experience of sexual abuse appear to impart further challenges (Vega & Gutiérrez, 2018).
Overall, family support plays a multifaceted role in the recovery process, encompassing emotional, material, and motivational dimensions (Al Ghafri et al., 2022; Bahl et al., 2022; Dekkers et al., 2020; Ferreira, 1997; Flynn et al., 2003a; Flynn et al., 2003b; Heinz et al., 2010; Hidalgo, 2014; James, 2012; Moran et al., 2018; Pettersen et al., 2023; Sidall & Conway, 1988; Smith et al., 2022; Sullivan et al., 2014; Williamson et al., 2007). Renewed and positive relational experiences, reestablishing good relationships, communication with family, and being able to take care of their children were stressed as essential aspects of this new life (Pettersen et al., 2023).
Parenthood can act as a source of motivation for positive change, with inherent responsibilities, the desire for a stable home, and the respect of family members (Dekkers et al., 2020; Heery, 2017; Moran et al., 2018; Patton & Best, 2022; Wangensteen & Hystad, 2022). However, if parenthood/motherhood can act as a pull factor for some, the awareness of the potential loss of access/relationship to a child may act as a push factor for others (Dekkers et al., 2020), due to the conflict between treatment and family obligations (Hamilton, 2019), the sense of guilt (Hong et al., 2021) and extensive worry about children, adding a burden to the recovery process (Hong et al., 2021; Tracy et al., 2010). Motherhood can be a significant concern or motivational factor for some women, often outweighing romantic relationships, while societal pressures for childcare can generate a harmful cycle of guilt-consumption (Kuri & Cáceres, 2015).
Partner Support
Seven studies examined the influence that partners may exert during recovery. Partners can act as a positive influence for recovery (Bahl et al., 2022; Day et al., 2013; Ferreira, 1997), but can also be a greater source of conflict and control (Kuri & Cáceres, 2015; Patton & Best, 2022; Tracy et al., 2010). Those who report having a drug-free partner describe them as a source of motivation (Bahl et al., 2022), while those with drug-using partners may feel additional pressure to use drugs during recovery (Patton & Best, 2022). This dynamic seems to pose greater challenges when people in recovery are entangled in dysfunctional relationships (Patton & Best, 2022), which seems to disproportionately impact women's journey (Kuri & Cáceres, 2015; Patton & Best, 2022; Tracy et al., 2010). Moreover, violent and abusive relationships appear to be a source of trauma that may thwart recovery (Patton & Best, 2022).
Professional Support
Professional support, examined in eight studies, significantly influences recovery, as both a motivator (Dekkers et al., 2020; Goeieman et al., 2023; James, 2012; Pasche et al., 2010; Smith et al., 2022) or a potential barrier (Hamilton, 2019; James, 2012). Strong therapeutic relationships are fostered by making individuals feel comfortable and secure (Dekkers et al., 2020; Hamilton, 2019; James, 2012), as effective support hinges on professionals’ ability to assist and listen without judgment (Dekkers et al., 2020; Hamilton, 2019; Jackson et al., 2022; Smith et al., 2023).
Some participants found it easier to connect with therapists who had personal experiences with drug use, as they could better resonate with their recovery journey (Hamilton, 2019; Hidalgo, 2014). However, professionals must differentiate support approaches for individuals still using drugs versus those in recovery, as their needs differ significantly (James, 2012).
Mutual Aid Groups
Mutual aid group, mentioned in six studies, are those developed amidst or as a result of a recovery group and appear to be sought as a means to experience a sense of social support (Smith et al., 2022), where people can seek to develop social bonds with other members (Patton & Best, 2022). These include community groups, like volunteering, and art groups (Smith et al., 2022); but mutual aid groups, such as Narcotics Anonymous, are the most prominent (Fomiatti et al., 2017; Hecht, 2015; Heinz et al., 2010; Majer et al., 2013; Patton & Best, 2022; Smith et al., 2022). These groups offer a safe place for people to share their experiences (Patton & Best, 2022; Smith et al., 2022), as well as relate to other members’ experiences (Hecht, 2015; Smith et al., 2022), assisting in the acquisition of new social lenses as people in recovery transition from subcultures that hinder recovery to more supportive environments (Patton & Best, 2022).
Drug Availability in the Substance Milieu
Drug availability and network renewal were explored in 15 studies, highlighting exposure to substances and substance use as significant recovery barriers (Bahl et al., 2022). Relationships within networks can hinder recovery through invitations to use drugs, emotional manipulation, or coercion to leave treatment, particularly for low-income women navigating complex support and dense drug use communities (Tracy et al., 2010). Distancing from high drug availability environments serves as a protective factor for recovery, with reduced substance use observed in those who sever ties with such networks (Bahl et al., 2022; Day et al., 2013; Flynn et al., 2003b; Hecht, 2015; James, 2012; Moran et al., 2018; Patton & Best, 2022; Pettersen et al., 2023). However, maintaining this distance can be challenging, especially for those sharing accommodations with other substance users (Moran et al., 2018). Proximity to individuals who sell or provide access to drugs exacerbates recovery difficulties, with some participants coerced into use or offered places to use substances (James, 2012; Tracy et al., 2010).
Network Renewal
Rebuilding a support network is a continuous process throughout recovery, essential for successful post-treatment integration into society (Hawkins & Fraser, 1987). Renewing these networks fosters improved social functioning among support members, such as family and friends (Bahl et al., 2022; Cosden et al., 2010; Fomiatti et al., 2017; Hawkins & Fraser, 1987; Sullivan et al., 2014). Upon entering treatment, individuals often find their networks dominated by people from the substance milieu (e.g., drug suppliers) (Patton & Best, 2022). As they distance themselves from these networks, feelings of isolation and loneliness can emerge (Hecht, 2015; James, 2012; Patton & Best, 2022), prompting a reassessment of relationships and the search for new, supportive connections while avoiding harmful environments (Patton & Best, 2022; Williamson et al., 2007). This shift reflects increased self-awareness of influences on recovery and may involve connecting with peers from treatment settings (Cosden et al., 2010; Fomiatti et al., 2017). Challenges arise when rebuilding networks requires cultural or linguistic adaptation or when alternative connections are limited (Pettersen et al., 2023).
Therapeutic Setting
Treatment experience, explored across 14 studies, is central to recovery, with person-centered, recovery-focused interventions addressing evolving needs (James, 2012). Services must balance structure (Heinz et al., 2010; Jackson et al., 2022; Truong et al., 2019) and flexibility (Hecht, 2015; James, 2012; Truong et al., 2019), accommodating life responsibilities while ensuring accountability (Hecht, 2015; Heinz et al., 2010; James, 2012; Truong et al., 2019). Meaningful activities help distract from substance use (Bahl et al., 2022; Cosden et al., 2010; Dekkers et al., 2020; James, 2012; Wangensteen & Hystad, 2021), foster peer and staff connections (Bahl et al., 2022; James, 2012), and prevent relapse due to boredom (Bahl et al., 2022; Dekkers et al., 2020). Spiritual activities can reduce idle time but should remain inclusive of secular approaches (Arnold et al., 2002; Heinz et al., 2010). Social assistance includes employment (Bahl et al., 2022; Hecht, 2015; James, 2012), housing (Hecht, 2015; Moran et al., 2018), education/training (Bahl et al., 2022; James, 2012), and child welfare services (Wu et al., 2012). Employment and education enhance motivation and self-worth (James, 2012), serving as a means to provide occupation during the treatment (Bahl et al., 2022; James, 2012). Child welfare services support parenting's role in recovery, aiding those balancing treatment and family responsibilities (Tracy et al., 2010; Wu et al., 2012). Post-treatment support is crucial for societal integration, mitigating dependence on structured environments (Dekkers et al., 2020; Fomiatti et al., 2017; Hecht, 2015; James, 2012). Psychological support may help cope with negative thinking (James, 2012), and peer support appears to be fundamental as a means to establish a support system inside the therapeutic setting (Bahl et al., 2022; Goeieman et al., 2023; James, 2012).
Stigmatization
The dimension of stigma is explored in ten studies, perpetuated in healthcare, government agencies, pharmacies, and other settings (Burgess et al., 2021; Fomiatti et al., 2017; James, 2012). Stigma is particularly pronounced in pharmacies, involving long waits for prescriptions and negative interactions with staff, influenced by whether the medication is related to SUD (Burgess et al., 2021; James, 2012). In hospitals, particularly emergency departments, stigma emerges through assumptions of drug seeking based on health records, prompting people to make specific care requests to counter this label (Burgess et al., 2021; James, 2012). Long waiting times, being turned away, receiving treatment in less favorable conditions, lack of compassionate care, and reluctance in prescriptions are some of the problems faced in accessing healthcare (Burgess et al., 2021).
External Stigma
External stigma is reinforced by media-driven stereotypes about self-identity and addiction struggles (Hecht, 2015). Negative portrayals by the government further diminish societal empathy and care for those in recovery, intensifying feelings of powerlessness (Hecht, 2015; Smith et al., 2022). Empowering users to share their perspectives could prompt shifts in government and societal attitudes, highlighting the complexity of recovery beyond simply achieving abstinence (Burgess et al., 2021; Hecht, 2015).
Internalized Stigma
Societal attitudes, including stigmatizing language such as “junkie” or “addict,” foster shame and fear of judgment, complicating identity reconciliation during recovery (Hecht, 2015; James, 2012). This language impacts access to treatment, reinforces societal judgment, and undermines self-worth, confidence, and mental well-being (Burgess et al., 2021; Hecht, 2015; James, 2012; Kuri & Cáceres, 2015). Stigma and internalized fears isolate people in recovery, straining personal relationships and fostering alienation (Burgess et al., 2021; Hecht, 2015; James, 2012; Kuri & Cáceres, 2015). This isolation often leads to depression, adversely affecting mental health and hindering recovery (Burgess et al., 2021).
Group Dynamics of Stigma
Within certain drug-using communities, hierarchies may emerge where those using heroin or crack cocaine (termed “hard users”) may experience stigma from marijuana users ('soft users”), who perceive them as “out of control” and physically degraded, leading to harsher judgments based on what they see as higher severity (Gunn & Canada, 2015; Kuri & Cáceres, 2015). Nonetheless, this perception of severity simultaneously affords “hard users” social power and authority within treatment environments, creating a paradoxical position of both inferiority and superiority. On the other hand, “soft users” experience a different form of devaluation, as their drug use is often dismissed as inauthentic or undeserving of treatment resources yet they retain social acceptability (Gunn & Canada, 2015). Despite these dynamics, “hard users” experiences of trauma and turmoil may serve as preventive tools, offering warnings to others and underscoring the need for a more unified community to overcome internal stigmas (Gunn & Canada, 2015).
Medication Stigma
The perception that discontinuing medication is essential for authentic recovery stems from peer influence in mutual aid groups, shame around medication use, idealized recovery images, and the notion of abstinence as the unique form of recovery (Moran et al., 2018; Truong et al., 2019). Anxiety about judgment and strained relationships, particularly with General Practitioners (GPs), often deters individuals from disclosing their reliance on MAT (Moran et al., 2018). A lack of trust in GPs fosters feelings of abandonment, isolation, and insufficient healthcare support, contributing to loneliness and fear, which may lead to treatment discontinuation and poorer recovery outcomes (Moran et al., 2018; Truong et al., 2019).
Workplace Stigma
Juggling work and treatment schedules while keeping recovery confidential seems challenging (Burgess et al., 2021), with pill counts, urine sampling, and group counselling described as challenging to manage alongside full-time employment (Burgess et al., 2021). The decision to remain secretive about drug use appears to be driven by the desire to protect the professional identity (Hecht, 2015; Patton & Best, 2022) and avoid potential negative consequences, such as colleagues’ perceptions and lack of support (Hecht, 2015).
Post-Treatment Integration
Integration after leaving treatment was discussed in only two studies. Challenges include returning to previous environments that may involve old networks, though most people aim to build new support systems, avoiding both peers from treatment settings and those involved in drug use (Hawkins & Fraser, 1987; Kuri & Cáceres, 2015). A key difficulty is ending relationships sustained by shared drug use, prompting a re-evaluation of connections (Kuri & Cáceres, 2015). Breaking these ties often leads to reliance on alternative networks, such as family, partners, or mutual aid groups (Kuri & Cáceres, 2015). Reestablishing family connections post treatment can enhance functionality across various aspects of family dynamics (Kuri & Cáceres, 2015). Recovered people tend to consider themselves as part of the norm, manifesting stigmatized behaviors or attitudes towards those who are still drug users, leading to a stigmatization paradigm (Kuri & Cáceres, 2015).
Discussion
This scoping review mapped the socioenvironmental factors influencing the pathway of recovery of people with SUD, with support networks as the most studied factor. Systemic inequities in housing, education, and employment compound vulnerabilities and interact with dimensions such as socioeconomic status and stigma, hindering recovery (Dekkers et al., 2020; James, 2012; Timpson et al., 2016). Individual constructions of recovery often extend beyond abstinence, emphasizing recovery as a continuum rather than a singular focus on abstinence (Dekkers et al., 2020; James, 2012; Timpson et al., 2016). Definitions vary across frameworks, but recovery as a dynamic process involving identity, emotional resilience, and a journey encompassing physical, psychological, and social dimensions is largely highlighted.
From the perspective of the socioecological model (Witkiewitz & Tucker, 2024), recovery can be better understood as the interplay of factors operating across individual, interpersonal, community/structural, and cross-cutting domains. Furthermore, the multi-level mapping in Table 3 makes explicit that most determinants are not level-exclusive, which justifies our decision to synthesize themes narratively while providing a crosswalk to the socioecological architecture.
At the individual level, recovery is shaped by personal constructions of meaning and well-being. For many people, recovery involves more than abstinence, encompassing identity development, emotional resilience, and self-realization (Dekkers et al., 2020; James, 2012). Minority stress processes—such as internalized stigma, expectations of rejection, and concealment of identity—further complicate this journey, as individuals belonging to stigmatized groups experience added psychological burdens that can undermine self-worth and heighten vulnerability to relapse (Meyer, 1995). Recovery is thus a deeply personal but also socially mediated process, embedded in intersecting systems of oppression and opportunity
At the interpersonal level, support networks emerge as central determinants of recovery. Strong support systems can predict treatment completion, reinforce treatment continuity, and reduce the likelihood of relapse (Sidall & Conway, 1988). When one support system is absent or unsupportive of recovery, other support systems become more critical (Bahl et al., 2022), though ruptures in these relationships can impoverish the overall support network (Kuri & Cáceres, 2015). People in recovery may find meaning and belonging in mutual aid groups, though some may feel alienated or struggle with the format (Heinz et al., 2010; Smith et al., 2022).
Family can have a positive influence when the dynamics are marked by tangible and positive emotional support (Al Ghafri et al., 2022; Sidall & Conway, 1988), though dysfunctional or distrustful family bonds can become barriers (Bahl et al., 2022). Here, Rhodes’ risk environment provides insight: interpersonal networks are not neutral but can be sites of both risk and protection, depending on whether they reproduce stigma, violence, or control (Patton & Best, 2022), or instead foster inclusion and stability. Minority stress processes also play out in these networks, with stigma, discrimination, and microaggressions eroding interpersonal trust and reinforcing cycles of marginalization.
At the community and structural levels, employment, housing, and education emerge as critical sociostructural determinants. Employment, in particular, is consistently linked with self-worth, identity, and legitimate social roles (James, 2012; Patton & Best, 2022; Pettersen et al., 2023; Wu et al., 2012). Interventions promoting employment through training or transitional programmed foster employability and facilitate new social identities, often proving more salient than abstinence itself (Sidall & Conway, 1988). Housing and education similarly act as both supports and incentives, encouraging treatment adherence and reflecting broader psychosocial adjustment (Sidall & Conway, 1988).
From a risk environment perspective, however, these structural dimensions also reveal inequities: systemic barriers in housing, labor markets, and educational access perpetuate exclusion, disproportionately affecting marginalized groups. Minority Stress Theory extends this analysis, demonstrating how structural stigma—through discriminatory policies, labor market exclusion, and unequal access to services—creates chronic stressors that undermine recovery (Meyer, 1995).
Drug availability within community environments further complicates recovery, with the substance milieu exerting influence even during or after treatment (Truong et al., 2019). Breaking ties with drug-related networks is crucial for sustaining recovery, as network renewal—replacing old ties with new, supportive ones—has been shown to support long-term outcomes (Bahl et al., 2022; Cosden et al., 2010; Fomiatti et al., 2017; Hawkins & Fraser, 1987; Sullivan et al., 2014). Yet, for those in structurally disadvantaged or geographically remote communities, opportunities for new supportive networks may be limited (Kuri & Cáceres, 2015).
At the cross-cutting level, stigma operates as a pervasive force that intersects with all others. Manifestations of stigma extend beyond healthcare and the substance milieu (Burgess et al., 2021; Fomiatti et al., 2017), shaping societal views, creating barriers to education, employment, and healthcare, and hindering recovery (Moran et al., 2018). Stigmatizing language reinforces discrimination, damaging self-worth and limiting treatment access (Burgess et al., 2021; James, 2012). Adopting neutral, inclusive language is thus essential to transform perceptions and reduce harm (Cervone et al., 2020). Integrating the Minority Stress framework highlights how stigma is not only interpersonal but systemic, producing cumulative stressors that disproportionately affect queer, racialized, and other marginalized groups. From a risk environment perspective, stigma functions as a structural determinant of health, limiting opportunities across multiple ecological levels.
Researchers have minimally explored post-treatment integration efforts, noting that developing new support networks is crucial for fostering belonging, though ruptures with pre-existing networks may hinder those in remote areas with limited options (Kuri & Cáceres, 2015). Multi-level interventions that simultaneously address individual resilience, interpersonal support, and structural inequalities, while also dismantling stigma and reducing minority stressors can be presented as an integrated approach, grounded in the SEM, the risk environment, and the minority stress framework, provides the most comprehensive lens for advancing equitable and sustainable recovery pathways.
Strengths and Limitations
This review highlights various dimensions of the social environment, revealing its interactions and influences on recovery. While recovery is multidimensional, most results focused on abstinence as the primary outcome, except in studies where participants focused on the essence of recovery. Although the primary intent was not to establish a consensual construct of recovery, this diversity could have impacted the interpretability of the results. Nonetheless, we sought to incorporate gray literature, ensuring a comprehensive overview of existing information, thus complementing theoretical and empirical findings from published peer-reviewed articles. The overemphasis on support networks overlooks other contributing factors, hindering a comprehensive understanding of other factors that could significantly impact recovery. Moreover, a restricted number of studies explore users’ integration after leaving treatment, reflecting the continued low number of follow-ups that are performed within the post-treatment, though included studies hypothesize the importance of following the person until their effective integration. Therefore, there is a need to expand the group of factors that are considered when exploring recovery, as a means to ensure a more holistic understanding of the multifaceted nature of recovery into society.
Conclusion
No single solution fits all, and different services must be available to respond to the various intersections of people in recovery. Therapeutic approaches should seek to be holistic and involve every network surrounding the individual to sustain treatment success and facilitate post-treatment integration. Services must address the underlying factors that perpetuate inequities in access, especially for those with multiple vulnerabilities. Though family and social networks play prominent roles, attention is needed in cases of family conflict or drug-using networks, which could result in the support provided being subpar to what is expected. By recognizing and mitigating the systemic barriers faced by people with SUD, interventions can be better tailored to support sustainable recovery outcomes.
Supplemental Material
sj-xlsx-1-cdx-10.1177_00914509261416129 - Supplemental material for Socioenvironmental Factors in Recovery of People with Substance Use Disorders: A Comprehensive Scoping Review
Supplemental material, sj-xlsx-1-cdx-10.1177_00914509261416129 for Socioenvironmental Factors in Recovery of People with Substance Use Disorders: A Comprehensive Scoping Review by João Pedro Ramos, Mariana Vieira, Cátia Moreira de Carvalho, Filipa Gonçalves, Pedro Barbosa, Ana Aguiar and Marta Pinto in Contemporary Drug Problems
Footnotes
Author's Contributions
All authors contributed to the conceptualization of the manuscript. João Pedro Ramos and Mariana Vieira wrote the main manuscript and prepared tables. João Pedro Ramos, Mariana Vieira, and Marta Pinto performed the search strategy and screening. Cátia Moreira de Carvalho, Filipa Gonçalves, Pedro Barbosa, and Ana Aguiar provided consultation. All authors reviewed and contributed to the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Fundação para a Ciência e a Tecnologia (Grant Number LA/P/0064/2020, UIDB/04750/2020).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.