
Abstract
Proponents and critiques of the brain disease model of addiction (BDMA) discuss its benefits and shortcomings in the light of agency. Yet, in this controversy, the experiences of the persons suffering from addiction have so far been widely neglected. This article investigates addiction service's clients’ experiences with their recovery in the light of the BDMA. It asks what role the BDMA plays in the recovery narratives of persons struggling with addiction. Eleven focus groups were conducted with clients of the Centre for Addiction and Mental Health in Toronto, Canada. The interview protocol consisted of direct questions and discussion stimuli concerning the BDMA. The transcripts were analyzed by a thematic analysis. Participants both approved and disapproved the BDMA. The recovery narratives demonstrate how agency can be constructed without autonomy. Whereas the BDMA questions the agency of persons suffering from addiction in denying them autonomy, it helped as a symbolic resource in including the contradictive experiences with addiction into an authentic biography. This study thus urges addiction research to make use of agency in its entirety and take both, autonomy and biography, into account.
Introduction
Neuroscientific research contributes to our understanding of addiction. Besides the benefits of dealing with addictions by implementing neuroscientific knowledge and techniques practically, the conceptualization of addiction as an issue of the brain also has wider implications. Hacking (1999), a Canadian philosopher, would term addiction as an interactive kind. Interactive kinds are intersubjectively shared blueprints for understanding the world and acting in it (cf. Egerer, 2014). Interactive kind concepts change constantly as people react toward them by integrating them into their lifeworld but also by active resistance meaning that as new information becomes available through daily life, individuals can either integrate new beliefs and knowledge into their identity or reject them (cf. Carr, 2011; Netherland, 2011).
In this article, we approach addiction as an interactive kind, a socially constructed and constantly reconstructed concept. We conduct focus-group interviews with addiction treatment clients. Specifically, we focus on the clients' experiences of recovery in the light of the brain disease model of addiction (BDMA).
The Disease and the Brain Disease Model of Addiction
While a considerable number of conceptualizations of addiction have existed in parallel, the disease model of addiction is well established as it is comprised of the basic concepts of addiction (Edman, 2009). The disease model received special momentum by its inclusion in the Alcoholic Anonymous movement and Jellinek's typology of alcoholism (Fingarette, 1988). Jellinek (2010 [1960]) describes four types of alcoholism, which resemble problematic patterns of drinking. The γ- and the δ-type would be diseases, while the others are problematic habits (ibid.). While three types of alcoholism have been widely forgotten beyond a specialist audience, the γ-alcoholism type is the most widely known and portrays addiction as detrimental consequences related to loss of control over an individual's consumption. Neurobiological research has been motivated by this understanding and has successfully identified the brain regions and mechanisms involved in the inability to control one's use of substances (Lewis, 2022). The disease model as well as the BDMA clearly places the root of the problem in the person—more specifically, the person's brain—and not in the substance or environment. This does not mean that the setting would be ignored in the BDMA, but these environmental determinants are merely considered external risk factors rather than inherent elements of addiction (cf. Heilig et al., 2021; Hellman & Egerer, 2022; Weinberg, 2022a).
The BDMA is not only reductionist by sidelining set and setting beyond the brain but also in being contradictive in itself. Proponents highlight the overly complex biochemical mechanisms in the brain but at the same time explain addiction as a product of one or two reward pathways (Fraser et al., 2014). Furthermore, the focus on these pathways unduly equates reward with motivation (Kalant, 2010). Overall, this challenges the assertion that neuroscientific research would have the ability of finding clear neurological equivalents to the loss of control component of addiction (cf. Weinberg, 2022b).
Proponents of the BDMA also suggest that subscription to the model will be beneficial in reducing addiction stigma. Similar to the historical disease model of addiction, the modern BDMA describes an individual's addictive behaviors as outside of their control thereby eliminating moral responsibility for their actions (e.g., Leshner, 1997; Volkow et al., 2016). Consequently, the BDMA decreases the stigma attached to addiction and leads to a more humane treatment (in its widest sense) of people suffering from addiction and may also increase help-seeking behaviors. That said, critiques of the BDMA question the beneficence of this model on exactly the same ground: the assumed loss of control. The brain's reward pathways of treatment-seeking drug users are activated more by unseen drug cues than visible ones (Childress et al., 2008). The drug users are thus not even aware, which incites their drug desire and makes them lose control over their drug consumption. Loss of control robs people of their agency by questioning their free will and ability to regain control of their behaviors which may lead to stigmatization itself (e.g., Heather et al., 2018; Lewis, 2017).
Theoretical Approach
The dominant biomedical models of addiction, addiction treatment, and addiction research have been under growing scrutiny in recent years (Fraser, 2020). The conceptualization of addiction has been criticized for its dichotomization of health, where one would be either addicted or “healthy” (Keane, 2001). The “tainted” body of the drug user gets juxtaposed to a “pure” and desirable one leaving the drug user stigmatized (Fraser, 2020). Continuous models of addiction also exist which may be a more accurate approach to addiction. Here, more intense consumption periods alternate with less intense consumption periods and the severity of addiction exists on a continuum ranging from low severity, with little consequences related to drug use to high severity with many consequences related to drug use (e.g., Morris et al., 2020; Reith & Dobbie, 2013).
The centrality of health in addiction research is also problematic from the perspective of its biomedicalization, which can go down to the molecular level (cf. Rose, 2009). Hellman et al. (2022) put forward the hypothetical extreme case where addiction is a “sick” brain to be treated independently from the human being carrying this organ around. While this remains a hypothetical exaggeration for illustration, Hammersley (2022) urges us to consider the human level. The human level integrates “social ideas, customs and behavior” (ibid. p. 177) and goes beyond reducing humans’ troubles to clear-cut diagnoses.
Treatment and research have not only been criticized as dealing with addiction as a narrow and dichotomous medical disorder but as an entirely individualized problem (e.g., Alexander, 2012). Adams (2016) calls this the particle view, which considers the self as a discrete autonomous unit. Addiction and its treatment become disconnected from social ties and the community. Instead, addiction needs to be understood and studied in context and as a social phenomenon (Alexander, 2012; Egerer et al., 2020), where the social dimensions are not merely reduced to variables and risk factors (Adams, 2016).
Criticism from the social sciences has not remained free from scrutiny itself. Crucial for fully understanding addiction is the materiality of the substances and the body (Fraser, 2020). The material dimension cannot be ignored. Demant (2009), for example, studying the drinking habits of Danish teenagers could demonstrate that alcohol itself becomes an actor in teenagers’ romantic relationships. The material dimension, yet, remains alterable and changes in a network of relations between all concerned human or nonhuman actors (Fraser, 2020).
Following the criticisms we just described, we understand drug use and addiction like a software program as “running” on the hardware, that is, the human body. Yet, individuals need to make sense of their experiences by using the intersubjectively among shared and constantly created concepts of addiction “available” in society (Egerer, 2014). For instance, Elster (1999) uses the example of emotions to illustrate the necessity of making sense of one's bodily sensations based on cultural scripts. Persons wanting to quit their addiction use intersubjectively shared models of recovery (Koski-Jännes & Hänninen, 1999). In this article, we inquire about these intersubjectively recreated concepts for addiction and addiction recovery in the framework of the highly individualized and biomedicalized BDMA.
Loss of Control and Agency in Addiction
In his landmark paper, Levine (1978) describes how the concept of addiction, defined as a loss of control over one's drinking, resulted from the puritan values of colonial US America and a shift from external to internal social control. With modernity, individuals are considered free and are thus the one's responsible for their actions and lives (cf. Elias, 2005 [1939]; Foucault, 1977). With the liberalization from traditional ties during the modernization process, individuals are expected to become autonomous actors in building a life course of their choice and to develop their own personal biography (Beck, 1986; Giddens, 1991). Losing the “core neo-liberal values of freedom (…)” the “addicts” get the “status as ‘the other’” and become stigmatized (Reith, 2004, p. 296). This also questions how a disease model, working with the assumptions of the loss of control, could be helpful in decreasing stigma (Fraser et al., 2017; Morris, 2022; Rundle et al., 2021). While studies enquiring the BDMA have looked at stigma from an instrumental perspective, such as its effect on treatment seeking and individual's feelings of guilt and shame (e.g., Kvaale et al., 2013), the current study scrutinizes stigma in the light of the contemporary societal context and examines the BDMA's interrelation with agency.
Essentially, agency is the capacity to act, but the concept is usually understood and used in a much more elaborated way. Studies on addiction that focus on the social frameworks of addiction often include agency and the role of freedom and autonomy (Uusitalo & Egerer, 2024). Gjelsvik (1999) distinguishes between the freedom of action, that is, that one can do what one wants, and the freedom of will, that is, the freedom to want what one really wants. People suffering from addiction usually have the freedom of action; they can either take the drug or not. Depending on the jurisdiction this may be an illegal activity, but there is usually no immediate obstacle to take the drug. The enigma of addiction is that people seem to act against what they really want; they have promised themselves and others multiple times to quit, but yet relapse again and again. The person with addiction is thus unfree when it comes to the freedom of the will (ibid.). Agency bears key importance in the conceptualization of addiction, but the loss of agency becomes even more paradoxical in the practical considerations of one's recovery (Levy, 2006). For recovery, agency is necessary, yet as defined by disease models of addiction, these individuals have lost control over their behaviors and therefore have lost their agency in regard to their addiction (McCullough & Anderson, 2013). This is an even more demanding paradox in the case of the brain disease model, as the drug desire originates outside the drug user's active awareness (Childress et al., 2008). Watson (1999) argues that addiction might be more so of a matter of appeal than brute force. Such a perspective also allows for differing degrees of agency in addiction, whereas this degree of agency is rather circumstantial than a fixed property of a person (Duff, 2011; Uusitalo et al., 2013). Relevant relations not only exist between human agents but include all factors connected in the assemblage of addiction and are in constant flux (Duff, 2014). Consequently, we agree with the Deleuzian approaches on the complexity of the addiction and recovery assemblages (see e.g., Duff, 2014; Fraser et al., 2014). This adds a new dimension to recovery from merely considering the outcome—quitting substance use and regaining self-control—to seeing recovery as a process of positively shaping one's life while still recovering (Theodoropoulou, 2021). In the following section, we will discuss this process of recovery in more detail.
Narrating Recovery and Scripted Narrations
Narratives take an important role in people's struggle and recovery with addiction, as it helps building and forming one's identity (McIntosh & McKeganey, 2000). Identity is something fluid, changing over time (Reith, 2004). This is crucial in recovery where persons suffering from an addiction need to reframe both their personal and social identities for themselves and the people around them (Koski-Jännes, 2002). Past studies examining individual's narratives in addiction recovery have identified progressions from an “addiction identity” toward various kinds of “ex-addiction” identities (Best et al., 2016; Downey et al., 2000; Jacobsen, 2001; Koski-Jännes, 2002; Koski-Jännes & Hänninen, 1999; McIntosh & McKeganey, 2000). “Ex-addiction" identities can vary between what Koski-Jännes (2002) called returning to an old (i.e., ‘pre-addiction’), an emergent (i.e., ‘new’), or an extended identity. The extended identity incorporates the old ‘addict’ identity into the new one, like the lifelong ‘alcoholic in recovery,’ in the AA (Alcoholics Anonymous) groups.”
Best et al. (2016) also discuss an identity change as someone recovers from addiction to their newly recovered self. The description of an individual's narrative about their past and present shapes their future selves. It may limit future options and construct chain reactions for future life but it also represents a consistent and acceptable course of life (McIntosh & McKeganey, 2000). Largely, this resembles the concept of biography as one dimension of agency (see e.g., Beck, 1986; Giddens, 1991). The narratives we tell both others and ourselves about our past are always embedded in culture and we get the stories out of society's “warehouse of narrative models” (Koski-Jännes & Hänninen, 1999, p. 1838) and rewrite our past and shape our future accordingly (Hacking, 1995).
For a long time, the disease model of addiction (for a critique of this model see e.g., Fingarette, 1988; Valverde, 1998)—popularized by the AA movement—has been the script for countless addiction biographies. The disease model considers distinct people as vulnerable to addiction, whereas the majority can consume the substance without becoming addicted. The danger of addiction lies in the person (Heather, 2017). Such prone persons are bound to become addicted after a trial and recreational phase, then use the substance excessively and finally hit rock-bottom. After that, they either manage to quit or eventually die. Interestingly, on one side, this model understands recovery as a lifelong process, but the other, focuses on the recovery as an outcome.
The pervasiveness of the disease model of addiction as a script for narrating one's addiction recovery can be seen in the six stages of addiction that Davies (1997) identified in his study of drug users. The first two stages concern the initial recreational use and the occurrence of the individual's first problems with their substance. Stage 3 is the genuine addiction phase, where the use of drugs has solely discordant connotations. Stage 4 is a stage of transition, where the individual's narrative breaks away from the “addicted” identity, either leading them to return to the previous stage of genuine addiction or progressing to either one of the last two stages. These last two stages are either the positive outcome of leaving addiction in the past or the negative version of stage five, “a kind of limbo” (ibid., p. 58) signifying an uncertain outcome. Comparing former alcohol dependents in Poland, Klingemann (2011) also identified the presence of a medical conceptualization of addiction in her interviewees’ recovery narratives, with a strong emphasis on willpower.
Similarly, Carr (2011) examined personal narratives of homeless women in an outpatient treatment program and found that these narratives play a crucial role in their recovery. The study demonstrated the importance of the centrality of language as part of contemporary drug treatment in the United States. The recovery from addiction is not limited toward a change in the substance use behavior but also involves making use of the individual's narrative, taking-up a healthy lifestyle and healthy language. While the women's recovery process is evaluated based on appropriate use of language and disclosure of their inner life, they are able to “flip the script” to their advantage, that is, use the officially authorized language without reference toward their inner feelings, or put mundanely, they lie to please their therapists and case workers. This strategy is a mixed blessing, which “simultaneously reproduces and undermines therapeutic practices” (Carr, 2011: p. 226). The phenomenon of “flipping the script” sheds new light on the production of clients’ power and active agency in addiction treatment.
The BDMA has adopted many of the main tenets of the traditional disease model of addiction, including the notion that addiction is a lifelong condition by terming addiction a chronic relapsing brain disease. Additionally, the notion of loss of control remains a defining characteristic of the BDMA (Satel & Lilienfeld, 2014). That said, the BDMA extends upon the traditional disease model by tracking the loss of control down to the biological, molecular, and neurological levels (exemplified as a “hijacked-brain”) (Volkow et al., 2016).
Biological explanations have the potential to become a very dominant script for narrating one's addiction recovery (cf. Hammer et al., 2012). Yet, clients in treatment for their addictive disorders have been also quoted on their understanding of addiction (Meurk et al., 2016). These individual's provided lay scientific explanations of the brain mechanisms involved in the chronicity of addiction but excluded physical and biological factors in their personal experiences. It is important to note that clients have also explicitly discussed that if addiction was defined as a brain disease, it would increase stigma toward them from the public and highlight that this label of being “brain diseased” may be too serious for their condition (Meurk et al., 2016; Morphett et al., 2017; Netherland, 2011). Lastly, clients and clinicians themselves have both raised concerns regarding how “brain disease” terminology may absolve those with addictions of their personal responsibility for the development and treatment of their addictive disorder (Barnett et al., 2018a; Meurk et al., 2016; Morphett et al., 2017).
Taking the closely related Foucauldian perspective on the matter of power, Barnett's investigations showed that the BDMA not only questions agency by questioning autonomy but raises fears of a shift in ownership of expertise and delegitimizes practitioners’ and clients’ knowledge about addiction (Barnett & Fry, 2015; Barnett et al., 2018b). This may deprive people with addictions of their (often only) last resource—their personal life experiences with substance use and addiction. Barnett and Fry (2015, p. 278), are also two of the few researchers who recognized the importance of enquiring the relevance of the BDMA in the light of treatment “clients’ phenomenological experience of addiction”; but left this issue for future investigations. Answering to this call, the current study tested the interplay between scientific models and beliefs (cf. Helman, 1981), that is, how treatment clients interpret their addiction experiences. We do this without judging the latter or evaluating knowledge about the former. Instead, we consider the use and expression of the BDMA by any stakeholder—including the persons suffering from addiction—as “the sociocultural production and dissemination of the notion that the brain plays a role in addiction” (Hellman et al., 2022: p. 26). This is why, in the current study, we investigate addiction service's clients’ experiences with their recovery in the light of the BDMA. We ask what influence the BDMA has on clients’ perception of their autonomy and biography, and what role the BDMA plays in the recovery narratives of the subjects struggling with addiction.
Material, Method, and Analytical Approach
Eleven focus-groups were conducted with former and current clients of the Centre for Addiction and Mental Health (CAMH) in Toronto (Canada), in February 2019. A total of 69 participants (25 identifying as female and 44 as men) were between 24 and 79 years old and sought help for various addiction problems (e.g., alcohol, opioid, or gambling problems). Treatment for addictive disorders at CAMH focuses on prioritizing the medical and psychosocial needs of individuals with addictive disorders. Treatment programs are evidence-based and largely follow cognitive behavioral therapy and motivational enhancement therapy guidelines while also taking into account novel neuroscientific findings in the field. Participants were recruited with on-site advertisements, as well as actively contacting clients via the treatment center's patient database. Persons having received an assessment or treatment at CAMH for an addictive disorder (either current outpatient or former outpatient or inpatient), without prior history of psychosis or a developmental disorder, and were judged capable of understanding the elements of participation were eligible to partake in the focus-groups. The participants received $50 reimbursement for the participation in the focus-groups and gave informed written consent. The study received ethical approval from the Research Ethics Board at CAMH.
The focus-group followed the Reception Analytical Group Interview approach, thereby making use of discussion stimuli and letting the participants lead the discussion (Sulkunen & Egerer, 2009). The interview protocol was structured according to the following three topics: (1) Knowledge, Hopes, Beliefs, and BDMA specific questions, (2) Practice and Implementation, and (3) Policy Implications. The discussion stimuli were pictures and media statements related to neuroscientific addiction research (e.g., images of brain scans), and a small group task regarding functional magnetic resonance imaging. The protocol was complemented by four direct questions concerning the BDMA and responsibilities in addiction.
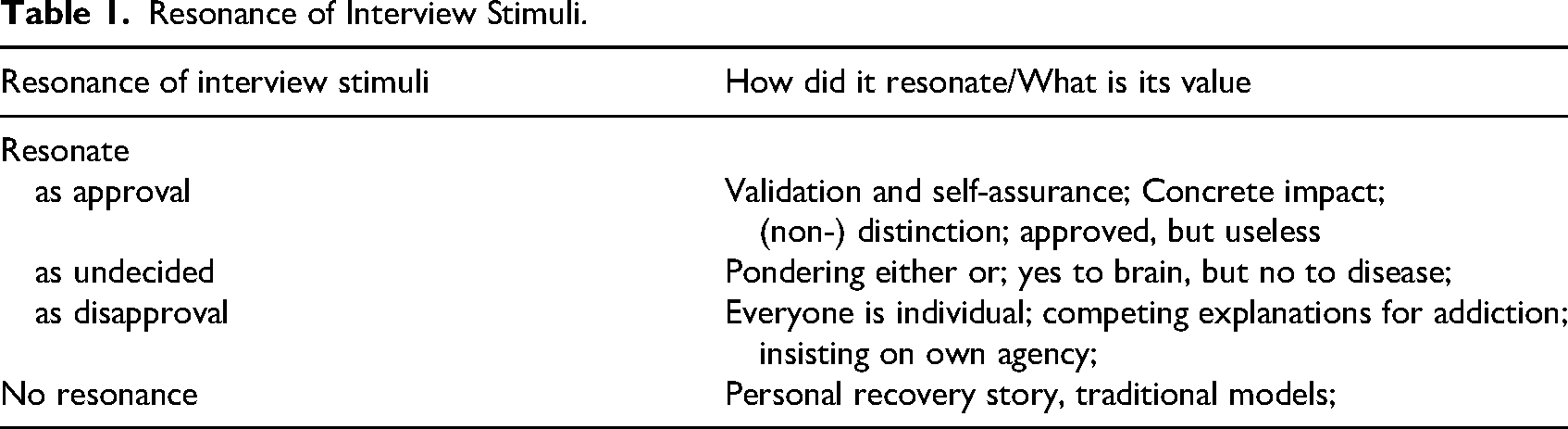
The interviews were transcribed verbatim and analyzed by the two authors (a sociologist and a psychologist) independently. For the analysis, we first indexed the data according to the topics addressed in the interview protocol (Deterding & Waters, 2018). Based on the indexing, our analysis followed-up the appearance of the BDMA in respondents’ discussions. Confronted with the conflict between their lay experiences and the assumptions of the BDMA (cf. Klingemann, 2011) we expected respondents to either agree and integrate the professional model or resist it (see also Netherland, 2011). Yet, we found more diverse reactions on how the respondents narrated their recovery in light of the BDMA. One could say that the BDMA resonated in the focus-group discussions: the participants incorporated the BDMA into their narrative by approval, disapproval, or pondering the pros and cons. There were also instances when the BDMA (offered in the form of the interview protocol) was not taken-up in the discussions, that is, the BDMA did not connect whatsoever to interviewees’ narratives (Table 1). This led us in the final step of our analysis to enquire the kind of the resonance of the BDMA in the focus-group discussions.
Resonance of Interview Stimuli.
Results
Resonate as Approval
In the interview discussions, elements of the BDMA were highlighted as being useful in a very concrete way. Respondents argued that the BDMA might reduce barriers to receiving support (e.g., from their health insurance) or tackling structural discrimination. The following quotation demonstrates how Amanda
1
experienced the autonomy-limiting framework of the BDMA as a resource in her job interviews: Amanda: (…) I mean, I went for a job interview recently and I have a criminal record and I told them like, this is where my addiction brought me to, I'm not that person anymore, so that was a good way to use addiction, to say like, “I’m not that person anymore, give me an opportunity to prove to you that I…”, you know, so I can use it in that aspect.” (Focus-group, No. 5) Peter: “As long as you have an addiction, people are going to have a negative attitude towards you, whatever you call it, if it's addiction, call it whatever you want, people hear that word addiction and you’re stigmatized.” (Focus-group, No. 2)
Working in the opposite direction, the distinction the respondents made between them and “normal” people helped construct their authentic self. The specific brain mechanisms involved in addiction were either interpreted as separating “normal” from “addicted” brains or as being proof that they are in fact not different from “the normies” (Focus-group, No. 7). The mechanisms are the same in all brains, which was experienced as comforting in making it possible to “heal” (Focus-group, No. 4). The question of “being normal” and becoming “normal” again, is a reoccurring theme in recovery stories (Anderson & Bondi, 1998; Koski-Jännes, 2002; McIntosh & McKeganey, 2000).
Finally, there were also instances when interviewees might have agreed with the premises of the BDMA, but at the same time questioned any added value for explaining addiction by brain mechanisms. In these cases, knowing what happens in the brain in relation to addiction was a nice novelty, but did not constitute real benefit for the persons in addiction treatment.
Resonate as Undecided
Taking an ambivalent stance on the BDMA became more obvious in the instances where the focus-group participants explicitly pondered not only about the usefulness of the BDMA and its explanatory power but when questioning the true value of the BDMA itself. They did not often discard the BDMA right away but instead looked at what corresponded to their own experience with addiction, and whatever did not align with the BDMA they deemed incorrect. Kyle: For me addiction… my addiction… I guess it's… [exhales in a struggle to find words]. Would I say it's a disease? I’ve had my addiction, yeah, I would say… I don’t know if it's a disease, I think it's, it's a… can I say it's a disease? I’ve had a problem with addiction since I was a little kid, can I say it's an addiction, it's something in my brain, can I define it as a disease? I think it's something, it's a chemical imbalance in the brain, for sure, there's some part of my brain that is wired this way and then it's fed and it's rewired and would I say it's a disease? I don’t know. (Focus-group, No. 3)
Resonate as Disapproval
Besides remaining ambivalent about the BDMA, persons in addiction treatment can also resist such a conceptualization of their problems (Carr, 2011; Netherland, 2011). Such active disapproval could also be observed in the present focus-groups. One way to challenge the assumptions voiced in the BDMA was referring to alternative explanations. Such explanations drew, for example, on social circumstances, psychological mechanisms, or genetics as different from brain mechanisms. Steve: I think the general consensus around the room is that the word “disease” is what's troubling everyone here [group agreement] Barbara: Yeah. I guess for me, I also don’t like “brain” exactly because I do feel like it is the emotion of stuff and the social stuff. There's lot of pieces. There's brain, and any behavioural thing obviously involves your brain and, our brains involve social and all the other stuff. (Focus-group, No. 2)
In the conversation, Steve and Barbara, not only identified the term disease in the BDMA as troublesome but Barbara highlighted the brain as being insufficient for explaining addiction. Instead, she lists different factors that relate to her addiction, and she has no problem adhering to different addiction models simultaneously (see also Room, 2005). The study participants also objected to the BDMA by insisting that everyone has a unique experience with addiction. A model like the BDMA would standardize all persons suffering from addiction, leaving no room for individuality or personal experiences. They insist that their own addiction story, the etiology of their addiction and their path to recovery, has been parts of their unique biography. Matt: Yeah but, you know what, it's your brain and your heart too, how you got to follow your heart too. It's not just the brain, it's the heart. You can have all the brain power in the world, but you don’t have the heart to stop, you’re not going to stop. (Focus-group, No. 6)
Furthermore, the respondents argued in a similar line with the critics of the BDMA (Heather et al., 2018). The BDMA, with its assumption of impaired autonomy, entails the risk of becoming a welcomed excuse to do anything about one's addiction problem. Matt's statement (quoted earlier) points out a general trait in the disapproving resonances of the BDMA: the importance of one's inner and individual consistent self in recovery (Downey et al., 2000; Koski-Jännes, 2002). The inner-self works beyond the brain's willpower and what would be normally referred to as the autonomous self. The people we interviewed viewed themselves as holistic human beings, which cannot be reduced to their brain and its mechanisms.
No Resonance
Finally, despite the direct questions regarding the BDMA and the BDMA-related stimuli in the interview protocol, the BDMA did not resonate with a considerable number of participants. In many cases, even when we explicitly asked about interviewees’ opinions on the BDMA, they discussed other traditional models of addiction or addressed their personal addiction experience without any reference to the brain and its mechanisms. Interviewer: Okay. Do you think that defining, umm, addiction as a brain disease is a good or bad way of defining addiction? Is there a time when this is a good or a bad definition? Alexander: It depends on how you look at it, because, like for me, for example, I grew up in an environment where it was a social thing. And then, from calling it social, it was like a need or an addiction, any way you wanna put it. And then I was dependent everyday, (…) I realized that, umm, I have to stay away from it because it's not good for me, and, it's just not good for me. I just have to cut it out of my life. (Focus-group, No. 11)
This missing resonance should not be confused with the open resistance to the model exemplified in the previous section. It rather demonstrates the strong persistence of a long-established conceptualization of addiction. It also shows that the BDMA doesn't connect with the respondents' own addiction experiences, their conceptualizations, and understanding of themselves. Alexander tells his story of addiction and his solutions, as he has probably done many times before. The BDMA does not offer him anything of value to rewrite (Hacking, 1995) his addiction biography.
Discussion
In this study, we investigated addiction service's clients’ experiences with their recovery in the light of the BDMA. While the current discourse on the pros and contras of the BDMA puts its emphasis on impaired autonomy and public stigma, the results of this study indicate a more complex picture.
In the argumentation for the virtues of the BDMA, the hijacked-brain (i.e., impaired autonomy) works in relieving one's responsibility for addiction and consequently reduces stigma (e.g., Leshner, 1997; Volkow et al., 2016). Although the BDMA seemed to have a role in reducing stigma in client's recovery stories, a different mechanism was at work. The focus-group participants indicated that the BDMA could reduce self-stigma, but was less successful at reducing public stigma. Whatever concept or label, they still feel stigmatized by society. Self-stigma instead concerns the internalization of negative public stigma on the self (Link & Phelan, 2001). The BDMA has offered a framework for personal validation in alleviating self-stigma in a retrospective acceptance of addiction. This echoes the successful recovery stage in Davies’ (1997) model, where the addiction problem is accepted, but assigned to the past.
Likewise, the results of this study also question some of the counterarguments about the BDMA (e.g., Heather et al., 2018, Lewis, 2017). Researchers in the field question the description of addiction as a hijacked-brain, on the grounds that this endangers a person's autonomy with a consequential loss of agency, stigmatization, and impaired help-seeking or treatment outcome. Yet, acknowledging that one suffered from a temporary loss of autonomy in the past, instead, makes it possible to create a consistent biography and secure one's agency in the present. This finding questions a simple dichotomization of health and disease common in universalistic addiction models (cf. Keane, 2001), by seeing agency also in its temporal dimension. Addiction realities are volatile and happen in “spatio-temporally specific encounters” (Fraser, 2020). The incorporation of one's past is also a crucial step in building a new, emergent identity (Koski-Jännes, 2002). Autonomy might be impaired due to alterations in the brain, but by referring to one's inner-self and constructing an authentic biography, the interviewed persons retain their overall agency.
Since Levine's paper on the conceptual changes of drunkenness (1978), the concept of addiction has been predominately discussed in social sciences as addressing the question of social control. The internalization of social control has been identified as the main factor in the concept of addiction and consequently, puts loss of control (i.e., loss of autonomy) at center stage. Yet, in late modernity, autonomy is only one of the two dimensions of agency. Agency is an attribution to persons, who demonstrate an independent course of life (Uusitalo & Egerer, 2024), irrespective of how restrained or unrestrained their life actually is (Woodman, 2009). The second dimension of agency is biography (Beck, 1986). Biography is not only to be constructed autonomously but also authentically. The late modern individual not only has the obligation to decide autonomously but also needs to have the right to be oneself in comparison to others (Sulkunen, 2009).
Overall, knowledge of the brain resonated in the focus-group discussions when participants discussed their personal narratives. The neuroscientific explanations and framework served as a symbolic resource to construct an authentic biography. It made it possible for participants to include one's addiction and make the distinction between who they were at heart and who they had been with their addiction (McIntosh & McKeganey, 2000). The disease model found in Alcoholics Anonymous has constituted this similar kind of symbolic resource before, thereby enabling individuals to extend their addiction identity with “in recovery” (Koski-Jännes, 2002).
We do not know if or when participants flipped a script on us (cf. Carr, 2011). They questioned the BDMA, when disapproving its claims but also reproduced the BDMA and utilized it while creating their addiction narratives. The case of nonresonance was therefore more ambivalent. For instance, while creating their addiction narratives, participants sometimes incorporated the BDMA but for others the BDMA did not align with their experiences with addiction and therefore did not become part of their identity in recovery (cf. Vitellone et al., 2022).
Keeping one's distinct self-consistent over time, and being rationally accountable for it are crucial in one's authentic biography. While we should not take the universality of rationality as given (Weinberg, 2022b), authenticity is a normative expectation and is at the core of agency creation in the context of late modernity (Beck, 1986). It is surprising that in addiction research, where recovery is one of the key issues, the question of biography has played a negligible role in discussing the virtues and flaws of the BDMA. Previous approaches developed addiction networks as transitory assemblages of human and nonhuman agents (e.g., Duff, 2014; Fraser et al., 2014), enlightening rather surprising interrelations in the creation of human freedom and autonomy. In comparison to autonomy, the concept of biography could broaden such networks in the temporal dimension, connecting the various agents and assemblages through time. Rose (2009) argues that we have entered the age of biopolitics, where the human brain is characterized rather by individual variety than abnormalities. Under such circumstances, society evaluates human agency less by immediate instances of autonomy, but by the consistent expression of agency over time. This includes retrospection of agency fluctuations in treatment client's life stories. We thus, urge addiction research to make use of agency in its entirety, and take both, autonomy and biography, into account.
The conclusions of this study are limited by the study sample. While the sample with 11 groups is itself a large dataset for a focus-group study, the participants all were, or have been, going through professional treatment. One also has to assume that persons in current particular distress with their addiction did not partake in the group interviews. Participants were also only recruited from one Canadian institution. Future studies are thus needed with persons outside professional treatment and in other contexts, especially outside the Anglo-Saxon world.
Footnotes
Acknowledgments
This study was funded by the European Research Area Network NEURON network's special call ELSA (No. 01GP1823). We would like to thank Brian Pereira and Dr. Christian Hendershot for their support in the data collection at CAMH.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the ERA-NET NEURON. Special Call ELSA (grant number NO. 01GP1823).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.