
Abstract
Ethnographers have long demonstrated that the design of spaces such as streets and city infrastructure can enable or prevent drug-using communities from practicing harm reduction and accessing life-saving services. Yet there is limited research about how spatial dynamics enable or hinder harm reduction workers' capacity to provide care and enact self-care. Addressing this gap, this article draws on ethnographic fieldwork at a community health center in Melbourne, Australia, which provided injecting equipment, public health education, and overdose response to a street-based population of people who injected heroin. To better understand how staff grappled with the complexities of providing care in this context, we pay particular attention to the spatial and material aspects of the service, focusing on a door and a window in the center building. Workers used these objects to draw professional boundaries and enact affective breaks, enabling them to cope with emotionally demanding work, provide a unique brand of relational care, and maintain their own well-being. These moral-spatial boundaries were also flexible and porous and had to be constantly renegotiated. We argue that paying attention to affective and spatial dynamics within a government-funded service reveals the inherent predicament faced by staff caring for a group that is considered radically “other” by the state.
Introduction
Critical drug scholars have long argued that to better understand the contexts of drug use—and by extension, service provision for people who use drugs—we must move beyond the well-documented structural dimensions toward a more localized, empirical attendance to space, embodiment, and practice (Duff, 2007; 2009; Vitellone, 2010). There is, for example, a tendency in academic literature to conceptualize harm reduction services as solely medically oriented interventions, while ignoring their social dimensions (Rance & Fraser, 2011). Redressing this blindspot, Rance and Fraser focused on diary entries from a medically supervised injecting center, finding that an “accidental intimacy” emerged through the workers' and clients' shared experience of injecting and overdose. More recent work has shown how such accidental intimacy can emerge even in the more strained relations between people who inject drugs and police (Selfridge et al., 2020). These studies emphasize that the relational dynamics of care are not ancillary to harm reduction services but are in fact integral (Dertadian & Yates, 2022).
In this paper, we seek to better understand relational care in harm reduction settings by paying particular attention to space. While acknowledging harm reduction is a movement enacted in multiple and often conflicting ways (Keane, 2003), we define harm reduction as a set of practices that aim to reduce the harms of drug use without pressing people who use drugs to reduce their consumption (Ritter & Cameron, 2005). Spaces, including streets and city infrastructure, have been shown to shape and constrain the capacity of drug-using communities to practice harm reduction and access life-saving services (Bardwell et al., 2018; Dilkes-Frayne, 2016; Malins et al., 2006). Moreover, Duncan et al. have urged researchers “to provide more sensitive accounts of the spatial, social and affective relations in which care is produced in [harm reduction] spaces” (2021, p. 643).
We respond to this call by examining how physical spaces shape both the relationships between workers and clients and the contours of care at a harm reduction service in Melbourne Australia. It was here that the first author, Andrew, conducted ethnographic fieldwork between 2016 and 2017. With approval from La Trobe University Human Research Ethics Committee (approval number HEC16-070), he volunteered at the service, undertook over 740 hours of participant observation, and conducted 39 interviews with staff, clients, and external stakeholders. Informed consent was provided by participants in both written and verbal forms, and the field ethnographer along with staff was actively engaging with client participants in an ongoing way to ensure they maintained awareness of the ethnographer's research activity. This paper is based on our analysis of the notes and interview transcripts arising from this fieldwork, which revealed the social life of a particular door and window in the center building. Both of these objects proved to be highly significant during fieldwork and became uniquely illustrative of the complexities of harm reduction work. Ultimately, we found that harm reduction workers used material and spatial elements of the care environment, both for deepening their relationships with clients and practicing relational care, but also for distancing and maintaining their own well-being in the face of an emotionally overwhelming role.
Background: Introducing Kirkby
The harm reduction service focused on in this paper was located in the neighborhood of Kirkby (a pseudonym), a suburb of Melbourne often referred to as a “hot spot” for public drug dealing and injecting. The service was nested in a broader community health center in the middle of a public housing estate: a grassed area bounded by multiple high-level and aging apartment towers. Workers saw hundreds of clients each day, providing a range of services including a Needle and Syringe Program (NSP), outreach, ad hoc nursing, harm reduction education and training, and mobile overdose response and after-care.
There were several features that made Kirkby a fertile ecology for a drug market: it was proximate to the CBD and easily accessible via public transport. It contained a labyrinth of backstreets and laneways, as well as large apartment buildings that made police raids unviable (Dalton and Rowe, 2004). Kirkby was also home to a large population of economically disadvantaged people and, anecdotally, local business owners known locally as traders capitalized in drug trafficking and sales. According to participants in this study, Kirkby heroin was understood to be both cheaper and of a higher quality than elsewhere in the state, which meant that buyers were prepared to travel long distances to obtain it.
Entrenched drug markets like Kirkby's have historically come hand-in-hand with an “everyday state of emergency” for people who use drugs (Bourgois & Schonberg, 2009). Since the drug war began (Zigon, 2019), people who use drugs have needed to be on the lookout for police, with whom relations have typically been hostile (Aitken et al., 2002; Fast et al., 2013; Moore, 2005; Park et al., 2019; Parkin, 2013; Small et al., 2006). Heroin's illegality meant that there was nowhere legitimate to inject it and avoiding arrest meant injecting in a hurry. As a result, injecting spaces—such as public bathrooms, laneways, or undercover car parks—were often unsanitary and unsupervised (Bourgois, 1998; Koester, 1994; Moore, 2004).
The Kirkby drug trade was frequently the topic of hyperbole in mainstream media and the target of intensive street-based police operations called “blitzes.” As found in other research, this both stemmed from and perpetuated the most extreme and defamatory stereotypes of heroin use (Reinarman & Duskin, 1999; Room, 2005; Scher et al., 2023).
Non-using Kirkby residents—especially those with children—were concerned about the visibility of dealing and injecting, and they pointed to the ubiquitous injection-related litter as symbolic of a community that had lost control. From time to time, Andrew witnessed residents entering Kirkby's health service in a fit of rage. On more than one occasion during fieldwork, they dumped a bag of injecting equipment collected from their yard or their apartment stairwells on the NSP counter—before storming out again. At other times, they would lambaste the team for providing the equipment that inevitably ended up scattered about the neighborhood. Other residents expressed frustration with the government's refusal to provide a supervised injecting facility, which left them as unpaid and untrained first responders to the overdoses they encountered on the street, in the laneways behind their houses, or in the bathroom of a favorite café. Meanwhile, traders articulated concern about the impact of an open drug market on their businesses or having to strategically prevent overdoses on their premises. Some paramedics expressed during fieldwork their moral indignation about people who use drugs, while others felt that a supervised injecting facility would be the only way to prevent the daily callouts.
Given these conflicting and emotive views about their existence, people who used drugs in Kirkby navigated a hostile terrain on a daily basis. In turn, the team at the Kirkby harm reduction service was constantly preoccupied with the relentless fallout. With such multiple and conflicting needs, Kirkby abounded with friction.
This friction was not unique to Kirkby. Around the globe, friction is a well-documented element of harm reduction work, where the status quo is often “a non-stop crisis” (Unachukwu et al., 2023). Harm reduction staff care for people with traumatic backgrounds and complex needs, on behalf of a state who otherwise tends to treat their clients as criminal and undeserving. Other scholars have noted that this inherent predicament can lead to value dissonance, in which employees feel a disconnect between their personal values and sense of responsibility and the constraints of the system they work within (Otterbein, 2022). On top of this, there is an increasing number of lived experience “peer workers”—those who use drugs while engaging in harm reduction work for their peers—for whom the precarities and high stakes of the work can be even more keenly felt (Greer et al., 2020). Harm reduction staff around the world report extremely high rates of job stress, vicarious trauma, and burnout (Butler et al., 2018; Unachukwu et al., 2023).
In response to these challenges, harm reduction workers often “establish boundaries” as a coping mechanism to “avoid the exhaustion” of investing in every client's complex needs (Otterbein, 2022). Boundaries are, therefore, crucial in harm reduction work. Yet there is a need for finer-grained ethnographic data—which we seek to address—of how professional boundaries are enacted in space, how spaces shape the establishment of boundaries, and how these dynamics shape the provision of care. We ask, what are the everyday ways in which boundaries are drawn and redrawn, respected, or breached in a harm reduction service? When do staff and clients mobilize together against outside forces, and when do boundaries become relevant between staff and clients? Asking these questions, we argue, provides rich insight into how frontline workers navigate moral ambiguity, maintain their own well-being and provide care for extremely vulnerable people.
Actor-Network Theory and Affect: A Theoretical and Methodological Framework
It is hard to theoretically capture the intensity of Kirkby's harm reduction service. Even on Andrew's first day at the service, he witnessed a stream of hardships. One client openly aired their grief about a brother's suicide. Another client was dismayed at the probable need to do “stupid things” to procure money for his next hit. A homeless client came in asking humbly for some soap. And yet, the place was energetic. In addition to sharing laughter and friendship with their clients, staff went to extraordinary lengths to offer emotional and practical help wherever possible, to extend solidarity (for example by advocating for clients in the face of police and neighbor hostility) and to shelter them from the hurtful stigma often directed at those who use drugs. Their core mission, it seemed, was to craft the center into a safe space in which clients could experience rare feelings of equality, respect, and holistic care. There was consequently a particularly special quality in the relationships between the workers and clients and in the overall atmosphere of the social space. This vivacity prompted us to ask the same question as that asked by ethnographer Anna Tsing: “How does a gathering become a ‘happening,’ that is, greater than the sum of its parts?” (2015, p. 27). Such a query lends itself to two conceptual tools we outline below: actor-network theory and affect.
Also described as a “sociology of associations” (Latour, 2005) actor-network theory (ANT) is a rich tradition emerging out of the sociological study of science in the late 1970s (e.g., Latour & Woolgar, 1979; Mol, 2010). It provides a set of methodological tools and sensibilities intended to decenter people, social structure, and culture as the primary foci of social research. In doing so, it conceptualizes all natural and social elements from a setting as “actors” on equal terms and encourages researchers to detail how these actors work together to form assemblages (or “actor-networks”) of significance. In this way, the actors impacting a harm reduction space are not only people who inject drugs, workers, police, and local residents, but also syringes, water taps, doors, and streets. Understanding these assemblages highlight the confluence of interrelated factors that lead to the heated conflicts in Kirkby.
Since ANT insists on analyses that do not distinguish between “social” and “natural” actors, it has been criticized for leading researchers away from the political and moral dimensions of the social settings being studied (Alcadipani & Hassard, 2010). Yet, in the words of Law and Singleton (2013), ANT “does not simply work in the world. It also works on it.” In fact, we argue that ANT is apt for studying politics and morality precisely because it enables us to trace the heterogeneous webs of interactions that compose them. Moreover, the political and moral dimensions of drug use and harm reduction can be well attended to through applying the concept of affect (see Duff, 2007; Vitellone, 2010). Related but not reducible to emotions (Blackman & Venn, 2010; Seyfert, 2012), affects are states of being that emerge through the encounters of multiple bodies (human and otherwise). For example, Bohling highlights the ways in which the assemblage of a nightclub—its particular blend of music, space, and sound (2014, p. 383)—shapes people's relationships to and decisions about drug-taking on any particular night. Duff (2009) also examined urban drug use contexts, finding that certain spaces were more amenable to fostering healthy relationships and “cultures of care” among people who use drugs than others. These spaces ultimately afforded “networks of social repair” which were “vital to the maintenance of health and well-being” in the drug-using community. The capacity of particular spaces to generate care relations was further examined by Duncan et al. (2021) who found that the social, affective, and material conditions of a drug consumption room in Germany “open up certain possibilities of care, just as they enhance, under certain conditions, capacities to enact it” (p. 642). These scholars highlight how attending to affect reveals the ways in which social qualities can be imbued in objects and spaces and, relatedly, how objects and spaces can evoke emotional, moral, and political responses, all of which can foster or hinder caring relations in harm reduction settings.
We can see affective qualities at play in the drug scene in Kirkby. Once there was a law in place prohibiting heroin, anyone who used the drug became part of the social body affectable by the enactment of such a law, which in turn altered the affective potential of the police. Time and, again, fieldwork illustrated that the simple presence of police at overdoses—even when there was no outward sign of hostility—was enough to instill fear and unleash a range of risks for people who used drugs, including heightened likelihood of violent conflicts, dangerous injecting practices, illness, and death. One worker, Jacquie, put it simply: the police “[don't] know the power of their uniforms” (Fieldnotes, June 20, 2017). Affects thus arise between bodies mutually but not symmetrically and can have significantly unequal effects.
Through thick description of social life at Kirkby Health, this article draws on the lenses of ANT and affect to better understand the modes of care and professional boundaries practiced by harm reduction workers. As we illustrate below, these dynamics were rendered visible by a particular door and window.
The Door
The team at Kirkby often described their clients as those “who come through the door,” signifying that the door itself was a significant part of the service. Found at C1 in the floor plan in Figure 1, this was the clients' door to their own space.
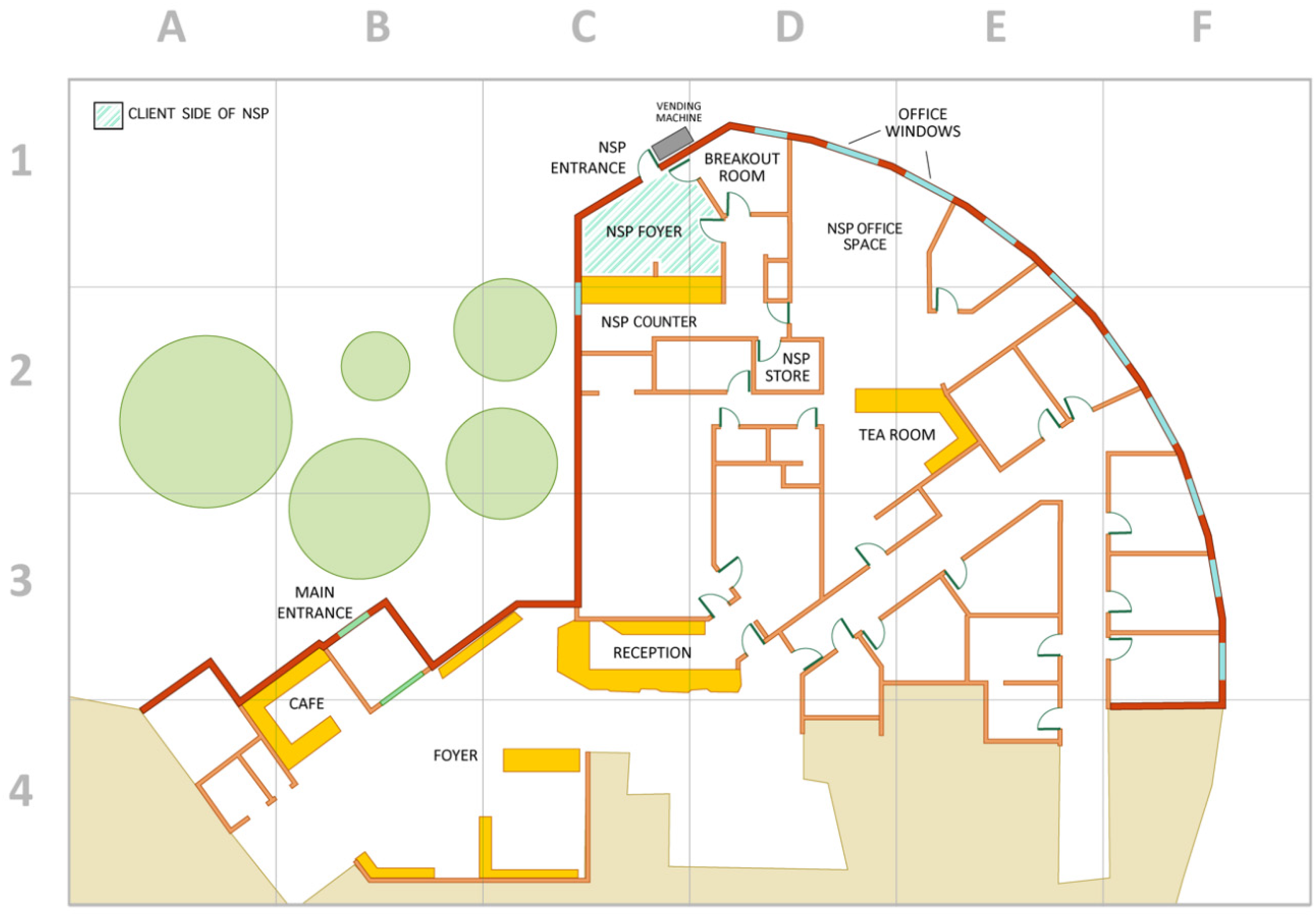
Floor map of Kirkby Health, recreated from the original floor plans (Illustration Credit: Yiyi Wang 2021).
The door was a relatively new feature of the service. The first incarnation of drug-related services at Kirkby was a simple Needle and Syringe Program (NSP), in which general reception staff at the community health center dispensed injecting equipment across the counter. Yet when Kirkby's drug scene intensified due to a nearby street-based market being displaced, a dedicated NSP service was necessary, as explained by the CEO, Felix: Because of the sheer volumes [of people using the NSP service] - it was just becoming chaotic in our waiting room – we had to provide a separate entrance. So, we built a little room with its own doorway and that became [our] first NSP that was not over the [reception] counter. (Interview, October 21, 2017)
When clientele increased again, the staff successfully rallied for a purpose-built NSP which featured its own entrance from the outside.
Many clients appreciated how the drug service was segregated from general health service-provision at the center. For Todd, it reduced the visibility of his stigmatized identity. Now in his 50s, Todd's height, clothing, gait, and overall manner continued to reflect his reputation as a tough guy. As with many drug scenes, street-oriented demeanors can facilitate success in the informal drug economy, signaling danger to those both inside and outside of it (Bourgois, 1995). From Todd's perspective, “you get respect by people likin’ you, and by people [being] scared’a you” (Interview, June 14, 2017). Moreover, some of the staff at the center, such as the manager Ash, sought Todd's friendship precisely because of the protection he—and his image—afforded them in the drug scene, which in turn helped them do their job. And yet, while appearing dangerous may have had its benefits in the unruly backstreets of Kirkby, this was not the case when they shared the health center with the general public:
Back then, we'd have to go inside where the [regular] people are, when you'd get the fits [syringes] and that, people sees everything, and it was small. We now feel the change, when people come [into the health centre] they don't see nothing. People don't see much what's happening in here […]
So, you prefer having your own door to the NSP?
Yeah … Just for the sake of the other people that don't come here for it, so they don't get scared […] I can just see it in their eyes, you know? [He hesitates] People don't know me, they only know what they see, until they get to know me […] obviously I must look fuckin' scary because a lot of people, sort of, back away with me, you know? […]
And that bothers you?
Of course. You know? ‘Cos I'm not doin’ nothing to you man. You don't know anything about me so don't fuckin' judge me when you don't even know me. You know? But then when an actual person get to know me, I'm fuckin alright you know?
Yep.
So don't judge people unless you fuckin' know who they are.
And you can avoid that kind of thing by coming in here?
Yeah. (Interview, June 14, 2017)
Todd made it clear that having people react to one's presence with fear was a distressing experience that clients would rather avoid, which was enabled through having their own door.
Holly, a worker who also had lived experience of drug use, was more equivocal about the merits of a separate space: It's a bit of a catch 22 that one. I've been to services where it's not a separate entrance […] You walk in and you've got to ask the receptionist for injecting equipment in front of the whole waiting room. Not so cool. But then it is, on the flip side it's like ‘oh, that's where they go’ […] So, it's hard, because I like having our own space. […] The clients feel safer. They know that in this section they will be treated fine, they're not going to have any dramas, they know that if they need to go next door to the health centre that we'll help them out, if they're not comfortable doing it themselves, so we can advocate on their behalf […] they know that no matter what, they can come here. So you get people that have just been stabbed and they come here before they come to the medical area because they know, I mean, they know that we're going to take them around to the medical area anyway, but they know it's us that are going to do it. You know, they're not just going to be confronted with some receptionist that's going to freak out because they're bleeding from the neck, or whatever it is. Yeah. So I think the benefits outweigh the stigmatising thing. I think. (Interview, October 17, 2017)
We can see here that having a segregated space enabled the team to create and maintain an alternative and egalitarian social setting that shielded clients from hurtful attitudes and treatment from the world outside. When team members escorted their clients across to the main center as required, they were crossing over from one kind of social space to another, adding perceived legitimacy to their usually marginalized clients, and therefore making this transition smoother for them.
However, the therapeutic possibilities of having a designated door were somewhat hindered by its controversial auto-locking design. This meant that staff needed to approve each client's entry by pressing a button beneath the counter to unlock the door.
On one level, the lock sent the message that clients were inherently untrustworthy. To counteract this, NSP workers tried to anticipate clients' needs by seeing them approach through a glass panel on the door and pressing the button even before they reached it. This enabled the door to open seamlessly for the client as though it was never locked. NSP workers would often successfully juggle this task while simultaneously packing bags of syringes, having conversations, restocking supplies, or entering transaction statistics. Yet when they were unable to, this often led to miscommunications through the glass, banging on the door outside and tense interactions. The situation frustrated workers and agitated clients.
However, the team was unable to reach a consensus about the problems that arose due to the auto-locking door. They were keenly aware that some clients were dangerous and could be unpredictable. This presented them with a dilemma, where the very entrance to their shared space was seen to undermine the core of their mission. This was emphasized by Holly: The NSP door has always been a contentious issue. […] There's some on the team that think, ‘no, it should be locked, it's a security precaution.’ Whereas, I know some of us, we look at it from, [she speaks slower] ‘yeah, but you're locking people out of another place.’ (Interview, October 17, 2017)
Nicky similarly raised this tension:
It's quite hard to admit that […] we'd say that we don't stigmatise people, we don't discriminate, but we've definitely got some structural issues …
And do you have any examples of the structural things here?
The electronic door. That fuckin' door. Yep. And all the other doors. We've got as many barriers […] ‘Keep them on that side because they can't be trusted.’ (Interview, February 27, 2018)
The dilemma was that in trying to mitigate risk and attend to their own safety, the team was sending a clear message to their clients that replicated the negative experiences they experienced elsewhere: marginalization from public spaces and being stereotyped as inherently risky. This was counter to the egalitarian vision that the team was trying to achieve within the space.
Space, Boundaries and Uneasy Control
Tensions over the auto-locking door heightened one day in 2017 when the door handle broke. The door became unopenable from outside which meant it had to remain ajar for service to continue. As it was a cold winter's day, the space became unbearably cold, and the door frequently slammed in gusts of wind.
Although frustrating, the open door did not seem to create any more problems than usual. Eager to capitalize on the opportunity, Nicky appealed to keep it this way, arguing that the team would still be safe and the clients happier, if they reversed the locking function. That is, instead of locking by default and opening with a button, it would remain open by default and lock with a button.
However, Nicky and other sympathizers knew that their newly promoted manager, Ash, who was currently on leave, would be opposed. While Ash was just as compassionate toward clients as the rest of the team, her opposition to a less-secure, unlocked door came from her own embodied experiences. This related to one particular client, Mike. Approximately ten years previously, Mike had forced his way behind the NSP counter and demanded $100 from Ash, threatening her with a used syringe. Ash told him to “get fucked” and leave, after which she called the police. Without telling Ash, the police charged Mike with attempted armed robbery. Sometime later, Mike came to the center asking for Ash. Upon being told she was not in, he revealed a pair of scissors strapped to his body and said that he had come to stab her with them. When this was relayed to Ash, she took out a restraining order against him. Since then, she had seen very little of Mike, and other clients reported that he was incarcerated for much of that time.
The door handle coincidentally broke soon after Mike had begun frequenting Kirkby again. The team considered Mike to be extremely mentally unwell. They were concerned not only about Mike's potential for violence toward staff but also the potential for violent interactions between Mike and some of the other clients, who were fiercely protective of the Ash, particularly her Indigenous friends.
Throughout Andrew's time at Kirkby, he had not seen anything like the range or extent of measures used against a client as happened with Mike. It was agreed that Ash would not conduct outreach while he was likely in the neighborhood. The team refused to unlock the door if Mike was attempting entry, leaving some clients temporarily stuck inside or out. Further, the team took the unusual step of proactively seeking police aid to help move Mike on and considered installing a CCTV camera overlooking the vending machine, a current blindspot. Ash once said very calmly: “[Mike is] just one of those people who you know the world would be better off without” (Fieldnotes, March 28, 2017). Erin later asked: “so if he was out there overdosing you wouldn't administer naloxone to him?” Ash replied, “No. Definitely not.” This was a tellingly intense statement from Ash, given her abhorrence of harsh attitudes toward people who use drugs. The team eventually decided Mike would be “banned for life” and put measures in place to enforce the ban.
The controversy over Mike and the question of reinstating the broken lock highlighted a moral tension—whether to allow one dangerous client to become representative of the entire client body. The team was acutely aware of the ways in which generalizations about people who use drugs are promulgated through mainstream media, drug policy, law, and everyday conversation. These discourses draw upon caricatures, partial information, problematic assumptions, and notable omissions which have spun into discriminatory stereotypes and draconian responses (Reinarman & Duskin, 1999; Selseng, 2017; Swalve & DeFoster, 2016). Moreover, harm reduction workers can struggle to navigate the tensions in sector understandings of their clients as either lacking in a range of standard capacities and attributes, or conversely as “competent citizens struggling to cope with material disadvantage” (Moore, 2009). To more faithfully understand and engage with their clients, the Kirkby team deliberately sought to avoid jumping to conclusions about them, instead trying to make judgments solely upon what they knew through their immediate, embodied experience.
Team members were, for example, commonly empathizing with clients about their experiences of discrimination outside, decrying these structural inequalities as deplorable. Staff would regularly express outrage about how their clients were treated by security guards and regularly denied entry to local supermarkets. The team's issue was not that their clients never stole—in fact, many admitted to doing so. It was rather how the actions of some became essentialized as characteristic of a population, and in turn, every member of that group became subject to spatial authority and control (a process that has been at the heart of drug stigmatization from its earliest days [Hickman, 2000]). Moreover, this kind of spatial treatment produces a certain kind of subject. For example, Fraser (2006) highlighted how the spatial and temporal aspects of queues at methadone clinics work to reproduce the same kinds of disorderly subjects that the programs purported to address. This too was part of the team's discomfort over the auto-locking door. Beyond simply the “message” sent by the lock, the team was concerned that ongoing daily disruptions to the process of entering reproduced the kind of distrusted subject that clients were presumed to be elsewhere.
On her return from leave, Ash quashed the notion of trialing an unlocked door. The controversy, however, remained. These tensions over the auto-locking door—heightened by Mike's presence—showed that the team was unlikely to overcome the moral and social ambiguities that were inherent to their role at Kirkby Health. However, they were forced to navigate them on an everyday basis and did so guided by an ethical orientation that prioritized embodied evidence, complexity, and care. These were similarly highlighted by their engagement with the window.
The Window
It's 9:25am and Izzy opens the blinds on the window. ‘Welcome world’ she says to no one in particular. (Fieldnotes, October 3, 2017)
The NSP workers mostly loved their job but the many demands, intermittent chaos, and sheer intensity of it all could be overwhelming. They would often share the NSP space with up to a dozen or so clients and were on call to attend to each rap at the door. Workers braced themselves for the onslaught of activity—enjoyable or otherwise—which arrived in an irregular rhythm.
The team's office, however, was in many ways a sanctuary, providing some shielding from the intensity of local happenings. Located at D1, D2, E1, and E2 of the floor map, it was also a place for planning, strategizing, chipping away at projects, banter, venting, jokes, and storytelling. There were two windows in the office—one on the drug and alcohol program side of desks and another on the social workers' side (see D1-E1 of Figure 1)— which were both tall and wide. They gave a sweeping view of the landscape outside the center, which included several large, grassed areas on the way to a busy street, bookended by two apartment buildings, a slice of the multi-deck carpark to the far right, and many passersby on foot, traveling to and from Kirkby Health's various programs. This section of the article examines how the team engaged with “the window,” as they singularly called it. We find they variously used it to maintain connections with—and separations from—the broader neighborhood and their clients.
A Connection to Outside “I like to see what's coming at me” (what's rather than what is)
Much of the team's work extended out into the community. This ranged from official duties from their job description, such as outreach and mobile overdose response, to more impromptu moments in which, for example, Izzy, the nurse attended to wounds on a park bench, or team members socialized with clients through sharing and smoking cigarettes in small companionable circles. Because their work involved so much blurring, shifting, or dissolving of commonplace barriers, even the work they did from the safety of their office required an ongoing connection to the outside. The window was their main avenue for this connection.
The visible information afforded by the window was critically important to the team. For example, Andrew was admonished one day when he forgot to re-raise the blind after he had closed it to gather some interview funds. “I like to see what's coming at me, Andrew!” Izzy said in her playful-yet-serious tone. “I get uncomfortable when I can't see what's coming at me!” (Fieldnotes, June 14, 2017). What was “coming at” the team could be something immediate, like clients running into the service to find a worker who could attend an overdose. At other times, they could spot a client who they had been trying to catch all week. Or it could alert them to police presence in the public housing grounds. Often it provided more subtle perceptions of how the area felt. Were people on edge? Were they in a playful mood? As Erin asked one day, “what's with all this blasé dealing today?” (Fieldnotes, March 2, 2017). Depending on such impressions, the team would either brace themselves a little harder as if the sky indicated a gale approaching or sink a little more comfortably in their chairs, hopeful that their senses were not deceiving them.
The team discussed, speculated, and acted upon what they were seeing through the window. On one occasion, for example, the team witnessed a drug deal between two clients directly outside the service, who did not know they were being observed. The team watched on through the window, expressing amusement at their brazenness. Eventually one of the workers knocked on the window, and the clients jumped, startled. The team members in the office cackled with laughter. The clients similarly laughed at themselves once their initial shock had subsided. A visiting rehab worker from an external organization who watched this scenario along with the team was awestruck. Holly, however, remained nonchalant. She turned from the computer and shrugged her shoulders as if to say “this is Kirkby, what do you expect?” After this interaction, however, Erin went out to the client and told him to deal elsewhere.
Thus, the team brought the window into their employ as one of the many tools required to do their job. This window revealed itself to be unique in the way that it both acted as a boundary and facilitated an ongoing connection—a practice we refer to as moving between “affective registers.”
Shifting Affective Registers and Taking Affective Breaks
The team used the window to create temporal breaks through which they affectively connected and disconnected themselves from the community and sometimes their clients.
The team's workday began before they opened their doors to the public, when one or two of them “swept” the immediate surrounds for discarded needles and other injecting paraphernalia. There was plenty of chit-chat, emails were sent, plans made, and there might be time for a cigarette. At this stage, the blinds on the window were still closed. This was a transitional period between their outside lives and the harm reduction community. The blinds were opened only when it was time to turn off the syringe vending machine—relieving it of its duty for the night—and the team allowed clients into the NSP proper. The importance of this ritual act was made clear when Ash inadvertently opened the blinds early one day, but then apologized to the others for “letting the world in” before 9:30am.
Commencing work entailed a shift in the team's affective register, a state of being that they experienced collectively, even as it was not exactly the same from person to person or day to day. As explained earlier, affects are experienced in and transmitted through bodies. Affective relations can bring smaller bodies together into larger ones or divide bodies into smaller ones. As the team members came into Kirkby and began their workday, they were enrolled as part of the team, thereby entering into affective relations with the clients, residents, and syringes on the ground in ways that they were not, prior to entering this arena. This altered their constitution in terms of how they felt and acted. A body's affective register is the constellation of affects we might call a state of being which is dynamically working in “a circuit of feeling and response” (Hemmings, 2005, p. 552) with everything else around it. Ash referred to it as a “rhythm,” “a headspace” (Fieldnotes, April 4, 2017). The daily shift in the team's affective register was significant enough that it required a period of transition, which they ritualistically performed with the opening and closing of the blinds.
The clients came and went throughout the day like a tide. Through weathering these ongoing movements, the team underwent personal and collective transformations. While they sometimes thrived on the local energy, the workers were also acutely aware that it took a toll on them as illustrated in these excerpts: We're chatting away in the office and the conversation shifts towards what it ‘means’ to work here. Izzy says, ‘it's like a form of self-harm except instead of physical it's mental.’ Erin adds, ‘you have to be a bit coo-coo’. John (a social worker) says it's ‘masochistic’. Everyone is laughing all the while. (Fieldnotes, July 12, 2017) I tell Jacquie that this place seems to be characterised by struggle. For the clients, but also the workers. She agrees. Among other things she's told Felix (the CEO) that the program is ‘unsustainable’. When I ask what she means by this she mainly speaks about the toll this work takes on the team. She says, ‘you can't live with adrenaline going…’ and waves her finger up and down in the air like a polygraph needle. (Fieldnotes, July 18, 2017)
The arduousness of this constant connectivity necessitated moments of respite. The team used the insulation afforded by the window for another purpose: to create affective breaks between themselves and the clients. These were brief, punctuated moments throughout the day where their connection with the clients was disrupted, leaving the team feeling as though they were separate. Often this involved simple distancing, as when team members spent quiet moments staring out the window: Izzy stands at the window watching a heavily drug-affected client and having a chuckle. ‘Ah Gracie, you're as wobbly as hell’ she says to herself, in a similar way as a mum seeing their child with ice cream all over their face. (Fieldnotes, May 5, 2017)
While the team often collectively observed and commented upon scenes through the window that they found entertaining, they would always head out immediately to tend to clients when needed.
Although it was not always possible to remove themselves from the everyday urgency of Kirkby, the office provided an insulated space and enabled them brief respite. Here, they could speak openly about clients with each other without fear of being heard; they could muse and vent. However, these affective breaks that the team craved were precarious and could be punctured or dissolved at any moment. This precarity became highly visible when the team instituted a peer program within their service.
Peers, Professional Boundaries, and the Relational Power of Humor
As state government attention toward public injecting “hot spots” increased, the team became involved in a state-funded initiative to recruit peer workers in NSPs. In their usual manner of trying to correct the injustices suffered by their clients in mainstream social settings, the team tailored the job to be extra inclusive. They did so by: naming the position “community development worker” (CDW) over the more common “peer worker”; stating in the position description that reading and writing were “preferred but not essential”; and only screening criminal records for extreme incidences that involved risks to people's safety, rather than assuming moral failings for petty crimes. Further, although it was understood that CDWs would likely be active heroin users, the only stipulation around drug use was that they could not arrive at work “smashed” as this would affect their capacity to work. Dealers were welcome to apply to be CDWs, but they would not be allowed to deal at work.
The team also sought to prevent negative attitudes from general Kirkby Health staff toward this new intake of peer colleagues. As Ash said, “you can't hide those kinds of reactions” and it would likely make the CDWs feel uncomfortable and unwelcome. She therefore wrote an email to be sent out to staff center-wide. CDWs were going to be provided with swipe cards, desks, and user accounts on their network. In sum, the team's development and implementation of the peer program mirrored their overall approach of providing social legitimacy and equality to people who were commonly considered incapable of positively contributing.
It was not until the eve of the peer program that the team realized a significant issue. That is, by bringing a selection of clients into their usually secluded staff-only space, their ability to create affective breaks would be compromised. As Ash stated firmly during one meeting, “our communication style has to change.” This meant refraining from overtly expressing frustrations or openly discussing clients’ names or details. (From then on, such communications needed to be limited to the team's group email list.) Moreover, Ash said, they needed to stop “taking the piss out of clients,” while affirming that “this is our humour.” Erin quickly jumped in, “and our coping mechanism!” Ash felt the team's jokes could be “taken the wrong way” and considered offensive.
To understand the broader implications of this new rule, it is first necessary to explore the role of humor at the service in more depth, as it was particularly illustrative of the team-client relationship. As Andrew noted in his fieldnotes: Ash explains that many people wouldn't get the team's sense of humour, but it's necessary to cope. She then tells a story about herself and Nicky in the parking lot one day attending an overdose. The situation was under control and they were waiting for Jacquie. While waiting, the two of them began ‘dancing like idiots,’ and it would've looked terrible to onlookers, but these are just the things you do to get by. You keep it absurd. (April 4, 2017)
The role of humor in the team-client relationship was multifaceted, as hinted at in Ash's story above. The first aspect of this is well-known among people in tough lines of work: it functions as a coping mechanism. The humor of psychiatric nurses in Gannon's (2021) study was best characterized as a kind of “getting on” in the face of a “grim reality.” Secondly, as in O’Neill's (1983, p. 154) work, black humor is “the humour of lost norms, lost confidence, the humour of disorientation.” In other words, humor enabled the Kirkby team to reconcile (or cope with the irreconcilability of) the inner world of the NSP and the outside world. “Absurdity” in Ash's words was a way of seeing this cognitive dissonance in a humorous light.
However, there is also a third dimension to the use of humor, here, outlined by the team in this research. Similar to research by Carty and Musharbash (2008), humor can function as boundary-work, a practice of including some while excluding others (see Carty & Musharbash, 2008). At Kirkby Health, the team engaged humor to enact solidarity with the clients and distance themselves from the mainstream public in Kirkby. In the anecdote above, both overdosing in public and “dancing like idiots” as a response to overdosing were not commonplace public behavior. Ash and Nicky performed a radical act of inclusion by dancing alongside the unconscious client, in contrast to the neglect, hostility, and disgust overdosed bodies engender in the broader neighborhood. The silly dancing was incongruous with the tragedy of overdose, creating a brief window in which the tragedy was temporarily relieved from their momentary experience. As Lacan (in Newirth, 2006) noted, comedy is a means to affirm life even in the most tragic of circumstances. In this way, comedy can be “liberating” because moments of humor can displace something once viewed as vastly important and make it feel trivial (Freud, 1928).
The clients similarly joked in ways that conjoined them with the workers, while affectively distancing them from their ongoing struggles. For instance, one day when about seven clients were buzzing around, Izzy walked in and cheerfully addressed the room: “What's going down everyone?” Bruce, a client, responded immediately: “Hopefully not us!” and everyone laughed. Because the clients “dropped” (overdosed) frequently—and the workers were frequent responders—this kind of black humor brought them together through shared experiences and enabled them temporary relief from shared hardships.
However, humor also raised the recurring tension for workers between the need for both solidarity with, and space from, their clients. Often enacted at the window, humor was an integral part of bearing through this tension. On one occasion, for example, an aggressive client shouted at Olivia, “You've got too much teeth in your fucking head!”, before turning towards Jacquie and shouting again, “what are you fuckin' smiling at!?” During the team's debrief about this at the window, everyone was able to laugh at this unpleasant interaction. Olivia joked “we need to start a book!” adding in a distinguished voice “a book of wisdom.”
The team's sense of humor thus enabled them to manage the daily challenges they experienced with clients. On one level, laughing at someone can enhance sociality among the joking group (Beckett, 2008). However, simultaneous joking at the expense of others also brings to the fore underlying elements of the relationship patterns at play (Douglas, 1968). Joking habits here were a means to bear the simultaneous “social conjunction and social disjunction” of two parties (Radcliffe-Brown, 1940, p. 196). Due to the overwhelming burden endured by the team, and the already stigmatized position of the clients just beyond the confines of the office, being able to laugh about them was critical to maintaining the relationship. Yet, to not cause offence, the clients had to be absent for the joking, while never too far away. These joking practices helped to stabilize the relationship and the structure of the service.
As such, when the structure was changed to allow the clients (outside) to become peers (inside), so too the issue of joking needed to be addressed. Ash told the team that they would need to “pull each other into line” noting that it was also going to be difficult for herself: “we've been doing it for so long and it's just so ingrained” (Fieldnotes, October 10, 2017). The challenges of refraining from this form of humor were already evident later that day. The staff were laughing about Janice, a client, who had recently begun flirting with Will, an NSP worker. Janice had been in the NSP earlier that day talking about jumping the counter and “raping him.” Holly re-enacted herself blurting out, “Janice, that's not ok!” to which everyone laughed and shared other stories of clients being inappropriate. Ash interjected in the conversation by saying, “I'm going to let this conversation continue, but only because our new [peer] staff aren't here” (Fieldnotes, October 10, 2017).
Used as boundary-work, staff humor created similar tensions as the auto-locking door. The team aimed to create an unusually compassionate and caring space in which people who used drugs were treated as normal people, as flawed as everyone else. Yet, when the team attempted to most fully enact this aim by welcoming clients as co-workers, it compromised their own needs for professional boundaries. Further, while they were acutely reflexive about the emotional toll of working with a client-base with such complex needs, they did not want to reproduce the mainstream construction of them as a burden. Thus, even as the team was concerned that their humor may be “taken the wrong way,” their joking was part of their egalitarian project. This approach is comparable to that observed in Dean and Gregory's (2004, p. 146) ethnographic study of humor in a palliative care setting, in which humor “enhance[d] the humanity of the experience.” What the Kirkby case study illustrates is that this therapeutic form of humor—as both professional coping mechanism and effort to enhance the humanity of their encounters with clients—was enabled through particular spatial and material arrangements.
In sum, the window was an integral part of the architecture that allowed the team the space and material for their radical brand of care. They ritualized the day's beginning with opening the window blinds as a symbolic and actual way of connecting with their clients and Kirkby as a whole. Enabling them both forewarning and a shield, the window allowed them to periodically divest themselves of the ongoing tragedy.
Similarly, they ritualistically closed the window blinds at the end of the day. There was a protocol to this: the blinds needed to remain open as long as they were engaging with clients and be closed only once it was time to leave the black, stout needle and syringe vending machine to carry on the bare minimum of their work until they returned in the morning. This closing ritual was captured neatly in the fieldnotes when Izzy scolded a social worker one day as he went to draw the blinds down early:
‘No don't shut them! Don't shut Kirkby out! I'm not ready for no craziness!’
‘lock her up!’
‘It's 5 o'clock? Ok, lock her up!’
referring to the syringe vending machine outside: ‘Is the big boy on?’
‘The big boy's on.’ (Fieldnotes, October 10, 2017).
Conclusion
Paying close attention to the spatial, material, and affective dimensions of a health service for people who inject heroin in Melbourne, Australia, has revealed unique insights into what enables and hinders relational care in harm reduction spaces.
Our case study confirms earlier research that certain spatial, material, and affective assemblages create the conditions for intimacy between workers and people who use drugs, which can ultimately have a positive effect on well-being and assist in achieving harm reduction objectives (Duncan et al., 2021; Rance & Fraser, 2011).
Going further, our analysis makes two important contributions to the critical drug studies literature. First, we find that, for the Kirkby workers at least, these intimacies were far more complex than simply being “accidental.” Workers deliberately nurtured intimate, caring relationships as a way of strategically addressing the stigma and exclusion that was usually experienced by their severely marginalized clients. The existence of a separate harm reduction service with a separate entry afforded them space to create an unusual atmosphere of respect and egalitarianism—albeit one that was in a constant dialectic with the outside world. While crucial to care, these affective assemblages also enrolled the staff into the clients' everyday emergencies, including situations in which the clients presented dangers to staff well-being. To minimize the value dissonance created by such moral ambiguities (Otterbein, 2022), it was crucial that the team had the space to periodically divest themselves of the emotionally overwhelming work.
Our second contribution is to highlight the ways in which harm reduction workers strategically used boundaries (both material and metaphorical barriers) in order to maximize their ability to practice relational care. In the Kirkby case, this was illustrated through the contested use of the door (and its lock), the window (and its blinds), and a morbid sense of humor. These enabled the workers to alternate between fostering closeness with clients and temporarily disentangling themselves from the drama. Moreover, these boundaries were porous, flexible, and constantly renegotiated. Understanding how these boundaries operated revealed both the extent of human connection and the periodic distance that are required to achieve locally effective harm reduction.
Through combining ANT and affect theory, we have shown the necessity of attending to architecture and physical space as relationships and boundaries are made and evolve between workers and clients. This process is dynamic and dialogical (Müller & Schurr, 2016), as the arrangements of physical space shape how boundaries and relationships develop, just as the desires of the groups involved—such as the harm reduction ethos of the team as they seek to create an egalitarian social space—shape how the space is arranged and used.
Given the high rates of stress, burnout, and high turnover that characterizes the harm reduction sector, this case study suggests that spaces that are consultatively designed and able to adapt to the (changing) needs of staff and clients may facilitate crucial flexibility in how boundaries are negotiated and ultimately improve safety, well-being, and the capacity for care.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a La Trobe University Postgraduate Research Scholarship).