
Abstract
Intrigued by the overwhelmingly positive response to the needle and syringe exchange program (NSP) by people who inject drugs in Stockholm, this article sought to untangle harm reduction in a prohibitionist drug policy context. The article drew on assemblage thinking and used semistructured individual interviews with 32 people who inject drugs, and three focus groups with staff at the Stockholm NSP. The aim was to dissect harm reduction in the form of NSP and how it worked to move people who inject drugs towards or away from drug-related harm. The analysis identified how bodies such as the NSP regulations, the setting, and stigma gathered in ways that reduced the capacity to move forward and enroll, as the inclusion of the NSP in the assemblage would decrease the capacity to uphold other connections considered to be more important. Regular NSP visitors however described how free injecting equipment, staff care, continuity, and trust were important objects that gathered in ways opening up for movement towards less harm. Fiercely, these profoundly caring experiences at the NSP could also block new becomings and moves forward as people who inject drugs, discouraged from previous negative experiences of other service providers and structural stigma, refrained from other connections that could improve their wellbeing. They risked becoming locked in at the NSP and similar services. A significant consequence of the agential cuts of us researchers, the staff, and policymakers alike, targeting primarily those that do access and benefit from harm-reducing interventions, is that alternative solutions embracing also those locked out and locked in become unimaginable.
Keywords
Introduction
In a research project on risks of injection drug use (IDU) in Sweden, we interviewed people who inject drugs about their lives, and explored how risks and harms were understood by both people who inject drugs and professionals. The recruitment primarily took place at the two permanent facilities of the Stockholm needle and syringe exchange program (NSP)—the only official NSP in the region. Peter was the first patient we met in the waiting room, and he kindly agreed to an interview. When asked about his experience of coming to the NSP, he said: The best thing about “the change” is that they are so freaking nice. The first time I was here, I was shocked. I was just like, ‘they were so nice!’ I wasn’t used to that.
What we came to learn in the following interviews was that Peter's narrative about “the change” (the NSP) was not unique. Similar stories were shared in almost every interview. Visitors stated that not only were the NSP staff professional in that they managed to draw blood from veins that usually resisted during infectious disease tests, but the staff was also nice, friendly, caring, angels, empathic, humane, and helpful. The list of superlatives used by the visitors to describe the staff was long. This was intriguing as Swedish drug policy is often portrayed as prohibitionist and, as a result, harm reduction interventions are strictly governed and have from an international perspective even been characterized as high threshold services (Barrett et al., 2022). For example, NSP in Sweden is according to law (SFS 2006:323, 2022) primarily targeting infectious diseases, and enrolment requires that the person is aged 18 or older, shows ID, registers in the program, and takes regular infectious disease tests. The law also requires a one-to-one exchange of equipment, with some room for discretion and distribution under certain conditions. Furthermore, staff must report all concerns about underage children to social services. Despite this, the people we interviewed described how the staff went out of their way to help them with a variety of issues unrelated to needles, syringes, and infectious diseases. While the work done at the NSP is officially characterized as medical, aiming at reducing medical “risk factors” related to IDU, the narratives of the participants raised questions about the role of these programs in tending to the challenges of a life with IDU—a life usually signified by not being treated “nice” (e.g., Eriksson et al., 2014; Holeksa, 2022; Lancaster et al., 2015; Lloyd, 2013; Radcliffe & Stevens, 2008).
As drug harms have increasingly become seen as shaped by specific social, political, and economic environments (e.g., Bourgois, 1998; Rhodes, 2009), so has also harm reduction research and practice come to “emphasize the social and contextual determinants of illicit drug use” (Duff, 2010, p. 337). This is emphasized in numerous studies suggesting that, for example, drug law enforcement in prohibitionist contexts might undermine harm reduction measures, due to police patrolling close to harm reduction programs, or confiscating injection equipment (Kammersgaard, 2019; Khorasheh et al., 2019; Holeksa, 2022; Houborg & Jauffret-Roustide, 2022; Urbanik et al., 2022), and that prohibition can have a negative influence on health and wellbeing for people who inject drugs (Holeksa, 2022; Richert, 2015). Following this, our point of departure is that risks and harms with drug use, as well as harm reduction, are created in a complex interplay between individuals, groups, institutions, and policy (Rhodes, 2002).
Amid this interplay are people who inject drugs, but also professionals situated to perform harm reduction. In Sweden, staff at harm reduction institutions are in the particular position of performing harm reduction interventions in a context traditionally dominated by strict prohibition with a zero-tolerance approach, where treatment and welfare services have been conditioned by drug abstinence (Tham, 2021). While harm reduction has become increasingly important for improving the health and wellbeing of people who use drugs also in Sweden (Eriksson & Edman, 2017; Richert et al., 2023), there is a growing body of research advising that harm reduction initiatives need to consider a variety of situations and structures to be successful: for example, anonymity and confidentiality at the harm reduction services (Michaud et al., 2023), trust between clients and health services (Treloar et al., 2016), geographic location and opening hours (Moore & Dietze, 2005; Värmå Falk et al., 2020; Walker et al., 2024), police actions (Shannon et al., 2008; Wood et al., 2003), and feared loss of child custody (Boyd et al., 2022; Värmå Falk et al., 2020). This emphasizes the difficult position of harm reduction in a prohibitionist context—in this case, the Stockholm NSP.
Emanating from these understandings, this article explores the role the NSP plays in reducing harms and improving the life situation for people who inject drugs. Evaluations have shown positive effects of Swedish NSP on hepatitis C (Kåberg et al., 2018), pathways into opioid agonist therapy (OAT), clients’ health-related quality of life (Bråbäck, 2018) and risk behaviors (Kåberg et al., 2020). To date, with few exceptions (see Nordstedt, 2023; Värmå Falk et al., 2020), very few studies focus on how people who inject drugs reason about NSP and other interventions offered in Sweden, and the extent to which these respond to their needs and the risks and harms involved in IDU. Similarly, there is a lack of staff perspectives. The aim of this article is therefore twofold: (1) to further describe what situations, relations, and structures that affect interactions between people who inject drugs and the NSP, and (2) to analyze how these work together to move people who inject drugs towards or away from various forms of harm related to IDU. While the results point to some critical aspects of the processes by which the NSP operates, our intention is not to deny the NSP's importance, or the life-changing work done there. Rather we intend to critically discuss the practices and role of harm reduction in a prohibitionist environment, and the consequences for the subjects of needle exchange. With a point of departure being that real harm reduction should actually lead to improved well-being for its visitors, the implications are significant as practice, research, and debate risk reproducing current stigmatizing images of people who inject drugs, and limit imaginable policy responses.
Theoretical Framework
A Sociomaterial Approach
As previous research has shown (e.g., Berridge, 1999; Gowan et al., 2012; Keane, 2003), harm reduction initiatives post HIV/AIDS tended to position drug users as “rational decision makers”—not acknowledging how for example gender, class, and stigma provide unequal access to resources (Moore & Fraser, 2006). Critics have since taken a more situated approach. Following the ontological turn—inspired by assemblage theory—the focus has shifted from individual responsibility to emphasize interactive and human, nonhuman, and symbolic bodies, and how they form to produce different drug-using behaviors, identities, and effects of drug use. Hence, this sociomaterial approach, by now prominent in critical harm reduction research (Dennis, 2019; Duncan et al., 2017; Fraser, 2006; Fraser & valentine, 2008; Yates, 2023), concentrates on processes of interacting and active human (e.g., substance users, treatment staff, police), nonhuman (e.g., waiting rooms, syringes, substances) and symbolic (e.g., service regulations, drug policy) bodies, and how they gather to form temporary phenomena. The growing body of research examining the relationality of drug use has, for example, investigated how alcohol and other drug (AOD) issues related to nonhuman materiality such as spaces and settings (e.g., the design of consumption rooms in Duncan et al., 2021; the methadone maintenance queue in Fraser, 2006); particular bodies (e.g., the syringe in Vitellone, 2011; the mobile phone in Dennis, 2016); and temporality (e.g., memories’ relation to cravings in Månsson et al., 2024; emergent causalities in Race, 2014) produces different affects related to substance use and harm reduction. This research suggests that “humans, substances and contexts are seen to have little that inherently distinguishes them from each other” (Dennis, 2019, p. 22), and therefore that research should focus on assemblages of different bodies where risk, harm, and pleasure can appear.
Assemblage Thinking
Assemblage thinking can thus inform a dynamic and relational understanding and push beyond viewing for example addiction, health, or harm reduction as “stable natural objects or self-evident, foundational concepts” (Fraser et al., 2014, p. 19). Following such considerations we focus on the assemblages of human, nonhuman, and symbolic bodies in the interview material and how they can produce movement towards or away from harm. Importantly, in a drug assemblage “the body connects up not only to the drug (its texture, its smell, its taste, its appearance, its speed) but also to other bodies […] such as people, substances, knowledges, institutions” (Malins, 2004a, p. 94). This means that it is the specific gathering of different bodies in a drug assemblage, rather than simply the chemical compound of the drug, that transforms bodies and enables specific affects. Following such considerations, the notion of place has been accentuated as central for understanding drug use behaviors (Duff, 2007). A place, like an NSP facility, is according to this reasoning also continuously being made and remade, contested, and stabilized in the situated encounters (e.g., between people who inject drugs, staff, the public, material, and structural bodies). In a context where the very premise of harm reduction is controversial, assemblage thinking has inspired our analysis to go beyond exploring harm reduction initiatives at surface level—as either good or bad, as either a success or an erosion of the core messages of the prohibitionist drug policy—“by looking at the affects each assemblage produces, the movements it makes, and the specific stratification it produces” (Malins, 2004a, p. 96).
Affect and Movement
The notion of affects is important in assemblage thinking, as they denote how bodies “are moved around and even transformed” (Latimer & Meile, 2013, p. 8). Deleuze's (1988) perspective on affect offers valuable insight, suggesting that affect reflects the transformations bodies undergo in their relations with other bodies (human or nonhuman). These encounters shape and alter affects as they course through bodies, determining how each body is capable to move others and be moved, and what it is capable of doing, enacting, or being. In this relationality in agency, all bodies are affected by other bodies in any encounter. This means that affect and place become intertwined. For example, a place like an NSP is mediated by different processes of territorialization (Deleuze & Guattari, 1987): Deterritorialization produces movements forward and opens up lines of flight (leaving the territory), and reterritorialization brings assemblages back and blocks forward movement (locking people in particular territories and locking them out of others).
This has been empirically illustrated by Dennis (2019) in her ethnographic work with people who inject drugs and professionals in treatment and harm reduction services. In Dennis’ analysis some assemblages brought positive affects, as bodies connected with other bodies that increased the power to act and to go on forming new relations and opening up lines of flight. These connections increased bodily potentials and capacities for life which made new becomings possible: for example, becoming "normal", becoming healthier, or becoming other with drugs. Other assemblages produced more negative affects when becomings were blocked, for example, if drug assemblages were dominated by bodies (e.g., media images, policies, police, drug dealers, mobile phones, criminal records) stratifying drug-using bodies as “junkies.” Stratification of bodies thus reduces its “capacity to form other relations and to become-other (a student, a sister, a friend, a lover)” (Malins, 2004a, p. 99). By focusing on the connections between bodies mentioned by the participants (e.g., NSP regulations, institutions, family members, needles) we analyzed the role the NSP had in opening up positive lines of flight or locking people in stratifying stereotypes. In reference to Dennis’ work, we sought to identify what connections produced movement and made new becomings possible, and through what connections becomings were blocked.
Methods
Sample
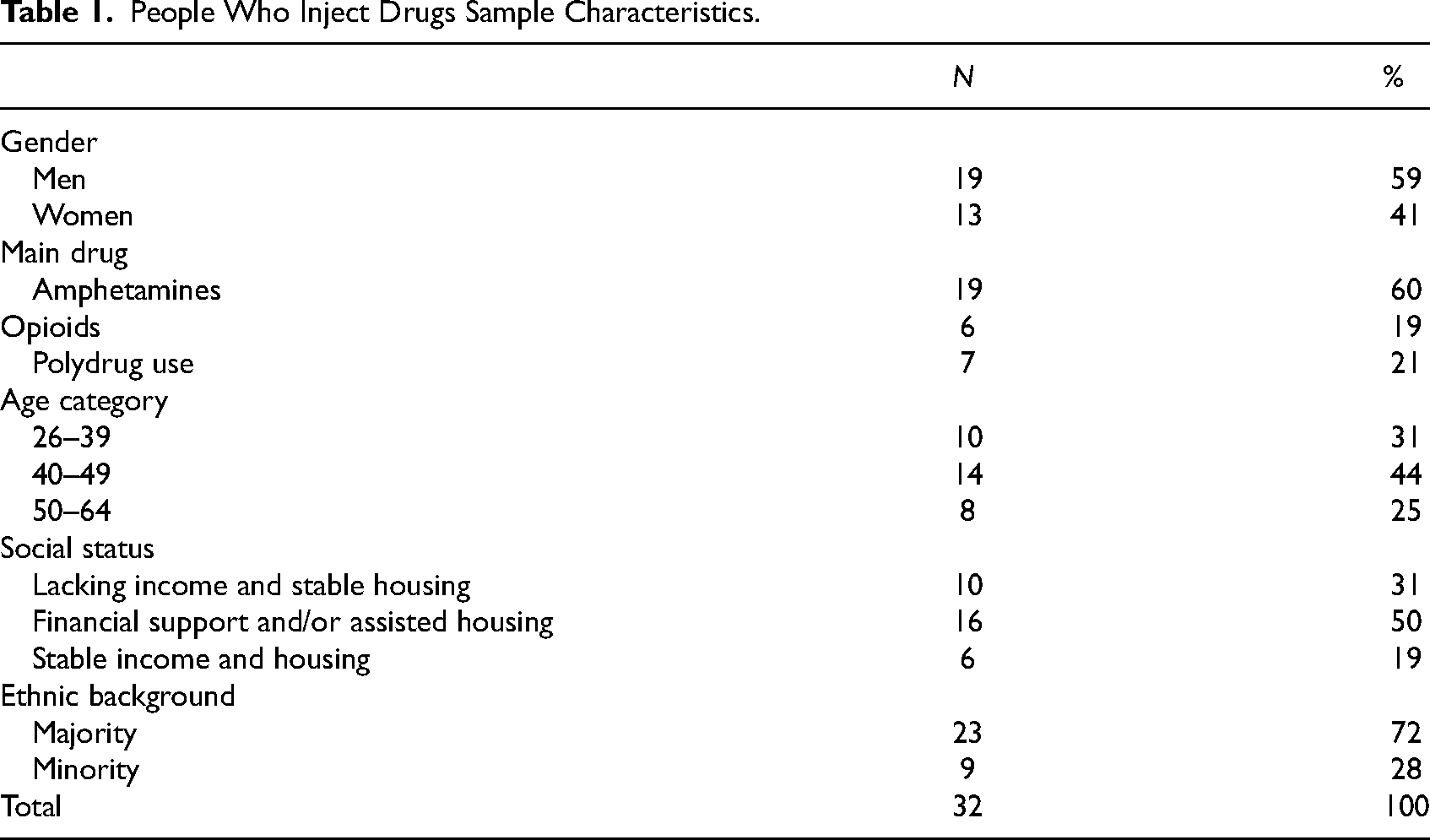
At the time of the study, there was only one official NSP in Stockholm, with two permanent facilities and one mobile bus visiting different locations. The permanent units were very similar in structure, rules, regulations, and staff (that generally moved between all facilities). The bus was somewhat different regarding the physical structure. We conducted individual interviews with people who inject drugs and focus group interviews with staff working at the Stockholm NSP. The sample of people who inject drugs consists of 19 men and 13 women, aged 26 to 64, and primarily those who stated amphetamines as their main drug of choice (see Table 1). These participants were classified into three socioeconomic groups: stable income and housing, financial support and/or assisted housing, and lacking income and stable housing. Furthermore, 10 had OAT.
People Who Inject Drugs Sample Characteristics.
For staff interviews, all Stockholm NSP staff were asked to sign up for interviews on three occasions, which resulted in groups of 3–5 participants in each focus group. The sample consists of 12 participants, all women, which reflects the gender distribution at the NSPs (see Table 2). Staff generally had experiences from working in all the different NSP facilities in Stockholm. All had extensive experience of working with what they called the NSP “target group.”
Staff Sample Characteristics.
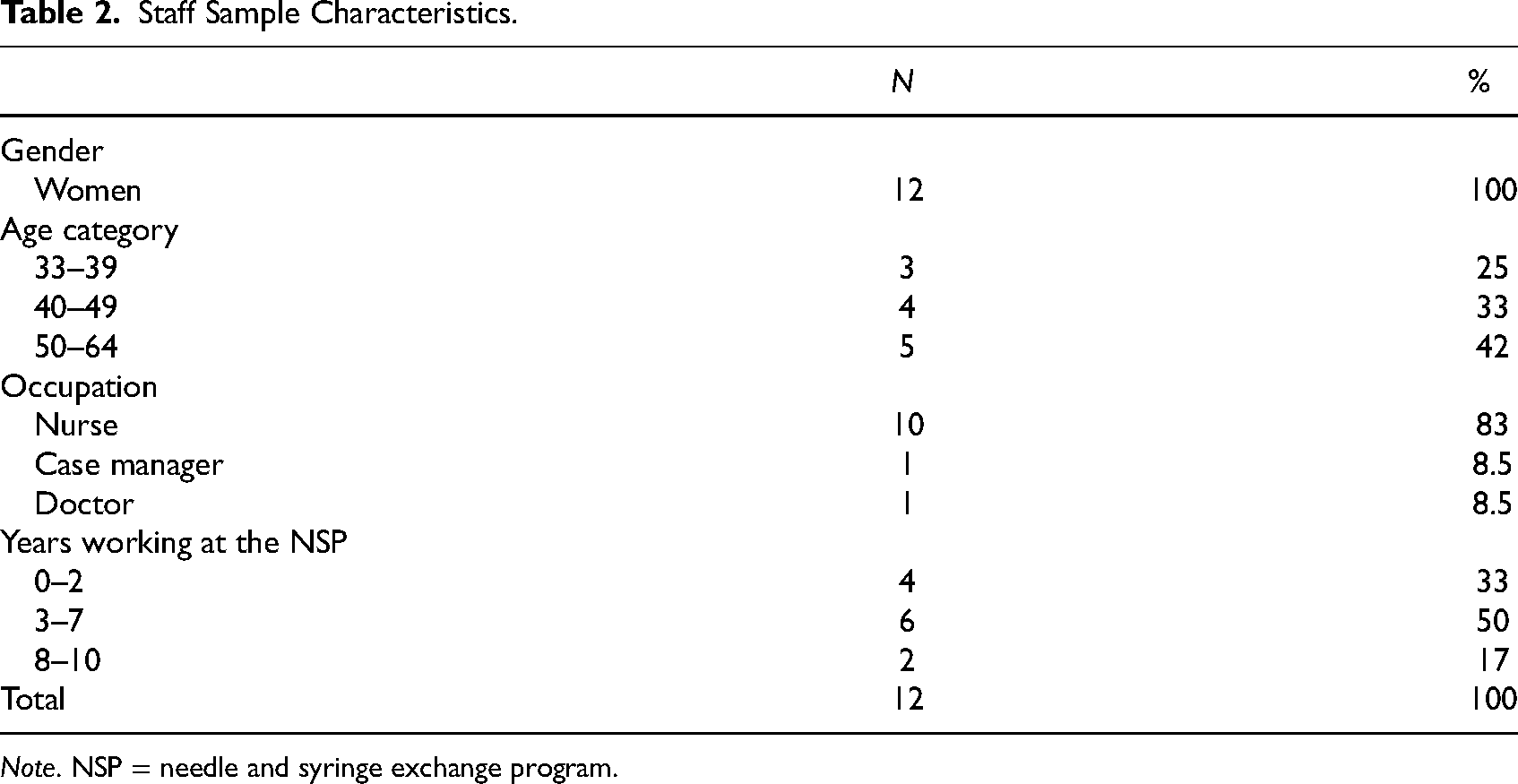
Note. NSP = needle and syringe exchange program.
Interviews
First, individual interviews with people who inject drugs, mainly recruited from the Stockholm NSP (permanent and mobile units), were carried out between August 2022 and March 2023. In addition to NSP visitors, we attempted to reach nonvisitors and further explore reasons for this by also using the Stockholm Drug User Union Facebook page and the project website for recruitment (n = 3). The interviews were done face-to-face (n = 29) or over the telephone/Zoom (n = 3). They lasted between 20 and 70 min (median 48). The interviews were semistructured and covered five main topics: background and living conditions; substance use; NSP; risks and risk management strategies in everyday life; thoughts about Swedish drug policy. More specifically, a typical interview started with talking about the NSP, reasons for the current visit and how it had proceeded. Some participants demonstrated the equipment that had been collected, and where they stored it as they would leave the NSP. Next, the interview moved on to ask about what a typical day, when injecting drugs, look like. This was contrasted with particularly good or bad days during periods of IDU. The interviewer probed into mentioned risks and participants were also asked about what they themselves found most risky regarding IDU. It has been suggested that qualitative interviews may be less suited to capture more-than-human-relations (Demant & Ravn, 2020), due to the way data becomes filtered by researchers who may lose sight of how various (nonhuman) bodies comprise in events such as NSP engagement. In an attempt to handle this, our interview approach, delving into typical-good-bad days, proved to be successful in providing rich descriptions of both human and nonhuman bodies related to experiences from the NSP. The participants received a gift card allowing for any purchase at a local grocery store as a token of appreciation.
Second, after finalizing interviews with people who use drugs, semistructured focus group interviews with the NSP staff were conducted. Interviews were moderated by two members of the research group, and lasted approximately 90 min. The rich descriptions from the interviews with people who inject drugs, along with experiences of spending hours in the waiting room at the NSP facilities when recruiting participants, informed much of the focus group interviews. The interviews covered three main themes: background; thoughts about risk and harm prevention; and professional dilemmas at the NSP. The staff did not receive gift cards as their participation was sanctioned by their workplace and were carried out onsite during work hours.
Analysis
To get an overview of the interview material from the first round of interviews, a broad stroke initial content-based coding was done collectively by all authors in the software program NVivo. To address the specific research question of this analysis, the initial codes “interaction NSP,” “interaction other care,” and “stigma” were analyzed and coded more closely. This resulted in new codes, including for example “continuity,” “needles,” “identification requirement,” and “trust,” that was structured according to how they could be viewed as either human, nonhuman, or symbolic bodies (see Table 3). These codes to a large degree overlap with previous research in what stands out as important drivers and barriers for visiting the NSP (e.g., as described in Boucher et al., 2017; Nordstedt, 2023; Värmå Falk et al., 2020 and Yates, 2023).
Analytic Structure of Coded Material.
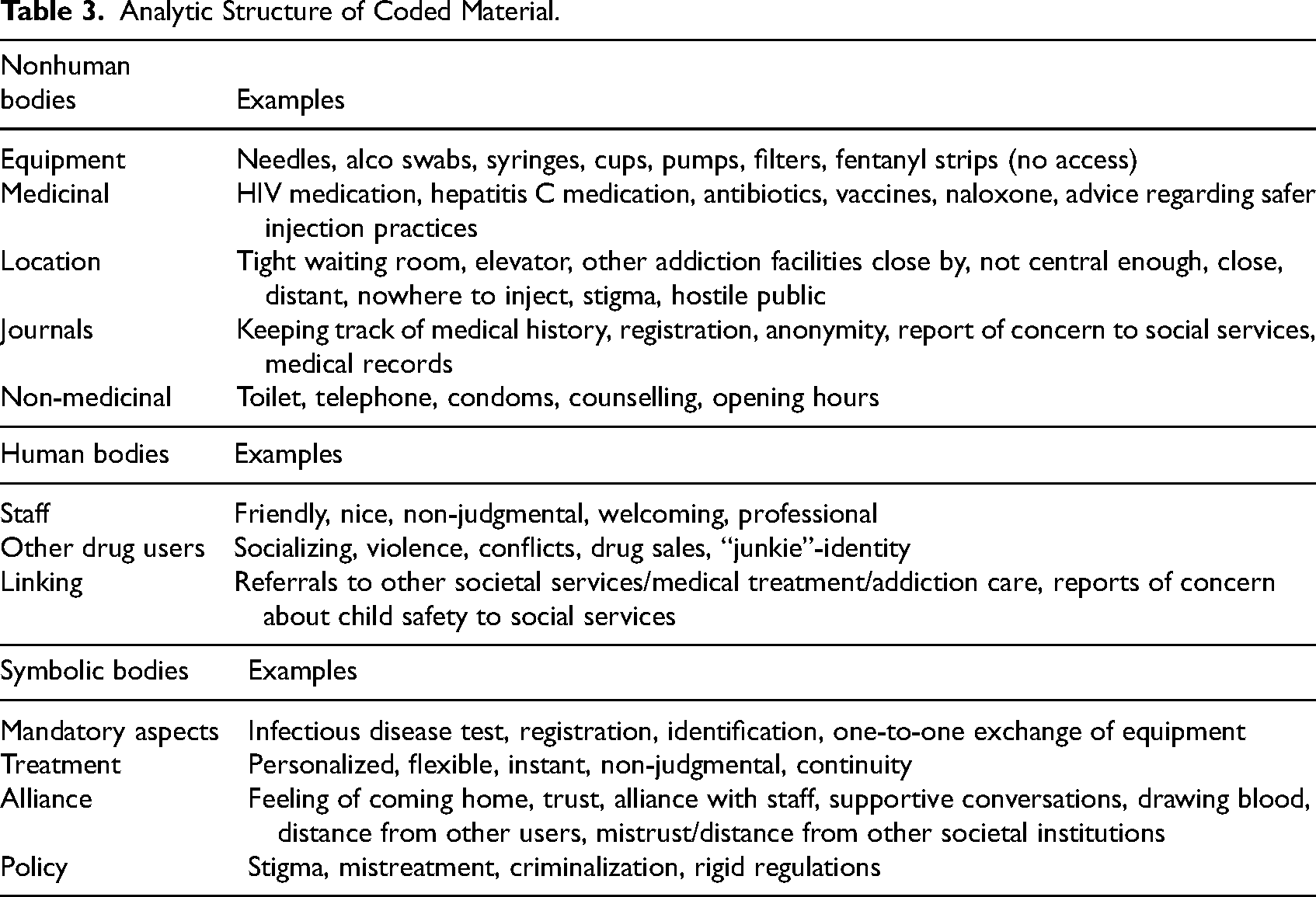
Emanating from assemblage theory, we then analyzed how the identified bodies could be congregated in different interview narratives. This was done by focusing on the event of enrolling at the NSP and visiting the NSP, and the specific bodies that were described as pivotal in each specific event. We have emphasized bodies that was prominent in the overall material, and present the most illustrative cases. Due to the somewhat specific character of the mobile NSP unit, the focus is primarily on the permanent units (which all NSP visitors had visited).
The theoretical idea of movement is of particular importance in this analysis as it allowed for a nuanced examination of how the NSP is not an inherently “good” or “bad” intervention where some bodies will automatically become drivers or barriers for visiting the NSP. Instead, this analysis allows for examining how different bodies gather in specific assemblages, and how these play into different possibilities for or blockages of new becomings—and how it may move people towards or away from harms related to IDU. For example, the registration procedure stood out as extremely influential in some assemblages, locking people out of the NSP, while it was not described as a factor in others.
Next, staff interviews were analyzed. After the first readings of this material, it could be concluded that there was a strong consensus between NSP staff and people who inject drugs about drivers and barriers for visiting the NSP. As a way to strengthen the analysis, we therefore triangulated the materials and coded staff interviews using the structure of Table 3 and the event of enrolling and visiting the NSP as it was disclosed in the analysis of the interviews with people who inject drugs. This resulted in four codes (with some child codes) that captured also the corresponding staff aspects on these themes: descriptions of visitors, locking out (e.g., journals, mandatory aspects), opening up (e.g., linking, alliance), and locking in (e.g., previous experience, location).
This project used written and verbal informed consent, and received ethical approval from the Swedish Ethical Review Authority (No. 2022-02343-01).
Results
In the methods section, we have demonstrated what bodies that stood out as drivers or barriers for visiting the NSP (Table 3). Looking closer at the individual interviews, particular gatherings of such bodies however seemed to affect interactions with the Stockholm NSP in different ways. The themes below illustrate how the intersection of particular bodies came to work to either block or open up movement towards strengthened possibilities to avoid harm for a person who inject drugs. The thematic structure helps to illustrate different events related to the NSP: the way in (enrolling) and the regular visit (enrolled).
The way in—Enrolling at the NSP
Although the NSP was generally recognized as a vital place opening up for movement towards reduced harm and better physical health by offering free injection equipment and care, the first entry was repeatedly described as difficult by people who inject drugs. This is exemplified in the introductory quote, where Peter (man with stable income and housing, 50–64 years) referred to the shock of being treated nicely at the NSP. People who inject drugs and staff described the general healthcare system as stigmatizing, rude, and lacking in knowledge about IDU, and that these experiences could deter from enrolling and visiting the NSP. This general mistrust in societal institutions, places dedicated to helping citizens, can be understood in light of societal stigma in the overall prohibitionist context (Holeksa, 2022; Rehman et al., 2024). In this section, we will explore the decision to enroll or stay away from the NSP, and what bodies stood out as important in this process. As we will see, most of them were related to the way a connection with the NSP acted to reinforce an identity as an “addict” or “junkie.”
Blocking Movement: Locking People out of Harm Reduction
A recurring description of why people we interviewed initially refrained from enrolling was related to parenthood. As seen in the quote below from a staff interview: And then it's also this thing with children, it's a bit tricky. Because then we say before the person has stated their name and social security number, we say “this is the way it is, if you enroll here there is this and this report of concern.” And then, some turn around and leave. (Kristina)
As seen here, staff were careful to inform about the need to report a concern about children to social services before the visitors stated their name, so they could choose to leave. This practice illustrates a general understanding that a connection with the NSP can limit bodies from identifying as both a person who injects drugs and a legal guardian. This general idea is also explicitly illustrated by Johanna (woman, lacking income and stable housing, 40–49 years), who had been using amphetamine on a daily basis for many years and visited the NSP regularly. When asked why she first turned to the NSP said: Well, first I was supposed to enroll [at the NSP] but then I chose to skip it when I realized that, like the woman said, there will be an automatic report to social services if you have any contact with the children. Even if you don’t see them… Well, if you have an ongoing contact, it isn’t good anyway of course. And as an addict, I know that. So, she said “there will be an automatic report because you have part of the custody left.” So, the day I gave up custody of my children altogether, well, then I could enroll. Otherwise, there would have been… I don’t want them to know, and I don’t want the father to know I inject either.
In this quote, Johanna described why she chose not to enroll on her first attempt. At this point she still had legal custody of her children, and saw them on occasions when she was not using amphetamines. While Johanna described that the father of her children knew about her drug use, the association with the NSP made her injecting visible and the report of concern tied her to this connection. She tried to avoid this as she described that it limited her potential of being a parent. What the quote shows is that the NSP rules, the report of concern, the practice of injecting, along with the ongoing contact with Johanna's children and their father assembled in such ways that they in practice blocked her from moving forward to enroll. It was first when she “gave up” custody of her children, that she decided to go back to the NSP. It is however clear that the practice of reporting concern did not affect our drug-using participants in the same way. For example, this practice was, with one exception, mentioned only as an influential body in relation to women who had children and injected drugs.
Similar lines of reasoning for not enrolling were found among nonvisitors who described that they were living “ordinary lives,” and how going to the NSP would make surrounding society, and health care, treat them as “addicts” or “junkies.” Like Hans (man with stable income and housing, 50–64 years), who used to identify as, what he called, an “addict,” but described that he at the time of the interview injected amphetamine daily as an “aid” in life, along with other prescribed pain medications. He had made the decision not to enroll, and made it very clear why the NSP was not an option: Those living in the streets, I understand that they go to the needle exchange. I would also have done that. But even if I don’t have a good economic situation, I feel I can afford it [buy needles online]. I can’t afford to be seen there [NSP], it would cost me too much. I have been living an ordinary life for too long.
This quote illustrates how going to the NSP would connect his body with needles and IDU, and how he believed that this would affect his connection with what he calls “an ordinary life.” In another part of the interview, Hans described that he would like the professional help of for example the NSP if he accidentally “make a mistake [injecting] at some stage,” but that it was still not worth it, even if it would result in his death. The stigma connected to IDU would according to this reasoning put his “ordinary life” at risk (unlike “those living in the streets”), as well as his right to prescribed medication. What these examples illustrate is that although Johanna and Hans described the material and medical resources at the NSP as important for moving toward strengthened potentiality due to less health risks, the connection with this place would determine and block their bodies’ capacity to interact with other, more important, bodies (e.g., children, general healthcare, medications, and social surroundings).
The mandatory identification and registration at the NSP also worked to connect people with a “junkie” identity, as exemplified by Johanna above and Elin (woman, 26–39 years) below who talked about the (un)willingness to enroll. Although Elin had not been injecting for two years at the time of the interview, she described her life when injecting, without stable income and housing, as marginalized. While she did attend the NSP regularly, she reasoned about why others might not want to enroll in the following way: Well, it's probably all these ideas and facts that you don’t want to be part of the registers, you don’t want to be registered as a junkie. Or that you are ashamed. While I was totally shameless in my addiction and didn’t feel any shame [laughter], it could be one of those things. Or that you are not that disadvantaged, at rock bottom. You might be a little more functional addict and don’t want to be associated with us [laughter], the bottom of the barrel. Stuff like that. Or that you are under threat and don’t want to mix with the people going there. They all gather there; everybody knows everybody in the end.
This quote is an illustrative comparison between how different bodies might gather to enable (shameless, bottom of the barrel, knowing everybody) or block (registers, shame, functional, associations with other users, threats) people from enrolling at the NSP. Taken together, these examples illustrate how parents and people who still had normality to relate to and uphold were locked out of the NSP due to the risks of stigma and retaliation if they were tied to this place. For these nonvisitors, a connection with the NSP was not seen as a way of moving forward. Instead, a connection with the NSP (e.g., the physical location, registers, connections with other people who inject drugs) was described as something that would decrease capacities to live an “ordinary” or “functional” life, and leave “little room for movement” (Malins, 2004b, p. 490). From the theoretical perspective of becoming (Deleuze, 1988), it was not until other becomings or identities were blocked and some connections had taken over ways of being a parent, a patient worthy of access to pain medication, or in “living an ordinary life,” that these participants accepted to “be registered as a junkie.”
What Elin's quote also demonstrates is how the actual place and its organization become important bodies that might act to lock people out of NSP. The NSP facility she refers to is located next to other addiction and homelessness services where marginalized people “all gather” in small parts of the city (the other facility is located nearby an AOD emergency unit). Similarly, the architecture of the premises (e.g., “you have to go up in an elevator, and there's a tiny waiting room,” Linda), and the safety arrangements of locked doors and separating glass walls clearly manifested and enacted the profound difference between staff and visitors. In situations where participants described that a connection with other people who inject drugs worked to reinforce an “addict” identity they did not want, a visit to the NSP would certainly be problematic (“everybody knows everybody in the end”). This illustrates how a place that becomes a “junkie” space will act to shape the social identity of the visitor, which in turn affects “what connections it can make with other bodies and what changes it can undergo” (Malins, 2004b, p. 490).
While staff described ongoing efforts to navigate obstacles that they believed made people hesitant to enroll (e.g., finding ways to identify people to facilitate enrolment despite lack of identity documents, trying to reach immigrant groups by using staff who speak the same language, and organizing woman-only days), they rarely mentioned bodies acting to lock out the more “functional” users described above. It was clear that their main “target group” was people who can be characterized as marginalized. One concrete example is the strict opening hours (10 a.m. to 4 p.m., with the exception of opening hours until 6 p.m. one day) on weekdays only, which in practice blocks people with ordinary jobs from attending. These examples show that the described affects of being connected to the NSP reduce some participants’ capacity to move forward and enroll, as the inclusion of the NSP in their assemblage would decrease the capacity to uphold other connections that they considered to be more important.
The Regular Visit—Being Enrolled at the NSP
Focusing instead on narratives from people who were already enrolled and regularly visited the NSP, they generally described how their previous hesitation disappeared immediately after enrolling. In the overall narrative about visiting the NSP, several bodies stood out as particularly important for this: free injecting equipment, staff care, continuity, and trust in staff ability. The narratives about the event of visiting the NSP however illustrated that the affects and possibilities for movement was described differently by the participants. In this section, we will explore how the particular gathering of certain bodies in relation to the NSP seemed to open up or block movement.
Opening Up for Movement: Making New Becomings Possible
While most visitors described the main reason for attending as a way of acquiring injecting equipment (needles, pumps, alcohol swabs, cups, naloxone, etc.), it was repeatedly emphasized that the way the staff interacted with visitors was important for coming back. This is showed in the quote below where Erik (man without stable income and housing, 40–49 years) talks about reasons for visiting the NSP: Interviewer: Does it happen that you come here without… I mean when you are not getting equipment, for other reasons? Erik: Yes, they help out with a lot of things. Counselling and conversations, sometimes I want to come in and talk to them, and sometimes they want to talk to me. It's a very nice relationship. I don’t know if you heard out there [in the waiting area], but I was joking around and asking the girl that is pregnant [staff] if she had… giving her advice about the baby and stuff. So, I mean, it's on a very familiar level. It doesn’t feel like coming to the doctor, it feels like coming home. […] They [staff] are wonderful. You can tell that they genuinely, honestly care.
While Erik lived with severe physical and mental health challenges, without stable housing, and “had been close to dying 14 times in the last six months”—he still succeeded to go to the NSP regularly. Erik described his life as very lonely; he had no contact with his former wife or kids, he had no friends, and he had recently lost a close family member in an overdose. In an assemblage where it could be expected that Erik would not prioritize coming to the NSP, the care shown by the staff is described as vital in his choice to come regularly. When asked about any reasons not to come to the NSP, he said “if I could come home again […] to the kids, and the bygone times.” This example illustrates the important role of the NSP staff and their care, and how their gathering opens up a little space of “home” and “familiarity” for Erik in an otherwise lonely situation. Similar to many other examples in the material, he described that the NSP was one of few places where he met people that treated him as a person, not as a “junkie.”
The experience that the NSP has the capacity to tend to wider difficulties and inequalities their visitors encounter in everyday life can be seen as ways of opening up to form new relations and possibilities. This was also emphasized in all staff interviews—that their “mission” is to help their visitors with several aspects of their lives—as demonstrated in the passages below: Sofie: I accompany patients who are going to… Elsa: Social services… Sofie: …X-ray, social services, first meetings with OAT-team, the police, the tax agency. So that the patient should be willing to take a step toward change or just get to where they are going. Accompanying them to the gynecologist. Then, if one patient has a really high confidence in [nurse] and needs to do an abortion, then she can accompany the patient there if it's… To make sure that the patient feels safe and wants to go. It's all a bit open, but we try to help the patient in any way we can.
Here, the NSP staff described their work to assemble human, nonhuman as well as symbolic bodies in their visitors’ lives so they can “take a step toward change,” clearly recognizing that harm reduction includes much more than sterile injecting equipment. This effort was also noted by the visitors, who repeatedly described the NSP staff as flexible, rule-bending, and accommodating. When we asked the visitors to compare the experience of coming to the NSP with the social services several expressed that it was a difficult comparison as their responsibilities are different, but also due to the relationship that is built through continuity: Well, here [the NSP] is where I am most frequently, you only have contact with social services when you need to prolong your housing and stuff like that, and then it is mostly over the phone. (Jan, man with financial support and/or assisted housing, 50–64 years)
What is demonstrated via Erik, Sofie and Jan's narratives, is how the needle supported a continuous care relationship, not only since people who inject drugs “frequently” needed to collect new equipment, but also since it necessitated a face-to-face encounter. The needle, which is described in the previous section as an important body in assemblages blocking people from visiting the NSP, here becomes a doorway to open up for taking “a step toward change” once people who inject drugs were enrolled.
The above extracts further illustrate that the care shown by staff clearly went beyond the typical medical institutions in its attention to bodies in different ways. This created an assemblage from where visitors described how trust could evolve: for example, trust to talk about difficult things, trust to accept help with a great variety of issues, but also trust in staff's ability to draw blood to check for HIV and hepatitis C. While the mandatory blood tests were sometimes described as difficult (e.g., due to damaged veins), visitors still described it as a positive part of the NSP practices: It “feels good, because they keep track of you and that you are OK” (Annika, woman with financial support and/or assisted housing, 40–49 years). Although mandatory aspects of other institutions were generally described as barriers to involvement, blood tests were accepted at the NSP within this framework of care and trust. Matti (man with financial support and/or assisted housing, 50–64 years), describes below how trust is something affecting the physical body in a very explicit way: Matti: I usually leave samples. I am HIV-positive and I have cured my hepatitis C here. […] Not just anyone can stick me, because these bad boys [veins], they will hide instantly if someone else holds the needle […] So, it is a bit difficult for me, but during these years I have gotten to know some people at the needle exchange. And for some reason they have managed to enter themselves into me, into my body… my psyche accepts them so that they can take samples on me. But they are not many. Interviewer: No, you have to feel calm? Matti: Yes, that… you have to make a certain impression to… I have a hard time with trust.
Here, Matti shows how drawing blood is intimately connected to relationships by describing the event of drawing blood as staff “entering” into his body. This illustrates a very “fluid and open notion of the body” (Dennis, 2016, p. 131), and how the affective body of trust opened up the physical body to accept help. This acceptance had also improved Matti's drug assemblage by curing his hepatitis C and by keeping track of his HIV.
The staff's efforts of attentive care were also clear in Thomas’ (man without stable income and housing, 40–49 years) interview. He had used amphetamines on and off for many years, and described it as self-medication for his undiagnosed ADHD and diagnosed bipolar disorder. He had been trying for years to get a functioning contact with psychiatry to get a neuropsychiatric assessment and legal medication. In his struggle to improve his health, he shared how he visited the NSP “for everything” related to healthcare, and to get equipment, two times a week because the staff “is the best,” and how they had “without me asking” decided to help him get to the appointments with psychiatry. He said: Thomas: But then it's this thing for me that I have to get to the meetings [with psychiatry]. I keep forgetting all the time. So, I actually asked social services […], that I could have a contact person that could call, tell me that “today you have to do this”. But you can’t have that if you’re not enrolled [at the social services] and have welfare, so that didn’t happen. So, now I have people here at “the change” to call and nag me instead. Interviewer: Very good. Thomas: Yes, this is actually a rescue for me, many times, that they do it, send texts that “today you have this, do that”. So, yeah…
Thomas illustrates in several ways how the NSP gathered human, nonhuman, and symbolic bodies that became part of an assemblage opening up possibilities for new becomings (a life with legal medication instead of illegal drugs). In a difficult situation of being homeless, with unmedicated diagnoses, he was inventively trying to navigate the system to increase his chances of moving on in life. In his comparison with social services who were described as unwilling to facilitate this with reference to rigid regulations, the NSP staff stepped in to help him navigate toward new connections. Unlike the social services, where Thomas experienced that “all questions are about what other drugs I took,” the NSP is in this description treating him as a person in an assemblage of connections that needs to be improved according to his preferences. The staff's creative doings (e.g., text reminders) thus supported improved capacities for life in a life situation characterized by notable mental, social, and material disadvantages.
Blocking Movement: Locking People in Unwanted Identities
As mentioned, visitors repeatedly compared the help they received at the NSP to other parts of the system, which were criticized for being stigmatizing and unhelpful. As a consequence, visitors described how they sought to “increase good encounters and limit the bad” (Dennis, 2019, p. 125) by turning to the NSP for help with an array of issues that officially fall outside of their responsibility: Interviewer: What do you think works well here [the NSP]? Lars: It's this, you get your equipment, you get help with… you get a referral to a doctor when you have the need for that, and you get help here for easier things, stuff that the general health center should take care of. In that way, it's a good complement to the existing health care that unfortunately isn’t that happy to help people with addiction problems and vulnerability. Interviewer: Ok, so that is your experience of regular health care? Lars: The regular health care is not that interested in dealing with people like me. That's unfortunately my experience. […] I would say it's an extension of the general stigmatization in society. (Lars, man with financial support and/or assisted housing, 50–64 years)
While health care for injection-related infections is part of the official aims of the NSP, general health care is not. As described above, the NSP however became a compensating factor for the “uninterest” and “stigmatization” experienced in regular health care, where the substance, and the needle, seem to disqualify people from “normal” care and being treated like patients (Dennis, 2019, p. 145). While this compensating role was certainly much appreciated by NSP visitors, it might also unintendedly reinforce stratifying images of the visitors as unable to receive regular healthcare. This is discussed by the staff below: Hanna: In the best of worlds, it wouldn’t be necessary for us to do everything. That they could actually visit other healthcare facilities, and you could be treated well and get the care and help you need from other places. Susanne: I also think, it's people, and we should meet people like people no matter their background. And, I mean, everybody has the right to be met like a person. Hanna: Because it's also that if this group is always supposed to have their own places, then it's also like… you become different. Susanne: Yes, why should you segregate? Hanna: It does something to your self-esteem, that you are always a bit on the outside and different.
While the staff shared their willingness “to do everything,” they also problematized how this might reinforce the feeling of being “on the outside” of regular society in the extract above. Further, staff described how their visitors sometimes stop visiting other care facilities making the NSP “the only connection” with societal institutions: Even if [they] become drug-free, and everything is going well, [but] something happens, then [they] come here, even if [they] don’t want equipment. Because here you get help, you are seen, you get treated nicely and you come here even when you are totally clean. (Sofie)
Due to experienced maltreatment in other parts of society, and inclusive treatment at the NSP, people like Lars have a hard time making new connections to move forward. These blockages (e.g., not visiting general healthcare) caused by stigmatizing treatment kept bringing people back to the NSP, potentially locking them in a stratified “junkie” position. The potential to move on and transform is in this reasoning clearly linked to relationality and gathering of particular human, nonhuman, and symbolic bodies, rather than the autonomy of people who inject drugs.
Correspondingly, visiting the NSP was characterized as locking in a “junkie” identity by some visitors, partly due to similar reasons as to why some refused enrolment. Like Johan (man with financial support and/or assisted housing, 26–39 years), who had been injecting substances for a long time, but was trying hard to stop, who said that to stop using he needs “to get away from these waiting rooms, from these queues.” He had been going regularly to the NSP for about five years, and had also had OAT for a few years. He described that for him, coming to harm reduction institutions has been very problematic: Johan: When I started with methadone my problems escalated… the social parts. If you join the [OAT] program, you put yourself involuntarily in a… […] you start talking to people at the [OAT]. And today, [some] years later, everybody knows my name. All the addicts in Stockholm. I can go to [neighborhood with many harm reduction institutions] and people say hello to me. […] Everybody knows about me, and I don’t want that. I don’t want to be a part of it. […] And then there is “the change”. Another institution you have to visit, with addicts everywhere. […] Dangerous situations with other addicts. And really, you should just try to eliminate… Because if someone is seeking care, then it's like “OK, just sit here with the other addicts and wait.” Everybody has the same problems, the same interests, if you know what I mean? Interviewer: You get lumped together? Johan: Exactly. If you aren’t a junkie, and you are addicted and get into this world… you will become a junkie eventually.
This passage exemplifies the frustration that Johan conveyed about not being able to “get out” of “this world” of addiction. His description of why he could not move on in life and was stuck in “a loop” yielded an assemblage of human (other addicts), nonhuman (methadone, the change, OAT, waiting rooms, queues), symbolic bodies and arrangements (lumped together, waiting). This illustrates how the relationality between these different elements kept “reterritorializing” (Deleuze & Guatarri, 1987) him as a “junkie.” As shown, to try to quit using opioids and stay healthy while injecting amphetamine he entered OAT and visited the NSP—but in these places he was socially recognized by other users and reluctantly became connected to a social network of “addicts.” In his efforts of trying to move towards new connections and possibilities, he described how his “junkie” identity was instead reinforced.
In some interviews, the particular location of the NSP facility close to other addiction and homelessness services was singled out as particularly problematic. For example, although Aino (woman with financial support and/or assisted housing, 40–49 years) stated that she thought “everything” generally works well at the NSP (e.g., getting “clean needles,” “borrow a cell phone,” getting help in “calling authorities”), she was still skeptical about going to one specific facility: Aino: In the beginning it was really though coming here. […] There is an OAT facility around the corner. And I have been trying to quit and then when we come here [NSP]… I promised myself that I would never start coming here. But it's so close and good because I come here daily for other reasons, so I started coming here anyway. Interviewer: Why didn’t you want to come here initially? Aino: I tried to quit, I didn’t want to use needles anymore. Interviewer: Ok, so the [other NSP facility] was better? Aino: Yes, but it's not so close. […] But I want to avoid hanging around outside here and this whole chasing, every day. I really don’t want to abuse.
Similar to Johan, Aino describes how she wants to stop using illegal drugs, and stop using needles and how the location of this particular NSP facility is influential in locking her in a particular assemblage that she wants to change. While the location is good (“come here daily for other reasons,” “close”), it is simultaneously problematic due to the proximity to other addiction services that gathers people who sell drugs. For both Johan and Aino, harm reduction institutions were two-folded as they enabled connections making their drug assemblages safer and healthier, but at the same time this meant that they became part of assemblages that blocked new becomings.
Conclusions
The findings illustrate how the human, nonhuman, and symbolic bodies connected to the NSP are important in moving people who inject drugs away from harm. What is made evident in the vast majority of the interviews is how the injecting equipment, the continuity the NSP enables and the caring attitude of the staff is highly valued and appreciated. These bodies create an assemblage from where “new ways of becoming are made possible” (Dennis, 2019, p. 182)—they open up lines of flight. Participants mentioned both health-related (e.g., help with infections and diseases) and social improvements (e.g., contact with psychiatry, support to call authorities). Where society in broad terms (e.g., hostile public, rigid authorities, criminalization) generally blocks other identities (e.g., patient, regular person) than that of the “addict” for many people who inject drugs, the NSP can become an important compensating factor. As expressed by Nordstedt (2023), NSP in Sweden represents a welcoming atmosphere with staff displaying moral courage in a treatment system otherwise permeated by discipline and repression.
However, while barriers to NSP participation (i.e., fear of losing custody or visitation rights to children, male partner violence, and limited opening hours) has been identified previously (Värmå Falk et al., 2020) our critical analysis also shows that the NSP, in its current form in a prohibitionist context, becomes something of a Janus faced service. It both helps in opening up for new becomings, and contributes to locking in and stratifying the person who injects drugs in “addict” or “junkie” identities depending on how different bodies gather in the assemblage for the visitor. The options for people who inject drugs in this study to some extent seem “binarized; reduced to two possibilities” (Malins, 2004b, p. 490): they either undergo a becoming-junkie in connecting with the NSP or they move away from such places and possible productive connections with harm reduction measures. While the drug assemblage without the NSP might be characterized as less stratified and with possibilities for other productive connections (e.g., healthcare, children), it is however an assemblage where certain risks increase. For example, when a body does not connect with harm reduction institutions like the NSP, it is placed at higher risk of injection-related damages and diseases.
It is also striking that it is not until the lives of the people who inject drugs assemble in such ways that it seems to block other more socially approved identities that they decide to visit the NSP. This blockage is to a large extent described as loss (Dennis, 2019): for example, loss of right to be with children, the possibility to regulate the image of oneself as a coparent, an “ordinary life,” self-respect, prescribed medication, and loss of shame. It was first when there was nothing left to lose that several participants described how they decided to enroll, and the NSP thus becomes part of assemblages where lines of flight to some extents have already gotten lost. Participants described that it was when their drug assemblages were dominated by stratifying bodies, locking them in as “junkies,” that they decided to enroll at the NSP. It has been argued before that the Swedish treatment system is organized for handling and maintaining marginalized people (Storbjörk & Room, 2008)—a system potentially designed to meet the needs of homeless, substance-using Swedish men. Our results corroborate these findings, people who had something to lose refrained from going to the NSP as they feared it would lock them into an unwanted stratified position where other, more important, connections might get lost. When the NSP is produced as a “junkie space” (Malins, 2004b, p. 493), due to for example its organization and location, it might lock out more integrated people who inject drugs who do not want their bodies transformed to “junkie” bodies.
As concerns limitations and implications, an important caveat is which groups of people who inject drugs we have been able to reach in this project. Just like the main bulk of research in this field (Larney et al., 2015), this study primarily recruited people from clinical settings—NSP visitors. People who inject drugs but do not attend are thus to a great extent excluded from research in general—and from this study. Making such agential cuts (Barad, 2007) means that the same groups that are locked out from NSP and similar services, are also locked out from research. Recruiting primarily those with a multitude of problems might also lead to an overestimation of the persistence of injecting or severity of trajectories (Larney et al., 2015). A probable effect of this is that we as researchers, just like the staff, tend to reinforce people who inject drugs as marginalized, when the more integrated are outliers in both research data and everyday harm reduction practices. It might further reproduce this group as “risky” and accidentally further the sanctions imposed in managing “risky behaviors,” which might be particularly troubling in a prohibitionist environment where harm reduction initiatives have been highly controversial. While the positive narratives about the NSP can be attributed to the human, nonhuman, and symbolic bodies represented by the staff, the results in this study also vividly paint a picture of the stigmatized and difficult realities for people who inject drugs in prohibitionist contexts. Both staff and NSP visitors described the importance of a plethora of practices developed to push the boundaries of the strict regulations at the NSP set by this political context. Other options, such as harm reduction for less marginalized people who inject drugs, appear as unimaginable.
The analysis also emphasizes the importance of the needle; while it stratifies and locks people in due to stigma, it also opens up to benefit from what is probably one of the most appreciated treatment measures in Swedish addiction care. The needle enables a continuous relationship between staff and patients, which creates opportunities for care and help with multiple issues. It therefore seems important to discuss how other medical and social services, that do not pivot around the needle, can create the same opportunity for good encounters. While the NSP offers something that is described as important for its visitors, and creates a “natural” entry into their lives, it is not self-evident that the event of needle exchange per se provides the basis for good encounters. For example, OAT, which also provides continuous staff-patient meetings, is generally described with a focus on bad encounters in this sample of people who actively inject drugs.
It could be argued that it is the voluntary nature of the NSP that makes encounters better, compared to the more regulated and coercive nature of for example social services. There are however also coercive elements of NSP, such as regular HIV and hepatitis C tests. But these were generally described as “good” because staff “keep track of you.” What stands out as pivotal is rather the assemblage of the needle, the continuity it provides together with the care and kindness of the staff. While it might seem like an insignificant detail, the aspect of being treated as “a regular” person, of being remembered, having small talks with staff and not only focusing on drugs seem to create a sense of belonging that is uncommon in the stigmatized lives described in the material. In line with what Yates (2023) describes as a process of demarginalization, NSP staff provides destigmatizing, normalizing and humanizing services, thereby offering a respite in challenging life situations by tending to isolation and distress in kind and caring ways. This is perhaps the most important lesson for other social authorities: Good encounters are made possible in an interaction between relevant treatment “tools” (be it needles, maintenance medication, or psychosocial measures), continuity, care, kindness, and individualized treatment.
Footnotes
Acknowledgements
We would like to thank the research participants for their generosity and willingness to take the time and effort to participate in this study. We would also like to thank the anonymous reviewers, the editors from CDP, and the RISK research group (Katarina Winter, Lena Eriksson, and Jukka Törrönen) for their valuable and insightful comments.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is supported by the Swedish Research Council for Health, Working Life and Welfare (grant number 2021-01712).