
Abstract
Background: Women comprise a minority of performance and image-enhancing drug (PIED) consumers, with use linked to undesirable side effects. Preliminary work suggests that many women have little knowledge of what substances they are using, with males close to them involved in their use. This study aimed to explore women's motivations for PIED use; to examine the negative health experiences related to use; and to understand how interpersonal relationships facilitate their use. Method: Women who had used PIEDs were invited to participate in an online survey (N = 28) and/or interview (N = 10). Open-text survey and interview data were analyzed using content and thematic analyses, respectively. Results: There were three key areas (motivations, health experience, role of third parties) within which 12 theme categories were developed from the survey data. There were three overarching themes developed from interviews that expanded on these data: socializing women's use, facilitating women's use, and PIEDs exacerbating existing issues. Conclusion: The findings substantiate the nuanced gender dynamics of women's PIED use, challenging stereotypes and revealing the complexity of their motivations and experiences. While women's reasons for PIED use may share some semblance with men's, there is a less comprehensive understanding of the physical and psychosocial impacts of these drugs. To empower women and destigmatize PIED use, interventions focusing on substance literacy and stigma management are crucial. Future research should explore these interventions’ effectiveness in promoting women's well-being and autonomy.
Introduction
Performance and image-enhancing drugs (PIEDs) comprise a variety of substances, with the most researched being anabolic–androgenic steroids (AASs) (Fink et al., 2019; Mullen et al., 2020). AASs have the potential to improve performance by stimulating muscle growth and strength (Kanayama et al., 2020). Globally, the prevalence of AAS use is typically higher among men (6.4%) than women (1.6%) (Sagoe et al., 2014), however, recent reports from European samples may indicate women may be engaging in AAS use at increasing rates (Andreasson & Henning, 2022; Chegeni et al., 2021; Scarth et al., 2022). Women who use AAS are at risk of developing masculinizing side effects, such as voice deepening, facial hair, acne, and clitoral enlargement, as indicated among South American, U.S., and Scandinavian cohorts (Abrahin et al., 2017; Havnes, Jørstad, Innerdal et al., 2021; Ip et al., 2010). Thus, for women who use AAS, there are concerns about negative impacts on their perceived “femininity” as linked to their health (Börjesson et al., 2016; Havnes, Jørstad, Innerdal et al., 2021; Kotzé et al., 2020; Piatkowski & Dunn, 2024; Piatkowski et al., 2023b; Scarth et al., 2022).
In the context of health, the use of PIEDs has been portrayed as a manifestation of an unhealthy association with masculinity (Keane, 2005). This has led to discourse surrounding PIEDs as inherently “risky” and, therefore, contradictory to the notion of “good health.” Recently, scholars have raised questions about the insecure, irrational, and unstable forms of masculinity that are constructed through the conditions of PIED-related health promotion (Nourse et al., 2024). These discourses surrounding PIEDs often fail to acknowledge the highly normative nature of enhancement practices in modern society (Latham et al., 2019), and how these practices contribute to shaping contemporary notions of health (Tanner et al., 2013). For example, for men in Australia, PIED injection practices may be seen as avenues for self-transformation within makeover culture, offering unforeseen possibilities for existence in society (Latham et al., 2019). By framing drugs and risk in this manner, these types of discourses have revealed gendered anxiety (Moore et al., 2020), shifting toward characteristics traditionally associated with femininity, such as a greater focus on bodily care and management, which has historically been devalued (Nourse et al., 2024). Fomiatti et al. (2019) recognized the gendered social dynamics inherent in AAS use, which perpetuates this further. Fomiatti et al. (2023) go on to explain that this is predicated on the fear that normative masculinity, as associated with the contemporary ideals of health, may be eroding to resemble a traditionally “feminine” approach to bodily care and management, which is often stigmatized. Female bodybuilders, for instance, are often labeled as “gender outlaws” for challenging these norms and embracing aesthetic strength sports (Shilling & Bunsell, 2009). Research suggests that stigma surrounding illicit drug consumption is intensified for women, who are “breaking the law” (Gibson & Hutten, 2021). This stigma is further heightened for women who use drugs such as PIEDs, as their actions also challenge traditional feminine norms, “compounding” the stigma they face (Piatkowski et al., 2023b). As a result, women's consumption of PIEDs is perceived as a more extreme departure from these norms, further marginalizing women in this context. We extend on these discourses, adding that perhaps as a result of this “erosion,” women have reportedly become reliant on others to provide advice about their substance regimes to maintain a balance between femininity and health (Börjesson et al., 2016; Kotzé et al., 2020).
In different countries, the legal status of AAS varies, leading to specific harm patterns associated with their use that depend on the region (Piatkowski et al., 2023a). For example, in jurisdictions where AAS use is legally allowed, about 60% of female users reported receiving advice or prescriptions from licensed medical professionals (Santos et al., 2023). Resultantly, these socio-political differences give rise to information regarding AAS reaching end-users in different ways. For example, in areas where AAS possession and use are prohibited, male partners have been identified as facilitating and guiding AAS use (Dunn et al., 2023; Havnes, Jørstad& Bjørnebekk, 2021; Havnes, Jørstad, Innerdal et al., 2021; Piatkowski et al., 2023b). For men who use PIEDs, they often inject with others, particularly within training partnerships and social or intimate settings, especially during initiation phases (Fomiatti et al., 2020); therefore, we draw on these social dynamics and extend them to women. Specifically, Fomiatti et al. (2023) go on to suggest there are varied interpretations and behaviors surrounding women's consumption of substances for fitness and strength training and we should take care not to reinforce assumptions of female vulnerability and passivity. They emphasize the portrayal of agency in discussions of health risks and initiation experiences and the importance of contextualizing women's consumption practices within wider cultural shifts toward health optimization and digital fitness cultures.
Building on Fomiatti et al.'s (2023) valuable insights for interrogating the nexus of women's PIED consumption within the context of gendered practices, we explore these interpersonal relationships, as related to gendered PIED practices. We do so by utilizing an intersectional perspective on femininity and the enhanced body (Andreasson & Henning, 2022). Theories of intersections between gender, sexuality, class, and ethnicity are used to investigate the different sociocultural categories (and national contexts) that influence the individual, constituting flexible and complex processes of belonging, identity, and power relations (Andreasson & Henning, 2022). Understanding women's use of PIEDs, within the context of gender, is successively altered by the intersection with other categories (Christensen & Jensen, 2014). This intersectional framework acknowledges the multi-dimensionality of societal factors, identities, and power. Such systems of stratification also emerge in the context of PIED use, potentially influencing how this unique group is understood and how risks with use eventuate. Intersectional positions are, thus, situated and contextual, resulting in complex and potentially ambiguous social relations. Applying this approach to power and identity (Andreasson & Henning, 2022; Christensen & Jensen, 2014) in combination with current evidence suggesting men have a role in women's PIED use (Börjesson et al., 2016; Dunn et al., 2023; Havnes, Jørstad, & Bjørnebekk, 2021; Piatkowski et al., 2023b), we investigated how women's approach to PIED use is facilitated. This study aimed to explore women's motivations for PIED use; to examine the negative health experiences related to use; and to understand how interpersonal relationships facilitate their use.
Methods
Sampling and Recruitment
This qualitative project comprised two components: online surveys and interviews. A purposive sample was recruited via research team contacts and networks and also through snowball sampling. Recruitment advertisement included a link and QR code to a short Qualtrics survey that included questions about participant's eligibility for the study, details about the study, plain language statement, and consent form. Participants were eligible if they identified as women, aged 18 years or above, and had ever used PIEDs such as AAS. Those who completed the first phase of the study (survey) were offered the chance to enter a draw to receive a $20 Visa gift card. Those who participated in the second phase of the study (interview) received a $50 Visa gift card as a reimbursement. Participants were able to participate in either phase of the study without being involved in both phases. Ethical approval was granted from the University Human Research Ethics Committee (Approval: 2022-156).
Data Collection
Phase 1: Survey
The first phase of this project invited participants via a link to an online survey to provide demographic information regarding themselves, as well as a history of PIED use, and associated side effects. The survey also asked participants for extended responses to three questions: (1) Why do you believe you use PIEDs?, (2) Can you tell us about a negative health experience you have had from using PIEDs?, and (3) Who supports you in your PIED use? The three questions allowed for open ended responses, with prompts indicating what participants could consider when responding.
Phase 2: Interviews
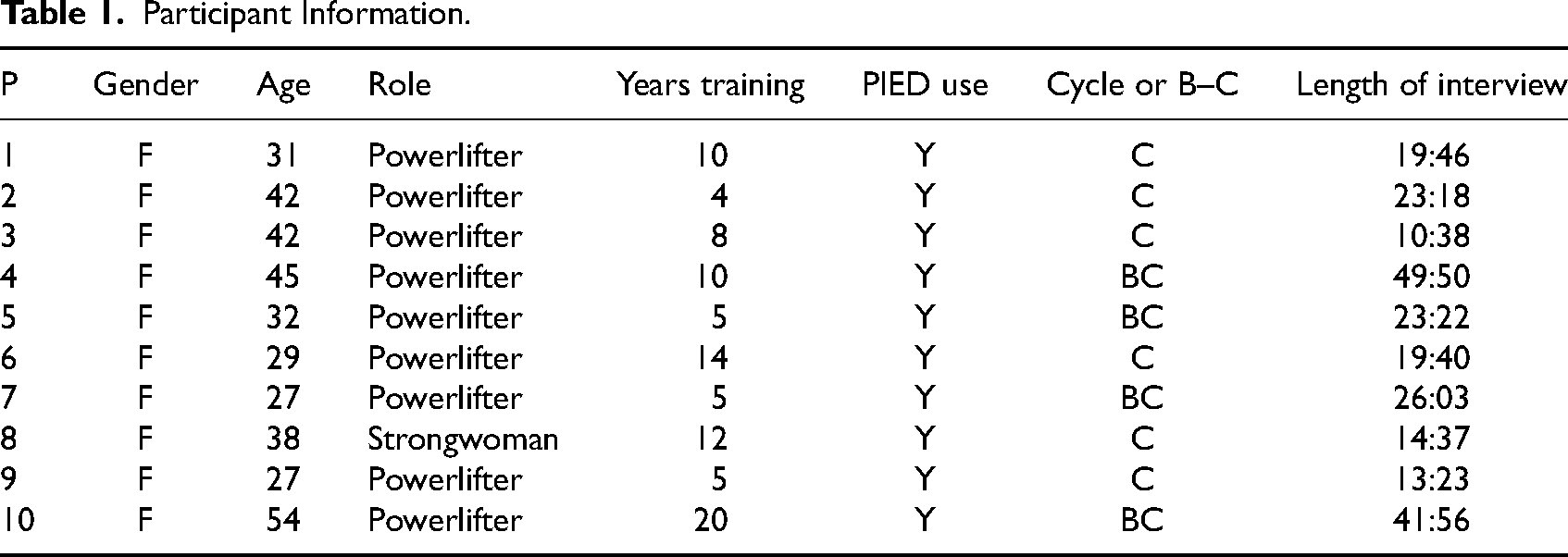
The second phase consisted of semi-structured, in-depth interviews with women who were using PIEDs, see Table 1 for details. The interviews were conducted online via the Zoom platform with one member of the research team. Interviews focused on the lived experience of these women, exploring how use was initiated, continued motivations for use, the health outcomes experienced, and how personal relationships influenced use and knowledge. A semi-structured interview guide was developed. Questions sought to explore motivations for PIED initiation and continued use, and the relationships participants had in their life that were linked to PIED use (e.g., Could you tell me a little bit about who helps you with your PIED use?). Interviews were digitally recorded and transcribed verbatim.
Participant Information.
Data Analysis
Approach
In the academic discourse surrounding gender and PIEDs, the concept of hegemonic masculinity has been a central point of discussion. In this context, being male and heterosexual can be considered as occupying a dominant position, whereas being female, working class, and belonging to a minority population can be seen as a marginal position (Toyoki & Brown, 2014). Hegemonic masculinities have sometimes been utilized in studies on PIED use to characterize a type of “traditional” or conventional masculinity (Christiansen, 2020). In this context, men involved in PIED use are often perceived as adhering excessively to stereotypical notions of masculinity, emphasizing traits like muscularity, performance, dominance, and rationalized lifestyles. However, an issue that scholars have raised with the application of this framing of masculinity is that it can lead to an almost absolute and unquestioned understanding of power dynamics, particularly regarding men's dominance over women (Sverkersson et al., 2023). Such viewpoints contrast sharply with alternative forms of resistance discussed in critical studies on both men and masculinity (Latham et al., 2019) as well as women and gendered notions of PIED use (Fomiatti et al., 2023). We complement these views by drawing on an intersectional perspective. By considering the intersections of gender, sexuality, class, and ethnicity, we aim to provide further understanding surrounding the complex social dynamics shaping women's engagement with PIEDs.
Analytic Process
The data from the survey were aggregated and screened for missing values (IBM Statistics version 28). Descriptive statistics and frequencies were calculated. The qualitative data collected from the survey and the interviews were pooled and analyzed concurrently in NVivo.
For the survey data, a content analysis of the open-text responses in the survey was conducted. A general inductive approach for raw data analysis was adopted (Thomas, 2006). This approach entailed preliminary analyses of the raw content ensuring frequently occurring themes and categories could be identified. A total of 60 text responses were analyzed (20 comments for each open-text question). Emergent coding methods were utilized to create categories from the data as they were analyzed (Erlingsson & Brysiewicz, 2017). The lead author generated a codebook of frequently occurring categories with guidelines and examples for each category (Erlingsson & Brysiewicz, 2017). The comments were divided into various sub-classifications, and then further aggregated into categories intended to reveal the manifest content of the data (Erlingsson & Brysiewicz, 2017). Lastly, the latent content of the categories was formulated into overarching categories (Erlingsson & Brysiewicz, 2017; Lindgren et al., 2020).
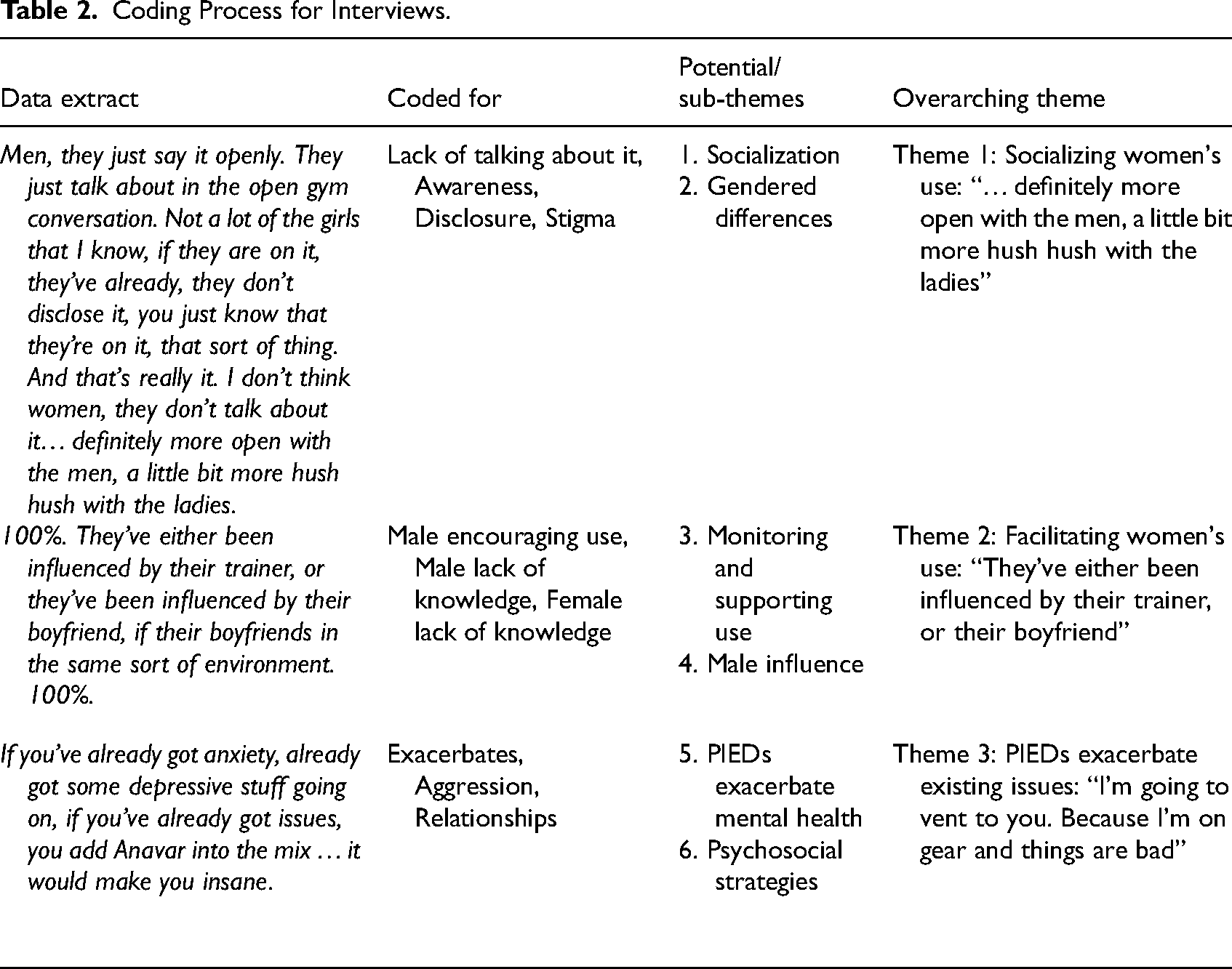
The interview data were analyzed using thematic analysis (Clarke et al., 2015). Thematic analysis followed Braun and Clarke's (2019) six-step guide involving data familiarization; initial code generation; identification of potential themes; review of themes; defining/naming themes; and writing up findings. Inductive analysis (Neuendorf, 2018) was used to identify codes that were synthesized into themes to summarize the key findings from the interviews. The team met regularly to discuss and review this categorization to arrive at final themes and through an iterative consensus decision-making process. Representative verbatim quotes were selected to best illustrate the themes and the underlying content within—see Table 2 for a summary of the coding process.
Coding Process for Interviews.
Results
Descriptive Survey Results
Demographics
All participants who completed the survey identified as female (N = 28). Of these females, 21 identified as heterosexual, one as homosexual, and six as bisexual. The average age of the cohort was 32.96 years (SD = 6.57, range = 23–46) with a mean height of 165.05 cm (SD = 5.25, range = 157–175) and weight of 81.04 kg (SD = 15.95, range = 56–131). Of the females who reported their body fat percentage (n = 11) the average was 22.41% (SD = 5.82, range = 14–35). Participants all resided within Australia, predominantly within Queensland (42.9%), Victoria (21.4%), and New South Wales (17.9%), with lesser representation from Western Australia (7.1%) and Tasmania (7.1%).
Training and Competition
Eight participants (28.6%) had ever competed in a bodybuilding competition. On average, participants had weight trained for 9.35 years (SD = 3.53). At the time of the survey, participants weight trained approximately four-and-a-half days per week (SD = 0.82) out of seven, on average. In terms of their training, approximately two-thirds (64.3%) of participants performed weight training with minimal/no cardiovascular training, while one-third (35.7%) performed both weight training and cardiovascular training, but primarily weight training. Most participants normally trained at a local, non-commercial gym (82.1%) with some training at commercial gyms (17.9%). Almost three-quarters (71.4%) of the group preferred to train by themselves as opposed to in a group. Most of the females had a coach (85.7%). Over half of the participants (60.7%) were preparing for a competition at the time of the survey.
Performance and Image-Enhancing Drug Use
All participants had used PIEDs such as AAS in their lifetime. The types of AAS participants used included: Oxandrolone (92.9%), Testosterone (39.3%), Drostanolone (28.6%), Methenolone (21.4%), Nandrolone (25.0%), Trenbolone (17.9%), Fluoxymesterone (17.9%), Stanozolol (14.3%), Methandienone (14.3%), Oxymetholone (14.3%), Chlorodehydromethyltestosterone (10.7%), and Boldenone (7.1%). The types of other PIEDs participants used included: Clenbuterol/Albuterol (42.9%), Selective Androgen Receptor Modulators (SARMs; 35.7%), Human Growth Hormone (HGH; 32.1%), Peptides (17.9%), Thyroid Hormones (14.3%), Insulin (10.7%), and Insulin-like Growth Factor 1 (IGF-1; 10.7%). At the time of the survey, 19 participants were using PIEDs and nine were not.
Females in this cohort typically opted to cycle their PIED use (78.6%) rather than blasting and cruising (21.4%). As per Dunn and Piatkowski (2021), cycling compounds refer to using these substances intermittently with regular breaks, for example, 12 weeks of use followed by 12 weeks abstaining from use. Blasting and cruising refers to using a dose of some compound (e.g., testosterone) constantly, and increasing the dose and/or adding compounds during “peaking” periods, for instance around competition time.
Content Analysis of Survey Responses
Consistent with the aim of the study, the motivations for use, negative health experiences related to use, and the role that third parties in initiating and maintaining use were revealed through content analysis. Analysis of comments identified the following 12 categories displayed in order of question posed and then by popularity (see Table 3 for example quotes).
Frequency Count of Participant Comments in Each Question Category With Accompanying Example Quotes.
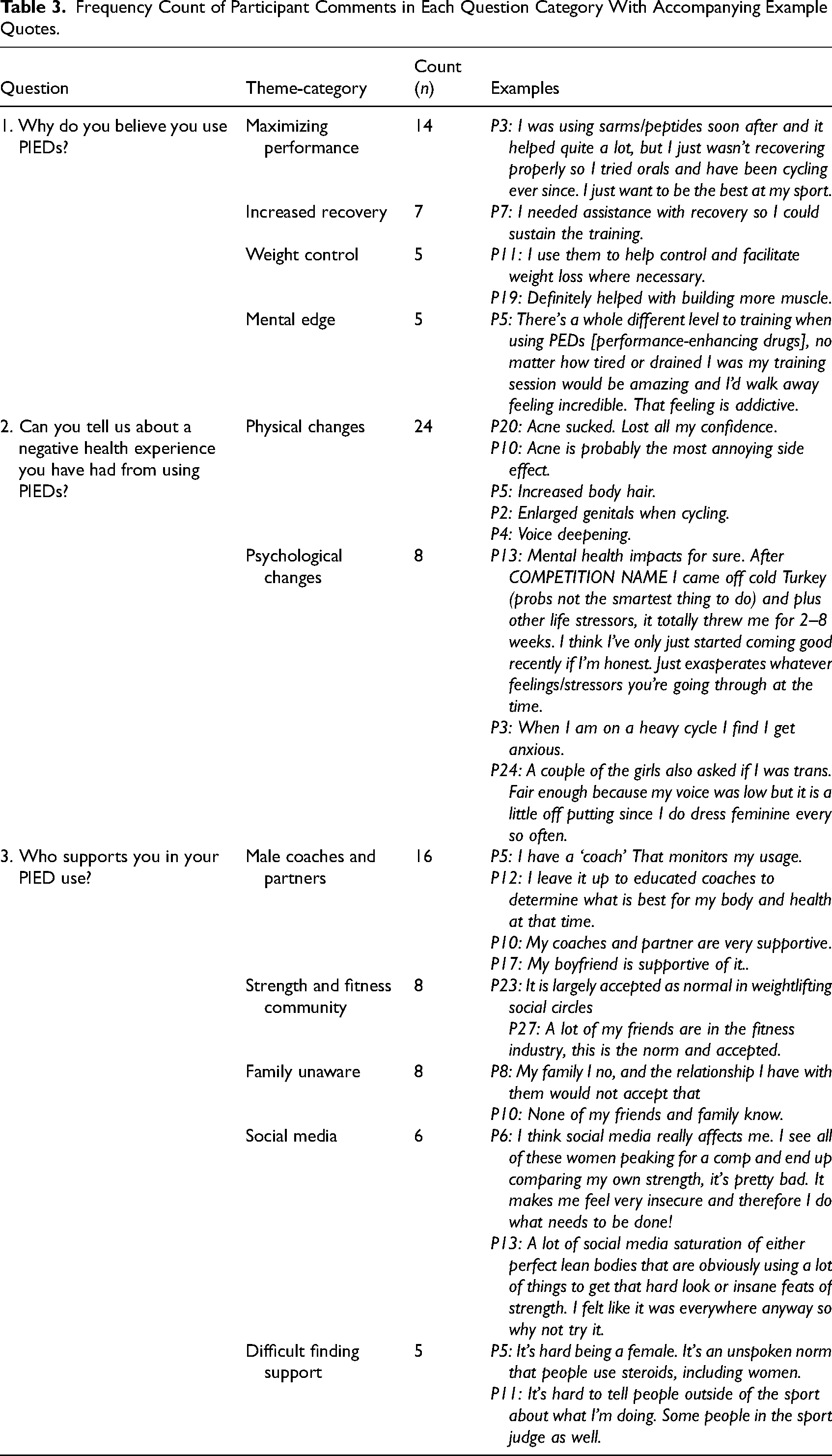
Why do you believe you use PIEDs: The overarching reasons for using PIEDs were: maximizing performance with the intent of positive competition outcomes (n = 14), optimizing recovery (n = 7), controlling weight (n = 5), psychological elements (n = 10), specifically increased confidence (n = 4), body image (n = 3), energy (n = 2), motivation (n = 2), and sex drive (n = 1).
Can you tell us about a negative health experience you have had from using PIEDs: The negative health experiences females were categorized into physical and psychological aspects. The physical aspects included: acne (n = 7), hair growth or loss (n = 4), voice changes (n = 4), clitoral enlargement (n = 2), menstrual changes (n = 2), tremors (n = 2), sexual drive changes (n = 1), sleep issues (n = 1), and blood pressure changes (n = 1). Females acknowledged psychological side effects more broadly (n = 8), such as increased anxiety (n = 3), depression (n = 1), paranoia (n = 1), and how virilization affected their femininity (n = 3), which reportedly took a psychological toll. One woman underscored that side effects were particularly “worse” when using injectable AAS rather than oral derivatives. This complements previous work which has demonstrated women's preference to use oral derivates (Havnes et al., 2021, Piatkowski et al., 2023b) and offers a suggestion as to their motivations for doing so.
Who supports you in your PIED use: Females acknowledged the supportive role of other people in their use including coaches (n = 12), strength training and fitness communities (n = 8), social media (n = 6), and partners (n = 4); however, family and close friends were often unaware of their use (n = 8). Some females acknowledged it was difficult finding support as a woman who uses PIEDs (n = 5).
The predominant reason women reported using PIEDs was centered around maximizing performance, overcoming injury, and decreasing recovery time, which is an area they share semblance with men (Greenway & Price, 2018; Santos & Coomber, 2017; Underwood et al., 2021). Furthermore, women reported increases in confidence, body image, sex drive, and energy that are similarly described among men (Harvey et al., 2022; Havnes et al., 2019; Piatkowski et al., 2020). Participants reported distinct physical (e.g., acne, voice deepening) and psychological (e.g., depression, anxiety) side effects of PIED use, which fit with extant work (Börjesson et al., 2016; Havnes, Jørstad, Innerdal et al., 2021; Ip et al., 2010). They also discussed the social influences facilitating their use, of which close males in their lives made up a large proportion, substantiating previous studies (Börjesson et al., 2016; Havnes, Jørstad, Innerdal et al., 2021). The interview data extended on the survey findings, underscoring how women's PIED use, holistically, was different from that of men.
Thematic Analysis of Interviews
Theme 1: Socializing Women's use: “… Definitely More Open with the men, a Little bit More Hush Hush with the Ladies”
Participants expressed a narrative around the social aspects that surrounded women initiating and continuing PIED use. For example, one of the prominent ways in which women initiated PIED use was through strength sport participation. This parallels with research findings that more women have joined recreational sports and fitness activities (Andreasson & Johansson, 2014), with some turning to PIED use influenced by societal body ideals (Piatkowski et al., 2023b). Part of this relationship with substance consumption appears to intersect involvement in sport and competition, through which PIED use emerged as a component of social influence:
P4: I saw that a lot of the elite level athletes, that I was looking up to and chasing, were on [PIEDs].
P3: And it's also the culture in a nutshell, if you’re around enough people that take performance enhancing drugs, it becomes less taboo because they’re like, well, we do it, why wouldn’t you do it?
P5: Somebody sourced them for me and gave me them. It was just someone that I knew from the gym, and they gave me like, what I call now ‘bro advice’ on what to do.
P10: My friends outside the gym, they had no idea except one or two really close that I knew would not be judgmental in any way. Even my, because I was married at that time, he still had no idea.
P7: Men, they just say it openly. They just talk about in the open gym conversation. Not a lot of the girls that I know, if they are on it, they’ve already, they don’t disclose it, you just know that they’re on it, that sort of thing. And that's really it. I don’t think women, they don’t talk about it … definitely more open with the men, a little bit more hush hush with the ladies.
P2: Yeah, it's hard for women. The blokes are very open. They all talk to each other; they’re all comparing where they get it from and what side effects and what's going. It's all very open with them. Women, you just can’t because 90% of the time you’re going to get a nasty reaction.
Theme 2: Facilitating Women's use: “They’ve Either Been Influenced by Their Trainer, or Their Boyfriend”
Although there were some women who asserted their agency, many participants discussed the role of men in facilitating women's PIED use more broadly. Particularly when discussing other women in their social circles, the women interviewed believed that men influenced females' choices to use PIEDs either in a role as a coach or as a romantic partner. These narratives shared by women illuminate the gender dynamics within drug cultures and communities. While both men and women may encounter risks associated with their use (Andreasson & Henning, 2022; Piatkowski et al., 2023c), women appear to contend with an additional layer of challenges stemming from the predominantly male-centric cultural context.
P5: 100%. They’ve either been influenced by their trainer, or they’ve been influenced by their boyfriend, if their boyfriends in the same sort of environment. 100%.
P1: That's another thing that really bothers me. Like, there's so few coaches in Australian bodybuilding and they tell the girls what to take.
P2: I have a lot of ‘Gym Bro’ recommendations of what I should take and what you should take for females. And pretty much everyone just told me Anavar [Oxandrolone].
However, there were other participants who were alarmed by the type of suggestions that men made regarding the type of compounds and dosages that females should be using. These suggestions were both made directly to them or had, inadvertently, been communicated through social circles. Some participants, who reported significant personal experience, spoke directly of the advice they had received which they believed was clearly inappropriate or misleading.
P7: So, blokes will suggest all kinds of crazy s**t that women should never go anywhere near. They were telling me to take growth hormone, Deca [Nandrolone] and there was all sorts of things that they suggested.
P1: That's what a lot of coaches are doing. Coaches for bikini and physique and things like that, they’re putting females on Tren [Trenbolone], test [Testosterone] and they’re also putting them on estrogen blockers to get them stage lean because they might hold water.
P10: Because the sports modelling and fitness has exploded and it's particularly for the young girls, they’re even being told beyond Anavar and Clenbuterol and T3 [Triiodothyronine] is, use some ice [crystal methamphetamine] or use speed [amphetamine].
Theme 3: PIEDs Exacerbate Existing Issues: “I’m Going to Vent to You. Because I’m on Gear and Things are bad”
Some scholars have asserted the paradox of PIED use, represented by the desire to improve well-being with a substance that impacts health detrimentally in other ways (Harvey et al., 2022). Women reported that using PIEDs, particularly AAS, had pronounced psychological effects on them. These experiences intersect with those of men who use PIEDs (Piatkowski et al., 2023b, 2023c), indicating common psychological impacts across genders. Many participants discussed distinct mental effects that using these compounds had on them, for example:
P4: Am I psychologically even more imbalanced on PEDs [performance enhancing drugs]? Absolutely.
P2: I’m a lot more grumpier than usual … I’ve noticed my anxiety goes up significantly when I’m on Anavar [Oxandrolone].
P9: [On using AAS] I found that it exacerbated my lack of patience.
Overall, there was a narrative from participants regarding existing mental health symptoms and the way in which using AAS interacts with those factors. Some participants expressed that if women intending to use AAS were considering doing so, pre-existing symptoms could lead to deleterious consequences. P9: If you’ve already got anxiety, already got some depressive stuff going on, if you’ve already got issues, you add Anavar into the mix … it would make you insane. P4: Like when you’re in the middle of a cycle like, you’re fairly deep into it … You definitely notice, like I, I’ve got this expression of you’ve got to cultivate your Zen.
P7: If I have a bit of a mental break or need it, I will definitely tell my coach straight away and maybe we’ll go seek help from there.
P8: I was speaking to my coach about this [mental effects] the other day, and it wasn’t about drugs, it was just about depression.
P4: I’ve got one really close friend in particular. And that is literally our job for each other. We are like, okay, I’m going to vent to you, because you know, I’m on gear and things are bad. And I know it's completely irrational, but I’m just going to tell you all this s**t, and you’re gonna go, yeah, it's all good, you’re fine, no worries. And then I’m going to feel better and move on.
Discussion
This research examined the intersecting dynamics of gender in women's PIED use. Firstly, our study reveals that women primarily use PIEDs to maximize performance, optimize recovery, and control weight, aligning with similar motivations reported among men. The data support Fomiatti et al.'s (2023) observation that women's PIED use mirrors conventional norms of feminine bodily care and management, yet it also highlights the stigma attached to it. This emphasizes the importance of incorporating gendered perspectives into the comprehension of PIED use and associated behaviors. Secondly, our data highlight the diverse range of negative health experiences associated with PIED use among women, both physical and psychological. When discussing the effects of PIEDs, particularly AAS, on themselves, women highlighted the exacerbated effects these substances had on their mental health. Many suggested they had pre-existing mental health symptoms, which fits previous work among men (Chegeni et al., 2021; Havnes, Jørstad& Bjørnebekk, 2021; Piatkowski et al., 2021) and women (Piatkowski et al., 2023b, 2023c; Scarth et al., 2022). Participants specifically reported that the use of AAS was believed to increase anxiety and depression and that women considering use should be appropriately forewarned. Thirdly, our findings elucidate the significant role of interpersonal relationships, particularly with male peers, in initiating and maintaining PIED use among women. Participants discussed the social components that contribute to how their use is supported and monitored, in which men were heavily represented in the form of “gym bros,” partners, and male coaches. Despite relying on male peers for guidance, women navigate physical and psychological side effects by seeking support from other women who use PIEDs. They had, through these organic networks, also cultivated some psychosocial strategies to mitigate these deleterious mental effects, such as peer harm reduction. The findings suggest these peer relationships and safe spaces contrast sharply with the stigmatization women experience in discussing PIED use in broader social contexts (e.g., family and non-“gym” friends).
For women who use PIEDs, there are interpersonal relationships that facilitate their use of these substances. These relationships are closely related to the power dynamic existing from an intersectional perspective on femininity and the enhanced body (Andreasson & Henning, 2022). Specifically, for men, the various categories of PIED users have been described in language that emphasized traits and values commonly associated with traditional masculinity, such as achievement, dominance, exploration, risk-taking, expertise, and self-restraint (Christiansen et al., 2017; Zahnow et al., 2018). By contrast, when approaching women's use of PIEDs, scholars and the public tend to sensationalize the matter and view it as deviant and unusual (McGrath & Chananie-Hill, 2009; Shilling & Bunsell, 2009). Given the conceptualization of PIED use largely through the lens of male hegemonic patterns (Andreasson & Henning, 2022), the question remains regarding how best to reorient discussions of PIEDs with consideration given to women's perspectives and experiences.
Fomiatti et al. (2023) have advocated for alternative language that prioritizes specific substances (e.g., AAS) and activities (e.g., strength training) rather than reinforcing the assumed effects of substances. For example, scholars have asserted that men who use PIEDs should not be viewed as damaged and vulnerable outliers, but rather as rational and self-aware individuals who actively manage their health and wellness, often with careful consideration and expertise in navigating associated risks (Fraser et al., 2020; Latham et al., 2019; Piatkowski & Cox, 2024). Therefore, we extend this work and suggest that for women, rather than being primarily about gender and societal expectations for gender, the use of PIEDs can be viewed as an expression of female identity and agency. In this way, it can be seen as a deliberate action through which physical achievements, health, and the reduction of harm specific to women are given significance and purpose. However, we note the expression of female agency appears to be somewhat influenced by men, particularly through socialization and facilitation as demonstrated by these findings. This demonstrates the power of the socially constructed nature of narratives when it comes to substance use (McIntosh & McKegany, 2000) and the potential for those narratives to pervasively continue if left unchecked. Notably, as evidenced by the current data, there is some development of exclusively female ways of “doing” social relations around PIED use (e.g., female-to-female peer consumer connections). However, the question remains, where to from here?
Although evidence is limited, there is research that shows improving health literacy among people who use substances has contributed to improved health outcomes (Rolova et al., 2021). The present study introduces the scope of interventions beyond what is presently envisioned by public health research in this area specifically. For instance, interventions geared toward substance literacy could be implemented to promote the development of women's knowledge regarding the substances they are using as well as stigma management strategies. At the same time, structural interventions are required to modify both the linguistic and material aspects of the social relationships that both constitute and restrict such potential interventions. The reason for providing health literacy to women who use PIEDs lies in the enhancement of their autonomy (Joosten et al., 2011) over health-related choices. Further research is required to ascertain whether health (substance) literacy, for this cohort may be an appropriate avenue for future intervention.
Limitations
Although a semi-structured interview protocol and prompts were used to encourage participants to speak about their experiences at length, interview times did vary (11–51 min). There was a strong representation of strength athletes in the participant pool and, therefore, the data reported are not necessarily generalizable to all women who use PIEDs. We recognize the significant role researchers have in shaping perceptions of drug-related effects, harms, and what is considered “real,” acknowledging scholars’ emphasis on the need for heightened awareness in designing and conducting research (Fraser et al., 2020; Seear et al., 2020). Consequently, we were encouraged to reflect on the research methodologies and how these influenced the interpretations we have made. Particularly regarding the directionality of asking participants of “negative health experiences,” we acknowledge that this may have led to a focus on negative outcomes. Further research is required to encompass a broader group of women and preferably acknowledge the inherent potential for positive elements associated with the use of these substances.
Conclusions
The current study explored the lived experience of women who use PIEDs to understand their motivations and health experiences and to understand how interpersonal relationships facilitate use. These findings demonstrate that women's motivations for PIED use align closely with those reported among men. Notably, both men and women face stigma for their PIED use; however, the stigma experienced by women is often also influenced by societal norms surrounding feminine bodily care and management, adding a unique layer to their experiences. Resultantly, perhaps, women also seek support from other women who use PIEDs, forming organic networks and cultivating psychosocial strategies to mitigate adverse effects. Moving forward, it is crucial to reorient discussions of PIEDs with consideration given to women's perspectives and experiences. Interventions focusing on substance literacy and stigma management strategies are essential to enhance women's autonomy over their health decisions.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article. This work was supported by the Deakin University (grant number Centre for Sport Research Grant).