
Abstract
Scholars have argued that stigma of opioid use disorder (OUD) is a significant barrier to implementing evidence-based responses to the opioid crisis, including the use of medications for opioid use disorder (MOUD). They have also documented a relationship between addiction frameworks and support for punitive responses to substance use. Using a representative sample of Pennsylvania residents (N = 1,033), the current study synthesizes this literature by empirically examining the relationship between addiction frameworks, opioid-related stigma, and policy-related attitudes (i.e., NIMBY syndrome, support for punitive treatment of OUD, and support for employment discrimination against individuals prescribed MOUD). Results show that support for the disease model of addiction was negatively associated with endorsing NIMBY syndrome for opioid-treatment centers, support for punitive treatment of OUD, and support for employment discrimination against individuals prescribed MOUD; however, these relationships were fully mediated by opioid-related stigma, such that support for the disease model of addiction impacted outcome measures only indirectly through opioid-related stigma. Policy implications are discussed within.
Introduction
The opioid epidemic is a public health emergency that continues to escalate in the United States (U.S.). It is estimated that 9.5 million people misused opioids in the past year with more than a quarter meeting the criteria for opioid use disorder (OUD; SAMHSA, 2021a). Between 1999 and 2020, overdose deaths increased by more than 500% (WONDER, 2021). A wave of prescription opioid deaths in the early 2000s followed by rapid increases in heroin-related overdose deaths a decade later triggered a public health response (CDC, 2011; Rudd et al., 2014). In recent years, overdose deaths have continued to rise due in part to the rise of synthetic opioids, particularly fentanyl. The COVID-19 pandemic further exacerbated risk factors related to illicit opioid use and overdose including increased social isolation, changes to the drug supply, disruptions to treatment initiation and completion, and decreased availability of medications for opioid use disorder (MOUD; Linas et al., 2021; Macmadu et al., 2021). Consequently, in 2021, 107,622 individuals lost their lives to a drug overdose—the majority from opioids—the highest number of overdose deaths on record (CDC, 2022a).
There has been a federal response to curb overdose deaths and thwart the opioid epidemic. For example, the medical community took action to decrease opioid prescribing which, due to these efforts, decreased by 33% between 2013 and 2018 (Harris & Mukkamala, 2020). To aid in this endeavor, prescription drug monitoring programs were developed to collect opioid-related data from pharmacies and report any high-risk behaviors on the part of patients (e.g., “doctor shopping”) or providers (e.g., prescribing high doses of opioids). Implementation of prescription drug monitoring programs has been associated with a decrease in opioid-related deaths (Patrick et al., 2016). In conjunction with targeting use of and access to opioids, there has been a push to increase the number of Drug Addiction Treatment Act (DATA)-waived practitioners across the country to expand the availability of buprenorphine, the “gold-standard” treatment for OUD (SAMHSA, 2021b; U.S. Department of Health and Human Services, 2021). Originally applying only to medical doctors, the Comprehensive Addiction and Recovery Act (2016) extended buprenorphine prescription authority to nurse practitioners and physician assistants. Additionally, expanding access to Naloxone by targeting and increasing co-prescribing has made a considerable impact with less than 7,000 Naloxone prescriptions in 2015 to over a million by 2019 (AMA, 2020). Utilization of MOUD is also a promising response to the epidemic, with data showing MOUD to be associated with better treatment retention rates (Timko et al., 2016) and decreased risk of overdose death (Ma et al., 2019).
Pennsylvania, one of the hardest hit states in the country, has been coordinated in its response to the opioid epidemic, at the state level. In Pennsylvania, rates of OUD are slightly above the national average (0.8% compared to 0.7%) with an annual prevalence averaging 84,000 people per year from 2017 to 2019 (SAMSHA, 2020). A decline in overdose deaths in 2018 was quickly followed by a 14% increase from 2019 to 2020 (Pennsylvania Department of Health, 2022). In 2020, and every year since, over 5,000 Pennsylvanians died of a drug overdose (CDC, 2022b), representing a rate of about 42–43 per 100,000 individuals each year (CDC, 2022a). Pennsylvania has consistently ranked in the “Top 10” states for highest drug overdose deaths over the last decade (CDC, 2022a). Addressing the opioid epidemic has been a top priority at the state level in Pennsylvania, as evidenced by the opioid disaster declaration and formation of a dedicated opioid response task force (Commonwealth of Pennsylvania, 2018). The statewide coordinated response has included the creation of an opioid data dashboard to track opioid-related trends, prescription drug monitoring, increased access to Naloxone (e.g., standing order, mail order, and drive-thru events), a dedicated substance use treatment hotline, increased availability of MOUD in correctional settings, expansion of provider service and capacity, and increased support for individuals in recovery. However, county-level implementation of these evidence-based responses has not been uniform; while some counties have implemented progressive, evidence-based responses to the crisis, others have taken punitive approaches, consisting of harsh prosecutions of people who use opioids and banning or limiting access to medication-assisted treatments for dependency, including MOUD. In fact, the U.S. Department of Justice recently sued Pennsylvania's court system for allowing counties to use such punitive responses to the opioid crisis, alleging that Pennsylvania's court system discriminated against individuals with OUD by providing inadequate and unequal access to MOUD, jeopardizing countless lives (Mahon, 2022). Indeed, harm reduction, broadly, continues to be a highly disputed facet of substance use treatment in the community and in the criminal justice system. Other researchers have found that stigma may be negatively related to support for harm reduction and could influence system responses to OUD (see Kruis et al., 2021; McGinty et al., 2018). Given that public attitudes can influence system-level responses to social crises, the goal of the current project was to build upon this literature base by assessing public support for punitive treatment of people who use opioids, support for discriminatory employment practices against those who are prescribed MOUD, and endorsement of NIMBY 1 syndrome for opioid-treatment facilities in Pennsylvania. Specific focus was given to exploring the role addiction frameworks and opioid-related stigma play in shaping support for these policy-related variables.
Literature Review
Social Stigma
An early conceptualization of stigma suggests an individual with an “attribute that is deeply discrediting” which leads society to discount that individual (Goffman, 1963, p. 3). The definition of stigma has since expanded to include the devaluing of a stigmatized individual through labeling, stereotyping, discrimination, and social exclusion (Link & Phelan, 2001). This “us” versus “them” mentality results in a desire for social distance or the avoidance and exclusion of the stigmatized group from interacting with society at large (Lucas & Phelan, 2012; Morone, 1997). Many types of stigma have been identified (e.g., self-stigma, enacted stigma, and structural stigma) but the focus of the current study is on social stigma. Social stigma is the public endorsement of stereotypes (i.e., thoughts) which can lead to the sanctioning of discriminatory behaviors (i.e., actions) toward individuals with a substance use disorder (SUD; Corrigan et al., 2017). Societal norms can deem certain traits unacceptable—individuals who embody these traits are subsequently shunned (Corrigan et al., 2005). Even among stigmatized disorders (e.g., depression, schizophrenia), individuals with SUD may be at increased risk for social stigmatization (Corrigan et al., 2009). This may, in part, be related to how social stigma manifests in the general public. Recent studies on social stigma and the opioid epidemic (Kruis et al., 2020; Kruis & Choi, 2020) have built on mental health stigma literature (National Academies of Sciences and Medicine, 2016) and identified four key components of social stigma of SUD, 2 including perceptions of dangerousness, blameworthiness, and fatalism, as well as a desire for social distance.
Dangerousness
Perceptions of dangerousness refer to the public's belief that individuals with a stigmatizing disorder will hurt themselves or others, are to be feared, or are a nuisance or threat to society (Pescosolido & Martin, 2015). There is a pervasive myth that people who use drugs are immoral and will commit any crime or depravity to feed their addiction (Hammersley & Reid, 2002). Previous studies have found that the public views individuals who use drugs as potentially dangerous and violent (Barry et al., 2014; Link et al., 1999; Schomerus et al., 2011).
Blameworthiness
Many individuals blame those who use drugs for “choosing” to use drugs in the first place and/or choosing to continue to use despite the risks involved (Lloyd, 2013). For example, one survey on public attitudes about substance use found that 45% of the respondents believed that “most people who end up addicted to heroin only have themselves to blame” (Ormston et al., 2010). Consequently, when individuals with SUD are judged to be responsible for their substance use and the resulting negative consequences, society tends to have less empathy for them (Corrigan et al., 2003; Hegarty & Golden, 2008).
Social Distance
Many members of the lay public are reluctant to interact with members of a stigmatized group (Pescosolido & Martin, 2015). This desire for interpersonal distance (i.e., social distance) is often how stigma is operationalized in studies of mental health and SUD (Corrigan et al., 2017; Crapanzano et al., 2019). In the United States, willingness to socially exclude individuals with OUD is high. For example, recent studies have found that most respondents are unwilling, or at least reluctant, to work closely with a person with OUD (Kaynak et al., 2022; Perry et al., 2020).
Fatalism
Fatalism in substance use refers to the public's belief that an individual with OUD will never get better, no matter what the public does to help or what the individual does to overcome their disorder. Fatalism is often measured by asking respondents whether individuals with SUD or OUD will recover from their disorder or whether effective treatments for SUD or OUD are available. One national survey found that 30% of the respondents endorsed that recovery from SUD was impossible and 59% endorsed that SUD treatment was ineffective (Barry et al., 2014). More recently, a statewide survey found fatalism to be lower, with 6% of respondents disagreeing that there are effective treatments available for OUD and 14% disagreeing that recovery from OUD was probable with effective treatment (Kaynak et al., 2022).
Social Stigma as a Barrier to Opioid Treatment and Recovery
Social stigma has implications for treatment initiation, utilization of evidence-based treatment, and availability of effective treatment, and thus is considered a barrier to responses to the opioid epidemic (Tsai et al., 2019). Social stigma can contribute to health inequities that undermine treatment and recovery and create disparities within substance use epidemics (Earnshaw, 2020; Hatzenbuehler et al., 2013). For example, within the opioid epidemic, stigma can vary based on several factors including details surrounding opioid initiation (i.e., being prescribed opioids for an injury vs. recreational use), the social identity and social network of the individual who is using (i.e., a poor and minoritized user vs. a middle class and White user), type of opioid used (i.e., prescription opioids vs. heroin); and treatment of OUD (i.e., MOUD vs. abstinence-based treatment; McCradden et al., 2019). Stigma is consistently endorsed as a barrier to treatment, although few studies have tied it directly to treatment-seeking behavior (Hammarlund et al., 2018). That said, recent stigma monitoring in Australia by Broady et al. (2022) found that stigma influenced the health-seeking behaviors of people who inject drugs (PWID) and that many PWID reported receiving negative treatment by health workers. Social stigma can have other treatment implications too, including limiting access to effective treatments, like MOUD. Treatment with methadone or buprenorphine reduces cravings and relapse as well as reduces the risk of overdose and death (Allen, Nolan, et al., 2019). Despite this, less than 50% of substance use treatment programs serving adults and adolescents offer MOUD, and even when it is offered, medication is underutilized (Knudsen et al., 2011). This social stigma is not limited to individuals with OUD but also can affect the people who are providing them with treatment too. Clinicians who work in MOUD programs report social stigma associated with the medication, the clients who receive it, and the counselors who provide treatment (Oberleitner et al., 2021). Closely related is the social stigmatization of the treatment programs themselves. The systemic stigmatization of evidence-based services has shaped the public health landscape in the United States in a way that makes it difficult for certain groups of people to attain the support they need in treatment and recovery (Friedman et al., 2022).
NIMBY and Support for Harm Reduction Services
One important aspect of social stigma and treatment access is the “Not in My Back Yard” (NIMBY) phenomenon, referring to community groups coming together to oppose and block services for stigmatized groups from being located in their neighborhoods. NIMBY syndrome can be a barrier to increasing the availability of harm reduction programs, such as syringe service programs (Allen, Grieb, et al., 2019). Harm reduction services utilize evidence-based approaches to treat clients where they are to reduce the negative health consequences associated with substance use (SAMHSA, 2022). Harm reduction programs offer a wide variety of services and resources which can include access to clean drug injection equipment, referrals to substance use treatment, distribution of opioid overdose reversal medication, education on preventing infectious disease transmission, testing for infectious diseases, and medical treatment (Des Jarlais et al., 2009). Social stigma toward harm reduction services has led to federal, statewide, and local bans that complicate funding and implementation of these programs (Nadelmann & LaSalle, 2017). This, in turn, makes it harder for people with OUD to access vital harm reduction services like syringe exchange (Allen, Grieb, et al., 2019; Tempalski et al., 2007).
From a community impact perspective, harm reduction programs are cost effective and reduce criminal activity; from a treatment perspective, they help reduce the transmission of infectious diseases, increase access to medical treatment, and provide much-needed social support to individuals who have been marginalized (Logan & Marlatt, 2010). NIMBY syndrome related to harm reduction often focuses on fears surrounding risks to personal security, decreases in property values, increases in people who use drugs in the area, as well as an overall threat to the quality of the neighborhood (Kolla et al., 2017). Additionally, some opponents of harm reduction believe that harm reduction condones illicit drug use and associated “immoral” behaviors (Des Jarlais, 2017). How the public frames SUD, including how it develops and how it is treated, may be related to their support or opposition for harm reduction. Moreover, in many ways, NIMBY syndrome could be the product of stigma, particularly a desire for social distance.
Addiction Frameworks
There are several ways to frame addiction, but the two most dominant models in the field are the disease model and the moral model. While definitions vary, scholars have defined the disease or medical model of addiction as perceiving SUD to be a chronic, relapsing disease that is characterized by (a) a compulsion to seek out and use substances, (b) an urge to continue substance use despite consequences, and (c) physical and emotional withdrawal if substance use is discontinued (Koob & Volkow, 2010). In our conceptual model, we perceive the disease framework as viewing substance use as a disease like diabetes, arthritis, or heart disease, with biological components and medical contributors and risk factors (i.e., genetics, chemical imbalances, etc.), which require—or at the very least, benefit—from medical intervention in the treatment process. This is a stark contrast from the moral model of addiction which does not see the need or benefit from medical intervention in SUD treatment. The moral model of addiction frames SUD as a personal choice and depicts individuals who use substances as weak, selfish, antisocial, and hedonistic (Frank & Nagel, 2017). Proponents of the disease model argue that acceptance of SUD as a disease will result in a public health-focused response that increases access to evidence-based treatment and reduces stigma (Volkow et al., 2016). The acceptance of the disease model has not progressed in the way that researchers and advocates had hoped. In 2018, 53% of Americans endorsed the belief that addiction was a disease (AP-NORC Center, 2018), but this number has remained relatively unchanged since a previous national survey in 2000 (Pew Research, 2001). A recent statewide survey in Pennsylvania found similar results with 56% of respondents agreeing that OUD is a medical illness like diabetes, arthritis, or heart disease (Kaynak et al., 2022). Studies of the association between endorsing the disease model of addiction and stigma have produced mixed results with some claiming little (Meurk et al., 2014) to no effect on public policies (Trujols, 2015). However, a recent national survey found that disregarding OUD as a medical disorder was associated with higher levels of stigma, endorsing OUD as a crime, and disagreeing with policies to increase access to OUD treatment (Taylor et al., 2021). Still, even when OUD is conceptualized as a disease rather than a personal responsibility, individuals with OUD continue to face high levels of social exclusion (Perry et al., 2020). The public's desire for social distance may be a result of the persistence of the moral model of addiction and its function in labeling an individual who uses substances as a “bad person.” In line with this, a recent national survey found that 44% of respondents said that OUD indicates a lack of willpower or self-discipline—32% said it is a result of bad character (AP-NORC, 2018). Similar results were found in Pennsylvania where 48% of respondents agreed that people who are addicted to opioids do not have the willpower to stop and 32% agreed that a lack of moral strength plays a large part in opioid addiction (Kaynak et al., 2022). Related, Broady et al. (2020) found that public attitudes in Australia toward PWID were more negative than attitudes toward other groups assessed (i.e., people living with HIV, HCI, and STIs). In their discussion, the authors made a distinction between stigmatizing behaviors, such as intravenous drug use (IDU), and stigmatizing conditions, such as people living with blood-borne viruses and sexually transmissible infections. They argued that greater stigma placed on the former group could be attributed to perceptions of IDU being a continual personal choice made that “is under the control of PWID” (p. 10), thus highlighting a potential relationship between the moral framework of addiction and public stigma.
Frameworks for addiction can impact responses to the opioid epidemic. Preliminary work has found higher levels of social stigma to be associated with higher levels of support for punitive policies and lower levels of support for public health policies like increasing access to OUD treatment and providing Naloxone to friends and family of individuals with OUD (Adams et al., 2021; Cheetham et al., 2022 ; Kennedy-Hendricks et al., 2017). Framing SUD as a treatable disease can reduce social stigma, but there are still questions as to whether that translates into support for public health policies (McGinty et al., 2015). Studies examining addiction frameworks have found that individuals who endorse a medical model for addiction are more likely to support expansion of drug treatment; those who endorse a moral model are less likely to support expansion of drug treatment (Murphy, 2017; Murphy & Russell, 2021). When the public views individuals with OUD as being “ill” and needing treatment, they are more likely to support harm reduction programs like safe injection facilities and needle exchange programs (Cruz et al., 2007). Among first responders, higher levels of support for the disease model were found to be associated with higher levels of support for the use of Naloxone (Kruis et al., 2022). However, a recent study found conflicting results in that although public support for harm reduction programs was high (64%), endorsing the disease model was related to increased levels of stigma and decreased levels of support for harm reduction programs (Wild et al., 2021). 3 While utilizing terminology like “chronically relapsing brain disease” can reduce blame attributions, it can also result in reduced optimism related to an individual's prognosis and recovery (Kelly et al., 2021). Still, knowing that the terminology used when discussing OUD can influence public support for treatment over punishment makes it vital to further explore this area. This may be especially important when garnering public support for local harm reduction services that may be susceptible to NIMBY syndrome due to the moralization of these services (Fry et al., 2005).
Current Study
Building on this literature base, the primary objective of the current study was to empirically examine the relationship between addiction frameworks, opioid-related stigma, and policy-related attitudes (i.e., NIMBY syndrome, support for punitive treatment of OUD, support for employment discrimination against individuals prescribed MOUD). Given findings from previous studies (see Kruis et al., 2022; Murphy, 2017; Murphy & Russell, 2021), we hypothesized that there would be a significant direct positive relationship between opioid-related stigma and expressions of NIMBY syndrome for OUD treatment. We also hypothesized that there would be a significant direct negative relationship between support for the disease model of addiction and NIMBY syndrome found in baseline models that did not control for opioid-related stigma. However, we anticipated that opioid-related stigma would fully mediate the relationship between addiction frameworks and NIMBY syndrome. That is, it was hypothesized that addiction frameworks would be significantly related to opioid-related stigma, which in turn, would influence respondents’ expression of NIMBY syndrome for OUD treatment. We anticipated that those who indicated support for the disease model of addiction would hold less opioid-related stigma, and in turn, would be less likely to express NIMBY syndrome for OUD treatment. It was hypothesized that similar relationships would be found between support for the disease model of addiction, opioid-related stigma, and our other outcome measures (i.e., support for punitive treatment of OUD and support for employment discrimination against individuals prescribed MOUD).
Methods
Sample
All research activities were approved by the Penn State University Institutional Review Board (IRB). Participants for this study were recruited as part of a larger project aimed at examining the nature, prevalence, and scope of opioid-related stigma in Pennsylvania (see Kaynak et al., 2022). 4 Led by the Douglas W. Pollock Center for Addiction Outreach and Research, a panel-based web survey was conducted to examine opioid-related stigma endorsed by individuals living in the Commonwealth of Pennsylvania. The survey was created by a group of addiction experts working at the research center and was administered using the Qualtrics web survey platform. Participants were recruited by Marketing Systems Group. Individuals who had previously signed up to participate in web survey panels were contacted to participate in the survey. Eligible participants were identified through demographic information provided in panelist profiles. All potentially eligible panelists were sent customized links with a respondent identifier. A series of screener questions were used to ensure the participant matched the information provided in the panelist profile and to determine if they met study inclusionary criteria. Quota-based invitation sampling was used to help produce a representative sample of Pennsylvania by age, gender, and geographical region. Regarding region, quotas were developed by totaling Pennsylvania's population by county and then determining the proportion of residents living in the counties represented by the region. Post hoc analyses revealed that the final sample was generally representative of the larger population at the time of data collection. Inclusionary criteria for participation in the survey included: (a) being at least 18 years of age, (b) currently residing in Pennsylvania, and (b) opting to participate in the web survey. If eligible, participants were directed to complete a self-reported survey through Qualtrics that took participants an average of 13 min to complete. Data were collected between June and July 2020. Participants who completed the survey received nominal compensation from the marketing research team ($1–$5). In total, 28,400 panelists were invited to participate, and 1,033 individuals completed the survey. The survey's participation rate was calculated using the American Association of Public Opinions Research's Response Rate 3 (RR3) formula which divides the number of completed surveys by the sum of surveys that were partially or fully completed, survey refusals, or noncontacts. The formula then adjusts to control for eligibility. Using this formula, the final participation rate was conservatively estimated at 4.8%, which likely underestimates the true participation rate.
Measures
NIMBY
The primary dependent measure used in this study referred to the expression of NIMBY syndrome for OUD treatment. To capture this construct, participants were asked to indicate their level of agreement with the following statement, “I would prefer that opioid treatment centers not be located near my home.” Response options followed a Likert scale ranging from 1 = “Disagree Strongly” to 5 = “Agree Strongly.” Participants were also given the option to select “Prefer not to say” or “Don’t Know/Unsure.” To further protect the validity of our results, these responses (n = 42) were excluded from analysis. Responses were then re-coded to create a dichotomous variable such that 1 = “Expressed NIMBY” (Responses 4–5) and 0 = “Did not Express NIMBY” (Responses 1–3).
Support for Punitive Treatment of OUD
The second dependent measure used in this study was support for punitive treatment of OUD. This variable was captured using responses to one survey statement, “There should be strong punishments for people who are addicted to opioids.” Response options followed a Likert scale ranging from 1 = “Disagree Strongly” to 5 = “Agree Strongly.” Participants were also given the option to select “Prefer not to say” or “Don’t Know/Unsure.” Again, these responses (n = 45) were treated as missing in analyses. Responses were then re-coded to create a dichotomous variable with 1 = “Support punitive treatment” (Responses 4–5) and 0 = “Did not indicate support for punitive treatment” (Responses 1–3).
Support for Employment Discrimination
The third dependent measure used in this study was support for employment discrimination for individuals prescribed MOUD. This variable was captured using responses to one survey statement, “Employers should be allowed to deny employment to a person taking medication to treat OUD.” Response options followed a Likert scale ranging from 1 = “Disagree Strongly” to 5 = “Agree Strongly.” Participants were also given the option to select “Prefer not to say” or “Don’t Know/Unsure.” Again, these responses (n = 74) were treated as missing in analyses. Responses were then re-coded to create a dichotomous variable with 1 = “Support employment discrimination” (Responses 4–5) and 0 = “Did not indicate support for employment discrimination” (Responses 1–3).
Stigma
The key mediating variable of interest in this study was opioid-related stigma. This variable was constructed using items modified from Kaynak et al. (2022), capturing components of dangerousness, blameworthiness, and fatalism. Specifically, the following seven items were used to measure opioid-related stigma: (a) “People who are addicted to opioids are just like anyone else” (reverse coded), (b) “Most people with opioid addiction will never get better and become productive people,” (c) “People addicted to opioids should be able to stop using them on their own,” (d) “People who are addicted to opioids are junkies,” (e) “Those who are addicted to opioids should not be given any responsibility,” (f) “People who have recovered from opioid addiction still can’t be trusted,” and (g) “Most people who are addicted to opioids don’t have the willpower to stop.” Response options followed a Likert scale ranging from 1 = “Disagree Strongly” to 5 = “Agree Strongly.” Participants were also given the option to select “Prefer not to say” or “Don’t Know/Unsure.” Again, these responses were treated as “missing cases” in the analysis. Responses were summed and averaged to create a scale measure of opioid-related stigma with higher numbers indicative of greater stigma. Factor analysis indicated that the items loaded onto one latent factor and reliability estimates suggested good internal consistency (α = .733).
Support for the “Disease Model” of Addiction
The main independent measure of inquiry in this study was support for the disease model of addiction. This variable, a measure of one's addiction framework, was conceptualized as a respondent's endorsement of opioid addiction being a medical problem (Murphy, 2017). To capture this variable, participants were asked to indicate their level of agreement with the following statement: “Opioid addiction is a medical illness like diabetes, arthritis, or heart disease.” Response options followed a Likert scale ranging from 1 = “Disagree Strongly” to 5 = “Agree Strongly.” Participants were also given the option to select “Prefer not to say” or “Don’t Know/Unsure” (omitted from the analysis, n = 46). Responses were then re-coded to create a dichotomous variable such that 1 = “Indicated support for the disease model of addiction” (Responses 4–5) and 0 = “Did not Indicate support for the disease model of addiction” (Responses 1–3).
Controls
Measures of gender (0 = “female,” 1 = “male”), political conservativism (0 = “not conservative,” 1 = “conservative”), race (0 = “non-White,” 1 = “White”), college degree (0 = “no degree,” 1 = “at least a 4-year degree”), age (18–94), annual household income (0 = “under $10,000” – 15 = “$150,000 or more”), personal substance use dependency (0 = “no,” 1 = “yes”), and having a friend or family member who is/was substance use dependent (0 = “no,” 1 = “yes”) were captured and included as control variables in analyses. 5
Analytic Strategy
All data were analyzed using SPSS Ver. 27. The data analysis proceeded in five key steps. First, data were appropriately inspected, cleaned, and coded. Second, preliminary analyses, consisting of calculating measures of central tendency and dispersion, as well as exploratory factor analyses (EFAs), were performed to assist with construct formation and model development. Third, bivariate analyses estimating correlation coefficients were run. Fourth, multiple Ordinary Least Squares (OLSs) and Logistic regression 6 were used to examine the correlates of our dependent measures at the multivariable level. First OLS regression was used to establish a relationship between support for the disease model of addiction and opioid-related stigma. Then, logistic regression was used to assess the relationship between our predictor variables and outcome measures. A multi-step approach was used for this part of the analysis. Specifically, part 1 of the logistic regression analysis involved regressing our outcome measures onto predictor variables excluding our measure of opioid-related stigma. Part 2 of the logistic regression analysis involved entering all of the variables into the models, including opioid-related stigma. Entering our key variables of interest into the models in a series of steps allowed for a cursory examination of the mediation effects of opioid-related stigma on the relationship between support for the disease model of addiction and outcome measures, as well as supported the use of more advanced analytical techniques to assess indirect effects. Once this cursory examination was completed, the fifth and final step in the analysis involved using the Hayes Process Package to provide a true test of mediation by examining the significance of the indirect hypothesized paths. The final models are reported below.
Results
Descriptive Statistics
Table 1 displays the sample demographic and descriptive information for all measures used in this study. As shown in Table 1, a slight majority of participants identified as female (52.3%). Most were White (85.5%) and not politically conservative (66.1%). Fewer than half of all participants had a college degree (43.8%). The mean age of the sample was approximately 48 years, and the average annual household income was reported as 6.18, representing between $60,000 and $80,000. Approximately 15% of participants indicated substance use dependency and nearly 60% indicated having a family member or close friend with substance use dependency. A slight majority of participants supported the disease model of addiction (61.9%), but nearly 42% of participants expressed NIMBY syndrome for OUD treatment. Approximately 13% of the sample indicated support for punitive treatment of OUD and nearly 20% expressed support for discriminatory employment practices against individuals who are prescribed MOUD.
Sample Descriptive Statistics.
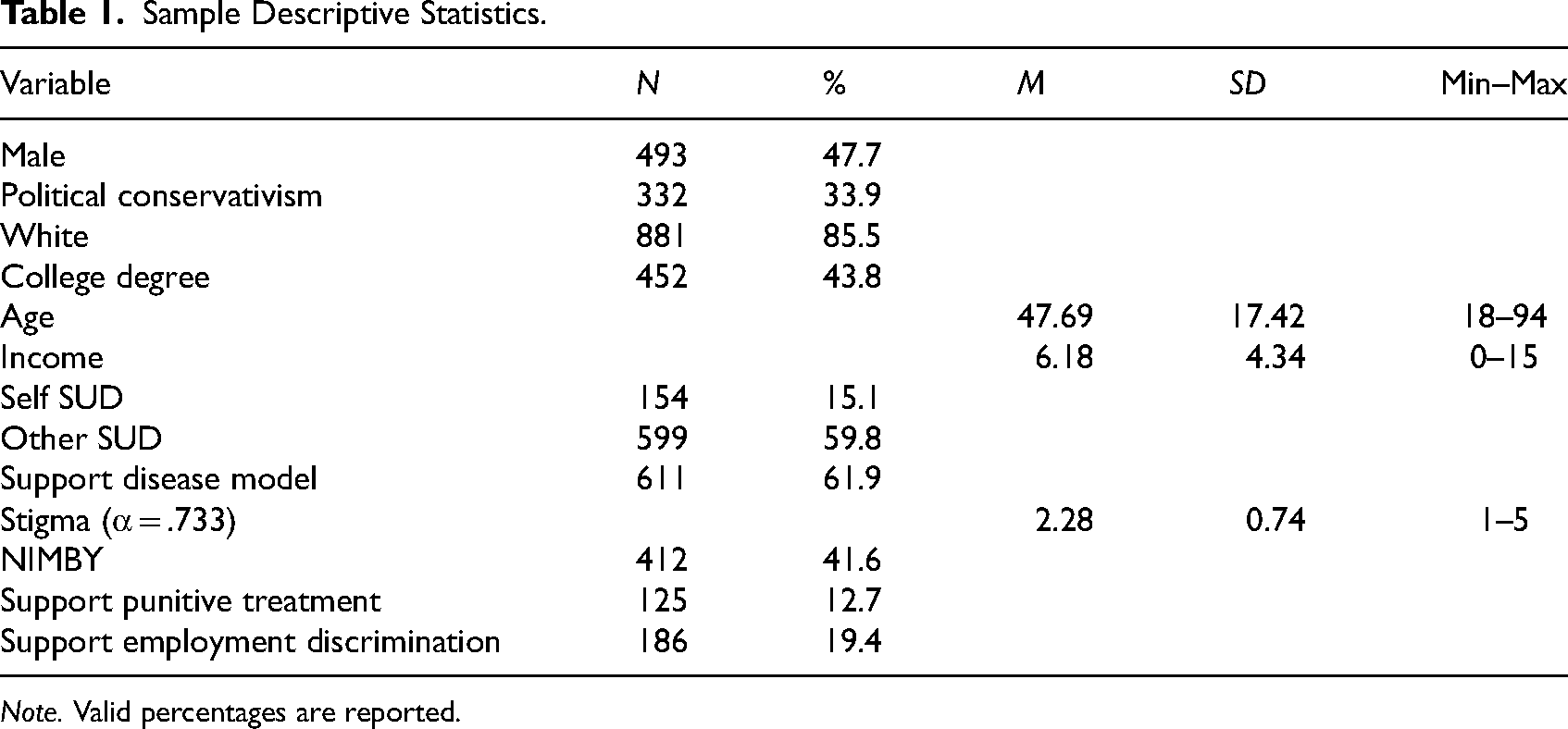
Note. Valid percentages are reported.
Opioid-Related Stigma
Table 2 shows results from the OLS regression analysis predicting opioid-related stigma. Overall, the model fit the data well and explained nearly 20% of the variance in the dependent measure (F = 22.672, p ≤ .001, R2 = .196). As hypothesized, support for the disease model of addiction (b = −.44, p ≤ .001) was found to be a significant negative predictor of opioid-related stigma. Other significant negative predictors of opioid-related stigma included indicating substance use dependency (b = −.23, p ≤ .001),having a family member or close friend who is/was substance use dependent (b = −.22, p ≤ .001), and age (b = −.00(4), p ≤ .05). Significant positive predictors included being male (b = .11, p ≤ .05) and politically conservative (b = .26, p ≤ .001).
Results from Regression Analyses Predicting Stigma.
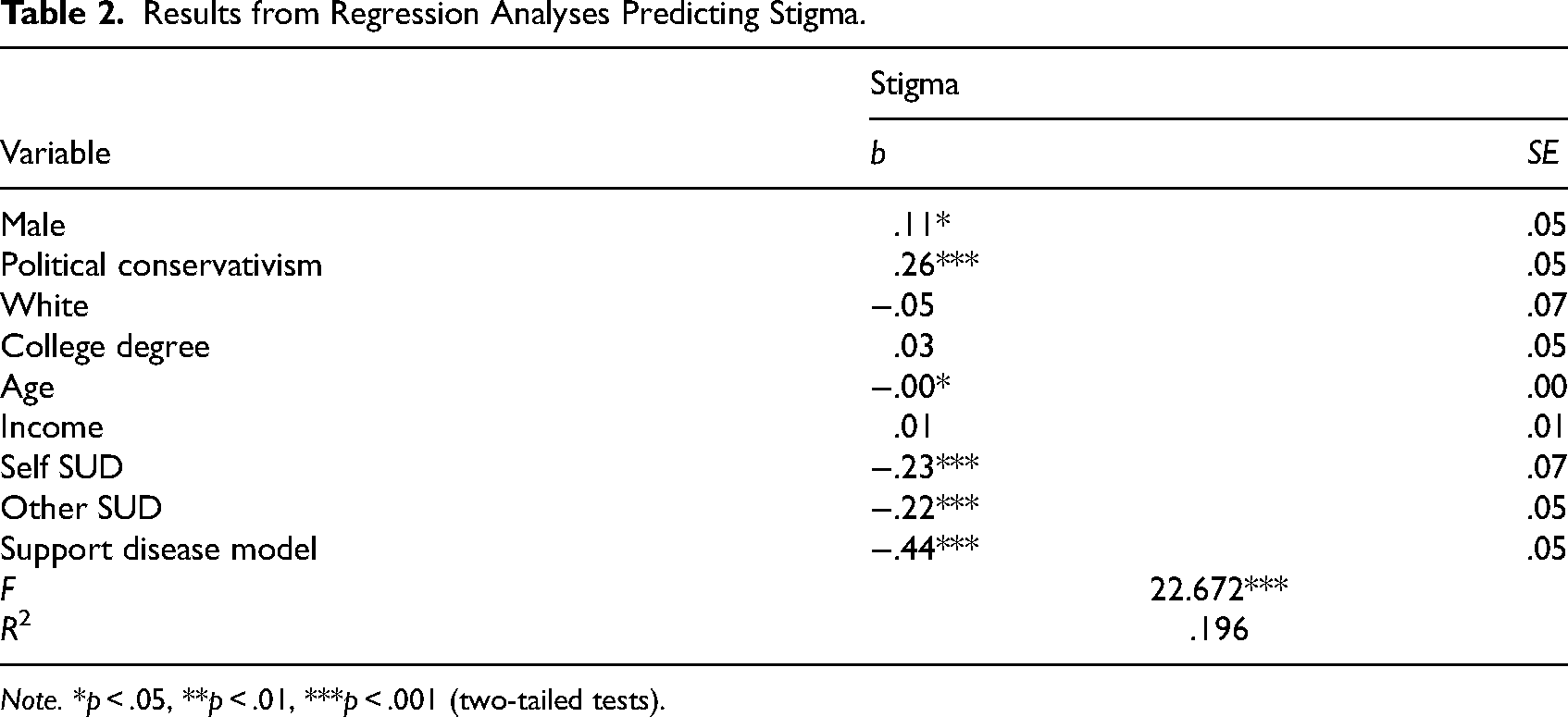
Note. *p < .05, **p < .01, ***p < .001 (two-tailed tests).
Support for NIMBY
Table 3 displays findings from logistic regression analyses estimating support for NIMBY syndrome, punitive treatment of individuals with OUD, and employment discrimination against individuals prescribed MOUD. The first group of rows in the table (Step 1) shows results from logistic regression analyses estimating support for outcome measures independent of opioid-related stigma. That is, all independent variables except for opioid-related stigma are included in the models. The bottom rows (Step 2) show findings from mediation analyses including opioid-related stigma.
Results from Regression Analyses Predicting Support for NIMBY, Punitive Treatment, and Employment Discrimination.
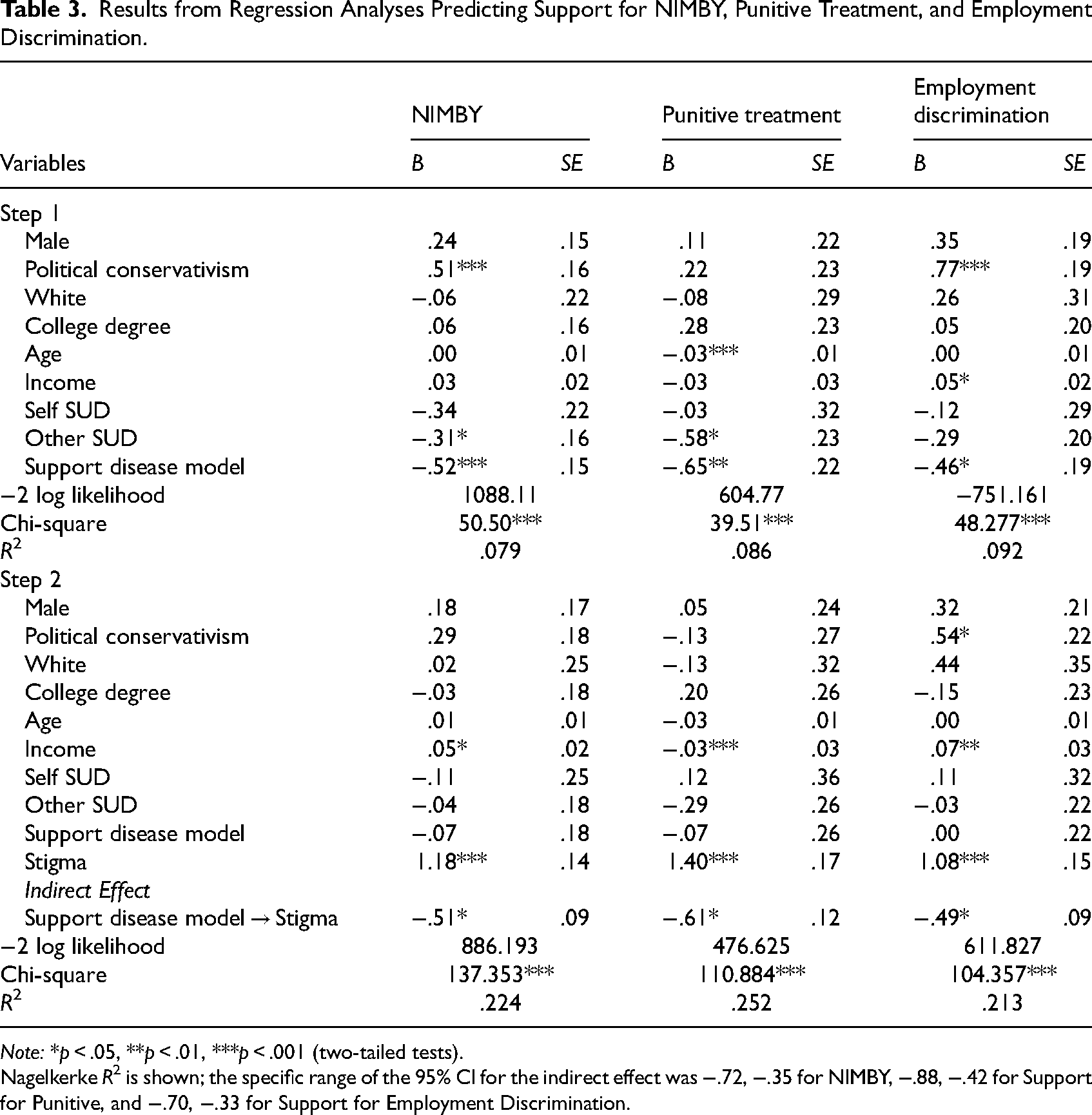
Note: *p < .05, **p < .01, ***p < .001 (two-tailed tests).
Nagelkerke R2 is shown; the specific range of the 95% CI for the indirect effect was −.72, −.35 for NIMBY, −.88, −.42 for Support for Punitive, and −.70, −.33 for Support for Employment Discrimination.
Regarding NIMBY, the model fits the data well in Step 1 of the analysis and explained approximately 8% of the variance in NIMBY syndrome (χ2= 50.50, p ≤ .001, R2 = .079). As hypothesized, support for the disease model of addiction (B = −.52, p ≤ .001) was found to be a significant negative predictor of expression of NIMBY syndrome. Having a friend or family member who is/was substance use dependent (B = −.31, p ≤ .05) was also found to be a significant negative predictor of NIMBY syndrome in that model, whereas political conservativism was found to be a significant positive predictor (B = .51, p ≤ .001). The model also fit the data well in Step 2 of the NIMBY analysis (χ2 = 137.353, p ≤ .001, R2 = .224). It is important to note that the inclusion of our stigma measures more than doubled the R2 from the first model. Significant direct predictors in the model included opioid-related stigma (B = 1.18, p ≤ .001) and income (B = .05, p ≤ .05). In support of our research hypothesis, the inclusion of opioid-related stigma in the model rendered the direct relationship between support for the disease model of addiction and NIMBY syndrome insignificant (B = −.07, p > .05); as hypothesized, a significant indirect effect between these two variables through opioid-related stigma was observed (B = −.51, p ≤ .05). Figure 1 provides a visual display of the mediation effects.
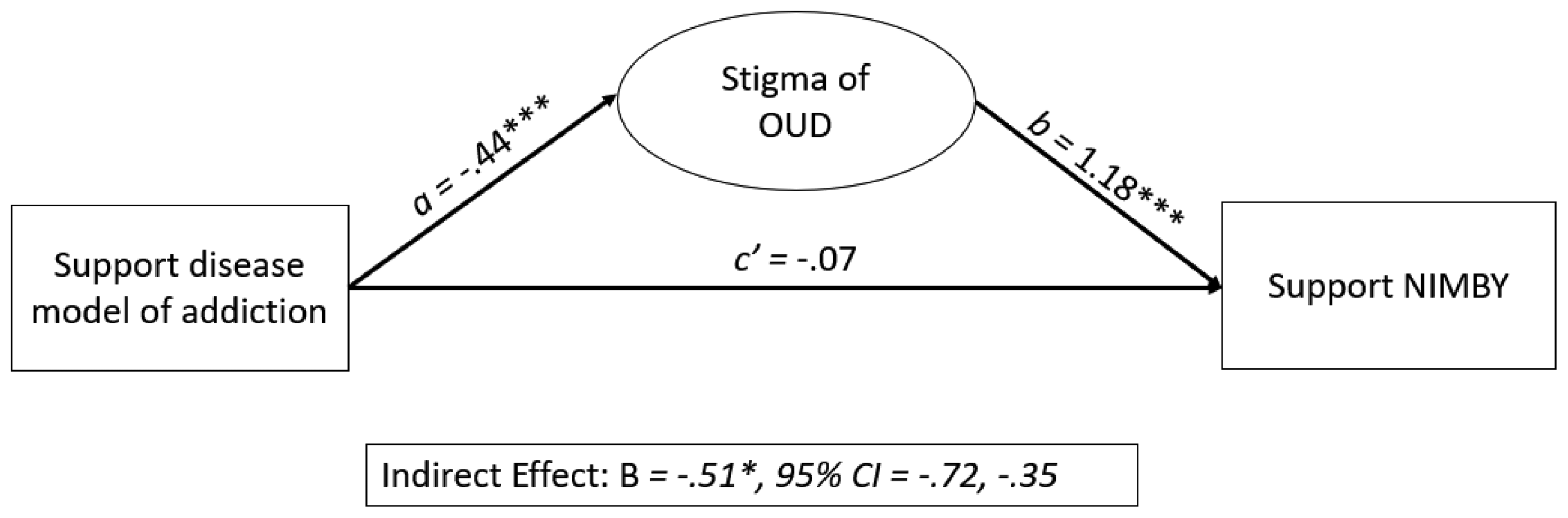
Visual display of mediation effects predicting expression of NIMBY for OUD treatment.
Support for Punitive Treatment of Individuals With OUD
The second group of columns in Table 3 shows results from the analyses predicting support for punitive treatment of individuals with OUD. The model fit the data well in Step 1 of this analysis and explained approximately 9% of the variance in support for punitive treatment of individuals with OUD (χ2= 39.51, p ≤ .001, R2 = .086). As hypothesized, support for the disease model of addiction (B = −.65, p ≤ .01) was found to be a significant negative predictor of support for punitive treatment of individuals with OUD. Having a friend or family member who is/was substance use dependent (B = −.58, p ≤ .05) and age (B = −.03, p ≤ .001) were also found to be significant and negative predictors in that model.
The model also fit the data well in Step 2 of the analysis (χ2 = 110.884, p ≤ .001, R2 = .252). Significant direct predictors in the model included opioid-related stigma (B = 1.40, p ≤ .001) and income (B = .03, p ≤ .001). Consistent with our hypothesis, the inclusion of opioid-related stigma in the model rendered the direct relationship between support for the disease model of addiction and support for punitive treatment of individuals with OUD insignificant (B = −.07, p > .05); as hypothesized, and consistent with the results from the NIMBY analysis, a significant indirect effect between these two variables through opioid-related stigma was observed (B = −.61, p ≤ .05). Figure 2 provides a visual display of the mediation effects.
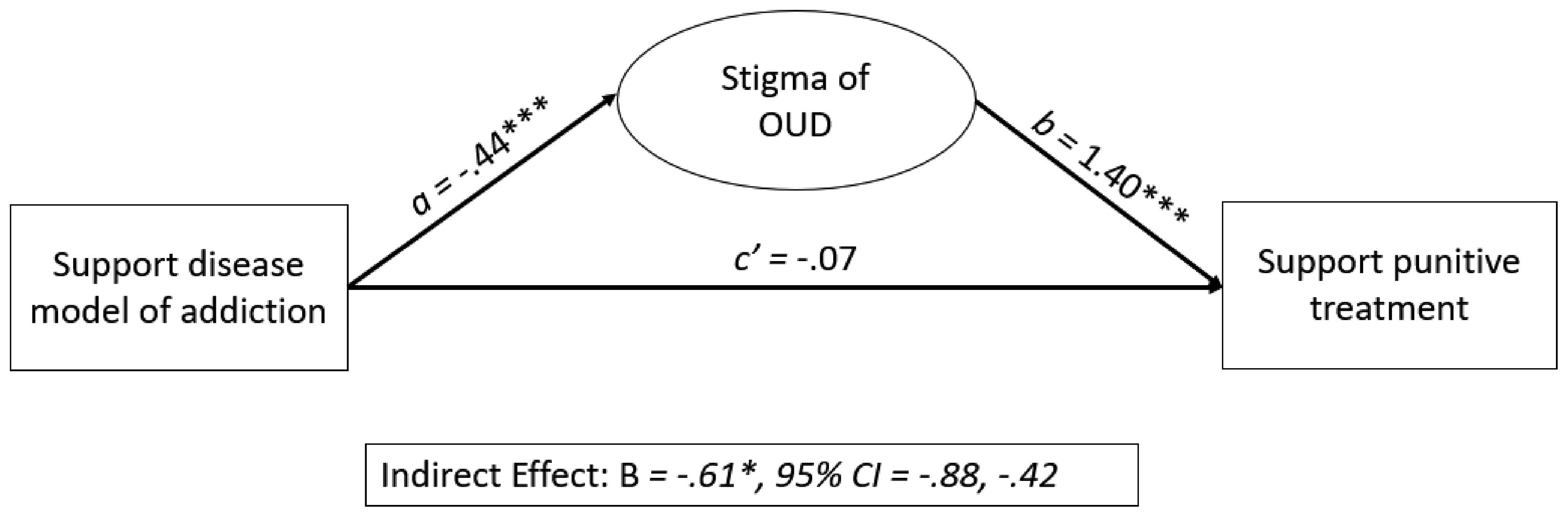
Visual display of mediation effects predicting support for punitive treatment of OUD.
Support for Employment Discrimination
The third group of columns in Table 3 show results from the analyses predicting support for employment discrimination against individuals who are prescribed MOUD. The model fit the data well in Step 1 of this analysis and explained approximately 9% of the variance of our outcome measure (χ2= 48.277, p ≤ .001, R2 = .092). Consistent with our other models, support for the disease model of addiction (B = −.46, p ≤ .05) was found to be a significant negative predictor of support for employment discrimination against individuals who are prescribed MOUD. Other significant predictors in that model were income (B = .05, p ≤ .05) and political conservativism (B = .77, p ≤ .001).
The model also fit the data well in Step 2 of the analysis (χ2 = 104.357, p ≤ .001, R2 = .213). Significant direct predictors in the model included opioid-related stigma (B = 1.08, p ≤ .001), income (B = .07, p ≤ .01), and political conservativism (B = .54, p ≤ .05). Consistent our other models, the inclusion of opioid-related stigma in the model rendered the direct relationship between support for the disease model of addiction and support for employment discrimination against individuals who are prescribed MOUD insignificant (B = .00, p > .05). However, as expected, and consistent with our other models, a significant indirect effect between these two variables through opioid-related stigma was observed (B = −.49, p ≤ .05). Figure 3 provides a visual display of the mediation effects.
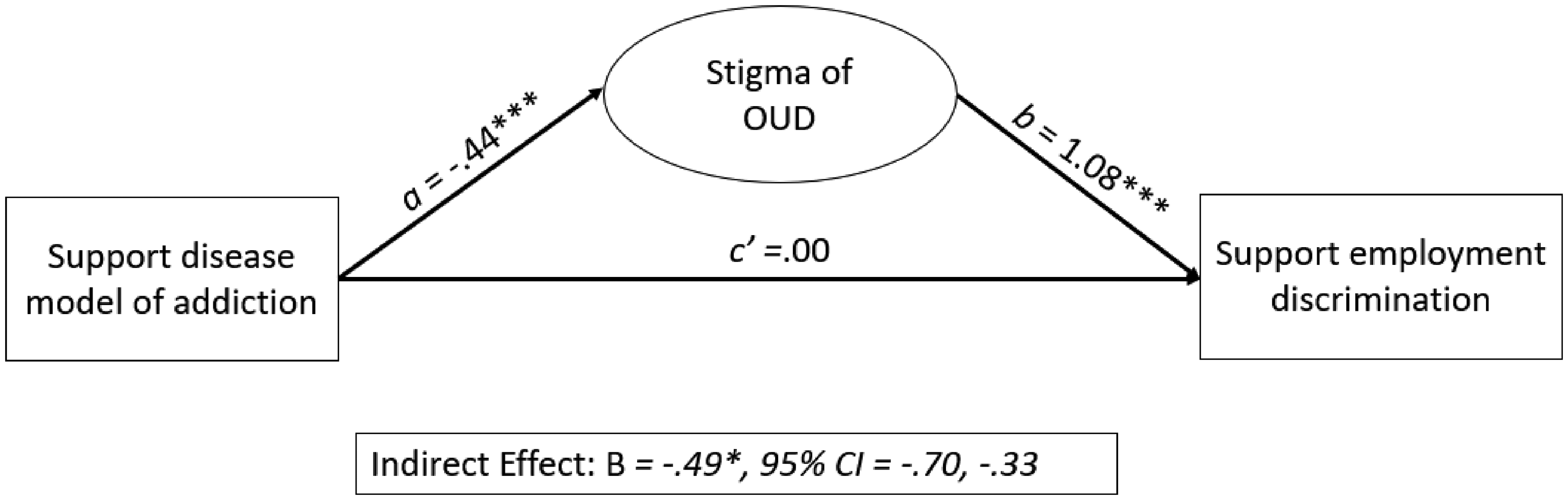
Visual display of mediation effects predicting support for employment discrimination against individuals prescribed MOUD.
Discussion
The goals of this study were to examine associations between addiction frameworks (i.e., support for a disease model of addiction), opioid-related social stigma, and policy-related attitudes (i.e., endorsing NIMBY syndrome for opioid-treatment centers, support for punitive treatment of OUD, support for employment discrimination against individuals prescribed MOUD), as well as to explore mechanisms underlying the relationship between addiction frameworks and policy-related attitudes. In support of our hypotheses, we found that support for the disease model of addiction was negatively associated with all of our policy-related outcome measures; however, the relationships observed in preliminary modeling were fully mediated by opioid-related social stigma, such that support for the disease model of addiction impacted endorsement of NIMBY syndrome, support for punitive treatment of individuals with OUD, and support for employment discrimination against individuals prescribed MOUD, indirectly through opioid-related stigma. Results show lack of support for the disease model of addiction can lead to elevated levels of opioid-related stigma that may have detrimental impacts on the availability and use of treatment and reintegration services for individuals with OUD. As such, these findings suggest that increases in support for the disease model of addiction may serve to reduce opioid-related stigma, and reduced opioid-related stigma may reduce support for NIMBY syndrome, support for punitive treatment of OUD, and support for employment discrimination against individuals prescribed MOUD—all of which are barriers to effectively responding to the opioid crisis.
Our findings are consistent with much of the previous literature and serve to clarify some of the mixed results examining the relationship between addiction frameworks and public policy. In previous studies, endorsement of a disease model of addiction has generally been positively associated with support for the expansion of drug treatment (Murphy, 2017; Murphy & Russell, 2021). Additionally, previous studies have identified positive associations between social stigma and policy attitudes; specifically, higher levels of social stigma were associated with more support for punitive policies and less support for public health policies (Adams et al., 2021; Cheetham et al., 2022; Kennedy-Hendricks et al., 2017). Our findings regarding the direct associations between addiction frameworks and policy attitudes, and between opioid-related stigma and policy attitudes, support these assertions. Collectively, our findings and those from previous works suggest that addiction frameworks and, more importantly, social stigma, may serve as significant barriers to public support for treatment, and subsequently, treatment access, effective treatment implementation, and successful reintegration for individuals with SUD.
These findings and others that highlight the association between support for a disease model of addiction and improved policy changes or attitudes (e.g., support for the expansion of drug treatment and harm reduction, reduced NIMBY attitudes; Cruz et al., 2007; Murphy, 2017; Murphy & Russell, 2021) identify addiction frameworks as one possible area to intervene to increase support for individuals with SUD. Helping the public to conceptualize SUD as a disease, rather than a moral failing, may help to garner public support for treatment services, especially treatment services like harm reduction due to the moralization of such services (Fry et al., 2005). However, others have previously questioned whether simply framing SUD as a treatable disease translates into actual support for policy (McGinty et al., 2015) and have suggested that such framings may have little (Meurk et al., 2014) to no effect on public policy (Trujols, 2015). Some scholars have even suggested that the addiction brain disease model can be harmful (Levy, 2013; Satel & Lilienfeld, 2022). For instance, Levy (2013) argued: “that accepting that addiction is not a brain disease does not entail a moralizing attitude toward people who suffer as a result of addiction; if anything, it allows for a more compassionate, and more effective, response to addiction.” Our findings refute this claim by empirically showing a direct relationship between endorsement of the disease model of addiction and opioid-related stigma; participants who supported the disease model of addiction were found to hold less stigmatizing attitudes toward persons who use opioids than those who did not support the disease model, and this stigma, in turn, influenced their perceptions of policy-related responses to opioid use, such that, comparatively, those who supported the disease model were less likely to support punitive treatment of people who use opioids, employment discrimination, and endorse NIMBY syndrome. Thus, participants who endorsed the disease model showed more compassion in modeling than those who did not. These findings suggest that addiction frameworks influence opioid-related stigma, and thus could be used as effective starting points in antistigma interventions; increasing public endorsement of the brain disease could help alleviate social stigma of SUDs more broadly.
The complex nature of changing policy attitudes highlights the need for comprehensive anti-stigma campaigns and educational interventions that target multiple aspects of social stigma. Specifically, campaigns should target both understanding of addiction as a disease and other aspects of social stigma, including dangerousness of individuals with SUD, blame for addiction, social distance from individuals with SUD, and fatalism about addiction and recovery. Such campaigns should address attitudes toward SUD from multiple perspectives and employ multifaceted strategies to encourage change (Tostes et al., 2020). One such campaign, Life Unites Us (Bonnevie et al., 2022) employs both education-based, contact-based, and advocacy-based strategies in a digital media campaign to reduce OUD stigma in Pennsylvania. Education-based strategies focus on increasing public knowledge about OUD and individuals with OUD while simultaneously correcting misinformation (National Academies of Sciences and Medicine, 2016). Contact-based strategies provide the public with direct contact with individuals with OUD (Livingston et al., 2012) and are employed in the form of videos of individuals in recovery from OUD sharing their stories. Lastly, advocacy-based strategies engage other stakeholders who are interested in engaging with the topic to enhance outcomes and reach (National Academies of Sciences and Medicine, 2016). For Life Unites Us, advocacy-based strategies include engaging community-based organizations that provide services to individuals with OUD, supporting community-based organizations in their work, and providing data on stigma to the public. These strategies allow for campaigns to address areas of stigma such as addiction frameworks, but also to address areas such as dangerousness, blame, social distance, and fatalism.
Such a multifaceted strategy for stigma reduction may prove particularly useful in reducing NIMBY syndrome and increasing general support for rehabilitative services for individuals with OUD. The NIMBY argument against locating addiction recovery services in residential neighborhoods may stem from many different resident concerns, including concerns for community safety and security, impacts on the quality of life, and decreased property values (Piat, 2000). These concerns often are due, at least in part, to misunderstandings about addiction, recovery, or specific addiction services; stigma about individuals with SUD, including that they are dangerous, and a fear that such services will actually bring in more individuals with SUD into the community (Smith, 2010). Such concerns often lead to attempts to either remove the service from the neighborhood or block its construction. Community opposition to addiction services can restrict the locations in which services are provided and decrease, or even restrict, access to the services (Strike et al., 2004). Approaches to reduce stigma that utilize education-based, contact-based, and advocacy-based strategies may be well-suited to address community concerns and change policy attitudes. Education-based strategies may be used to correct misunderstandings about addiction services and individuals in recovery; contact-based strategies may be used to decrease fears of individuals with SUD and combat stigmatizing attitudes about how individuals with SUD are dangerous; advocacy-based strategies may be used to engage community partners and other stakeholders in building support for bringing addiction services into communities. Given the role that social stigma plays in the relationship between addiction frameworks and policy attitudes, multifaceted attempts to change social stigma hold promise. For context, it is worth noting that there could be a potential for unintended negative consequences for some of the understudied interventions discussed above (i.e., multimedia/contact campaigns, etc.), although, to our knowledge, preliminary analyses have not found any yet and the LUU campaign has demonstrated positive effects in the community. As such, we suggest that these campaigns be extended to other states and efforts should be incorporated to evaluate their impact on reducing stigma and improving policy attitudes.
Limitations
While this study had many strengths, including the large sample size and the use of a representative sample, the findings should be considered in light of several limitations. First, the data used in this study were cross-sectional. As such, causal relationships between study variables cannot be inferred. Related, many of our variables were dichotomous in nature, and as such, we were unable to assess varying levels of support for policies. Future research should utilize longitudinal data, and employ multidimensional measures, to examine directional relationships between addiction frameworks, social stigma, and policy attitudes, as well as within-person changes in these constructs over time. Second, data were collected during June and July of 2020, at a time when many cities and states in the United States were implementing social distancing requirements and limiting nonessential activities due to the COVID-19 pandemic. This context in which data collection occurred may have influenced participant responses to stigma and policy items. Lastly, all participants were residents of a single state, Pennsylvania. As described previously, Pennsylvania has been particularly hard-hit by the opioid epidemic and has implemented various responses to address the issue across the state. Results may differ in other geographic regions. Research should be replicated with participants from other geographic areas. Moreover, regarding NIMBY syndrome, individuals may be supportive of the introduction of treatment facilities that provide MOUD, but express reservations about the location of such services. 7 Data limitations prevented us from examining this hypothesis directly. Future work should attempt to explore these nuances more closely. We encourage future researchers to examine this hypothesis and the nuance between NIMBY syndrome and elements of social stigma, including the desire for social distance.
Conclusion
In conclusion, these findings highlight the important role that stigma plays in informing individuals’ policy attitudes and highlight the potential of stigma reduction as an avenue for changing such attitudes. Our findings support the notion that recognition of addiction as a disease may decrease NIMBY attitudes and support for punitive treatment for individuals with OUD; however, the association between such addiction frameworks and policy attitudes was indirect, through social stigma. Efforts to change addiction frameworks to recognize addiction as a disease, as well as efforts to address other areas of social stigma directly, may help engender greater support for public health policy for individuals with SUD. More stigma reduction efforts, utilizing multifaceted strategies to reduce stigma, are needed.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.