
Abstract
Introduction
Workers with lived and living experience of alcohol and other drug (AOD) use have a long history of contributing to AOD treatment and support services. “Lived or living experience” in these contexts is operationalized as the personal experience of AOD use and engagement in recovery, treatment, and/or harm-reduction services. It may also relate to the experience of supporting a family member or friend who uses AOD (Victoria State Government Department of Health, 2021). A well-known example of individuals with lived experience supporting others in recovery is Alcoholics Anonymous, which has provided informal peer support via the use of sponsors since 1937 (Eddie et al., 2019). In Australia, workers with lived and living experience have been active in the AOD field for decades, in part facilitated by the adoption of a harm reduction approach to illicit drug use in the 1980s, and played a pivotal role in the response to the acquired immunodeficiency syndrome (AIDS) crisis (Crofts & Herkt, 1995; Drug Education Network Inc., 2020; Hallam, 2006).
The contribution of workers with lived experience to AOD treatment and harm reduction services is increasingly recognized. Research demonstrates the value of consumer participation in service provision in terms of improved health outcomes, clinical decision making, and service development (Bassuk et al., 2016; Brener et al., 2009; Rance & Treloar, 2015; Reif et al., 2014), and those with lived experience are accordingly being integrated into service delivery models with the development of paid employment roles in addition to volunteer positions (Byrne et al., 2021; Western Association for Mental Health, 2014). The inclusion of workers with lived experience is also evident in related fields such as mental health (Shalaby & Agyapong, 2020).
The lived experience workforce comprises two groups. “Peer workers” are those employed in identified peer roles for which lived/living experience is the primary requirement, and provide “peer support” to clients based on their mutual experiences. By contrast, other workers with lived/living experience can be employed in nondesignated roles (i.e., any role) and may or may not disclose their lived experience to others in the workplace (Chapman et al., 2020; Eddie et al., 2019; Greer et al., 2019). These workers may vary in the degree to which they consider their personal experiences with AOD use to be important or relevant to their work role.
To-date the majority of the published literature in the lived experience space has focused on peer workers. Peer workers can be found in a range of roles within the AOD workforce including treatment, prevention, and harm-reduction services such as needle/syringe exchange and opioid overdose programs (Bardwell et al., 2018; Chapman et al., 2020; Kennedy et al., 2019; Marshall et al., 2015). Research highlights the professional and personal rewards of peer work such as stability, job satisfaction, improved career prospects, confidence, personal growth, and the ability to give back (Gagne et al., 2018; Hymes, 2015). However, key challenges have also been identified, including role ambiguity and work/life conflict (Almeida et al., 2020), unclear job roles, low pay, and conflict between different treatment approaches (Gagne et al., 2018; Hymes, 2015). Some workers may also struggle to reconcile differences between their personal and professional ideologies. Experiences of stigma and discrimination are also common (Almeida et al., 2020; People with Lived Expertise of Drug Use National Working Group et al., 2021), a finding that is echoed in the mental health field (du Plessis et al., 2020).
However, while workers in identified peer roles are visible members of the lived experience workforce, those with lived experience who are working in nonidentified roles (i.e., any role) represent an important yet unseen cohort of workers. Very little research has explored workers with lived experience across all work roles in the AOD workforce (WA Peer Supporters’ Network, 2018). In one of few studies in Australia or internationally to do so, Chapman et al. (2020) found that 43% of a survey sample of AOD workers in the nongovernment sector reported lived experience. These workers were more likely to be older, male, identify as nonheterosexual, have lower salaries, abstain from alcohol but use opioids, and report workplace discrimination and less support outside of work. Of particular importance to how the lived experience workforce is conceptualized and quantified, Chapman et al. (2020) found that workers with lived experience were not necessarily designated to specific peer or consumer support positions, but rather were more widely dispersed across the workforce in many other roles. Indeed, only 18% of workers with lived experience were in a designated peer role or equivalent (Chapman et al., 2020). However, these results were limited to nongovernment workers within a single jurisdiction. The prevalence of workers with lived experience—and their personal and professional characteristics—within the national AOD workforce remains unknown.
Developing a greater understanding of the size and characteristics of the Australian AOD workforce with lived experience across all work roles should be considered a priority for a number of reasons. Mapping the lived experience workforce can make a valuable contribution to reducing the stigma associated with problematic alcohol or other drug use, as well as establishing these workers as a legitimate and important part of the AOD workforce. In addition, professional development and other workplace supports should ideally be tailored to the specific needs of particular workforce groups; however, these cannot be established nor efficiently provided without an understanding of the size and characteristics of the workforce in question. Similarly, while the value and contribution of workers with lived experience is now acknowledged, workforce planning and development decisions regarding how best to utilize these workers necessitate accurate and up-to-date workforce data. Finally, AOD work is widely recognized as having the potential to be both very rewarding and demanding, with a significant risk of burnout (Skinner & Roche, 2021). Yet little is known regarding the workplace factors that impact the wellbeing of workers with lived experience, and whether they differ between those with personal versus other types of lived experience and those without any lived experience. Recruitment, retention, and wellbeing initiatives specifically for workers with lived experience are therefore limited in scope and efficacy.
The aim of the current study is to explore the lived experience workforce within the national Australian AOD sector. Building on previous research (Chapman et al., 2020), this study is based on a broad conceptualization of the AOD lived experience workforce that includes (a) workers in any work role, including identified roles such as peer workers, and (b) primary (personal) and secondary(family) lived experience. Four aspects of the AOD lived experience workforce are examined:
The size of the AOD lived experience workforce, including the relative proportions of those with personal vs family/other lived experience. The demographic, social, and employment profile of the lived experience workforce. The extent to which personal and professional characteristics differ between those with personal vs other types of lived experience, and those with and without lived experience. The extent to which levels and predictors of wellbeing differ between those with personal vs other types of lived experience, and those with and without lived experience.
Method
Data Source
A custom-designed cross-sectional survey was conducted of the Australian AOD workforce in 2019. The survey instrument was developed in consultation with an expert advisory group comprising representatives from government and nongovernment organization (NGO) sectors, policy, research, and service provision. The survey comprised validated scales and items sourced from existing jurisdictional AOD workforce surveys (e.g., those conducted by the Network of Alcohol and other Drug Agencies, and Victorian Alcohol and Drug Association). Eligible participants for the current analyses were those who provided direct AOD client services in a specialist AOD service or a health/human services organization, including both NGO and government sectors.
The survey was disseminated through AOD-related publications, conferences, and social media. Industry stakeholders, peak representative bodies, and government agencies also promoted the study through their professional networks and communications (e.g., newsletters). Data were collected from August 2019 to February 2020 through the online survey platform Qualtrics. Ethical approval was obtained from Flinders University Social and Behavioural Research Ethics Committee, Southern Adelaide Clinical Human Research Ethics Committee (under the National Mutual Acceptance Scheme) and jurisdictional research ethics and governance bodies.
Measures
The full survey addressed: Demographics; employment and client characteristics; qualifications and professional development needs; working conditions; organizational characteristics; recruitment and retention; and health and wellbeing. The full survey protocol is available from the authors upon request. The variables included in the present study are detailed below.
Lived Experience
Participants were asked: “Do you identify as having lived experience in relation to alcohol or other drug issues?” and could select one or more of the following response options: (a) I do not identify as having lived experience, (b) personal experience of alcohol or drug problems (past or present), (c) family member who has experienced alcohol or drug problems (past or present), (d) other lived experience, or (e) prefer not to say.
Participants who indicated any type of lived experience were asked additional questions on disclosure and support. Participants were asked if they had disclosed their lived experience in the workplace (e.g., to supervisor or colleagues). For those who had chosen not to disclose, participants were asked to indicate the reason for nondisclosure (response options listed in Table 2). Participants were presented with a list of workplace supports for workers with lived experience and were asked to indicate the supports (a) which they could personally access if needed and (b) which would be most beneficial for workers with lived experience (response options listed in Table 2).
Social Demographics, Qualifications and Work Experience
Participants indicated their gender, age, sector of employment (government, NGO or private 1 ), highest general (non-AOD) tertiary qualification (undergraduate degree or higher) and highest AOD specialist qualification (vocational Certificate IV or higher). AOD experience was assessed with the question: “how many years have you been working in the AOD sector (less than 1 year; 1–3 years; 4–6 years; 7–9 years; 10 + years).
Burnout and Engagement
Burnout was assessed by a 6-item scale (Kristensen et al., 2005) comprising three items addressing burnout frequency (e.g., “How often do you feel worn out at the end of the working day”) (1 = never/almost never, 5 = always), and three items addressing burnout intensity (e.g., “To what degree is your work emotionally exhausting?”) (1 = to a very low degree, 5 = to a very high degree). Engagement was assessed by a 3-item scale (e.g., “I am immersed in my work”) (1 = never/almost never, 5 = always) (Schaufeli et al., 2019).
Job Quality
Five domains related to job quality were included in the current study: work intensity, job insecurity, respect/support, work meaning, and organizational openness to change. All job quality items were assessed on a 5-point agreement response scale (1 = strongly disagree; 5 = strongly agree).
Work intensity was measured by a 5-item scale (e.g., “I have constant time pressure due to a heavy workload”) (Siegrist et al., 2004). Perceived job insecurity was assessed by a 4-item scale (e.g., “I feel insecure about the future of my job”) (Vander Elst et al., 2014) (Cronbach's α = 0.88). Respect/support was measured by a 5-item scale (e.g., “I experience adequate support in difficult situations”) (Siegrist et al., 2004) (Cronbach's α = 0.84). Work meaning was assessed using a 3-item scale (e.g., “The work I do is meaningful to me”) (Spreitzer, 1995). Organizational openness to change was assessed by a 5-item scale (e.g., “You are encouraged to try new and different ideas”) (Lehman et al., 2002) (Cronbach's α = 0.80).
Statistical Analyses
All analyses were conducted in IBM SPSS Statistics 25.0 (IBM Corporation, 2017). Group differences (p ≤ .05) were explored on variables of interest via frequency statistics, χ2 tests of independence, multivariate analysis of variance (MANOVA) and linear regression.
Results
Sample and Descriptive Statistics
The sample comprised 986 AOD workers in direct client service roles such as counseling (25.2%), intake assessment (14.6%), and case management (10.6%). Only 2.4% (n = 24) of respondents were in a designated peer support or living/lived experience role.
Most respondents were women (70.9%), aged 35 + years (77.4%) and employed in the nongovernment sector (58.0%). The majority of respondents (69.3%) reported seven or more years’ AOD work experience (Table 1). While official demographic data on the Australian AOD workforce is not available, this profile is consistent with previous surveys of the AOD workforce (Duraisingam et al., 2020; McEntee et al., 2020).
Demographic Profile of Direct Client Service Workers with Lived Experience (LE).
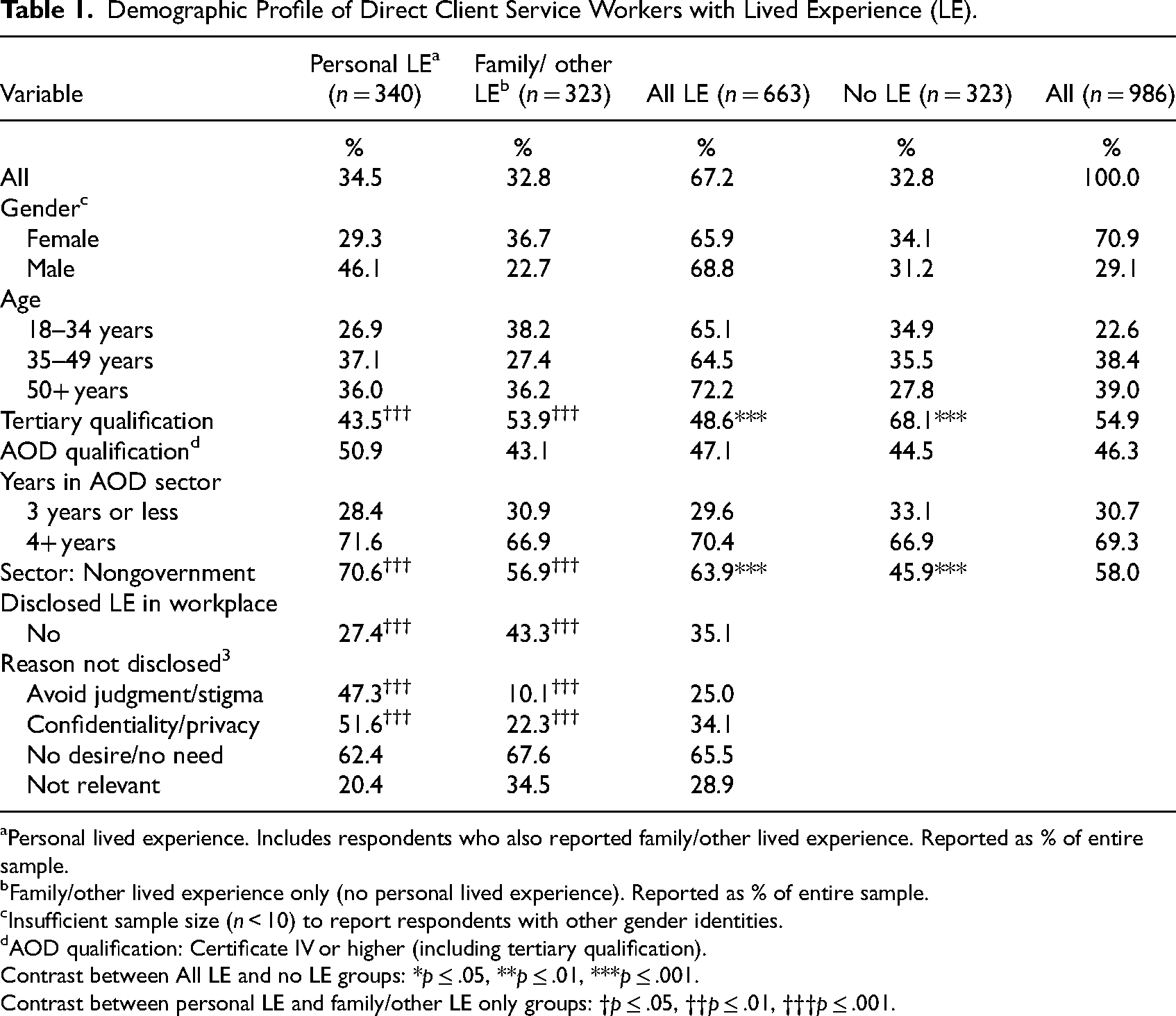
Personal lived experience. Includes respondents who also reported family/other lived experience. Reported as % of entire sample.
Family/other lived experience only (no personal lived experience). Reported as % of entire sample.
Insufficient sample size (n < 10) to report respondents with other gender identities.
AOD qualification: Certificate IV or higher (including tertiary qualification).
Contrast between All LE and no LE groups: *p ≤ .05, **p ≤ .01, ***p ≤ .001.
Contrast between personal LE and family/other LE only groups: †p ≤ .05, ††p ≤ .01, †††p ≤ .001.
Lived Experience
Overall, two-thirds (67.2%) of participants reported some type of lived experience with around one-third (34.5%) reporting personal lived experience and one-third (32.8%) reporting only family or other lived experience (no personal experience). Tertiary qualifications were significantly (p ≤ .001) more likely to be held by workers with family/other lived experience (compared to those with personal lived experience) and by workers with no lived experience (compared to those with any lived experience). Workers with personal lived experience were significantly more likely to be employed in the nongovernment sector (compared to those with family/other lived experience), as were workers with any lived experience (compared to those with no lived experience). No significant differences were found between groups in terms of gender, age, AOD qualifications held, or years of experience (Table 1).
Just over one-third (35.1%) of participants with lived experience indicated they had not disclosed this to their workplace; participants with family or other types of lived experience were significantly more likely to keep their lived experience confidential (i.e., undisclosed) than those with personal lived experience. Of those participants who had not disclosed their lived experience, those with personal lived experience were significantly more likely to cite concerns about judgment/stigma or confidentiality/privacy as the reason for their nondisclosure, compared to those with family or other lived experience (Table 1).
Wellbeing
Mean ratings of burnout did not differ significantly between workers with (M = 2.76, SD = 0.75) and without (M = 2.71, SD = 0.72) lived experience. Ratings of work engagement were also consistent between groups (M = 3.72, SD = 0.59, and M = 3.69, SD = 0.62, respectively). Similarly, workers with personal and other types of lived experience also reported comparable levels of burnout (M = 2.80, SD = 0.76 and M = 2.72, SD = 0.73, respectively) and engagement (M = 3.70, SD = 0.59 and M = 3.75, M = 0.60, respectively) (data not shown).
MANOVA analysis including all of the job quality, satisfaction and wellbeing measures indicated that workers with lived experience reported higher work meaning (M = 4.51, SD = 0.66 vs M = 4.36, SD = 0.71; F(1, 857) = 9.81, p ≤ .01) and higher job insecurity (M = 2.21, SD = 0.91 vs M = 2.05; SD = 0.80, F(1, 857) = 6.62, p ≤ .01) than those with no lived experience. Workers with personal lived experience also reported significantly higher perceived job insecurity (M = 2.31, SD = 0.96), compared to those with family or other types of lived experience (M = 2.10, SD = 0.84, F(1,589) = 7.63, p ≤ .01). No other significant differences were found between groups (data not shown).
Key workplace supports perceived to be the most beneficial for workers with lived experience included informal support (peers/colleagues) and regular debriefs with a colleague, which were able to be accessed by 86.3% and 68.3% of workers with lived experience, respectively. Support groups (29.5%), wellness/chillout rooms (19.3%), and external programs (32.6%) were the least accessible supports for workers with lived experience, however the majority of respondents reported that they would find these types of supports beneficial (58.6%, 60.7%, and 57.5%, respectively). Informal support groups and external programs were reported to be significantly (p < .001) more accessible among those with personal compared with other types of lived experience (Table 2).
Workplace Supports for Workers with Lived Experience (LE), %.
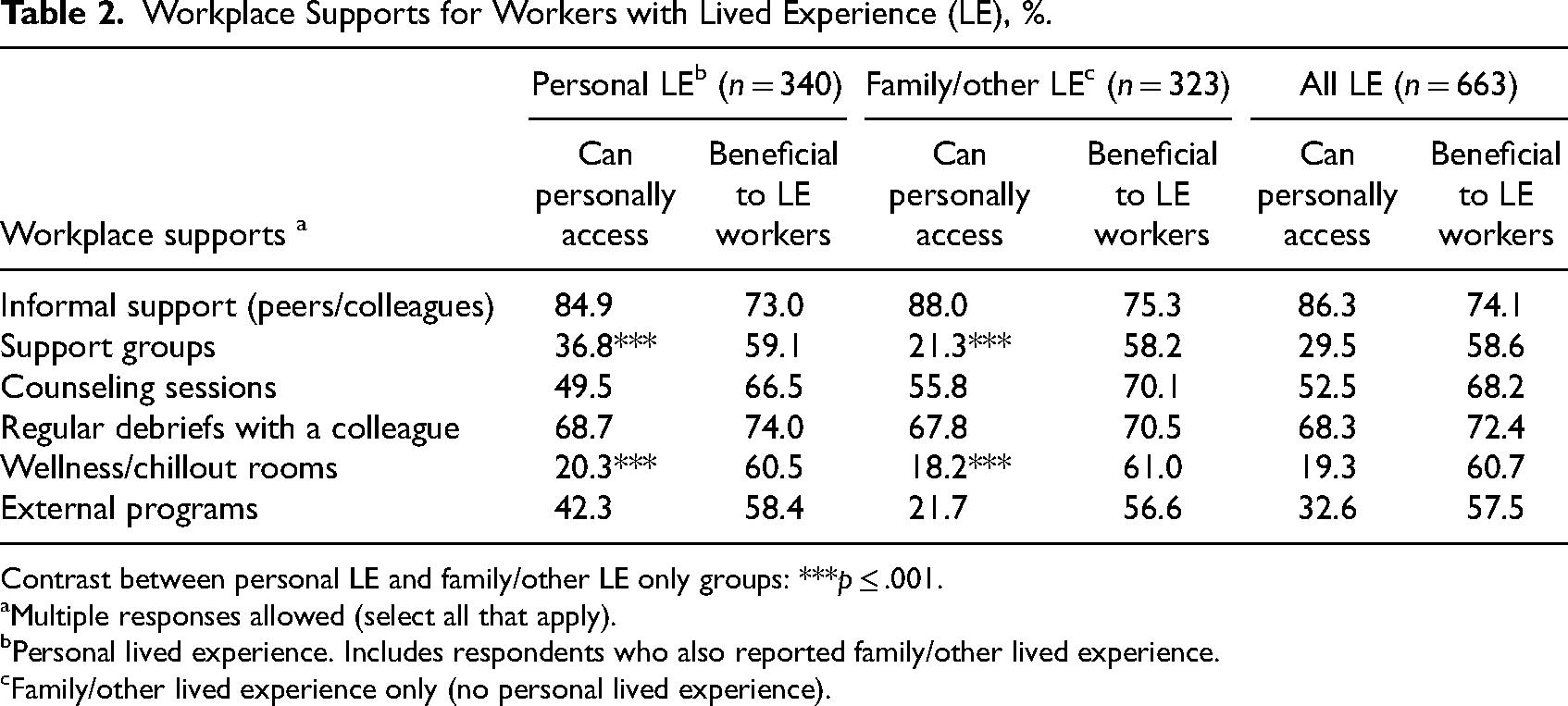
Contrast between personal LE and family/other LE only groups: ***p ≤ .001.
Multiple responses allowed (select all that apply).
Personal lived experience. Includes respondents who also reported family/other lived experience.
Family/other lived experience only (no personal lived experience).
Predictors of Burnout and Engagement
Burnout and engagement scores were moderately negatively correlated. As expected, burnout was negatively correlated with job resources (respect/support r = –.32; work meaning r = –.15; and organizational openness to change r = –.25), and positively correlated with job demands (work intensity r = .52 and job insecurity r = .20). Engagement was negatively correlated with job demands (work intensity r = –.15 and job insecurity r = –.23) and positively correlated with job resources (respect/support r = .38; work meaning r = .34; and organizational openness to change r = .31) (all p < .001; data not shown).
Predictors of burnout and engagement were examined separately for those with personal lived experience, those with family/other lived experience, and those with no lived experience. Among all three groups, burnout was more likely among younger workers and those who experienced high levels of work intensity. Lower levels of organizational openness to change additionally predicted burnout among those with personal and no lived experience, while lower levels of work meaning predicted burnout among workers with personal lived experience only (Table 3).
Predictors of Burnout.
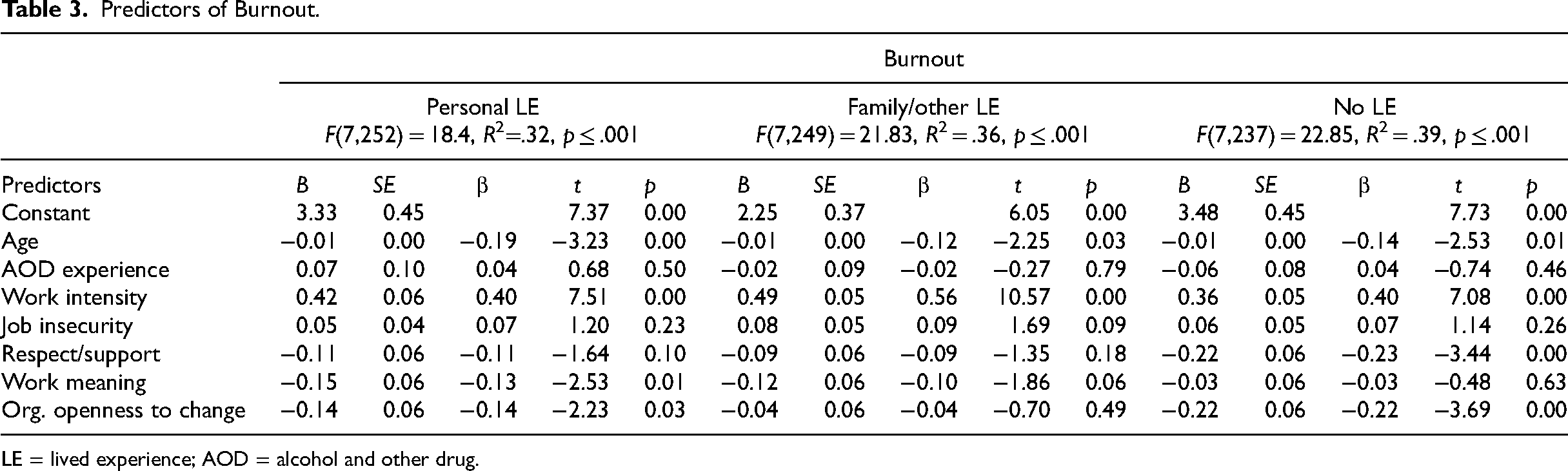
LE = lived experience; AOD = alcohol and other drug.
Work meaning predicted engagement levels among workers in all three groups. In addition, engagement was predicted by older age and work meaning for those with personal lived experience, lower levels of work intensity for those with family/other lived experience, and lower levels of job insecurity and organizational openness to change among those with no lived experience (Table 4).
Predictors of Engagement.
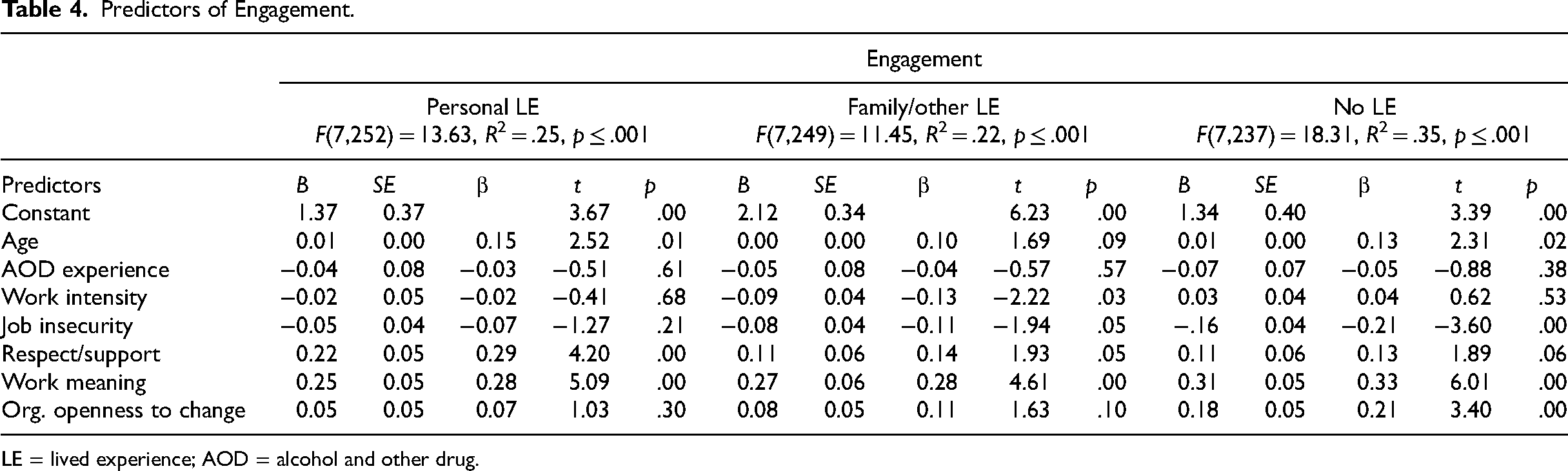
LE = lived experience; AOD = alcohol and other drug.
Discussion
The current study is the first to examine lived experience in the Australian AOD sector nationally across both the NGO and government workforces. Preliminary evidence has suggested a substantial proportion of Australian AOD workers identified as having lived experience in relation to drugs and alcohol (Chapman et al., 2020; Meumann & Allan, 2019; Roche & Skinner, 2021); the current research confirms and extends these results in a national context.
Our findings demonstrate that workers with lived experience tend to have fewer formal qualifications while also experiencing high levels of job insecurity; other research similarly highlights numerous challenges faced by this group (Chapman et al., 2020). Given these potential challenges, it is suggested that providing appropriate and accessible support (e.g., permanent contracts, access to professional development) to this group is a key priority for the AOD field. Recent years have seen increasing recognition of the value of peer workers within the AOD sector, and corresponding calls for enhanced workforce development initiatives and support for this workforce group (Intergovernmental Committee on Drugs, 2014; Lived Experience Workforce Strategies Stewardship Group, 2019; Victoria State Government, 2018). We now call for these supports to be extended beyond those in identified peer roles and provided to all workers with lived and living experience.
A number of workplace supports were identified by participants as potentially beneficial for the wellbeing of workers with lived experience; these may represent a good starting point for organizations seeking to do more to support this workforce group. In particular, the accessibility of support groups, wellness/chillout rooms, and external programs was found to be low—especially for those with family or other forms of lived experience—despite the majority of participants reporting that they would find these types of supports beneficial.
This study also highlights several key challenges that exist in the provision of workforce development support for workers with lived experience. Results indicated an extremely wide disparity between the number of workers with lived or living experience and the number of designated peer positions, with the latter being very small. Existing research suggests that the number of peer roles may be particularly low in Government services (van de Ven et al., 2022). Consequently, workforce planning and development initiatives which utilize the number of peer roles as a metric of the size of the lived experience workforce in Australia are likely to be inaccurate, and providing support only to workers in identified peer roles will exclude the vast majority of workers with lived experience.
Furthermore, a relatively large proportion of workers were found to have not disclosed their lived experiences. As such, the provision of workplace supports must be done in a way that protects anonymity and autonomy. It is clear that many participants in the current study, and particularly those with personal lived experience of AOD use, perceived there to be a substantial risk of judgment and discrimination if they revealed their background. This caution is not unfounded given the potential occupational health and safety and even criminal implications of disclosing illegal behaviors. It is therefore vital that workers are not required or pressured to disclose their lived experience in order to gain access to workplace support.
It is noteworthy that rates of nondisclosure were significantly higher among those with family/other types of lived experience, who were not themselves engaging in stigmatizing or illegal behaviors. Whether this is an artifact of secondary stigma (Corrigan et al., 2006), an effort to protect their loved ones’ privacy, or simply because disclosure was seen as irrelevant, may be an interesting avenue of future research.
Regardless, addressing the persistent stigma associated with AOD use is not only a moral imperative but will also facilitate the delivery of professional development activities. Recent initiatives to destigmatize mental health conditions may serve as models for the AOD field to emulate. However, some workers with lived experience will inevitably be hesitant to disclose even in the absence of perceived stigma, for a variety of reasons. This group must likewise be supported without compromising confidentiality. The most effective methods for providing support while protecting personal privacy and autonomy is an important subject for future research.
The present results provide some reassurance that workers with lived and living experience do not appear to be at increased risk of burnout, nor do they experience lower levels of work engagement, compared to their counterparts with no lived experience. Neither does there appear to be significant differences in wellbeing between workers with different types of lived experience. However, this does not necessarily imply that initiatives to address burnout and increase engagement are not required across the whole workforce. Previous research suggests AOD workers in general may be at high risk of poor wellbeing (Skinner & Roche, 2021); the current study may therefore provide some potential starting points for intervention. Specifically, age and work intensity predicted burnout among all three groups considered here; initiatives providing additional support for younger workers and ensuring reasonable caseloads are therefore likely to be effective across the entire workforce. Similarly, promoting opportunities to experience meaning from one's work is also likely to assist in building an engaged workforce.
Interestingly, several predictors of both burnout and engagement were different for those with personal versus other types of lived experience. Although these two groups did not differ significantly in their overall levels of wellbeing, these results suggest that they may be (de)motivated by different factors. Given that most demographic and work-related characteristics do not differ significantly between these two groups, the precise nature of these differences and why they occur warrants further examination. The few key differences found between those with personal and other forms of lived experience (i.e., rates of disclosure, qualifications, and sector of employment) may provide a starting point for future research seeking to explore this issue further. Alternatively, it is possible that the unique nature of the lived experience journey itself may predispose individuals to be engaged or burnt out by different factors.
Additional research conducted in collaboration with workers with lived experience will be imperative going forward, in order to understand the most effective strategies to promote worker wellbeing more fully. In particular, more in-depth exploration of the perspectives and priorities of those who have and those who have not disclosed their lived experience, and how (or if) these respective groups would prefer to be recognized and supported. This focused research could act to complement and inform broader discussions around what the peer and lived experience workforces should look like and how these workers can best be integrated within the broader AOD sector. In the meantime, comprehensive initiatives that target well-known workplace factors such as promoting openness to change and a respectful/supportive environment within the organization, as well as ensuring manageable caseloads and meaningful work, are likely to have benefits for most workers.
Limitations
There is currently no national data repository that provides an accurate record of the size of the AOD workforce in Australia; consequently it is not possible to estimate what proportion was captured in the current study, or the degree to which our sample is representative. Despite considerable promotional efforts, it is uncertain how many workers the current study reached, particularly among groups that may be overworked and suffering from burnout. Nevertheless, the present results represent one of the most recent sources of data available in Australia regarding the characteristics of the AOD workforce. However, it is acknowledged that the sample size is still relatively modest, and future research with larger samples is needed to explore the between-group differences identified here in more depth (e.g., sector of employment). This study also asked respondents specifically about their experience of problematic AOD use. This is a relatively narrow conceptualization of the concept of lived experience; if this definition was widened to include all forms and degrees of use, the population of workers with lived experience would be considerably bigger and potentially more diverse. Similarly, it is acknowledged that “lived experience” will mean different things to different people, and these nuances are unlikely to be captured using quantitative data as in the present study. Finally, it is possible that there may be key differences between the experiences and needs of workers with lived experience of alcohol vs other types of illicit drug use. Future research may wish to explore this issue with more disaggregated data than was available in the present study.
Conclusion
The size of the lived and living experience workforce in the Australian AOD sector is substantial and considerably larger than the number of designated peer roles would suggest. Workforce planning and development initiatives are required to safeguard the wellbeing of these workers, and ensure that they are supported to provide the best care to their clients. Such initiatives must be cognisant of the continuing stigma associated with lived experience in the AOD field and actively seek to combat it, while still protecting the privacy, anonymity, and autonomy of workers with lived experience.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval was obtained from Flinders University Social and Behavioural Research Ethics Committee, Southern Adelaide Clinical Human Research Ethics Committee (under the National Mutual Acceptance Scheme) and jurisdictional research ethics and governance bodies.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Australian Government Department of Health.