
Abstract
Substance use in pregnancy has been a prominent public health concern for the last several decades. Since the legalization of cannabis in Canada and across several American states, cannabis use during pregnancy has gained considerable public health, scientific, and media attention. This critical interpretive synthesis explores how the problem of cannabis use in pregnancy is constructed in the scientific literature and illuminates clinical, social, and political responses this construction engenders. The state of empirical evidence regarding the impact of perinatal cannabis use is fraught; a number of studies, of variable quality, have found no associations between cannabis use and adverse neonatal outcomes, while others have found cannabis to be associated with low birthweight and prematurity among other risks. Despite the inconsistent nature of the evidence base, the literature is underpinned by two important assumptions: prenatal cannabis exposure is an asocial phenomenon that can be disentangled from the social determinants of health, and cannabis exposure has detrimental effects on fetal and neonatal health. These assumptions shape indicators of signal and noise in the data by influencing the significance ascribed to particular findings, producing patterns of data interpretation that ultimately transform evidence of potential harms into certain risks and creates the mirage of a cohesive, unambiguous evidence base. We argue that the way that cannabis use in pregnancy is framed as a scientific and public health problem in the literature contributes to the stigmatization of pregnant people who use substances. We caution that failure to consider the interplay between environment, resources and other social determinants of health may ultimately cause undue harm to families and foreclose opportunities for investments that may promote health and well-being.
Introduction
Substance use in pregnancy has been a prominent public health concern for the last several decades (Roberts et al., 2017; Thomas et al., 2018). Since the legalization of cannabis in Canada and across several American states there has been a proliferation of scholarship on cannabis use during pregnancy (Corsi et al., 2019; Crume et al., 2018; Grant et al., 2018). At the heart of this dialogue are questions of risk, fetal safety, and responsibility. These conversations are not new; they reflect long-standing social, political, and scientific discourses on the use of substances—both legal and illicit—during pregnancy and the potential for adverse neonatal outcomes (Greaves & Poole, 2004; Lupton, 2012; Reid et al., 2008). Science that attempts to evaluate, often imperfectly, the relationships between substance exposure and neonatal outcomes has been particularly influential in the formulation of substance use in pregnancy as a public, legal and policy problem, and has had significant impact on the lives and well-being of pregnant people and their families (Stengel, 2014; Stone, 2015).
Contemporary research on cannabis and other forms of substance use in pregnancy are situated in the uneasy legacy of the crack cocaine moral panic and the devastation it wrought on marginalized communities. The publication of a single study by Chasnoff and colleagues (1985) in the New England Journal of Medicine is often cited as a major catalyst for the “crack babies” moral panic (Litt & McNeil, 1997; Terplan & Wright, 2011). This study described the outcomes of 23 neonates born to women who used cocaine, detailing a higher incidence of congenital anomalies, placental abruption, and poorer scores on the Brazelton Neonatal Behavioral Assessment Scale (Chasnoff et al., 1985). A cascade of scientific studies followed that seemed to confirm these observations by reporting a variety of catastrophic outcomes, fueling media outcry about a generation of irreparably damaged children (Ortiz & Briggs, 2003; Roberts, 1991). This moral panic wrought much more than the condemnation of pregnant people who use crack cocaine; it gave rise to a number of draconian policies and laws that targeted pregnant people who used substances, and restricted their capacity to parent their children (Beckett, 1995; Roberts, 1991). Much like contemporary punitive drug policies, rather than protecting or promoting fetal health, these measures ultimately created a strong incentive for the non-disclosure of substance use and the avoidance of both prenatal care and substance-use treatment (Beckett, 1995; Roberts, 1991). More than a decade after Chasnoff’s initial study, a series of meta-analysis and systematic reviews problematized the adverse outcomes described in the literature, ultimately finding no convincing evidence that perinatal cocaine exposure was associated with any negative outcomes that could not be explained by co-exposures to other substances (i.e., alcohol, tobacco, etc.) and the lived realities of urban poverty (Addis et al., 2001; Fares et al., 1997; Frank et al., 2001).
The crack cocaine panic serves as an important cautionary tale that reminds us that science is not a purely objective pursuit; the meaning that scientists, and their audience, draw from data is shaped by their values, perspectives, and beliefs. Substance use in pregnancy continues to be highly stigmatized; it violates a number of dominant discourses on gender, motherhood, citizenship, risk mitigation, and care (Nichols et al., 2021; Reid et al., 2008; Stone, 2015). The stigmatization of substance use in pregnancy has been intensified by the rise of reproductive citizenship, fetal rights, and the attendant responsibilities bestowed on pregnant people to protect fetal health above all else (Lupton, 1999, 2012; Salmon, 2011; Weir, 2006). These trends have resulted in increased public and scientific scrutiny of the bodies, consumption patterns, and everyday lifestyles of pregnant people and have contributed to the de-centering of pregnant people’s needs, liberty, and capacity to choose (Flavin & Paltrow, 2010; Paltrow & Flavin, 2013; Roberts et al., 2017). While punitive policies that punish pregnant people for their substance use by restricting their liberty or their ability to parent may reflect prevailing cultural beliefs, they are ultimately counterproductive; they encourage the avoidance of prenatal care, do not improve neonatal health outcomes, and increase healthcare costs for the state (Roberts & Pies, 2011; Subbaraman et al., 2018).
While pregnant people and their behaviors are highly scrutinized, the same cannot be said of non-gestational parents and social environments. There has been a notable lack of meaningful consideration of how health behaviors of the non-gestational parent and broader social environments and inequities may shape neonatal health outcomes (Richardson et al., 2014; Sharp et al., 2018, 2019). The disproportionate focus on the gestational environment and the overwhelmingly punitive nature of policy responses suggests that the restriction of pregnant peoples’ reproductive and bodily autonomy is the central aim of these cultural trends rather than the promotion of health and well-being of pregnant people and their offspring (Roberts et al., 2017; Thomas et al., 2018).
The fraught social and political context that fostered the crack cocaine panic endures, and concerns have been raised that this context may be shaping the emerging science around cannabis use in pregnancy (Dinsdale, 2019; Silverstein et al., 2019). Given our collective tendency to lose sight of how moral judgment and implicit biases come to bear on perinatal substance use research, we must critically examine how the problem of perinatal cannabis use is constructed in the scientific literature and draw attention to the clinical, social, and political responses this framing engenders. If we fail to critically examine the emerging trends in the literature, we risk willfully repeating past mistakes and producing new harms.
Methods
Critical interpretive synthesis (CIS) is an inductive review methodology that draws on techniques from qualitative inquiry to generate a coherent theory of the underlying assumptions that shape and contour a particular body of literature (Barnett-Page & Thomas, 2009; Dixon-Woods et al., 2006; McFerran et al., 2017). This review type is theory generating rather than aggregative: it does not attempt to provide a quality appraisal or synthesis of the findings that comprise the evidence base. The strength of this review type is that the literature itself is the central object of inquiry, which allows for a critical exploration of how knowledge is crafted and presented in a given field and draws attention to the broader implications of this mode of knowledge production. The purpose of this CIS is to explore how the problem of cannabis use in pregnancy is constructed in the scientific literature and how this construction shapes our thinking about pregnant people who use cannabis and their offspring. This study is guided by three research questions: How is cannabis use in pregnancy framed? How is evidence of harm framed and interpreted in the literature? What clinical and policy recommendations are made in the literature and how do these recommendations shape ongoing conversations about cannabis use in pregnancy?
Sampling and Analysis
CIS, unlike other review methodologies, does not follow a linear process and literature searching, sampling, data extraction, and synthesis do not proceed in discrete stages. Instead, a CIS approach is both iterative and recursive; each step of the review process unfolds alongside, and is informed by, one another (Dixon-Woods et al., 2006). To reflect the iterative nature of this process we report our sampling and analysis procedures together.
Like other forms of qualitative research, CIS is an interpretive method that is informed by the experiences and perspectives of the researchers who use it (Finlay, 2002). We recognize that our unique orientations toward the topic of substance use in pregnancy shaped the questions we asked and how we interpreted the data. RP is a sociologist, GH is a medical student, FGB is a pediatrician and clinical pharmacologist, and TT is an obstetrician and gynecologist. We all share an interest in women’s health and both FGB and TT provide clinical counseling for pregnant people who use substances. As the research process unfolded, we frequently reflected on how our interests and experiences influenced our analysis and the types of insights we brought to our discussions. The interdisciplinary nature of our team helped us to challenge the assumptions we each brought to the data and consider how the data upended those assumptions.
To assemble our preliminary sampling frame (Dixon-Woods et al., 2006), we searched PubMed using a combination of key word, title, and abstract screening and handsearching. The aim of our initial search was to sample papers that were topically diverse and maximally relevant to our research questions. Perinatal cannabis use literature is broad and diverse; it includes editorial commentary work, integrative and systematic reviews, original quantitative and qualitative research, case studies, policy documents and clinical guidelines. To allow for a wide breadth of coverage, we applied no limitations on methodology or paper type. To meet our inclusion criteria a paper had to be principally concerned with one of the following two objectives: 1) describing or quantifying the nature or scope of the problem of perinatal cannabis use; or 2) determining or describing the relationship between cannabis use in pregnancy and maternal or neonatal outcomes. We selected 10 full text papers for inclusion in the preliminary sampling frame.
Each member of the research team reviewed the full text for each of the 10 papers. To ensure that members of the research team approached the review, extraction, and critique of data in a systematic fashion we developed a basic data extraction tool. This tool consisted of a series of prompts related to our research questions (i.e., how is cannabis use in pregnancy framed in various elements of texts?). These prompts were intended to attune the reviewer to the research questions, to identify and map recurring concepts, and to develop an understanding of the relationship between the conceptual categories. While a data extraction tool is not a required component of CIS methodology, given our multiple reviewers and diverse disciplinary backgrounds, we found the tool helpful for approaching data systematically and for providing a basic structure for our analytic conversations.
Following the completion of the first round of sampling and analysis, we engaged in reflexive discussions (Finlay, 2002) about our interpretations of the data and identified emerging conceptual categories. As sampling in CIS is intimately entangled with theory-generation (Dixon-Woods et al., 2006), procedures for the subsequent rounds were informed by our emerging theoretical insights. Specifically, we purposefully sampled two types of papers: 1) studies that compared perinatal cannabis exposure to other legal or illicit substances; and 2) commentary pieces that engaged with features or trends in the literature. Papers in these categories were eligible for inclusion if they also met the original inclusion criteria. 13 additional full-text papers were selected for inclusion through multiple search techniques including hand searching, reference chaining and a database (PubMed) search.
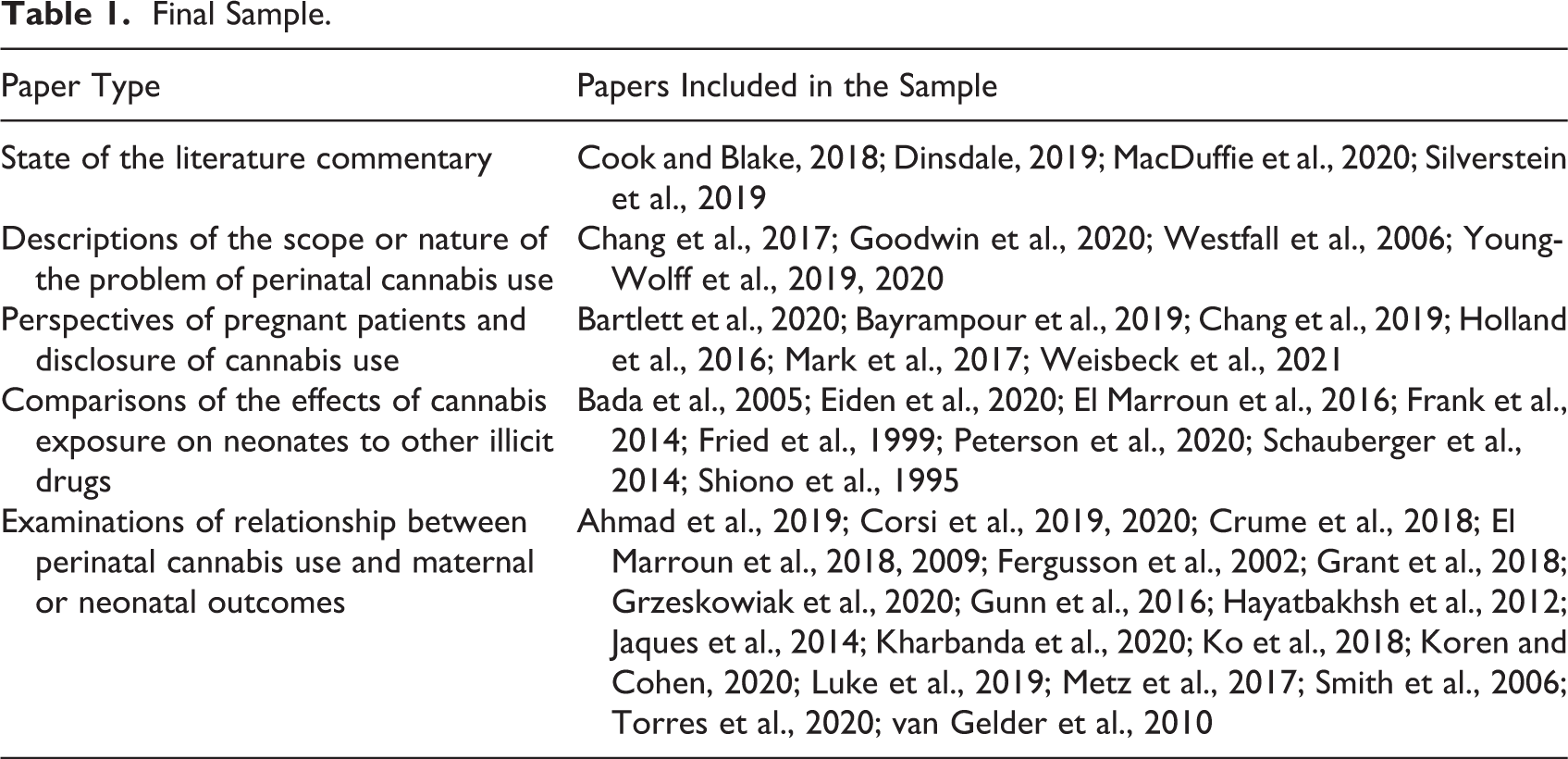
In the second round of data analysis, each paper was read by two members of the research team and analytic notes were recorded in the data extraction tool. We discussed each of the new papers in relation to the papers from the previous round with the aim of refining our understanding of the emerging conceptual categories and the relationships between them. These conversations informed our subsequent sampling. Consistent with a CIS approach, our emerging theoretical insights guided the sampling process and additional papers were selected for the purpose of elaborating, exploring, and testing the limits of our conceptual categories (Dixon-Woods et al., 2006). 20 papers were selected for inclusion in the final round, yielding a total sample of 44 papers. Each paper was read by two members of the research team. During this round, we met regularly to develop and refine a critical, synthesizing theory (Dixon-Woods et al., 2006) that accounted for the conceptual categories we identified and the relationships between them. To test the explanatory power of our theory, we continuously sought out discrepant cases in the data that challenged the boundaries of our concepts. We ceased sampling once our conceptual categories were determined to be rich, have sufficient depth and complex connections, and new data did not add further insight into their boundaries and properties (Morse, 1995). Our final sample is detailed in Table 1.
Final Sample.
Results
The state of the empirical evidence regarding the impact of perinatal cannabis use is fraught; a number of studies have found no associations between cannabis use and poorer neonatal outcomes (e.g., Ko et al., 2018; Metz et al., 2017), while others have found cannabis to be associated with low birthweight, prematurity, and other risks (e.g., Corsi et al., 2019; Crume et al., 2018). Despite the incomplete and often inconsistent state of the evidence base, this literature is underpinned by an important assumption: cannabis exposure has detrimental effects on fetal and neonatal health. This assumption shapes indicators of signal and noise in the data by influencing the significance ascribed to findings. This pattern of data interpretation ultimately transforms evidence of potential harm into certain risk and creates a mirage of a cohesive, unambiguous evidence base.
How Is Cannabis Use in Pregnancy Framed?
The literature on perinatal cannabis exposure is framed as a response to two often overlapping problems. In the first problem configuration, cannabis use in pregnancy is positioned as an urgent public health problem with implications for population health. In the second, cannabis use in pregnancy is positioned as an arena of scientific challenge, in which scientists must grapple with the limitations of observational study design and navigate various confounding factors to discern the “true” effects of cannabis exposure on offspring. Importantly, both problem formulations are linked by a shared assumption that in-utero cannabis exposure has deleterious effects on neonatal outcomes. This assumption shapes the way that the problem is described, the gaps in the literature that are identified and the recommendations that are made possible.
A Problem of Population Health
The literature frequently describes cannabis use as a large and growing problem fueled by decriminalization and legalization efforts across North America and the increasing social acceptability of the substance. In this context, interest in measuring the prevalence of cannabis use has proliferated. From 2002 through 2014, past-month use among pregnant women increased from 2.4 – 3.9%. With increasing use, there is an urgent need for high-quality data regarding the health effects of marijuana in pregnancy to appropriately educate women and health care providers. (Metz et al., 2017, p. 478)
A Perceived Problem of Measurement and Replication
The state of the science on in-utero cannabis exposure is consistently framed as disparate, and thus problematic. Within the literature, this disparity is positioned as a product of methodological limitations that plague research on substance use in pregnancy. As ethical and safety concerns prevent researchers from enrolling pregnant people in randomized control trials, a methodology that allows for direct comparison between treatment and control groups, researchers must rely solely on observational studies. Although the literature on the effects of maternal cannabis use during pregnancy has been steadily growing, it has a number of limitations which include: the use of relatively small samples; the failure to provide estimates of the extent of maternal cannabis use; lack of prospectively collected measures of cannabis use; and failure to control for factors that may potentially confound the association between cannabis use and pregnancy outcomes. (Fergusson et al., 2002, p. 22)
How Is Evidence of Harm Framed and Interpreted in the Literature?
We identified two distinct, but often intersecting, patterns in how evidence of harm was framed in the literature. In the first pattern, neonatal outcomes are foregrounded as the primary locus of concern. In the second pattern, perinatal cannabis exposure is constructed as an asocial phenomenon that can be disentangled from the social determinants of health, social inequities (i.e., the effects of sexism and racism), and other social behaviors that may affect pregnancy outcomes (i.e., alcohol and tobacco consumption).
Framing Evidence of Harm
The potential harms of cannabis exposure for neonatal health are the focus of this literature; there is a striking lack of attention paid to the potential harms or benefits of cannabis use for pregnant people. This is remarkable given that the literature emphasizes that people who use cannabis during pregnancy tend to have several sociodemographic characteristics and risk factors associated with poorer maternal health outcomes including high rates of depression, anxiety, and stress (Ahmad et al., 2019; Goodwin et al., 2020; Luke et al., 2019; Young-Wolff et al., 2020), food insecurity (Crume et al., 2018), a history of domestic violence or trauma (Ko et al., 2018; Young-Wolff et al., 2020), higher rates of alcohol and tobacco use in pregnancy, polysubstance abuse (Eiden et al., 2020; Luke et al., 2019; Peterson et al., 2020), and inadequate or sporadic prenatal care (Bada et al., 2005; Corsi et al., 2019, 2020). Despite the prevalence of these risk factors, cannabis use in pregnancy is implicitly framed as a phenomenon whose effects can be disentangled from the numerous risks factors that differentiate pregnant people who use cannabis from the general population by using appropriate statistical methods. In this way, the effects of cannabis exposure are framed as asocial and dislocated from the social determinants of health. The possibility that the social characteristics and risk factors of pregnant patients may shape neonatal outcomes is consistently de-emphasized or absent altogether. For example, one study (Bada et al., 2005) found that being African American resulted in higher odds ratios for prematurity, intrauterine growth restriction (IUGR), and low birth weight (LBW) than cannabis, opiate, and tobacco use during pregnancy. These findings were discussed only briefly and without acknowledging how systemic racism negatively impacts health and well-being.
Interpreting Evidence of Harm
Methodological rigor was a central focus across the literature, particularly with respect to confounding factors and co-exposure to other substances such as alcohol and tobacco that may have similar effects on neonatal outcomes. Many researchers attempted to account for these confounders using various statistical approaches. Their efforts were deemed rigorous only when statistically significant associations between perinatal cannabis exposure and adverse neonatal outcomes were found. Our data are inconsistent with findings of studies that have not found a significant association between cannabis use in pregnancy and birth outcomes. The existing discrepancy between the findings might be due to the difference in the level of adjustment for confounders…our study suggests a significant effect of in-utero exposure to cannabis on birth outcomes examined independent of sociodemographic background and use of other substances. (Hayatbakhsh et al., 2012, p. 217) Robust evidence that continued cannabis use during pregnancy is associated, independent of continued cigarette smoking, with significant reduction in infant gestational age at birth, birth weight and length, and head circumference, as well as increased frequency of severe neonatal morbidity. (Grzekowiak et al., 2020, p. 522)
The consequence of interpreting statistically significant results as evidence of rigor is that studies that yield no statistically significant associations or statistically significant protective associations are interpreted as evidence of flawed design. For example, one study that found no significant associations between prenatal cannabis use and adverse neonatal outcomes concluded their discussion by stating: Further research is needed to determine the true association between illicit drug use and perinatal outcome…it remains uncertain whether prenatal cannabis exposure as well as exposure to other illicit drugs affects the occurrence of birth defects and developmental problems later in life. (van Gelder et al., 2010, p. 245)
A small number of studies in the sample found that cannabis use in pregnancy was associated with a reduction in risk for gestational diabetes and pre-eclampsia. In one such study, the authors acknowledge that their findings “merit consideration,” but dismissed the statistically significant 0.5% reduction in the incidence of gestational diabetes and pre-eclampsia as “modest” and “not clinically important” (Corsi et al., 2019, p. 151). In other studies, protective associations were dismissed as a product of lingering confounding variables and thus clinically insignificant (i.e., Luke et al., 2019). Notably, no studies included in the sample dismissed any associations of prenatal cannabis exposure with poorer neonatal outcomes, even in cases where populations were strikingly dissimilar to the general population.
In addition to shaping the interpretive threshold for generalizability and rigor, the assumption that cannabis is deleterious for neonatal health also informs how evidence of harm is interpreted and reported. Across the literature, we found that statistically significance differences were interpreted as evidence of clear harm, regardless of clinical significance. For example, El Marroun and colleagues in their 2016 study found that children who were exposed to cannabis in-utero had thicker frontal cortices than unexposed children. This difference was determined to be statistically significant, but no further investigation was conducted by the study team to determine if the observed differences in brain structure had any functional implications. Despite this, the authors concluded that cannabis should be avoided during pregnancy due to the documented “long-term consequences” of exposure (p. 977).
In some cases, the conclusions drawn from the evidence extended beyond the actual data and were more speculative than scientific. One team (Peterson et al., 2020) conducted an MRI imaging study that compared the brain structures of children exposed in utero to three substances (cannabis, opioids, and cocaine) to non-exposed children. They reported statistically significant differences in the brain tissue patterns of children exposed to cannabis. However, none of the 11 neurodevelopmental clinical outcomes assessed at 12 months of age differed significantly in the children exposed to cannabis. The lack of statistical significance was included in the supplemental materials but absent from the results and discussion. Despite this, the researchers concluded that children exposed prenatally to cannabis may exhibit poorer outcomes at 12 months. This conclusion appears to be based on the subtle differences in brain tissue patterns alone and dislocated from any evidence that these differences affect neurodevelopmental outcomes in a deleterious manner. The possibility that these differences in anatomical structure may be protective or even advantageous is absent entirely.
What Clinical and Policy Recommendations Are Made in the Literature?
We identified four broad, overlapping clinical and policy recommendations across the sampled literature: unequivocal clinical counseling about the risks associated with cannabis use in pregnancy and the promotion of abstinence (e.g., El Marroun et al., 2009; Fried et al., 1999; Luke et al., 2019; Smith et al., 2006); increased drug screening and surveillance of pregnant people (e.g., Ahmad et al., 2019; Goodwin et al., 2020; Ko et al., 2018; Mark et al., 2017); additional research on long-term impacts (e.g., Corsi et al., 2020; Grzeskowiak et al., 2020; Kharbanda et al., 2020; Ko et al., 2018); and occasionally, public health interventions for pregnant people who use cannabis (e.g., Bada et al., 2005; Shiono et al., 1995; Young-Wolff et al., 2020). Taken together, these recommendations obscure the discrepant nature of the evidence and create the impression of a cohesive knowledge base that provides clear evidence of harm. Importantly, the clinical and policy recommendations present the harms of perinatal cannabis use in general terms and do not describe the impact of that harm for the health, development, and well-being of offspring in any meaningful way.
Calls for clinical counseling were highly prevalent in the sample. These recommendations were broad and encouraged health care providers to advise all pregnant patients to abstain from cannabis, and to refrain from prescribing medical cannabis under any circumstances to female patients of reproductive age. Notably, no recommendations targeted male patients. Recommendations for targeted counseling of pregnant patients identified as being “at – risk” of cannabis use due to age, socio-economic status, or other risk factors (i.e., tobacco or alcohol use) were also frequently included. Importantly, these recommendations were focused solely on abstinence and did not prompt clinicians to inquire about patients’ social determinants of health or needs for social supports. These recommendations are underpinned by the assumption that once pregnant people are informed, they will cease to use cannabis. Our participants emphasized their desire for healthy pregnancies and children and suggested that learning more about potential health and developmental risks would compel them to quit. Future health communication thus needs to make use of this motivation. (Chang et al., 2019, p. 11)
Recommendations for frequent, definitive counseling messaging were often augmented by general statements about the risks associated with cannabis use in pregnancy. As illustrated in the previous section, the conclusions and recommendations offered by researchers were often informed by statistical significance alone; discussion of the magnitude of the purported effects, their clinical significance, or practical implications for offspring were absent. However, statistically significant differences in mean or standard deviation alone do not provide enough relevant information for clinicians, public health policy makers, or individuals to determine whether the observed difference will have a meaningful, detrimental effect on neonatal and maternal outcomes. Further, the way that the statistically significant measures are reported are often dislocated from population data or specific clinically relevant measures like small for gestational age, creating space for multiple interpretations.
While a number of studies included in the sample encouraged health care providers to educate patients on the potential harms of cannabis use in pregnancy, the absence of clinical significance makes it challenging to describe the nature of potential risks. The ambiguous nature of these risks hinders the ability of patients and clinicians to engage in informed decision-making around cannabis use, particularly if the patient perceives their cannabis use to be beneficial. Further, the absence of clinical significance in the conclusions and recommendations are lacking in three important ways: (1) meaningful, unbiased, future directions for research, (2) useful, actionable guidance for public health and public policy, and (3) digestible, practical information for clinicians to use while counseling patients about the risk-benefit balance of cannabis exposure. Instead, the conclusions offered in the literature primarily function to uncritically uphold the assumptions that underpin this field of research: in-utero cannabis exposure, to the exclusion of social determinants of health, has deleterious effects on neonatal outcomes.
Discussion
Substance use in pregnancy is highly stigmatized; pregnant people who struggle with substance use are subject to blame, widespread judgment and unsympathetic attitudes (Greaves & Poole, 2004; Reid et al., 2008). Scientists, despite their commitment to objectivity, are not immune to culture; they bring their beliefs, values, and perspectives to their interpretation of data. This finding is not new: the influence of socio-cultural discourses has long been documented in science that grapples with the thorny issue of substance use in pregnancy (Frank et al., 2001; Terplan et al., 2015; Terplan & Wright, 2011). Previous work has shown that substances associated with similar neonatal outcomes– such as tobacco and cannabis—have discrepant interpretations; illegal substances are interpreted as being more dangerous and policy recommendations are more severe (Frank et al., 2001; Konijnenberg, 2015). Despite the aims of objectivity, it may not be possible to remove the influence of sociocultural discourses on substance use in pregnancy from research that seeks to understand the relationship between substances and neonatal outcomes. Given this, it may be useful for scientists to adopt a reflexive stance throughout the research process and explicitly reflect on how their perspectives may shape their methodological choices and interpretation of data.
The framing of perinatal cannabis use as an asocial problem contributes to the stigmatization of pregnant people who use substances by positioning substance use as an individual choice and cessation as a matter of willpower. There is ample evidence that clinical counseling approaches that conceive of substance cessation as a simple matter of knowledge and choice are ineffective (Martin, 2016; Stone, 2015). Instead, these approaches create a number of unintended consequences that hinder efforts to promote substance reduction or cessation—including the avoidance of prenatal health care (Greaves & Poole, 2004; Salmon, 2011; Stone, 2015; Wigginton & Lee, 2013). People who use substances while pregnant experience cessation-based counseling as paternalistic and stigmatizing, and report that it encourages them to conceal their substance use from health care practitioners, and in some cases, steels their resolve to continue the behavior (Greaves & Poole, 2004; Wigginton & Lee, 2013). Thus, the counseling recommendations advocated for in the cannabis literature at best may be ineffective and at worst, counterproductive.
The striking absence of concern for the well-being of pregnant people within the perinatal cannabis literature raises critical questions about why certain substances, like cannabis, become a popular focus of scientific inquiry, while other, modifiable sociodemographic lifestyle factors that are known to pose harm to the health of the pregnant person do not. Existing data suggest that pregnant people who use cannabis have a number of risk factors—including stress, poor nutrition, poverty and poor mental health—that may negatively impact their heath and may account for the poor outcomes observed in infants exposed to substances like cocaine, opioids and cannabis (Bauer et al., 2002; Frank et al., 2001; Schempf & Strobino, 2008). Thus, as we continue to develop public health messaging and polices about cannabis use in pregnancy, it is vital that we center and seek to account for the lived experiences of people who use cannabis during pregnancy by addressing their needs and resource constraints in a meaningful way.
Critical scholars have argued that substance use in pregnancy must be examined in the social and economic context in which it occurs as it is inextricable from overlapping factors, including trauma, gender-based violence and inadequate nutrition and housing that contour the conditions of people’s lives (Martin, 2016; Salmon, 2011; Wigginton & Lee, 2013). Interventions designed to reduce substance use in pregnancy must meaningfully take these factors into account and address them through the provision of social and economic supports. This requires a harm-reduction approach that acknowledges that it is difficult for patients to stop using substances on their own, even when they desire to do so (Burns et al., 2016; Poole, 2013). Models of counseling and substance treatment that exist outside of the current cannabis literature tend to embrace the principles of harm-reduction (Gould, 2014; Martin, 2016; Wright et al., 2012) and have shown improved outcomes for both neonates and their parents (Weight et al., 2012).
Beyond the development of public health recommendations and policy, we also need to develop research approaches that consider—rather than exclude—the role of the social determinants of health in shaping neonatal and maternal health. Across the literature on substance use in pregnancy, calls have been issued for research that moves beyond simple, linear cause-and-effect analysis to consider the role of multiple variables—including environment and social determinants of health—on neonatal and childhood outcomes (Bauer et al., 2002; Jones et al., 2019; Schempf & Strobino, 2008). Failure to consider the interplay between environment, resources, and other social determinants of health causes undue harm to children and families and foreclose opportunities for the identification of opportunities for interventions and investments that may promote health and well-being (Flavin & Paltrow, 2010; Jones et al., 2019). If the goal of this body of literature is truly to improve the health of the population and promote the well-being of pregnant people and neonates, it is vital to consider substance use within the context that it unfolds. Vitally, we must also consider pregnant people as people—not just pregnancies—with problems, desires, concerns, and choices that pre-exist their pregnancies and will persist after their babies are delivered.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors thank the Department of Obstetrics & Gynaecology, London Health Sciences Centre for their generous support of this research via the Internal Research Fund.