
Abstract
Amphetamine-Type Stimulants (ATS), such as amphetamines, MDMA, and methamphetamine are a commonly used class of illicit drugs in Europe. There is a large existing literature on motives for the use of illicit drugs, often focusing on initiation. However, few studies have explored the reasons why some people choose not to use drugs (non-use), and even fewer focus on the social processes influencing non-use of ATS specifically. We explored social processes related to normalization, and how persistent non-users negotiate their non-use in social contexts where ATS is used, using qualitative interview (n = 21) and survey questionnaire (n = 126) data from a mixed-method study conducted in the Netherlands and England. Our findings showed that in both countries, most participants were repeatedly exposed to ATS use, often in social or nightlife settings. Participants abstained from use for a number of reasons, including: lack of interest in illicit drug use in general; desire to maintain control over their own behavior and environment; and to avoid the associated health risks. Social processes also shaped persistent non-use of ATS, via conscious socialization with, and selection of, other non-using peers over time. Our findings contribute to the literature on the normalization thesis, showing that recreational ATS use is only partly socially accommodated and normalized among persistent non-users, suggesting differentiated normalization.
Keywords
Introduction
Both in Europe and globally, Amphetamine-Type Stimulants (ATS), such as amphetamines (“speed”), methylenedioxymethamphetamine (“MDMA” or “ecstasy”), and methamphetamine (“meth”) are the second most commonly used class of illicit drugs after cannabis (European Monitoring Centre for Drugs and Drug Addiction, 2019; United Nations, 2019). Across Europe as a whole, 3.7% of those aged 15–64 have used amphetamines (including methamphetamines) at some point during their life; for lifetime MDMA use, rates are higher at 4.1%. Among European young adults (15–34 years old), 1.0% report use of amphetamines, and 1.7% report MDMA use during the past 12 months (European Monitoring Centre for Drugs and Drug Addiction, 2019). However, prevalence of ATS use varies by country, and by type of ATS. Within the European Union, the highest rates of MDMA and amphetamine consumption were found in the Netherlands and United Kingdom (UK). In 2017, lifetime prevalence of MDMA use among those aged 15–64 years old was 9.4% and 10% in the Netherlands and UK respectively; with 5.4% and 9.9% reporting lifetime use of amphetamines (European Monitoring Centre for Drugs and Drug Addiction, 2019). Greater variation is seen in rates of use during the past year among young adults; 7.1% of those aged 15–34 years in the Netherlands had used MDMA and 3.9% had used amphetamines, compared to just 3.3% and 1.0% respectively of this age group in the UK (European Monitoring Centre for Drugs and Drug Addiction, 2019).
Demand for, and supply of, illicit substances continues to grow, with a marked rise in the diversity of drug markets, particularly in recent years (United Nations, 2019). Since 2009, there has been a 30% increase in those reporting past-year use of any drugs, although global population growth partly accounts for this trend (European Monitoring Centre for Drugs and Drug Addiction, 2019). At the same time, there has been an expansion in the types of different drugs available to users, particularly novel synthetic psychoactive substances (NPS), alongside an increase in the potency of certain substances, with associated heightened risks (Freeman et al., 2019; Peacock et al., 2019). In response to these trends, governments in Europe and elsewhere have introduced a range of different policy approaches aimed at tackling the substantial adverse health, social, and economic consequences of licit and illicit substance use (Barrio et al., 2017; Tsai et al., 2019). Drug policies which focus on the demand side generally aim to control and reduce these risks, by discouraging people from using drugs, or encouraging them to decrease their use, and/or switch to less risky substances or consumption practices. Demand-focused drug policies can be placed on a continuum from more repressive (“tough”) to preventative (“soft”) approaches. More repressive policy approaches are generally implemented through the criminalization of drugs, and law enforcement. In contrast, preventive approaches employ education, information, treatment, training, and other harm reduction measures to reduce or remove the risk factors of drug use; limit exposure to drug use opportunities; and empower people to refuse drug offers. In doing so, these preventative approaches build on an underlying assumption that knowledge of what motivates people to use drugs can usefully inform strategies aimed at encouraging non-use.
There is a vast existing literature on drug use motives, which is informed by varying theories and academic disciplines. In criminological theory, social relationships often play an important role in understanding and explaining illicit substance use, in different social, cultural, and subcultural (open/closed) contexts. Some scholars place emphasis on the social influences of drug use. Generally, social mechanisms can be grouped into three areas: pressure (people are strongly influenced by others to act in a certain way); selection (people select peers and/or partners who are similar in behavior to themselves); and socialization (people mutually influence each other’s behavior in interaction) (Liebregts et al., 2015). Influence is considered a more subtle, indirect form of pressure, which involves adapting one’s behavior to meet others’ perceived expectations, rather than feeling directly urged by others to change one’s behavior (Burns & Darling, 2002). A well-known elaboration of the importance of social context is the social learning theory, according to which individuals learn new behavior by a process of observation and imitation of, and reinforcement from, people they associate with (Akers, 2011; Zinberg, 1984). As drug use is often a social activity, this theory could also help explain the initiation and subsequent phases of consumption (Akers, 2011; Norman & Ford, 2015; Vervaeke et al., 2008). Research on the role of peers in young adult drug use has been scarce, but findings to date suggest patterns of both peer socialization and selection (Andrews et al., 2002; Van Ryzin et al., 2012). Other scholars focus more on individual psychological elements of theories of deviance, such as rational choice theory. Central to this line of thought is the perspective that individuals make decisions based on an informal cost-benefit calculus. Perceptions of these costs and benefits are influenced by individual and contextual factors, including personal characteristics and life experiences (Pratt, 2008). As such, it has been argued that recreational drug use can be considered as a rational process, where people who use drugs make balanced choices about when, where, and with whom they use (Aldridge et al., 2011; Liebregts et al., 2015).
In terms of the specific reasons cited by people who use drugs themselves, previous empirical research has mainly focused on factors related to the initiation of particular substances, such as ATS (O’Donnell et al., 2019). Studies have identified a variation of motives for the use of ATS, including: curiosity or tendency for experimentation (Duff & Moore, 2015; Levy et al., 2005); positive mood, pleasure and social motives, such as pursuing togetherness, talkativeness and increased sociability (Benschop et al., 2020; Green et al., 2020; Sznitman & Taubman, 2016); coping with stress, trauma, or other mental health issues (Fast et al., 2009; Levy et al., 2005; Smirnov et al., 2013); to improve work/studies performance (Boeri et al., 2006) or in private settings (such as stamina in nightlife settings) (Eiserman et al., 2005; O’Donnell et al., 2019).
Some studies have explored the social motives of non-use and attempted to categorize them, but these seldom explore how non-use was maintained by those individuals who want to continue participating in a social context. Two UK studies among adolescents and young people aged 11+ found that motives for non-use were mostly related to a lack of interest in the anticipated effects of illicit substances, combined with fear of those effects and the risk of potential harm (Fountain et al., 1999; McIntosh et al., 2005). A study in the Netherlands from Vervaeke et al. prospectively monitored young adults who were “ecstasy-naïve” at baseline but were likely to take ecstasy as they expressed intentions to use and had ecstasy using peers (Vervaeke et al., 2008). After approximately 1.5 years, 60% of the sample reported persistent non-use of ecstasy. Frequently cited motives for persistent non-use included lack of interest in and/or fear of the effects; concerns about potential harms; and lack of opportunity. A review by Rosansky and Rosenberg of 15 studies on drug abstinence also identified concerns about physical health and/or psychological damage, alongside a lack of interest or desire to use as the most salient reasons (Rosansky & Rosenberg, 2019). Other reasons were limited availability or access; concerns regarding illegality; and the cost of substances. Importantly, they also concluded that motives for non-use were specific to different types of substances. For example, fear of addiction was less applicable to cannabis compared to heroin (Rosansky & Rosenberg, 2019).
Overall, however, in contrast to the substantial body of work on drug use motives, studies on non-use of drugs remain scarce, with a particular paucity regarding the social processes involved in non-initiation. Measham and Shiner (2009) explored the important interplay between social structures and human agency in relation to ecstasy use, yet their debate did not include ATS and continuous non-use and rather offered a theoretical perspective of drug use as a “situated choice” that includes meaning about (shared) identity, practices and social processes (Measham & Shiner, 2009). There are some interesting elements to take from this and other previous studies on social processes and normalization that can shed light on the social context of non-use.
The normalization thesis was first described in 1998 by Parker and colleagues (Parker et al., 1998). They defined normalization by six dimensions through which recreational drug use is manifested: increased drug trying rates; increased regular drug use; increased availability and accessibility; more liberal attitudes toward recreational drug use among young people, especially young people who do not use drugs; a higher degree of cultural accommodation (visible in popular culture, media and policy). They found that recreational drug use had become normalized in the UK, being part of an everyday, non-deviant lifestyle of young people, which was, socially and culturally accepted by people who use and people who do not use drugs (Parker et al., 1998, 2002). However, while they found strong evidence of normalized cannabis use, they were more ambivalent about the extent to which stimulant drugs had a similar status. In particular, the frequently reported effects of stimulant drugs made some young adults less positively inclined to their use, and social acceptance was mainly limited to the party scene (Parker et al., 1998, 2002). Since this early work, the normalization thesis has been explored by several researchers in different countries, for several drugs and/or populations. Some researchers have found evidence in support of it, or for parts or specific sub-groups such as differentiated normalization, while others have contested the thesis (see Pennay & Measham, 2016).
With regard to the social context of normalization, previous research has focused on exploring dimensions such as tolerance to drug use, the extent to which people who use drugs have positive expectancies toward drug use, and whether drug use is perceived as deviant or unsafe (Sznitman & Taubman, 2016). Other measures of social accommodation of drugs among people who do not use drugs included drug use among peers, approving attitudes of drug use, and being “drug-wise” (Sznitman & Taubman, 2016). However, again, most existing studies have focused on the perspective of people who use drugs, and often in relation to use of recreational (illicit) drugs in general, as opposed to specific substances. This lack of research to explore perspectives of people who do not use drugs is especially striking given that one of the key features of normalization is the social accommodation of recreational drug use, including “attitudes to ‘sensible’ recreational drug use by adolescents and young adults, especially of non users” (Parker et al., 2002, p. 944).
In this article, we focus on the normalization thesis, more specifically the social accommodation and social processes of recreational ATS use, among people who do not use. We draw on findings from a broader, transnational study (“ATTUNE”) on ATS trajectories to explore social processes and interpersonal relationships related to normalization, and how people who do not use ATS negotiate their non-use in social contexts where ATS is present. The aim is to understand micro level processes underlying decisions about non-ATS use in social contexts where ATS use takes place.
Materials and Methods
Study Design
The ATTUNE study was multinational, and aimed to investigate which individual, social and environmental factors shape individual ATS use pathways over the life course (see for the published protocol for further details of this study Rosenkranz et al., 2019). Conducted in the UK, Germany, Poland, Czech Republic and the Netherlands, the study used a sequential, exploratory mixed-methods design, comprising qualitative interviews followed by structured questionnaires with people who use ATS and people who do not use ATS. Our initial qualitative approach here was informed by constructivism (Crotty, 1998) and the need to start by developing a deeper understand of how the experiences of people who do not use ATS were constructed as they engaged in different social and cultural settings and countries with others who chose to use. In starting this way, we were able to begin to understand not only how these individuals experienced their social world but also how they behaved and acted with and toward others in different social and cultural settings (Atkinson & Hammersley, 2007). A mixed-methods design was essential to enable us to first explore these factors in relation to individual experiences and perspectives on dynamics of change in ATS use patterns using qualitative methods. Next, these qualitative findings informed the development of a structured questionnaire which was used to validate and enhance the generalizability of the results in a larger sample of people who use ATS and people who do not use ATS. Thus, the methods were seen as complementary, and together aimed to generate an in-depth, contextualized understanding of the research topic.
For purposes of this paper, we focus on data captured in interviews and surveys with people who do not use ATS based in the Netherlands and UK only. Dutch drug policy is characterized by the separation of drug markets policy, dividing substances with an “unacceptable risk” (List I—commonly referred to as “hard drugs”) from cannabis products (List II—“soft drugs”), as laid down in the 1976 Opiumwet (Drug Act) (Blom, 2008). The Opium Act sets out that supplying drugs (possession, cultivation/manufacture, import or export of drugs) is punishable, depending on the quantity and type of drug involved, by up to 12 years’ imprisonment, however drug use itself is not criminalized. For ATS, changes in recent years include listing amphetamine-based NPS as a List I drug and an increasingly “zero-tolerance” policy regarding hard drugs (de Gee & van der Gouwe, 2020). In the UK the political landscape of drug policy is more complex (HSCC, 2019). The legal framework which underpins and relates to the misuse of drugs in all areas of the UK includes the Misuse of Drugs Act 1971, and the Psychoactive Substances Act 2016, which made the production, sale and supply of NPS, including particular types of ATS, illegal (HM Government, 1971, 2016). However, each of the separate UK administrations (England, Scotland, Wales, and Northern Ireland) can develop their own policy responses and approaches to tackle misuse in areas where responsibility is devolved. In England specifically (UK site of the ATTUNE study) policy has been driven by a largely criminal justice approach (HSCC, 2019) to reduce demand, restrict supply, and build recovery provision (HM Government, 2017). More recently however, there has been a call for a more “health focused and harm reduction approach” in UK drug policy, including decriminalization of possession for personal use of all substances (HSCC, 2019).
Yet despite some marked differences between the Netherlands and the UK when it comes to drug policy, with a focus on harm reduction in the former and criminal justice in the latter, both countries report high rates of MDMA and amphetamine use in comparison to other parts of Europe. As such, these settings provided valuable settings in which we could explore the social processes and normalization (aspects) of non-ATS use.
Participants and Recruitment
Purposive sampling methods were used to identify different groups of people who use ATS according to the currency and frequency of ATS consumption and a group of people who do not use ATS. For both the qualitative interviews and survey questionnaires, participants needed to be aged
The group of focus for this paper, exposed non-ATS users, were defined as individuals who had never used ATS, but had experienced opportunities to take these substances due to being present when family members, friends and/or partners were using ATS. For the ATTUNE study, ATS included a variety of stimulant-type substances, but most frequently concerned use of MDMA, amphetamine, followed by methamphetamine, and misuse of amphetamine-type prescription drugs (methylphenidate, e.g. “Ritalin”).
Multiple strategies were used to enroll participants into the study, including: snowball sampling, whereby individuals interested in the research were encouraged to share information about the study with other potential participants in their social networks; social media advertisements; leaflets distributed at universities; via gatekeepers working within substance use services/treatment facilities, third sector organizations and other relevant agencies; and through the researchers’ personal social networks. Recruitment continued until sampling criteria were met for diversity for the total sample in terms of age, gender, and socio-economic status of participants.
Data Collection and Analysis
Interested individuals were given an information leaflet and had the opportunity to ask questions about the study and the interview or survey. If the person was willing, able, and eligible to participate, written informed consent was obtained. Participants were then screened for eligibility and appointed to one of the sampling groups; this allowed research teams in different countries to monitor the course of the fieldwork and balance division of participants across groups. Both the qualitative interviews and survey questionnaire took place at a quiet location, mainly at participants’ preference: generally, either at participants’ homes, in a private room within a specialist or third sector service provider, at the respective research institute, or in a public space such as a cafe. After completing the interview or survey, participants received a small incentive by way of thanks for their participation (£10 shopping voucher in the UK; in the Netherlands €20 cash for the survey, and €30 for the interview).
For the qualitative interviews, a topic guide was developed with input from research teams and with input from an Expert by Experience (EBE) in the UK. This guide was used to structure conversations which captured participants’ life stories, including: critical events and key experiences (see Liebregts, 2018; Martens et al., 2020); information about friends, families and wider social networks; and perspectives on ATS non-use and/or other consumption of any other substances. It enabled the research team to engage those with lived experience and provided a platform from which to understand their experiences, motivations and opinions of factors that influenced and shaped their behaviors (Ritchie et al., 2013). It also allowed participants to reflect in greater detail about their own circumstances, as questions allowed them an element of control and freedom over the discussion which resulted in a fairer and fuller representation of the interviewee’s perspective (Mason, 2002). For those participants identified as non-users of ATS, we were particularly interested in exploring settings of exposure, motives for non-use despite having the opportunity, and whether and how non-use affected participants’ social relationships.
The survey included questions based on the key themes emerging from the qualitative study, as well as employing several validated instruments to assess participants’ substance use, mental and physical health, and psychological factors/personality traits (Franke et al., 2017; Hahn et al., 2012; Sarubin et al., 2015; Saunders et al., 1993; Sherer et al., 1982). For people who do not use ATS, questions focused on: factors shaping their exposure to ATS, such as the setting in which they first had an opportunity to use ATS; the reasons why they did not try ATS; and the number of times they had been exposed to ATS. All in-depth interviews were digitally recorded (with participant consent), fully transcribed, and entered into NVivo version 11 to support data management and analysis.
Qualitative data were analyzed using the Framework Approach following a five-step process: (1) familiarization; (2) identifying a thematic framework; (3) indexing; (4) charting; (5) mapping and interpretation (Ritchie & Spencer, 1994). Quantitative survey data were analyzed descriptively, using SPSS version 26. To integrate the qualitative and qualitative datasets, we used the “following a thread” approach (Moran-Ellis et al., 2006). In short, we first identified key themes in the qualitative data from both countries. Subsequently, these themes (threads) were explored in the quantitative data, with a focus on highlighting notable differences and commonalities in our results. Findings are presented as exemplar trends only, as we did not perform country-by-country comparisons with statistical tests, but rather, focused on the common patterns that emerged across both countries. All quotes presented in this paper are derived from the in-depth qualitative interviews. Tables summarizing key data on participants are based on findings from the survey questionnaire.
Ethics
Ethical approval for the UK qualitative interviews was granted by Newcastle University, Faculty of Medical Sciences, Ethics Committee (REF: 01204/2016) on 8th September 2016. Ethical approval for the UK survey questionnaire was granted by North East – Newcastle & North Tyneside 2 Research Ethics Committee on 25th May 2018 (REF: 17/NE/0283). Ethical approval for the Dutch data collection was not necessary.
Results
Participant Characteristics
A total of 147 individuals who do not use ATS took part in the qualitative interviews and survey questionnaires carried out in the Netherlands and England. The Dutch qualitative sample included 10 non-users and the quantitative sample 48 non-user respondents, totaling at 58 unique participants. In England, we interviewed 11 non-users and surveyed 78 respondents. Table 1 depicts the sociodemographic characteristics of participants in each country. In both countries, most participants were female, and the age of participants ranged from 19 to 64 years. Additionally, most participants were in employment, and were educated at secondary school level or higher.
Sociodemographic and Substance Use Characteristics of Qualitative Interview and Survey Participants in the Netherlands and England.
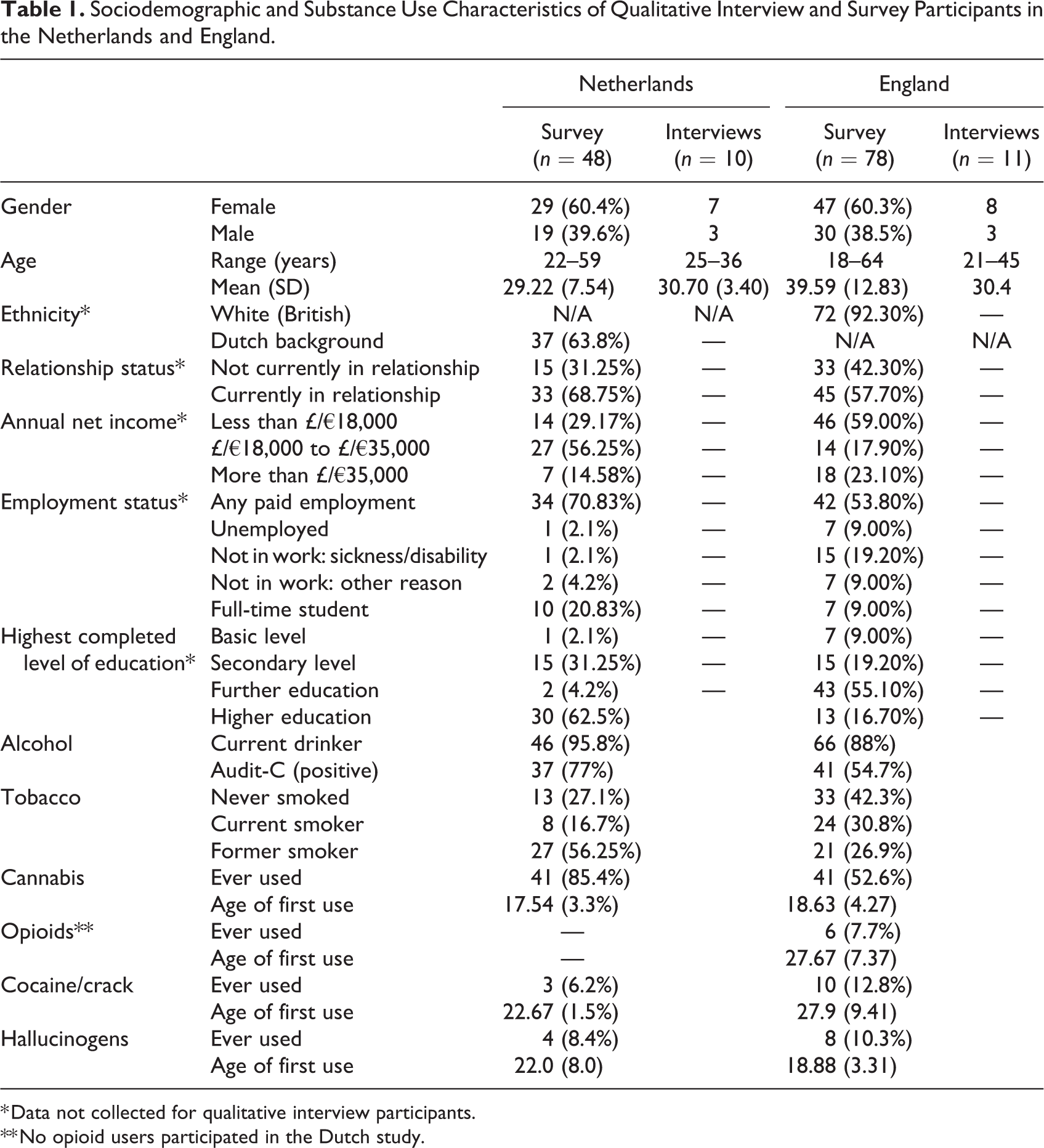
* Data not collected for qualitative interview participants.
** No opioid users participated in the Dutch study.
We also captured data on participants’ use of other licit and illicit substances. As shown in Table 1, although participants were all classified as people who do not use ATS, they were not abstinent from all substances. In both the Netherlands and England, the majority were current alcohol drinkers and the majority had smoked tobacco. Most participants had also used cannabis, particularly in the Netherlands (85.4% of participants compared to 52.6% in England), and some participants in both countries also reported lifetime consumption of other illicit drugs, including hallucinogens, cocaine and in England at least, opioids.
ATS Exposure: Place, Persuasion, and Temptation
Interviewees were on average 18 years old when they were exposed to ATS for the first time in the Netherlands and aged 20 in England (see Table 2). With a few exceptions, most participants had been exposed to ATS use on multiple occasions, varying from several times to all the time.
Age, Context, Frequency of Exposure to ATS and Reasons for Non-ATS Use of Survey Participants in the Netherlands and England.
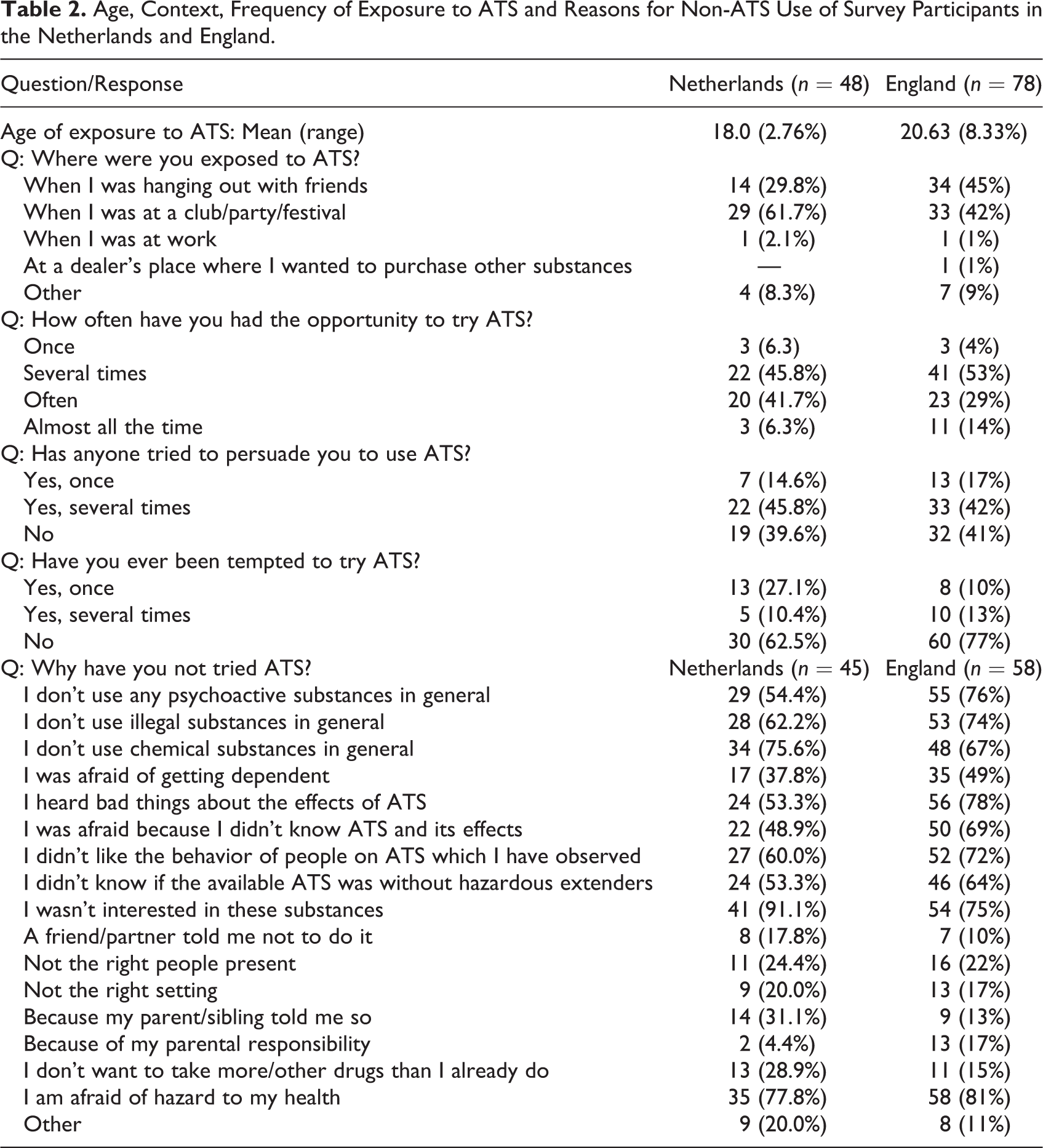
Most survey participants in both countries described being exposed to ATS in either social settings or at clubs, parties, or festivals (see Table 2). Exposure to ATS occurred in a nightlife setting, such as a club or party, where participants attended these events with peers who were already somewhat experienced with ATS use: The first time I came across MDMA, was at a New Years’ Eve party, and everyone I went to the party with used it…it was a different group [than my own friends]: friends of a friend of mine. And they all used drugs, or at least MDMA so he asked if I wanted too, but I turned it down, I didn’t want it. (Susan, age 31, Netherlands) When it started being the big nights out in the second year, then that’s when I noticed that people were planning beforehand…I’d be at normal pre-drinks with a certain group of people and I’d notice that no-one’s drinking. I’m like, “Why is that?” and they’re all just sorting out this stuff, totally alien to me, I’ve got no idea what’s going on. Figuring out how many bombs they’re going to do of especially MDMA. (Stephanie, age 23, England) The atmosphere was fun, we had drunk some alcohol. I knew they had it, but I didn’t know they would offer it. At a certain moment we were just sitting somewhere and they pulled it out their bags and they said: do you want a half? And I really thought about it, but rather not. Despite a very nice atmosphere. (Johan, age 36, Netherlands) The only time that I’ve ever thought anything was a good idea was when Ritalin was coming around. We were in our third year. I don’t think I’d ever have done it but because it was an ADHD drug, I just thought if people take it medicinally then it might not be that bad. Obviously, I wouldn’t have done it because I would have been worried. Yes, I just thought if they are giving it to people then perhaps it wouldn’t cause schizophrenia and because I really valued my exam results. (Callum, age 24, England)
Non-Initiation and Motives for (Persistent) Non-Use
Participants cited a variety of reasons influencing their non-use of ATS. Table 2 shows the motives for non-use provided by participants in the survey questionnaire. The most frequently mentioned reasons for non-use in both England and the Netherlands were: “I wasn’t interested in these substances”; “I’m afraid of hazard to my health”; and “I don’t use chemical substances in general.” Alternatively, the least mentioned reasons for non-use were: “a friend/my partner told me not to do it”; “not the right setting”; and “not the right people present.” In the qualitative interviews, some participants articulated a general lack of interest in, or aversion toward, illicit drugs in general, and described themselves as being “anti-drugs.” Others appeared more averse to using ATS specifically. Given that exposure to ATS was a prerequisite for inclusion in our study, it is probably to be expected that none of the participants mentioned lack of availability as a barrier to ATS use. Most interviewees believed that ATS would not add anything to their life, felt no interest in ATS, and/or no need to use them.
As suggested by the survey questionnaire results, the narratives captured during the interviews suggested that motives for non-use were frequently connected to a desire to maintain “control” and to avoid personal risk: It’s also about losing control. I’ve seen enough people who totally lost it at a festival. Lying at the outskirts of the festival foaming at the mouth. I don’t want to experience that. You don’t know how it will work out. (Robert, age 25, Netherlands)
ATS Use and Social Relationships: Processes and Consequences
A key theme which emerged from the data was the social influence of peers to use. Many participants reported that they had to fend off repeat attempts by their members of their social network to get them to try ATS (as above, Table 2). Nevertheless, for most participants, refusing to try ATS appeared a relatively unproblematic experience, for example: Well, they know more or less what I think about it. So “dude you should do it” doesn’t happen. I could use everything. But I’m not attracted to it, so why should I. They are very relaxed about it, they would never push it. They only tell me to let them know if I want it. Or that someone will stay sober if I would like half a pill. (Robert, age 25, Netherlands) Those nights that we would have in [name of club] where everyone else was just ridiculous, off their face on MDMA, those actually ended up being relatively fun nights, even though I was completely stone-cold sober and I’d maybe only had a couple of beers, because everyone else was just so happy. It kind of rubs off on you, like you end up actually having a relatively good night because of that, really. (Stephanie, age 23, England) She used a lot of drugs, regularly she gave me the feeling that because I didn’t use any, I was a boring person, and that was also where we clashed. That contributed to the break-up, because she lied about it [her drug use]. She started lying more and more. And the lying was the break-up. And also, we were totally different types. Totally different future perspectives. (Emily, age 34, Netherlands) The first time I ever felt pressured to use drugs was by her and it was at her party. She had this Halloween party and she was using cocaine and speed…She was being really arrogant about it and she was like, “Why not? Why won’t you use it? There’s nothing wrong with it.” (Lisa, age 36, England) Sometimes I’m the designated driver, but usually I’ve had some beers myself, so I won’t see so sharp either. Maybe we’re at a different level, but we can still laugh together. They supposedly experience the lights and sounds in a different way. But we both have a good time. A bit of laughing, chatting, dancing. And for me that’s fine. (Robert, age 25, Netherlands) In my peer group there are always others who don’t use, so they become a bit of your buddies at festivals. I also hang out with the others, but around 4-4:30 AM I’m done and go to the tent, and they continue partying (…) But I took distance from several peer groups in the past. I thought: ok, I really like to have a chill night, but not when every weekend everything is displayed full house, because then you’re not levelling. I’m drunk, babbling, and the other one is like: “yeah man yeah, fucking nice here and I love you man.” That’s not the same level. And if someone always goes left and you always go right, you’re not heading into the same direction. (Mike, age 30, Netherlands)
While most accounts described how participants would initiate these processes of peer selection, there were examples of this working the other way around. For example, as another participant reported: Every time they’d go off they’d say, “Right who’s coming?” And I made it quite clear early on that I didn’t want to do that, but then a couple of people had. A couple of people had said quite early on, “No we’re not interested.” But then gradually over time they’d started going off with them as well, and I was quite worried because I wasn’t worried that I was going to cave, I was just worried that my group was going to get smaller and smaller and I was going to become the minority of people. Because it started off, I remember two or three of them going off, and by the end of it there’d be like a whole hour where there’d be people off, and it made it quite—they were quite divisive in the way that they took themselves off to do it. Which I suppose was quite a good thing because it meant you weren’t actually surrounded by people taking drugs. (Emma, age 24, England)
Interviewees’ views of their peers' ATS use and drug use in general varied. While not necessarily expressed as disapproving of their substance use, some interviewees did appear to evaluate their peers’ behavior while consuming ATS negatively: You could see that they were a kind of euphorically, but I saw that as total affectation, you know. (Rose, age 27, Netherlands) Some years ago, I noticed that people who are now having jobs, that they didn’t really experience it [drug use] during their puberty. And they now started to experiment a lot with all types of drugs, at festivals. But I had the idea that many of them only did it because everyone was doing it. To fit in. I always was very reluctant to that. I still had no need for it, for me nothing changed. And I’m definitely not gonna do it because others do it. (Stephanie, age 33, Netherlands) I think it’s immature, and I wouldn’t, if I’m going out now, I have to really enjoy my night, and so that would just be super boring to me. So I would just go home, and I don’t like the risk element or anything…I definitely would associate it with age. If I saw somebody my age taking ecstasy, I would just think I would feel sad for them. That they had to do that, and I guess I would just see it as pathetic…. (Lucy, age 34, England) I think that over time my vision has changed. I can accept it more now than before. It used to be a big no-go for me. But [ATS use] it happens so much now, that I shrugged it off, like: ok it happens, I can’t prevent it. People use it and I try to see that they don’t get addicted and do it incidentally. I better accept that it happens. I can worry about it or not, that doesn’t concern them. It used to be very far out there for me, now I’m older so you’ve seen more. The first time when you see someone high, it scares you. My god what is she doing?! Those eyes…And now it’s like: next. A kind of habituation. (Susan, age 31, Netherlands)
Discussion
We explored the social processes shaping persistent non-use of amphetamine-type stimulants (ATS) in relation to normalization using data from a mixed-method study conducted in England and the Netherlands. All our participants had been exposed to ATS use via social and familial networks, often on multiple occasions, but had actively decided not to use these substances. Some interviewees had always stood firm in their decision not to use ATS, while others had experienced second thoughts at some point about whether to try stimulants.
Reasons for ATS non-use among people who persistently do not use ATS were related to a lack of interest in ATS and its effects, concerns about the associated health risks, and an aversion to “chemical” substances in general. This is largely in accordance with the findings of other studies in this field (Rosansky & Rosenberg, 2019). However, in addition to previous studies, our study also found that motives concerning health risks were mainly associated with feelings of “staying in control” and “responsibility.” Thus, it was not the unfamiliarity of ATS effects, but rather the uncertainty of its specific consequences that refrained them from ATS use; the non-users in our study were often quite informed about effects of ATS, however they weren’t sure how those would manifest for themselves. Interviewees were not abstinent from other non-ATS substances, either licit or illicit. However, apart from alcohol and cannabis, the majority did not regularly consume other illicit substances. Many interviewees opposed drugs in general, yet some were particularly averse to using ATS. This partly reflects previous evidence that suggests motives for non-use are specific to different types of drugs (cf. Rosansky & Rosenberg, 2019).
For the majority of participants, opportunities to try ATS comprised exposure to MDMA (ecstasy) specifically and occurred in nightlife settings when socializing with peers, for example in a club or at a festival. Commonly, these interviewees described a social context where there was mutual respect and understanding from both parties about decisions around whether to consume ATS or not. Most participants reported peer or partner influence to try ATS (mainly to meet others’ expectations or preferences), but had not experienced overt, direct peer pressure. As such, despite the acknowledgment that peer influence to consume ATS existed within social networks, the behavior was not imitated. Interviewees’ attitudes ranged from disapproval to the perspective that ATS were just not for them. Additionally, several interviewees felt they had developed a more accepting attitude toward people who use ATS over time, which they ascribed to repeat exposure within their social network; a trend that could be interpreted in terms of the normalization thesis of party drugs in particular social and cultural contexts (Measham et al., 1994; Parker et al., 1998; Taylor, 2000).
In contrast, narratives from other interviewees suggested that continued ATS use by members of their social networks resulted in a gradual process of peer selection being undertaken. Sometimes this process took place alongside their peers’ ATS use, meaning the friendship was maintained, but the participants carefully avoided contact during times when consumption could be expected. For example, when they consciously socialized with other (less close) people who do not use drugs instead of with their ATS using peers at festivals, or when they made the decision not to attend a certain party because their friends had notified them that they would use ATS. Due to their peers’ ATS use, these participants chose to select other peers who were similar in behavior to themselves, to (partly) associate with, rather than being influenced by their peers to act similarly (peer socialization). The unmet desire of some participants to be on “the same level” while going out when they used alcohol and their peers used ATS, is interesting in light of the increased sociability and pursuing togetherness that are often reported as motivations for and effects of ATS, especially MDMA use (Green et al., 2020). However, in a few cases, this peer selection was more permanent: the discrepancy between interviewees’ non-use and their peers/partners ATS use had led to the ending of their relationship. Nonetheless, these individuals tended to be part of peer groups where a considerable proportion were individuals who do not use ATS, and/or had less opportunity to spend time in the types of spaces (clubs, houses, university accommodation) and events (parties, festivals) where ATS could be more easily accessed. This meant that in these cases exposure was infrequent and less normalized. Additionally, the fact that some participants perceived continued ATS use in adulthood as immature, stemming from insecurities or a desire to fit in, and found it unacceptable or wrong for these interviewees seemed a way to reinforce their non-using identity and behavior. This clearly distancing themselves from their using peers also opposes social accommodation of ATS use. Existing studies on drug use of young adults show that both peer socialization and peer selection shape consumption practices (Andrews et al., 2002; Van Ryzin et al., 2012). Our findings show that these social processes also appear to influence non-use, at least for ATS, however peer selection seems to be a more prevailing factor.
Overall, despite differences in substance use contexts, similar key themes emerged from our analysis of interviews with non-ATS using people in both the Netherlands and England. There were some differences identified in relation to certain survey questions (e.g. prevalence of lifetime cannabis use was higher in the Netherlands; age of first exposure to ATS in England was higher; slightly different top three motives for non-use), but the general picture was one of similarities and overlap between the countries. In both England and the Netherlands, most participants were exposed to ATS in social or nightlife settings; had experienced repeated opportunities to try ATS; and motives for non-use were commonly connected to a lack of interest, a desire to maintain control and to avoiding personal (health) risks. Moreover, social processes of persistent non-use appeared similar in both countries and individuals appeared to be able to negotiate substance use within their social contexts (cf. Measham et al., 1994). This was achieved in various ways, for example by keeping firm in their non-use, by associating more with other non-using people, or by reinforcing their identity as someone who does not use ATS by negatively inferring or stigmatizing their peers ATS use. Since experiencing drug-related stigma can have several effects, such as poorer health, difficulties with achieving a house or a job, assumingly can deter persons who experience substance use problems from seeking treatment and as stigmatization can eventually affect policy makers (Kelly et al., 2021; Seear, 2020), such processes of stigmatization are undesirable. It is therefore important to encourage common understanding among people who use and who do not use ATS, and to use non-stigmatizing, person-first language (Seear, 2020).
Thus, on the one hand, our findings contribute to the literature on normalization, showing that on the one hand recreational ATS use is socially accommodated and normalized among many individuals who do not use ATS, because of tolerant or (increasingly) accepting attitudes toward ATS use, and the knowledge non-users have about ATS, which can be interpreted as being “drugs-wise” (Sznitman & Taubman, 2016). Another type of boundary work involving both our participants and their using peers was the capability to talk about the topic and negotiate on boundaries in terms of times and places were ATS is used, which is part of assimilative normalization (Sznitman & Taubman, 2016). Also the often reported mutual respect about ATS (non-)use decisions and the effortless mingling of people who do not use ATS and people who do use ATS indicates social accommodation. In contrast, however, the negative inference and stigmatization of some participants toward their using peers, the labeling of ATS as deviant or wrong, and the processes of peer selection or shorter or longer term due to their using peers, all point to non-accommodated, and non-normalized ATS use, also in the party scene (cf. Parker et al., 1998). All in all, several findings point into the direction of normalization of ATS, yet more likely suggests differentiated normalization (Measham et al., 1994; Parker et al., 1998; Pennay & Measham, 2016; Williams, 2016).
Strengths and Limitations
This study greatly benefits from a mixed-methods design, as it gave additional perspectives to our findings. Another strength is that our study is one of the few studies on non-use that includes only people who do not use ATS and who have been repeatedly exposed to ATS use in their own social environment, and who actively turned it down. Participants all (as an inclusion criterion) had to be exposed to ATS for the first time at least 5 years before the interview, to have had the opportunity to develop a drug use career. Consequently, they can be considered as (true) persistent non-users. Overall, this study brings forward some interesting in-depth insights into social processes of persistent ATS non-use and normalization of ATS.
However, some limitations should be acknowledged. Firstly, it should be noted that the non-using people in our sample consisted of a selective sample of recurrently exposed participants, and as a consequence, ATS had been (at least in a certain period in their life) available for them, and because of its use in their social networks it could be argued that they were already more familiar with it than other non-users would be. This could have affected their motives for non-use, as well as their perspectives on their peers. Interviewees’ perspectives on their peers could have been affected by their participation in our study, as they were invited to describe their views on ATS use and their peers who use ATS, and how that relates to their own behavior. The emphasis on this topic could perhaps have created a sharper contrast, a more distant view or different wordings than actually experienced or thought. In this perspective, the interviews might have “co-produced” a sense of stigmatization of ATS use. On the other hand, several indications suggest this probably did not occur. Interviewers were trained, adopted a neutral stand toward the interviewees, and the interview focused on experiences from the interviewee’s perspective and understanding. Moreover, participants were not abstinent from all substances, their motives for non-use were diverse, and so were their views on people who use drugs, and on their peers using ATS; varying from being anti-drugs to ATS being just not for them. ATS use of their peers was also varying, yet mainly recreational and our findings showed a general mutual respect between people who do not use ATS and those who do use regarding each other’s drug use/non-use. Nonetheless, this possible coproduction of stigmatization is something for researchers to be aware of when conducting research in this area (e.g., discuss it within the research team before conducting the interviews) and more generally reflect on their own (possible) role in data collection. Thirdly, the age of their first exposure to ATS use was 18 years on average, and often continued from then on. At this age adolescents become young adults. Exposure therefore did not often take place during early adolescence, and our participants at this age stage might be more autonomous, and less sensitive to peer influences, in particular peer pressure. Nonetheless, we found interesting findings regarding peer processes among non-using young adults. Furthermore, there were some methodological differences between the Netherlands and UK regarding sample size, incentives given, and recruitment procedures. Our aim was not to structurally compare country differences, but to describe and explore the social processes and contexts of persistent non-use of ATS in two countries. These methodological differences could have affected the final creation of the sample, and with that the comparability of the data between the countries. Yet, as mentioned above, findings between the countries were largely in accordance. Finally, our sample could be considered as relatively small, and while we sought to recruit as diverse a sample as possible, included an overrepresentation of females. Moreover, our quantitative sample can be considered somewhat heterogeneous in terms of socio-economic status. Thus, we cannot claim our findings to be representative for all people who do not use ATS. However, given the scarcity of studies on persistent non-use of stimulant drug use, this was an exploratory study and we did not aim for representativeness.
Implications for Policy, Practice, and Future Research
Our findings give some guidance/directions regarding prevention and policy. Participants’ attitudes toward drugs were somewhat varied; some were rather open to licit and illicit substances, others considered themselves as anti-drugs. For both types, we found that the effects of ATS they had seen with their peers could play a role in wanting to refrain from ATS, which may be present an opportunity for prevention and education. Since motives for ATS non-use among people who persistently do not use ATS were related to a lack of interest; concerns about health risks; and aversion of chemical substances in general, this also gives some tools for prevention to focus on, such as expanding awareness of health risks at young age. Some participants had different, more tolerant views on methylphenidate such as Ritalin (even when used as non-prescriptive) and on some NPS because of their legal status and the features they connected to it such as being less harmful. Additionally, a majority reported that they did not use ATS because they do not use illegal substances in general. This suggests that at least for people who persistently do not use ATS, drug policy would affect attitudes and perhaps also behavior of non-users toward drugs. Further, while our interviewees experienced peer influences but seemed less sensitive to act on these, prevention might want to focus on increasing resilience of teenagers and young adults to feel strong enough to make their own decisions.
For future studies it might be interesting to see if our findings regarding social processes can be extended to persistent non-users of other drugs, or in other countries. We found a general mutual respect between people who do not use ATS and those who do use regarding each other’s drug use/non-use, yet at the same time there was sometimes strong disapproval and negative attitudes toward people who use ATS, which could indicate differentiated normalization of (certain) ATS. It could be argued that in other countries where these substances are less prevalent and/or normalized, or where drug policy and legislation is more divergent, people who do not use ATS experience different peer processes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: ATTUNE was a collaborative project supported by the European Research Area Network on Illicit Drugs (ERANID). This paper is based on independent research commissioned and funded in the Netherlands by ZonMw (project number: 63200000103) and in England by the National Institute for Health Research (NIHR) Policy Research Programme (project ref. PR-ST-0416-10001). Amy O’Donnell is funded by a National Institute for Health Research (NIHR), Advanced Fellowship (grant reference: NIHR300616). The views expressed in this publication are those of the authors and not necessarily those of the national funding agencies or ERANID.