
Abstract
Drug consumption rooms (DCRs) have been established to reach high-risk people who use drugs (PWUDs) and reduce drug-associated harm. Despite effectiveness, their establishment requires strong advocacy and efforts since moral perspectives tend to prevail over health outcomes in many countries. DCRs have generally emerged as a local response to inadequate central government policy. Likewise, the initiative of the Municipality of Helsinki in 2018 opened up a discussion between central government, society, and local actors in Finland. This would be the first DCR in Finland, which makes the policy process and the progress of the initiative interesting for analysis. In this article, the identification of agents, structures of interactions, environmental challenges, and policy opportunities are analyzed within the framework of complexity theory. Our results show that the initiative faces policy barriers that have mainly arisen from the conceptualization of DCRs in moral frameworks that result in the prolongation of political and professional actors to take a position on DCRs.
Introduction
Drug-induced deaths have become a significant issue in Europe over the last few decades (Alho et al., 2020). Finland has higher rates of drug-induced deaths compared to the European average. The average drug-induced mortality rate among adults (aged 15–64 years) was 22 deaths per million in Europe in 2017, whereas in Finland it was 53 deaths per million (European Monitoring Centre for Drugs and Drug Addiction, 2019). Drug-related deaths increased by more than one fifth the year before and reached 261 deaths in 2018, which was the highest level in Finland’s history. Opioids, mainly illegally-sold buprenorphine, and amphetamines, both injected, are the primary substances linked to high-risk drug use and drug-induced death in Finland (European Monitoring Centre for Drugs and Drug Addiction, 2019).
Drug consumption rooms (DCRs) are one example of the promising interventions for reducing the harms of drug use (The European Monitoring Centre for Drugs and Drug Addiction, 2018). They are designed to reach isolated people who use drugs (PWUDs) at risk of death by overdose and the spread of infectious diseases. Besides promoting treatment and increasing the associated economic benefits of harm reduction programs, they target minimizing public order problems and crime reduction in certain areas (Belackova et al., 2019; Kennedy et al., 2017; Watson et al., 2013).
DCRs were first introduced to people who inject drugs as supervised injection facilities, safe injection sites, and medically supervised injection centers. However, their target population has expanded over time and they have begun functioning as supervised smoking facilities for people who smoke or inhale drugs (especially crack cocaine) as well (Potier et al., 2014; Vander Laenen et al., 2018; Watson et al., 2013). Some of the factors that undermine DCRs’ capacity to provide safe and secure services to PWUDs include lack of control over the type of drugs consumed, the limited availability of drug-use equipment, the presence of others in the booth, and poor physical design of facilities. Additionally, the availability of public health programming (or lack thereof), local policing practices, and broader criminal justice approaches to illicit drug use are also contextual factors for the better functioning of DCRs (Watson et al., 2013). However, despite their risks and the less-than-ideal contextual factors, the positive attitude toward DCRs across Europe has not diminished.
Since drug use is mainly an urban phenomenon, DCRs emerge in metropolitan areas where local responses are inevitable for public drug use, particularly injecting drug use, in open drug scenes, including railway stations, staircases in residential buildings, and parks. The availability of drug treatment, harm reduction and social services, and as well as law enforcement efforts may not deter PWUDs from public drug use (Hedrich et al., 2010). The local context mobilizes civil society activism to enforce local and central government to take effective measures. Disobedient activities, public gatherings, and media outcry were used to attract public attention (Houborg & Frank, 2014; Zampini, 2014). During such discussions, public opinion and attitudes tend to change. DCRs were sometimes established with local consensus in contrast to central government will, as in Belgium (Smith et al., 2019), or with national-level regulations, as in France (Jauffret-Roustide & Cailbaul, 2018).
However, DCRs require a substantial policy shift and political support because their relevance is discussed beyond the health framework. Various moral or ideological approaches still have a considerable impact on shaping drug policy in many countries, which sometimes undermines the evidence and postpones the establishment of DCRs (Belackova et al., 2019). Besides, the social construction of the DCR phenomenon affects the selection of the evidence and rationales of responses to the drug problem (Lancaster, 2014). Disagreements and counter-arguments have the potential to be a reason for policymakers’ reluctance and to make DCRs a controversial policy issue.
The literature emphasizes that DCRs have generally emerged as a local response to this complex social-political issue (Houborg & Frank, 2014; Jauffret-Roustide & Cailbault, 2018). The previous experience of DCRs shows that local politics and local negotiations not only lead the discussion and progress, but also local actors share the responsibility of service delivery in the field. The first DCRs in Switzerland, the Netherlands, Germany, Denmark, and France were municipality initiatives (Houborg & Frank, 2014; Jauffret-Roustide & Cailbault, 2018). Although discussions regarding DCRs in these cities started many decades ago, they were either ignored as a policy tool or faced legal and political obstacles at the national political level for many years (Houborg & Frank, 2014; Jauffret-Roustide & Cailbault, 2018).
Despite central/national governments’ indifference (at best) or resistance (at worst) toward DCRs, local actors and their engagements constitute the driving force for DCR policy transformation around the globe. Such a wide disparity between central and local governments has necessitated a bottom-up initiative for DCR implementation to tackle drug-related problems. This bottom-up approach to a complex policy problem can be understood through the lenses of complexity theory.
Complexity theory analyzes the role of actors, their interactions, the rule structure that governs relationships, and the environmental context of the political system. It enables researchers and policymakers to model and predict the co-evolution of behaviors and attributes of actors in a system. This generates a more accurate picture of complex policy problems and their potential solutions. Therefore, this article uses complexity theory for analyzing DCR policy development and implementation in Finland.
Traditionally, Finland is a country with repressive drug policy where even personal use of drugs is considered a criminal offense. Using, possessing, and attempting to acquire smaller amounts of drugs are considered drug-user offences and carry a sentence ranging from a fine to 6 months’ imprisonment. In practice, this policy is implemented strictly although recently minors may be summoned to see a prosecutor, young first-timers may get a warning, and high-risk PWUDs may be referred to treatment (Kainulainen, 2009). However, from the late 1990s onward, a harm reduction policy including substitution treatment, needle exchange programs and other low-threshold services has gained a strong footing in Finland. In fact, this created the new paradigm for Finnish drug policy, the dual tracks model, where both harm reduction and criminal control approaches became well-established and expansive (Hakkarainen et al., 2007). However, no DCRs have so far been included in the range of harm reduction services. In this respect, an initiative by the City of Helsinki in 2018 to open DCRs in its own region can most probably be seen as a turning point for the policy. It has created a lot of societal debate and has put pressure on central government and political actors to take a stance. This debate is still ongoing, and as we know from other countries, as a controversial issue, progress may be slow.
The purpose of this article is to provide an overview of the emergence of DCRs, discuss stakeholders’ engagement in DCR policy development, and analyze DCR implementation in Finland from a complex systems perspective. More generally, it also explains how a turning point in drug policy can be created and developed, even in a repressive and restrictive context.
The remainder of the article consists of five sections; in the first section, complexity theory is introduced as the theoretical framework for this research. Next, the methodology section explains the procedures used for data collection and analysis. The three sections that come after the methodology section explain the progress of DCRs in Finland, and the application of complexity theory in DCR adoption and implementation. Finally, the article concludes with the discussion and conclusion section.
Theoretical Framework
Governance systems represent the complexity of the society they are embedded in (Simon, 1996). As human societies get more complex, so do the governance systems. DCRs emerge as a reaction to a set of complex social problems that include drug use, the health of people who use drugs, secondary health threats of drug use such as the spread of infectious diseases, and public nuisance. The implementation and governance of DCRs is inevitably a complex policy issue, and requires a theoretical and methodological viewpoint that will account for the complexity of the problem being examined (Seear & Moore, 2014; Stevens, 2020). Researchers have adopted the complexity theory approach for addressing complex and dynamic policy issues like DCRs for decades (Kiel, 2014).
Complexity theory is a set of theoretical and methodological tools for analyzing phenomena that are complex in nature. Its scope spans a broad spectrum of scientific disciplines such as statistical mechanics, applied mathematics, physics, ecology, system science, and social sciences. Because of this diversity in its application, complexity theory can best be defined within the specific discipline it is used. In public policy and administration research, complexity theory is used for developing solutions for complex (i.e., “wicked”) problems, and it is often coupled with system theory. That is because complexity is a characteristic of a system, which makes complexity theory a systemic theory (Byrne & Callaghan, 2013). This article uses the “complex systems” approach for analyzing the Finnish case in the adoption of DCRs.
A complex system is a “collection of diverse, connected, interdependent entities whose behavior is determined by rules, which may adapt, but need not.” (Page, 2011). 1 Complex adaptive systems consist of four fundamental elements (see Figure 1). These are agents, networks and interactions, rules that govern actions and interactions of actors, and the internal and external environment (Epstein & Axtell, 1996). In the context of DCRs (depending on the unit of analysis and the research question), an agent may be a PWUD, a local government agency, a national government agency, a healthcare agency, a local NGO, or a citizen group. These actors are interdependent with respect to the implementation and governance of DCRs. Their interactions are governed by formal laws as well as social norms (i.e., rule structures). Actors and their interactions with each other shape the environment within which they exist. In return, the environment shapes actors and their interactions. For example, drug consumption is a social behavior as much as it is an individual choice, and it happens within a social system (or network) of PWUDs, sellers, distributors, producers, and so on. When the environment changes, for example, police start cracking down on street sellers, and actors in the system adjust their behavior to cope with environmental changes. A change of behavior in the drug system triggers the modification of policing strategies and tactics. Such changes are a result of the continuous interaction between the agents and the environment in a complex system. These fundamental elements of CAS give rise to defining characteristics of CAS, which are emergence, self-organization, co-evolution, and nonlinear dynamics.
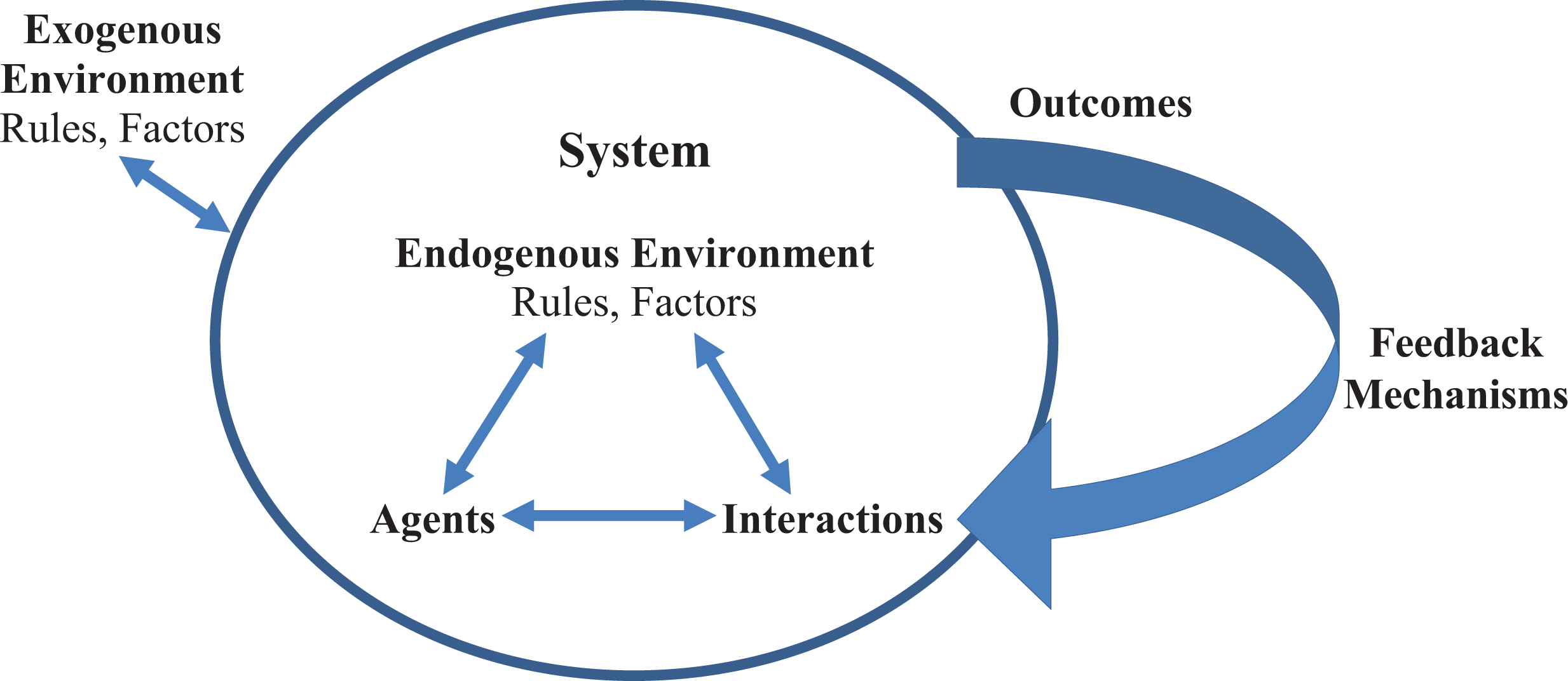
Core elements of a CAS are agents, rules, interactions and processes, the environment (endogenous and exogenous), and feedback mechanisms (Adapted from Rhodes et al., 2011, p. 11).
Emergence, self-organization, co-evolution, and nonlinear dynamics are widely discussed in complexity literature, as they apply to public policy and administration (Morçöl, 2013). Emergence refers to the characteristics of a system that emerge out of patterns of interactions between actors in a system. Emergent properties of a system are different than the properties of components at the micro-level and cannot be reduced to the micro-level. For example, human consciousness is an emergent property of the human brain, which consists of billions of neurons and their connections (Minsky, 1988). Therefore, consciousness cannot be reduced to individual neurons.
Similarly, societies are complex adaptive systems (Buckley, 1998) consisting of individuals, interactions, rule structures (e.g., laws, social norms), and the environment within which people live. Specific properties of society, such as culture, emerges out of communicative acts among people, and such emergent properties cannot be reduced to properties of citizens of that society (Byrne, 1998; Luhmann, 1996). Such communicative acts are not limited to verbal communication but include behaviors, written and nonverbal communications, and symbols (Luhmann, 1996). In other words, communication between actors is the primary form of interaction in social systems, which leads to emergent properties in society. In the implementation and governance of DCRs, just like in many other policy issues, it is essential to identify communicative patterns between the stakeholders of DCRs, PWUDs, and the local community. Such patterns can be helpful for understanding the potential outcomes of policy decisions. For example, introducing DCRs in a specific location in a town, such as near a school, may convey an unintended message to some stakeholders. The reactions of the stakeholders to such a symbolic message, albeit unintended, can cause the emergence of a backlash from an otherwise disinterested community.
Self-organization is the second characteristic of CAS. In a complex adaptive system, actors will always seek ways to get more information and position themselves in a more advantageous way to advance their survival (Holland, 1995; Page, 2011). Interactions between the actors and the feedback mechanisms between the system and its environment allow actors to sense changes in their immediate environment and adapt their behavior to those changes (Holland, 2012). Such adaptations happen at the micro-level and do not necessarily impact every actor in the system (Holland, 1995, 2012). When enough actors modify their behavior, the system self-organizes itself in response to the environmental changes.
In complex social systems, actors are reflexive, which means that they can make a decision on their own and do not have to act based on natural law. Actors in social systems can plan, think, predict, anticipate, and respond (Teisman et al., 2009). The reflexivity of actors implies that they have the capacity to receive, store, process, and convey information and act based on the interpretation of that information. Such characteristics of self-organization point to the close association between self-organization and emergence. In fact, self-organization can be characterized as the “emergence of new structures enforced by interactions, without the imposition of any external or internal actors” (Teisman et al., 2009, p. 9). This is a defining characteristic of collaborative governance networks that are salient in some policy areas. More specifically, self-organization refers to steering activities of various actors such as government agencies, nonprofits, and citizen groups, without a hierarchical, bureaucratic structure. Here, each actor in the system tries to steer or control the activities of others through communicative acts (Buijs et al., 2009). Such efforts inevitably require technical, administrative, and leadership capacity as well as appropriate legal and political foundations that would allow such efforts to take place.
Co-evolution, which is the third characteristic of CAS, is similar to self-organization from a procedural perspective. However, there is an essential distinction between the two. Self-organization focuses on the actions of actors within the complex system, whereas co-evolution focuses on the adaptation of a complex system to the changes in its environment (Teisman et al., 2009). In other words, self-organization happens at the micro (actor) level, while co-evolution is a macro- (system) level phenomenon. In policy implementation, co-evolution between a social system and the environment is crucial for success.
In many cases, public policies bring changes to the physical environment through building new infrastructure, shaping the natural environment, retrofitting or expanding existing facilities, etc. Furthermore, policies can be made in reaction to changes in the physical environment, such as expanding a city, or social environment, such as social acceptance of marijuana use or increased drug deaths. In such cases, the social complex system adapts its behaviors in reaction to the changes in the environment. In other words, it coevolves with its environment.
The fourth characteristic of CAS is nonlinear dynamics. Policy design and implementation often rely on the assumption of linearity between cause and effect. This reductionist approach assumes that if one variable in an equation changes, it leads to a linear change in the outcome variable. In reality, this rarely happens (Pierre & Peters, 2005; Teisman et al., 2009). Pressman and Wildawksy’s (1984) work on implementation show the nonlinear and unpredictable nature of government operations and policy execution, even in hierarchical, bureaucratic structures. In complex social systems, nonlinearity implies that interventions in a subsystem may yield particular outcomes for a specific time, but the repetition of this intervention may yield completely different results (Teisman et al., 2009). Differences in results in multiple repetitions in complex systems stem from sensitivity to the initial conditions. Even a slight change in initial conditions in a CAS can lead to dramatic changes in outcomes. A well-known example of sensitivity to the initial conditions is weather forecasting. A minor change in the input data for a weather forecasting model (e.g., a 0.001 unit increase or a decrease in one of the variables) can generate a significantly different model than the original one (Gleick, 2011). In public policy, sensitivity to initial conditions can make policy transplants from one country to another one very difficult. Cultures, legal systems, and social norms vary across countries. When a successful policy in a country is adopted by another country, the outcomes may be unpredictable in the latter location because of the differences in initial conditions in both countries.
Methodology
This article aims to explore and analyze the early Finnish experience of the adoption of DCRs from a complexity perspective. By employing the complexity lens, the article focuses on agents who are actively participating in the governance of the DCR issue, their networks and interactions, the rule structure that governs these interactions, and the internal and external (political) environment. Furthermore, the article examines system characteristics such as emergence and self-organization to identify key coalitions and oppositions (if any) of actors in the system.
To identify the fundamental elements and characteristics of the governance system for DCR adoption and implementation in Finland, the researchers reviewed the content of city council decisions, committee reports (mainly working group reports), documents created by government agencies (law enforcement, State Prosecutor, Finnish Institute for Health and Welfare), drug expert feedback (including public statements, thesis, media interviews), an ongoing study on drug consumption room policy, and newspaper articles as a source of data. Since the issue is still progressing at the local level and has not yet emerged to attract parliament-level discussions, besides the Office of the Prosecutor General and law enforcement’s statement there is no government-level statement to include and analyze. However, the data contains politicians’ statements representing various individual-level views, gathered from online content. These documents were collected from the institutions’ websites, public forums, and newspapers to identify actors, their interactions, and attitudes toward DCRs. All the official statements and reports were collected and analyzed to describe the history of DCR debate and government actions in Finland, to interpret the political context and relevance of the initiative, to identify actors, arguments, and attitudes of stakeholders toward DCRs, and finally, to reconstruct the policy process from a complexity theory perspective.
Next, researchers identified stakeholders (i.e., actors) in DCR policy, laws, and norms (i.e., rule structure), and interactions among stakeholders by reviewing the content of the documents collected (Spencer & Ritchie, 2002). To do that, the data were coded into the following categories: stakeholders (i.e., agents), rules/government actions, interactions between stakeholders, their attitudes toward DCRs, and finally, the policy environment. Finally, the coded data were analyzed to interpret the DCR governance system from a complex systems perspective. The findings from the data provide information on the emergence of DCRs as a tool for drug policy, actors involved in the development of the DCR initiative in Finland, and interactions between them. These findings also identify the components of the complex governance system for DCR adoption and implementation. The following sections in the article will present the results.
Progress of DCRs in Finland
An initiative “to explore the possibility to establish a space for supervised injecting” was filed in March 2018 by a Green Party city councilor in Helsinki (Helsingin Kaupunginvaltuusto, 2018). The initiative immediately received a lot of media attention and generated active discussion both among professionals and the general public 2 (Liitsola & Brummer-Korvenkontio, 2018). In her analysis of the web discussions on the DCR initiative, Noora Väisänen (2019) concludes that the discussions were very polarized: on the one hand PWUDs were presented in a very stereotypical and negative manner, and DCRs as an immoral practice, but on the other hand there was also an opposite discourse arguing that PWUDs are an oppressed group of people lacking human rights, and that DCRs are one solution to alleviate their difficult situation.
At first, the City of Helsinki requested opinions on the initiative from the police and the National Institute for Health and Welfare (THL) (Helsingin Kaupungin Päätökset, 2018). The view of the police was critical, and they saw the current drug law as being inconsistent with the DCR initiative (Helsinki Police Department, 2018). The statements of experts from THL were built on a summary of research evidence on DCRs, and they ended up taking a positive stance on experimenting with DCRs in Helsinki (Tammi & Brummer-Korvenkontio, 2018).
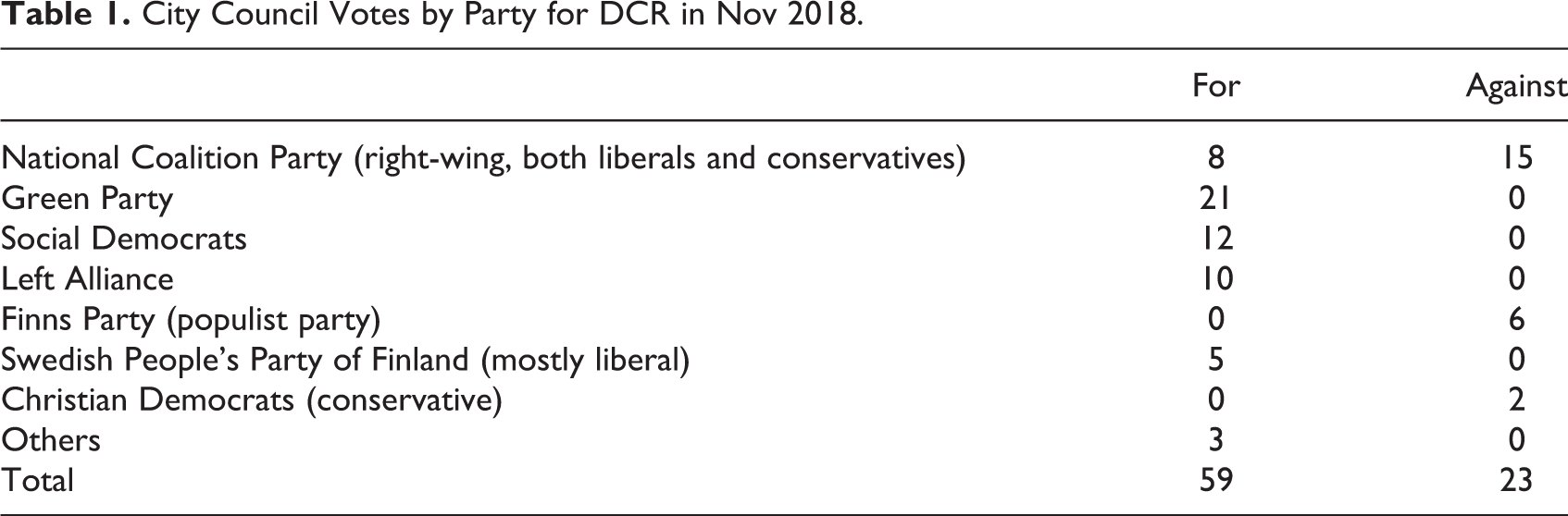
In November 2018, Helsinki City Council approved the initiative to consider the introduction of a DCR in the city (Helsingin Kaupungin Päätökset, 2018). Helsinki City Council voted—after a lengthy discussion 3 —with a clear majority for the DCRs (see Table 1 below). On the surface, the political divide was between the parties of the left and right. The divide was, in fact, was between liberal and conservative values, especially among non-left parties.
City Council Votes by Party for DCR in Nov 2018.
Next, the City of Helsinki set up a working group to produce a report on the issue: how and where could such a consumption room be established (Helsingin Kaupungin Päätökset, 2018). The report by the working group took a positive stance toward DCRs, but they also referred to the statement of the Office of the Prosecutor General that a law change would be needed (Helsingin Kaupungin Päätökset, 2019). The City Board decided in March 2019 that Helsinki would propose to the government that it would prepare to make necessary changes in the law (Municipality of Helsinki, 2018). Should this happen, the new parliament that was elected in spring 2019 will continue the discussion on DCRs; however, the Ministry of Social Affairs and Health has not displayed any activity in processing this so far. One apparent reason for that is the ongoing COVID-19 pandemic, which has stopped many, if not most, non-COVID–related development processes at the Ministry.
The development of the DCR initiative in Finland was influenced by DCR practices in other cities across the world. For example, when the first needle exchange services were established in Finland at the end of the 1990s, initially their working model was more or less copied from Glasgow, Scotland (Tammi, 2005). Continuous interactions with the external environment (i.e., cities that use DCRs) allowed the DCR initiatives in Finland to co-evolve with the cities they followed (Tammi, 2019).
The first DCR ideas in Finland originated from Barcelona, where the social and health board of Helsinki had been on a study trip, and one of the visit sites was a local DCR. Soon after the board had returned to Helsinki, there was news in the local media stating that some public toilets were closed permanently because they were being used for injecting drugs and were full of dirty paraphernalia. One of the health board members, Hannu Tuominen, then suggested to Kati Juva, a councilor and medical doctor specializing in neurology, to make a council initiative on establishing a DCR to respond to such problems. She filed the initiative in mid-March 2018.
Soon after that, in April 2018, the board of social and health affairs made another study trip, to Copenhagen, where they were given a presentation about the local DCRs. Later on, when dealing with the initiative, the DCR in Copenhagen was used as an example of good practice. For instance, in October 2018, journalists from the national broadcasting company (Yle) traveled there to film a TV reportage about the Danish DCR, including interviews with the local police who expressed positive views about the service. In the news piece based on the reportage, the heading created pressure on the Finnish authorities: “In Copenhagen, drug injecting rooms save lives in overdoses cases—the police allow the possession of drugs near the rooms. In Finland, the police in particular have opposed the creation of injecting rooms” (Yle News, 2018).
Actually, the Finnish police have not explicitly opposed the DCR initiative, even though the media initially portrayed the police as being against DCRs. What the police actually wrote when requested to provide their opinion was that: “The current legislation in force is inconsistent with the approach outlined in the initiative and, therefore, the presentation is not considered feasible by the police” (Helsinki Police Department, 2018). One repeated argument by the police was that if a citizen reported any suspicion that illegal activities were taking place at a DCR, the police would have no other choice than to raid the facility and investigate the suspected crime.
On this basis, the DCR working group then requested another opinion on the legislation, this time from the Office of the Prosecutor General. The Prosecutor General’s opinion repeated the same message as the police: the law needs to be changed if DCRs are to be established. The Prosecutor General also used Norway as a recommendable example: “The Office of the Prosecutor General is of the opinion that the experiment with injecting rooms already requires the introduction of a statutory law, for example, according to the Norwegian model, initially as a temporary pilot law” (Helsingin Kaupunki, 2019).
During the first phase of the DCR discussion, there was no evidence for direct model-taking from other cities’ DCR practices. However, DCRs in different countries and cities have been cited repeatedly. Also, the chair and four members of the local DCR working group took part in the European Harm Reduction Conference in Bucharest, where there were two special sessions arranged on DCRs (Niemi, 2018). In these sessions, presentations dealt with DCR experiences in Berlin, Frankfurt, Lisbon, Paris, and Strasbourg. In the final report of the working group, mention was made based on these presentations. All in all, international models have been present more or less consistently throughout the discussion: from the viewpoint of diffusion, they can be regarded as “secondary” policy actors.
This local attempt opens up space for discussion and policy transformation. This is not the first conflicting drug policy issue between local and central government in Finland. A similar case was experienced during the establishment of the needle exchange program in the 2000s. At that time, there were four organizations behind the policy, including A-Clinic Foundation (an NGO), the National Public Health Institute, the Health Department of Municipality of Helsinki, and the Ministry of Social Affairs and Health. When the issue became public, the representatives of these organizations defended its applicability and benefits. The advocacy group created an expert-driven network and were actively involved in the discussion to assure critics of the legal and ethical dimensions of the new policy (Tammi, 2005).
The network created a delegation that later visited the Ministry of Justice and the Ministry of Interior to explain the rationale behind the needle exchange program. Moreover, the network encouraged experts to share their thoughts, respond to critics, and write expert opinion letters to the public institutions. Both sides shared their opinions in the national media, and experts addressed the concerns of law enforcement successfully. Moreover, at the time of the debates, a National Drug Policy Committee was working to create a national drug strategy. This committee also recommended harm reduction measures in its final report (Finnish Drug Policy Committee, 1997). The network and their active involvement in the policy process gave support to the reform (Tammi, 2005).
The formation of a multi-professional advocacy network was one of the reasons for the success of the needle exchange program in Finland. It not only abolished institutional resistance but also justified the necessity of the intervention program in the public sphere. The advocacy network produced strong arguments that fulfilled the public health, security, economics, and ethical concerns and adapted to the local political reality (Tammi, 2007).
Thus, the discussion around DCRs can be seen as a second wave of harm-reduction debate in Finland. The ongoing debates about DCRs are challenging the prevailing drug-policy consensus. Compared to “only” needle exchange, DCRs also bring partial decriminalization (of drug use and possession) as a relevant topic to the discussion. DCRs do not only allow drug use but also provide professional assistance to use them more safely. During the first wave, when needle exchange was discussed, it was stressed by the advocacy network that harm reduction is not in contradiction with the drug control policy. So, the primary policy line does not need to change, even if needle exchange is allowed.
Despite the fact that drug laws and policies are designed at the national level, drug-related harm always occurs locally. The policy process related to DCRs has interestingly brought up the potentially tricky and tense relationship between local and national level policymaking. As described in this article, after receiving the opinions from the police and the Office of the Prosecutor General, the City of Helsinki proposed to the government that it should make the required law change to enable drug consumption rooms. This—presenting a substantial, if not paradigmatic, drug-policy shift from city level to national (ministerial) level—is a new setting in Finnish drug policy, which has always been entirely a matter of governmental decision making for the last 50 years. It remains to be seen how the ministries and parliament will react if the Ministry of Social Affairs and Health starts a process for law reform.
Analysis
To understand and manage the initiative for the adoption of DCRs in Finland from a CAS perspective, it is crucial to identify the components of the Finnish political system in accordance with the CAS framework in Figure 1.
Actors
Almost a dozen different actors at the local, national, and international levels of government are directly involved (see Table 2). Six of these actors were at the local level (citizens, PWUDs, City of Helsinki Municipality, Helsinki Police Department, Helsinki Working Group for DCR Implementation, Social and Health Board of Helsinki), three actors were at the national level (Ministry of Social Affairs and Health (MSAH), Prosecutor General, National Institute for Health and Welfare), one actor was both local and national (media), and one actor was international (European Harm Reduction Conference).
The Breakdown of the Finnish Political System in the DCR Policy Using the CAS Framework.
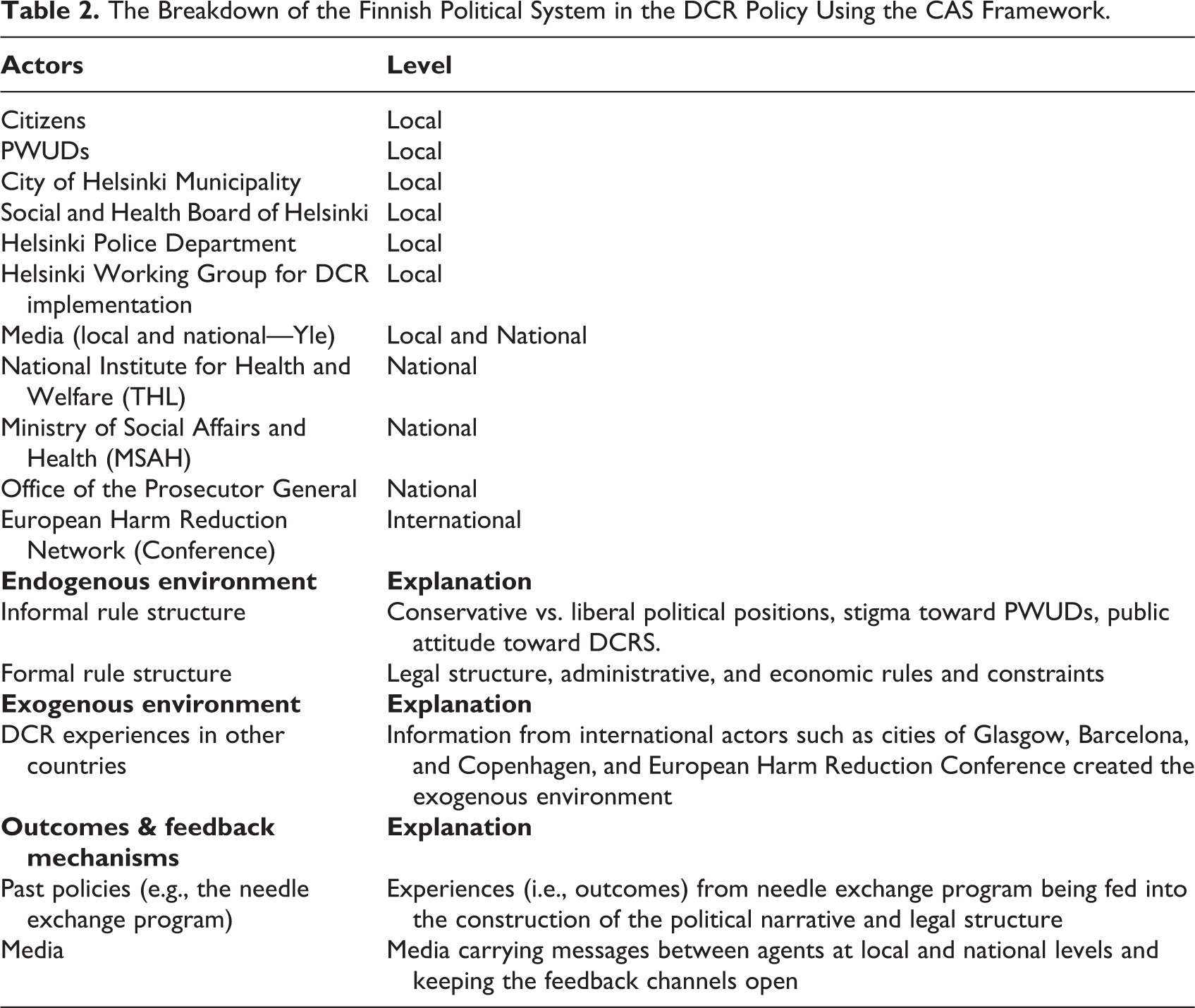
The actors in the system are positioned at three levels: local, national, and international. Local level actors have sparked the DCR policy initiative and pushed for changes at the national level. National and local actors were in constant communication, except for during 2020 due to the COVID-19 pandemic. International actors, such as the cities of Glasgow, Copenhagen, and Barcelona, were part of the exogenous environment and fed into the policymaking process in Finland with their experience. Lastly, the media played a crucial role for carrying messages and feedback between actors at all levels and facilitated the communication.
Interactions
The DCR policy initiative is a network of actors at all levels. The structure of interactions among these actors provide additional evidence regarding how the policy process was shaped. Figure 2 visualizes the network of interactions among actors at the local, national, and international level. Although the network does not capture interactions between all actors (e.g., only institutional actors were included in the graph), the sociogram shows that the City of Helsinki and the Helsinki DCR Working Group were at the center of the DCR initiative. They interacted with local, national, and international actors and played a crucial role in pushing the DCR agenda at the national level. Also, the graph shows that the media was instrumental in connecting international actors with domestic actors.
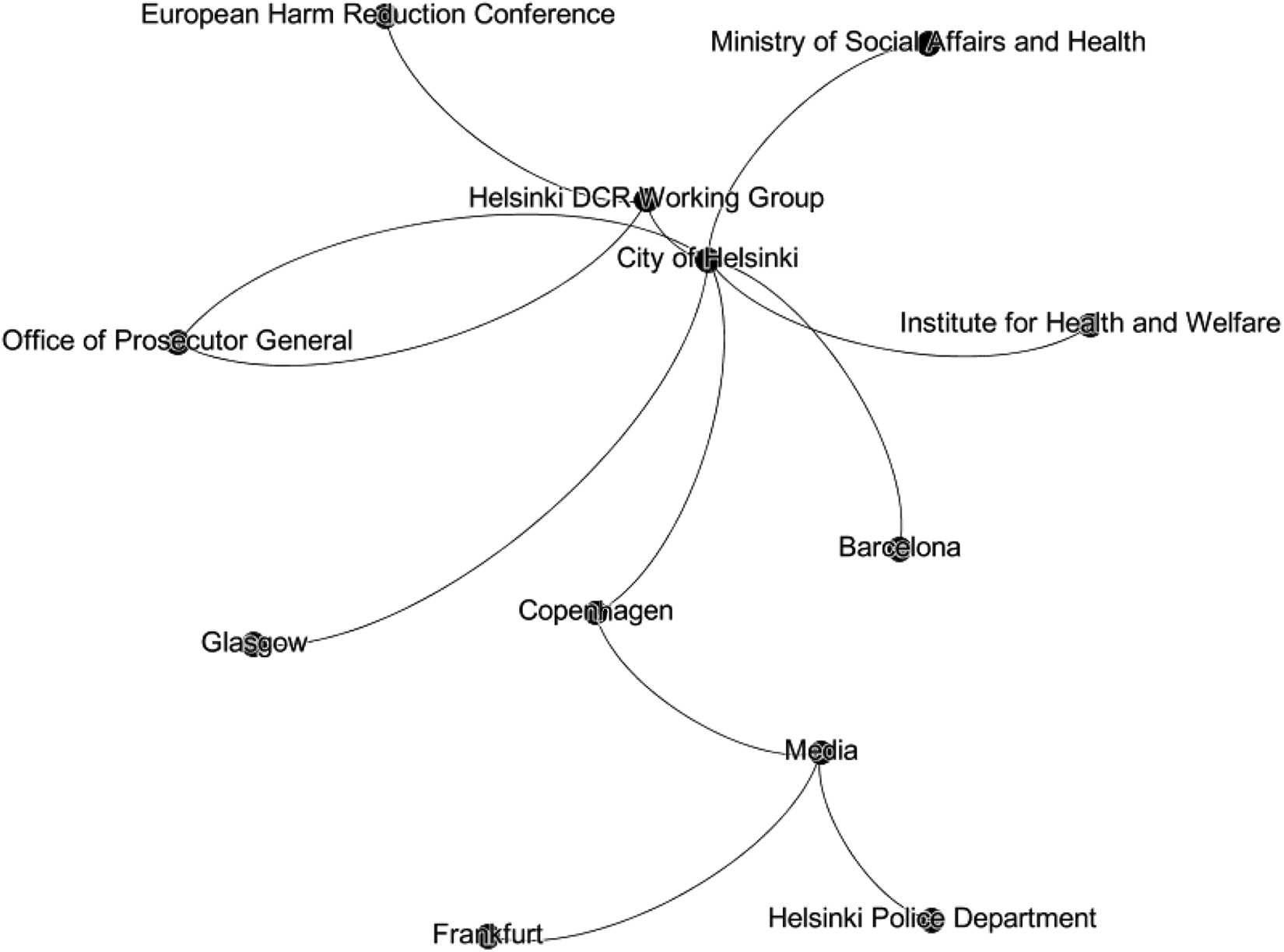
The network of interactions between actors in the DCR policy initiative.
Rule structure
Two main rule structures shaped interactions between the actors. The first is the informal rule structure that consists of political positions and social-cultural norms. Both political positions and social-cultural norms shape how DCRs are perceived by the public. Both the opponents and proponents of DCRs try to shape public perception by advancing their own normative and political agenda. In general, proponents of DCRs emphasize the improvement of the treatment system, better care of PWUDs, and reducing the number of drug-related deaths. Opponents, however, express concerns about unintended consequences, especially in terms of attitudes toward crime. The struggle between the two sides may take a significant time to settle. In France and Denmark, for example, it took more than 2 decades to find common ground for DCR establishment (Houborg, 2014; Jauffret-Roustide & Cailbault, 2018). In Finland, at the local level, the opponents and proponents of DCRs were separated mostly by liberal and conservative political positions.
The tug-of-war between the liberal and conservative political positions on Helsinki City Council resulted in a favorable attitude toward DCRs. This is partly because of the shift in public attitude toward the DCR initiative. In the last few decades, attitudes toward harm reduction programs have changed in favor of DCRs in Finland. According to the latest National Drug Survey, more than 51% of respondents were in favor of DCRs (Karjalainen et al., 2020; Yle News, 2020). This shift in public attitude toward DCRs is due to the media’s influence. The media coverage of PWUDs in Denmark and Finland have particularly enabled individuals to consider their lives in different settings, more specifically with or without DCRs.
The second rule structure that has shaped the interactions between the actors is the formal legal structure (laws, regulations, statutes, etc.) The current laws in Finland require public officials to act against drug possession and consumption. This means that if citizens complain about drug consumption in public spaces, police have no option but to respond to such calls. The push from local actors for DCRs has nudged central government to make the necessary legal structural changes. Any changes in the formal rule structure in favor of DCRs would minimize potential friction in the implementation; however, DCR policies might need to overcome other technical and administrative constraints. Establishing, staffing, and funding DCRs require stakeholders to reallocate various resources (e.g., personnel, money, and equipment) for this purpose. Such efforts require significant coordination and collaboration between actors. Furthermore, other environmental factors (e.g., the COVID-19 outbreak) may quell political capital for the adoption of DCRs and push this issue lower down on the national political agenda.
The DCR policy initiative in Finland is an ongoing systemic change that can best be understood from a CAS perspective. The breakdown of the Finnish political system in DCR adoption using the CAS framework is provided in Table 2. Although the adoption of DCRs has been a bottom-up movement, there is a tendency to explore and learn from the experiences of other cities and countries in DCR implementation. This might be a good practice from the surface; however, there are caveats regarding copying from others’ experiences. Sensitivity to initial conditions in complex systems makes it very difficult, if not impossible, to replicate a policy in different times or locations and get the same results. Systemic characteristics (actors, relationships, time, society, religion, culture, political environment, etc.) in different contexts (e.g., Barcelona and Helsinki) are likely to vary significantly. This may create positive outcomes in one context and cause chaos in another. Policymakers need to be careful about learning from others’ experiences. Instead of copying from other cities, it is vital to analyze and understand the actors, the relationships between them, rule structures governing these relationships, and the endogenous and exogenous environmental factors.
Discussion and Conclusion
Establishing DCRs is a complex policy process because reaching a consensus on such a controversial issue is a challenging task for policymakers. Although governments and public institutions generally recognize the problem of marginalized groups, public perception of and concerns regarding DCRs may deter policymakers from promptly taking the necessary steps. Moral judgment and political positions are important barriers to discussing DCRs in a health context among public officials and politicians (Jauffret-Roustide & Cailbault, 2018).
Although control over the legislature and public institutions gives politicians a substantial role in framing the policy (Jauffret-Roustide & Cailbault, 2018), central government is no longer the sole actor in policymaking. Social problems have become too complex to be handled by the efforts of a single government agency. A governance perspective may enable them to comprehend and manage complex systems (Squazzoni, 2014). There is a growing trend for replacing hierarchical and bureaucratic structures with more integrated, horizontal networks (Kapucu, 2014).
The politics of drug control is indeed a multi-actor governance process, and DCRs represent a good policy case of how various actors can collaborate and produce outcomes. The multi-centered nature of society requires negotiations and interactions between public and private institutions, community, and political actors in modern societies (Houborg, 2014). Neither government nor private actors have the capacity to solve the increasingly complex and dynamic problems of communities (Morçöl, 2014).
Awareness of differences in perception is necessary to alleviate misunderstandings, discussions, and threats to an agreement. Klijn and Koppenjan (2014) suggest that the availability and quality of the information are not necessarily effective in reducing conflict among actors. Instead, in some cases, expert involvement and establishing research commissions may deepen differences while they aim to convince others and strengthen their argument.
The attributes of legislation have different implications in reality. It is pertinent to consider legislation as a way of protecting the facility (DCR) from changing political turns and conditions by institutionalization. However, it also serves to protect the government itself from international treaties while resisting local pressure. It can be used strategically if the change is not substantial and feasible for local implementation without institutionalized solutions; maybe having a self-administrative authority, such as municipality, to run DCRs fits the context more appropriately (Zampini, 2014).
The reason for rejecting the DCR proposal in the UK in 2018 was based on concerns for law enforcement, ethical hesitations of the medical professionals, and media attitudes that has an asymmetric influence on related actors (Atkinson et al., 2019). Without political and institutional support, the issue could lead to trivial policy problems and keep out of public and media attention (Jauffret-Roustide & Cailbault, 2018). At the moment, there is neither sufficient institutional support for nor resistance to DCR policy in Finland; the current initiative is supported mainly by individual politicians, experts, and practitioners rather than by institutions and organizations. Voting in Helsinki City Council has shown that there were individual differences in some parties, but the parties who unanimously supported DCRs, namely the Social Democrats, Green Party, Left Alliance, and Swedish People’s Party of Finland, are all included in the present government of the country. So, from this perspective, it is feasible that the MSAH could prepare a proposal to the government and the parliament. However, the problem is that Helsinki City Council is much more liberal than Parliament. Although the Ministry of Social Affairs and Health has the primary responsibility of responding to and dealing with the initiative of Helsinki, the policy papers are still waiting on the ministry’s desk.
In conclusion, public officials are expected to be more cautious about contemporary drug policies. The prolongation of political and professional actors taking a position on DCRs is one of the factors that slowed down progress. A shift from the moral judgment of drug use to the judgment of transforming the risk environment requires time and knowledge (Jauffret-Roustide & Cailbault, 2018). However, timely intervention saves many lives and reduces the spread of infectious diseases. While science and expertise play a significant role in addressing concerns and leading negotiation, the media brings the case to the policy agenda and facilitates co-evaluation of the problem, fitting it to public values and norms.
DCR policies in Finland are in their infancy, and they are likely to evolve over time based on the inputs received from internal and external environmental feedback. An important environmental factor to focus on would be the role of a strong welfare state in Finland. Future research can focus on how the welfare state shapes DCR policies in Finland as well as other Nordic countries, compared with DCR policies in other countries such as Spain. Additionally, exploring the role of the media in shaping the rhetoric and DCR policy, and analyzing the intergovernmental and cross-sector networks in agenda-setting and policymaking in DCRs, would be significant contributions to the literature as future research.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: The first author disclosed receipt of the following financial support for the research: This work was supported by the Kone Foundation [grant number 201906595].