
Abstract
Guided by Andersen's behavioral health model, this study examined factors associated with preventive dental service utilization among older Korean-American residents in subsidized senior housing in Los Angeles. All participants were enrolled in Medi-Cal, allowing investigation beyond dental insurance. We focused on predisposing (age, sex, marital status, and socioeconomic status), need (perception of worsening oral health), and enabling factors (acculturation, family network, usual place for dental care, and physical health check-up). Data from 318 participants were analyzed using logistic regression. Results showed that approximately half utilized preventive dental services within the same period. Perception of worsening oral health, acculturation, having a usual place for dental care, and receiving a physical health check-up in the past year were associated with higher odds of using preventive dental services. With low rates of use among older ethnic immigrants with dental insurance, enhancing acculturation, expanding healthcare access, and promoting routine dental check-ups could improve utilization.
Keywords
Introduction
Recognizing the crucial role of oral health in overall wellbeing (American Dental Association, 2015; Institute of Medicine, 2011; U.S. Department of Health and Human Services, 2000; Wang et al., 2020), it is important to emphasize that many oral diseases are preventable and tend to accumulate over time (Peres et al., 2019; Watt et al., 2019). Routine preventive dental services, such as check-up and cleanings, are widely acknowledged as effective in reducing the incidence and severity of adverse oral health issues (Al-Nasser & Lamster, 2020; Åstrøm et al., 2014). While there have been improvements in the oral health status of the overall US population (Dye et al., 2019; Fellows et al., 2022), national reports highlight persistent racial/ethnic inequities (Institute of Medicine, 2011; Lin et al., 2019; US Department of Health Human Services, 2021). Extensive research has demonstrated that older Black and Hispanic adults often experience poorer oral health and insufficient access to preventive dental services compared to their non-Hispanic White counterparts (Gupta et al., 2018; Lin et al., 2019; Treadwell & Evans, 2019).
The understanding of oral health disparities becomes more nuanced when examining Asian Americans. English-speaking Asian Americans, captured in national surveys conducted in English and/or Spanish such as the Medical Expenditure Panel Survey and the Behavioral Risk Factor Surveillance System, demonstrate better oral health outcomes than their White counterparts (Chevarley, 2010; Stierman et al., 2021), which aligns with the model minority myth. Conversely, Asian Americans with limited English proficiency, as captured in data from community-based surveys conducted in ethnic languages, face significant language and cultural barriers to access to dental care, resulting in poorer oral health (Cruz et al., 2010; Jung et al., 2017; Shelley et al., 2011; Smith et al., 2013). This highlights the importance of adopting linguistically and culturally sensitive approaches to address oral health disparities within the Asian American community.
In some states, Medicaid healthcare coverage includes preventive dental services to tackle oral health disparities (Center for Health Care Strategies, 2019). For example, California's Medicaid program, Medi-Cal, provides coverage for preventive dental services such as examinations, x-rays, and teeth cleanings, which facilitate early detection and treatment of dental issues. However, statistics show that 61% of Medicaid enrollees eligible for preventive dental services at no cost received them (Jang et al., 2020). This emphasizes the need for additional support, beyond overcoming access barriers to dental insurance, to promote the utilization of preventive dental services. Importantly, despite their oral health vulnerability (Cruz et al., 2010; Jung et al., 2017; Shelley et al., 2011; Smith et al., 2013), the use of preventive dental services among ethnic minority Medi-Cal enrollees with limited English proficiency and the factors impacting their use remains largely unexplored.
Focusing on older Korean-American residents in subsidized senior housing who are Medi-Cal enrollees, the present study aims to investigate factors associated with their utilization of preventive dental services. Since all participants are enrolled in Medi-Cal, which provides no-cost preventive dental services, the study examines factors associated with their dental service utilization beyond dental insurance status. Koreans in the United States are known to have a high rate of limited English proficiency, and older Koreans, in particular, are predominantly foreign-born and present significant cultural barriers (Batalova & Zong, 2016; Pew Research Center, 2021). To address these challenges, we used linguistically and culturally sensitive approaches to collect data from this population in the Los Angeles area.
The current study was guided by Andersen's behavioral health model (Andersen & Newman, 1973), which has been widely used to explain the utilization of health services, including dental care with diverse populations (Andersen & Davidson, 1997). This model features three fundamental determinants: (1) predisposing factors, (2) health-related needs, and (3) enabling components. Predisposing factors represent an individual's propensity or proclivity to seek healthcare services, encompassing demographic and background characteristics (e.g., age, gender, marital status, education, and financial status). Health-related needs are primarily related to functional and other health problems, serving as the immediate motivation for seeking healthcare services. Andersen's model (Andersen & Newman, 1973) highlights the importance of an individual's perceived needs when modeling healthcare service utilization. In the context of oral health, the subjective assessment of oral health is considered the perceived need for healthcare services and is strongly associated with clinical measures (Jones et al., 2001; Wu et al., 2011).
Of particular interest in the present study was identifying culturally relevant enabling factors for preventive dental service utilization. Enabling factors are defined as the resources and knowledge that either facilitate or impede individuals’ access to healthcare services. Health insurance coverage is widely known as a critical enabler across all age groups (Lillie-Blanton & Hoffman, 2005), especially for ethnic minorities who often comprise a large portion of the uninsured population (Cohen et al., 2021). However, even when social insurance programs such as Medicaid offer preventive dental service coverage at no cost, the entitled services remain unused (Jang et al., 2020). To address this, we considered the unique sociocultural characteristics of ethnic minorities (Andersen, 1995), drawing from existing literature on healthcare utilization among both general and ethnic minority populations. Acculturation, defined as the process of cultural adaptation to a host society (Berry, 2003), emerges as a significant determinant of health service use for ethnic minority immigrants (Derose et al., 2007; Sam & Berry, 2006), particularly when they speak a different language or are not the majority in the host society. Additionally, family network can serve as a cultural enabler in promoting health service utilization among older immigrants (Diwan, 2008), especially for older Asian American adults, who often face limited English proficiency and value familism culture. Lastly, in addition to considering these sociocultural characteristics of older ethnic minority adults, we examine the importance of having a usual place for care and a regular physical health check-up as these are known to predict the utilization of preventive healthcare services across all racial/ethnic groups (Blewett et al., 2008; Deguchi et al., 2019; Lutfiyya et al., 2019; Xu, 2002).
In summary, the current study aims to investigate the contribution of predisposing (age, sex, marital status, education, and financial status), need (perception of worsening oral health), and enabling factors (acculturation, family network, usual place for dental care, and physical health check-up) to preventive dental service use in older Korean-American residents in subsidized senior housing who are enrolled in Medi-Cal.
Methods
Data
Using purposive sampling, we conducted surveys with Korean-American residents in subsidized senior housing in the greater Los Angeles area. We first identified target facilities in the area resource database we had previously established, which lists available resources and services within Asian communities in the greater Los Angeles area. With input from social service providers in these local communities, we created a short list of target facilities within a radius of 20 miles from our research site. Our data collection goal was to have a minimum sample size of 300, ensuring sufficient power for multivariate models of key contextual characteristics. We surveyed 351 participants at six facilities from April to June 2023.
At each participating facility, invitation flyers were distributed by the housing staff. The eligibility criteria were (a) self-identified Korean American; (b) aged 65 years or older; (c) residing in the participating facility; and (d) being able to read, understand, and sign a consent form. On scheduled dates, our research team visited each facility to conduct surveys. To follow the IRB-approved protocol, all participants were informed of the study's goals and procedures, and then they signed a consent form. The self-administered portion of the survey was a 10-page structured questionnaire in a paper-and-pencil format. The questionnaires were available in English and Korean, but all participants used the Korean version. At each site, bilingual and bicultural survey assistants were available for participants who needed help. The surveys were carried out in facility common areas, such as meeting rooms and cafeterias. Upon completing the self-administered survey, trained research personnel assessed participants’ cognitive function in Korean using the Mini Mental State Examination (MMSE) (Folstein et al., 1975). Of those who participated, eight individuals with severe cognitive impairment (MMSE ≤ 10) were excluded. Seven participants who either did not report their medical insurance status or were not Medi-Cal recipients were excluded. Additionally, 18 participants with missing data for measures of interest were also excluded, resulting in a final sample of 318. A comparison between the included and excluded respondents showed no significant differences in age, gender, marital status, education attainment, perceived financial status, self-rated oral health, acculturation, family network, usual place for dental care, physical health check-up, and use of preventive dental services.
Measures
Outcome Variable
An outcome measure used in the analyses was preventive dental service use. Participants were asked whether they had received a preventive dental check-up in the past 12 months. Responses were coded as yes (1) or no (0).
Exposures
Predisposing variables included age (in years), gender (0 = male, 1 = female), marital status (0 = married, 1 = not married), educational attainment (0 = > high school graduation, 1 = ≤ high school graduation), and perceived financial status (0 = ≥ adequate, 1 = inadequate). Self-rated oral health status change was used as an indicator of dental care need. Participants were asked how their oral health status has changed in the past 12 months. The responses were dichotomized (0 = same or improved, 1 = worsened).
Enabling variables encompass acculturation, a usual place for dental care, and physical health check-up. Acculturation was evaluated with a 12-item inventory (Jang et al., 2007) that included questions on language usage, media consumption, dietary habits, social relations, sense of belonging, and familiarity with the host culture. The total score could range from 0 (the lowest level of acculturation) to 36 (the highest level of acculturation). Previous research with older Korean Americans has validated this instrument (Jang et al., 2007), and the internal consistency of the scale in the present sample was high (α = .86).
Family network was measured with a subscale of the Lubben Social Network Scale 6 (LSNS-6) (Lubben et al., 2006). The items assess the number of family or relatives that the respondent (a) sees or hears from at least once a month; (b) feels at ease with, such that they can discuss private matters; and (c) feels close to, such that the participants could call on them for help. Each item was scored using a 6-point scale (0 = none to 5 = nine or more), with total scores ranging from 0 to 15. The Korean version of the LSNS-6 has been validated in prior studies with older Korean Americans (Hong et al., 2011), and a high internal consistency was found in the present sample (α = .90). Usual place for dental care was determined by asking participants if they had a regular place for dental services, with answers coded as yes (1) or no (0). Physical check-up was assessed by asking participants about their clinic visits for routine physical examinations within the past 12 months, with responses coded as yes (1) or no (0).
Analytic Strategy
Descriptive statistics were performed to assess the sample characteristics. Prior to multivariate analyses, bivariate correlations were calculated to understand the underlying associations among study variables. Multivariate logistic regression models were estimated by entering independent blocks of predictors in the following orders: (1) predisposing variables (age, sex, marital status, education, and financial status), (2) oral health need (perception of worsening oral health), and (3) enabling factors (acculturation, family network, usual place for dental care, and physical health check-up). Analyses were performed using Stata Version 16 (StataCorp LLC, College Station, TX, USA).
Results
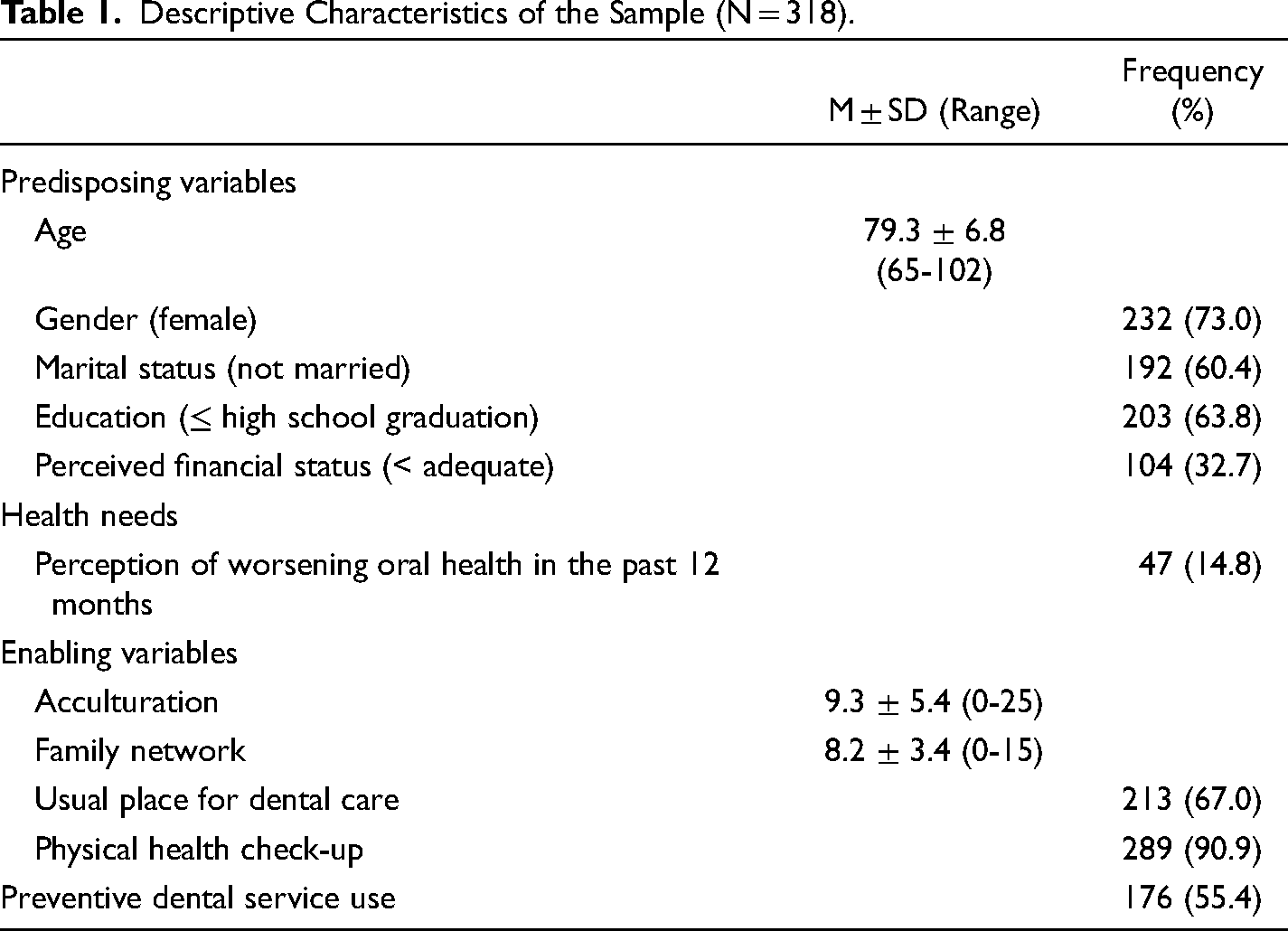
Table 1 presents the sample characteristics. The mean age of participants was 79.3 years (SD = 6.8). The majority of residents were women (73%), unmarried (60%), and lacked a high school degree (64%), with one-third of the participants perceiving their financial status as inadequate. Furthermore, one-sixth of the participants reported a decline in oral health over the past 12 months. Acculturation averaged 9.3 (SD = 5.4), ranging from 0 to 25, while the mean score for family network was 8.2 (SD = 3.4). Two-thirds of the participants reported having a usual place for dental care, and 91% of them reported regular physical check-up in the past 12 months. Additionally, approximately half of the participants received preventive dental services in the past 12 months.
Descriptive Characteristics of the Sample (N = 318).
In bivariate correlations among study variables (results presented in Table 2), preventive dental service use was found to be significantly correlated with younger age (r = −0.19), worsening oral health (r = 0.20), higher levels of acculturation (r = 0.21), having a usual place for dental care (r = 0.45), and having a physical health check-up in the past 12 months (r = 0.13). Moreover, acculturation had a negative association with age, female, and no high school graduation, while it showed a positive association with having a usual place for dental care.
Correlations Among Study Variables.
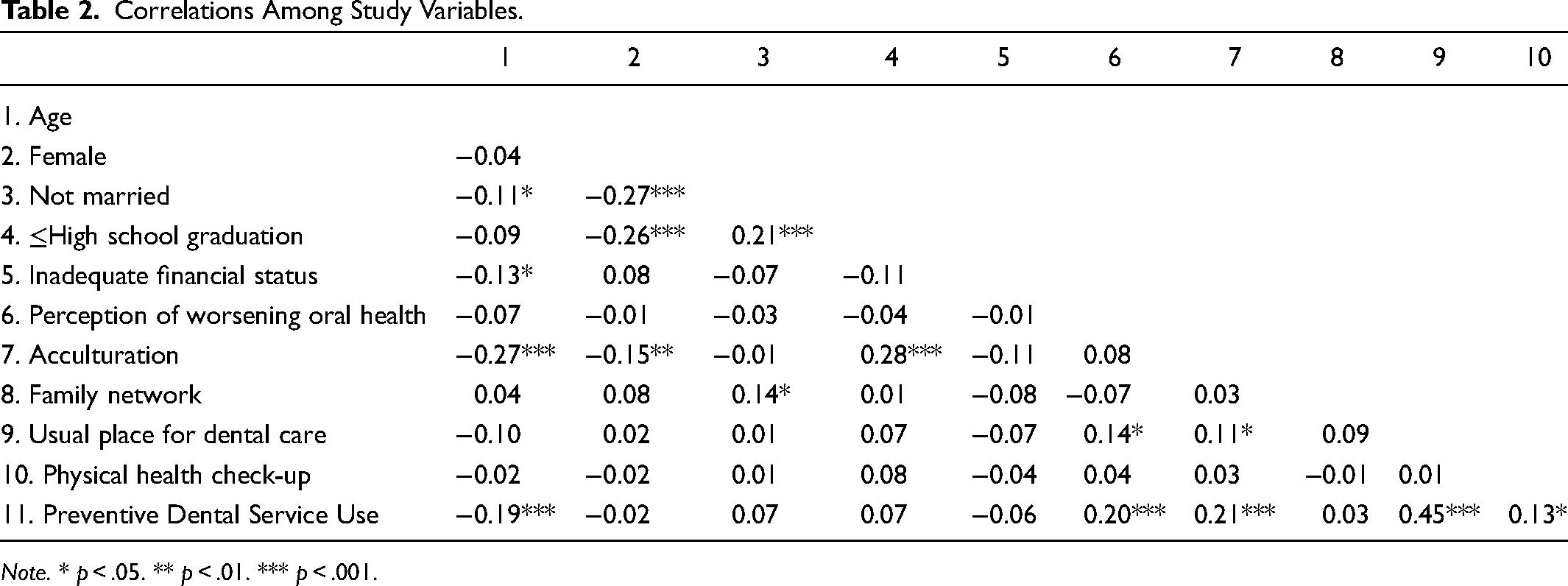
Note. * p < .05. ** p < .01. *** p < .001.
Table 3 presents the results of logistic regression models of preventive dental service use. Advanced age was associated with a decreased odds ratio (OR) of preventive dental service use in models 1 and 2 (OR = 0.94, 95% confidence interval [CI] = 0.91, 0.98), but became insignificant after including enabling factors in model 3 (OR = 0.96, 95% CI = 0.92, 1.00). Perception of worsening oral health in the past 12 months was associated with an increased OR of preventive dental service use (OR = 2.49, 95% CI = 1.10, 5.64). Among enabling factors, acculturation and having a usual place for dental care were associated with an increased OR of preventive dental service use (acculturation: OR = 1.07, 95% CI = 1.01, 1.13; usual place for dental care: OR = 7.41, 95% CI = 4.18, 13.14). Older adults who received a physical health check-up within the past 12 months were 2.9 times more likely to utilize preventive dental services than those who did not receive a physical health check-up (OR = 2.86, 95% CI = 1.16, 7.04).
Logistic Regression Models of Preventive Dental Service Use.
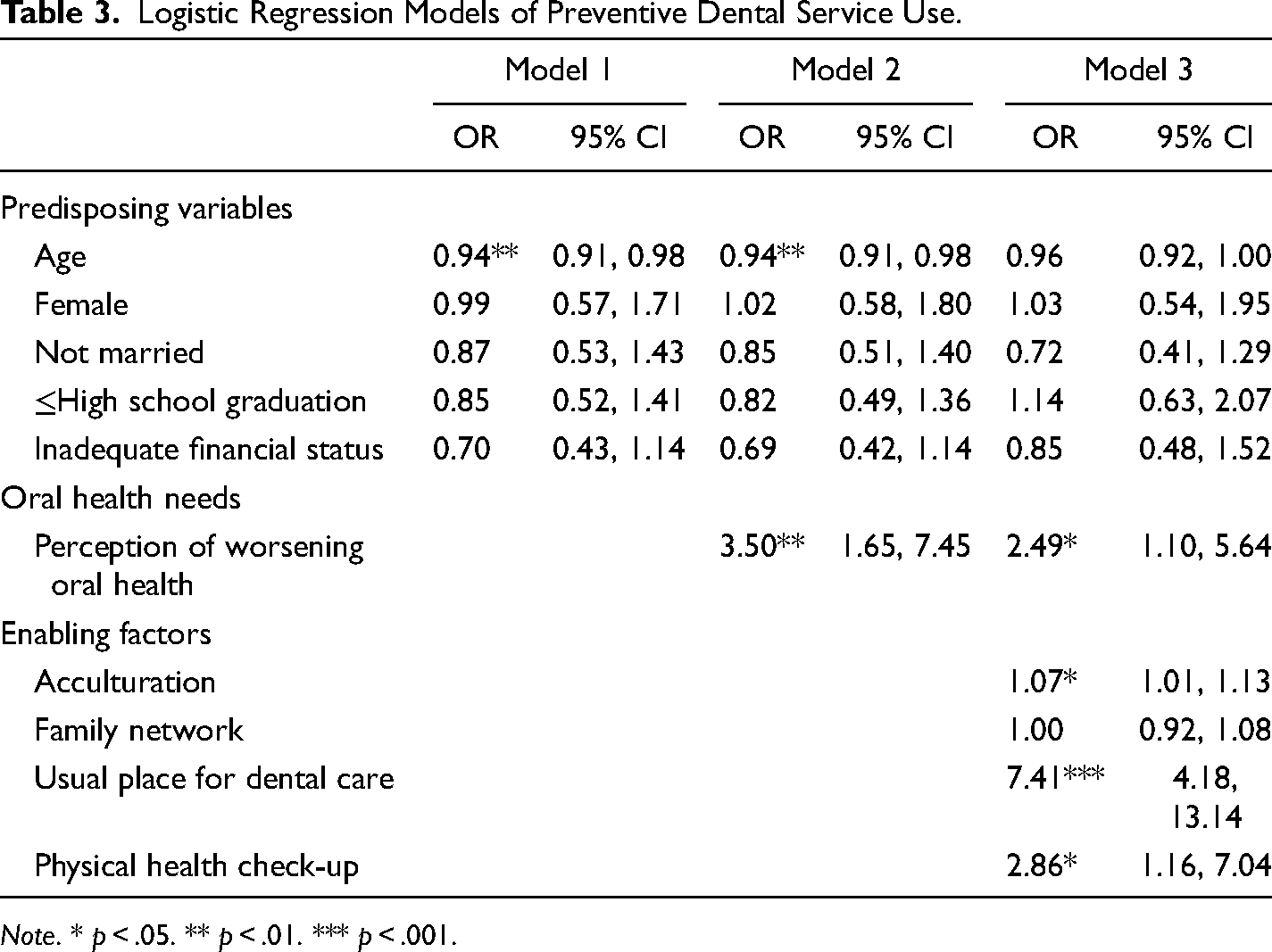
Note. * p < .05. ** p < .01. *** p < .001.
Discussion
In response to persistent oral health disparities (Institute of Medicine, 2011; Lin et al., 2019; US Department of Health Human Services, 2021), this study aims to enhance the understanding of preventive dental service utilization among older ethnic minority Medi-Cal enrollees with limited English proficiency (Cruz et al., 2010; Jung et al., 2017; Shelley et al., 2011; Smith et al., 2013). This study assessed the current status of preventive dental service use among older Korean-American residents in subsidized senior housing with Medi-Cal coverage and explored predisposing, needs, and enabling factors associated with their utilization, guided by the Andersen's behavioral health model (Andersen & Newman, 1973).
The descriptive analyses conducted on the sample revealed significant oral health needs, as approximately 45% of the participants did not utilize any preventive dental care services in the past 12 months. This statistic closely aligns with the findings from a national sample of Medicaid-enrolled older adults, indicating a consistent pattern of service under-utilization in the broader Medicaid-enrolled older adults nationwide (Khouja et al., 2020). Such consistency strengthens the validity and relevance of the study's findings within the broader context of demographic trends in dental care utilization, emphasizing the importance of addressing oral health needs in this group.
In the multivariate analyses, among predisposing factors, age initially emerged as a significant predisposing variable; however, its significance disappeared when enabling factors were included in the model. This indicates that enablers such as acculturation, having a regular dental care provider, and receiving a regular physical health check-up—more common among younger older adults—may play a more significant role in preventive dental service utilization or could mediate the association between younger ages and a higher likelihood of utilizing preventive dental services. Notably, a statistically significant negative correlation between age and enabling factors emerged in bivariate analyses, indicating that acculturation, usual place for dental care, and physical check-up—considered age-related components— are noteworthy targets. Additionally, we tested age as a potential moderator in the relationship between enabling factors and preventive dental care use—however, the analysis did not find significant moderating effects. Furthermore, contrary to existing research showing a positive association between socioeconomic status and dental service use (Palència et al., 2014; Pavi et al., 2010), our multivariate analysis did not find a significant association between socioeconomic status (i.e., education level and financial status) and preventive dental service use. This insignificant association may be attributed to our sample comprising with comparable socioeconomic backgrounds, specifically low-socioeconomic Medicaid enrollees.
The perception of worsening oral health over the past 12 months was found to be significantly associated with a higher likelihood of using preventive dental services. It is important to note that our analysis focused on “recent changes” in oral health needs rather than the traditional measure of perceived oral health status (Jones et al., 2001; Wu et al., 2011). As a sensitivity analysis, substituting the measure of perceived oral health changes with perceived oral health status, commonly used in past literature, revealed nonsignificance at alpha 0.05 (p-value = 0.186; results not shown). Our results indicate that individuals seek dental care primarily when experiencing symptoms of discomfort or other oral health concerns.
In an effort to explore a culturally sensitive intervening strategy for promoting the utilization of preventive dental services among older ethnic minority adults, we incorporated both conventional and culturally relevant enabling factors into the model. As observed in previous studies (Berry, 2003; Derose et al., 2007; Sam & Berry, 2006), acculturation was associated with the use of preventive dental services. Focusing on older Korean-American adults living in the greater Los Angeles area, California, known as the largest Korean-American community and for having an abundant Korean-speaking dental care resources, our study sheds light on the significance of acculturation even in such resource-rich area, highlighting its relevance for individuals in other regions.
We also identified having a regular dental care provider as the most influential enabling factor, consistent with previous literature (Blewett et al., 2008; Deguchi et al., 2019; Xu, 2002). Dentist–patient relationships significantly impact patients’ trust and satisfaction with dental care, consequently influencing oral health outcomes (Song et al., 2020a, 2020b). The presence of a familiar dental provider is crucial for facilitating access to preventive dental services. This may be particularly important for ethnic immigrants, as limited English proficiency can hinder them from establishing a regular place for care (Gulati & Hur, 2022; Pippins et al., 2007). Given that one-third of respondents lack a regular dental care provider, it is important to examine the factors associated with having such a provider as an intervention measure to encourage preventive dental service utilization. Additionally, the experience of undergoing a physical health check-up was associated with a higher likelihood of preventive dental service use (Lutfiyya et al., 2019). Considering that the majority of respondents (91%) have undergone a physical health check-up, this presents a potential intervention opportunity to link patients receiving a physical health check-up with preventive dental care.
Family support and network, in general, play a crucial role in healthcare utilization among older ethnic minorities (Diwan, 2008); however, our study did not find a significant association with dental service use. This may be influenced by a combination of cultural, financial, and structural factors specific to oral healthcare. For example, structural barriers, such as geographic proximity to dental providers or availability of culturally competent services, might outweigh the influence of family support. Further research into these comprehensive factors could help inform targeted interventions to improve dental service utilization and promote equitable access to oral healthcare for older ethnic minorities.
The present study has several limitations. First, although the recruitment strategy aimed to include individuals who were culturally and linguistically isolated by sampling across multiple locations, the sample is limited to older Korean-Americans living in assisted living facilities—thus, it is not nationally representative of older Korean Americans covered by Medicaid, limiting the generalizability of the findings. The cross-sectional design also restricts the ability to establish causal relationships between variables. Future research should include more diverse and nationally representative samples, including older Korean Americans in various care settings and communities, and consider longitudinal designs to better understand causal relationships. Second, because the study relied on self-reported measures of oral health needs, the results may not fully capture the individuals’ objective oral health status. Objective measures of oral health may include clinical oral examinations, including assessments of decayed, missing, and restored teeth, as well as mouth dryness and gum condition. Also, the use of a single-item self-reported measure of oral health may not be sufficient to capture the complexity of oral health status. Future research should include multiple measures for a more comprehensive assessment of oral health status. Additionally, detailed information on preventive dental service use, such as ethnic and linguistic concordance with care providers and levels of satisfaction with the services, was not included in the study. Furthermore, participants’ understanding of preventive dental check-up may have varied. While our survey aimed to capture routine dental care, such as cleanings and radiographs, we acknowledge the possibility that some participants may have interpreted preventive care more broadly, including treatment-seeking behaviors. Future studies should incorporate this information to provide a more nuanced understanding of dental service utilization patterns among older Korean Americans. Lastly, future studies should examine other factors influencing oral health needs and dental service utilization, such as dental fear and anxiety, oral health literacy, cultural values and beliefs, personal health choices, psychosocial resources, and community/environmental characteristics. Understanding the interplay of these factors could inform interventions to improve oral health outcomes among older Korean Americans and other culturally diverse populations.
Despite these limitations, the present study enhances our understanding of dental service needs beyond dental insurance among older ethnic immigrants with language barriers and identified factors associated with their service use. The findings revealed low rates of preventive dental service utilization among older ethnic immigrants, highlighting the need for additional support to promote the use of preventive dental services. Effective interventions should focus on improving acculturation and healthcare accessibility, such as establishing regular dental care providers. Additionally, encouraging those who routinely have a physical health check-up to also have a routine dental check-up could be beneficial.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project was supported by a grant from the National Institute of Dental and Craniofacial Research (R21DE029579, PI: Yuri Jang, Ph.D.).
Ethics Approval
This project was approved by the University of Southern California Institutional Review Board.