
Abstract
In prospective studies on religiousness and depressive symptoms, it remains unclear whether religiousness is a predictor or parallels the fluctuating course of depressive symptoms. The current study focuses on several affective aspects of religiousness in their associations over time with late life depressive symptoms. As part of the population-based Longitudinal Aging Study Amsterdam, a subsample of 222 respondents (mean age 76.3 years) completed up to three postal questionnaires with 3-year intervals. The questionnaires included the Center for Epidemiologic Studies Depression scale and subscales of the Questionnaire God Representations and the Brief Religious Coping scale. Analyses were performed using mixed model analysis and logistic regression. Positive feelings toward God were associated with fewer depressive symptoms over time. Anxiety toward God, discontent about God, and negative religious coping predicted more depressive symptoms over time (between-subject effects) but also tended to run parallel to the course of depressive symptoms (within-subject effects).
Introduction
In the study of associations between depression and religiousness, at least three mechanisms can be assumed. First, religiousness generally protects against depressive symptoms, providing hope, comfort, and support (Braam & Koenig, 2019; Koenig et al., 2024). Second, worries and struggles surrounding religious questions or disappointments may lead to depression (Braam & Koenig, 2019; Koenig et al., 2024). Third, depression may deprive people of their familiar, comforting feelings with respect to religion (Jaspers, 1973; Nieuw Amerongen-Meeuse et al., 2024). Especially when people feel connected to their religion throughout their lives, all of these mechanisms may be at work. The current study aims to add to the empirical body of knowledge by describing patterns of associations over time between several positive and negative aspects of religiousness and depressive symptoms in older people.
Most scholars consider religiousness as a multidimensional concept (Bergin, 1983). Individual, social, and cultural attitudes toward religion have cognitive, affective, motivational, and behavioral dimensions (Bodling et al., 2013; Hayward, 2021; McClintock et al., 2016). In survey research in the social and medical sciences, the cognitive, behavioral, and motivational dimensions generally receive attention, and the empirical evidence on fairly consistent patterns of associations between these dimensions and aspects of mental health is gradually growing (e.g., Koenig et al., 2024; Rosmarin & Leidl, 2020). The empirical evidence of the affective dimension, however, has received less attention and is less unambiguous.
Affective or emotional aspects of religiousness can be conceived of as emotion-focused religious coping (Pargament et al., 1998) or as originating from religious attachment styles (secure, anxious, or avoidant; Kirkpatrick, 2005). A positive attachment, for example, is reflected by the perception of a positive or supportive image of God or the deity (Rizzuto, 1979). Here, a perceived sense of mutual trust is a likely core element of positive emotion toward God. In addition, other aspects of religiousness reflect a troubled relationship with the deity or religious community, as can be apparent from “religious struggles” (Pargament et al., 1998). For example, religious struggles may reflect anxious or detached attachment styles, such as those involving pessimistic interpretations about punishment or being abandoned by God, representing so-called “negative religious coping.” A meta-analysis of cross-sectional studies indicates that measures on God representations show more prominent associations with well-being or mental distress than measures that assess general aspects of religiousness, such as church attendance or salience of religion (Stulp et al., 2019).
Religiousness has not only been identified as a cross-sectional correlate but also as a possible determinant of depressive symptoms and depression over time (Braam et al., 1997; Braam & Koenig, 2019; Koenig et al., 2024; Paz Mosqueiro et al., 2021). Associations between the aspects of the affective dimension of religiousness with depression can follow different pathways. Positive aspects of religiousness may act as protective factors against the onset of depression, and negative aspects may contribute to vulnerability to the onset of depression. Similarly, the course of depression over time may be affected by positive aspects of religiousness (earlier remission) or negative aspects (prolonged course) (Braam & Koenig, 2019). Other pathways can be conceived of as well (e.g., Pargament & Lomax, 2013), such as that religious affect and depressive symptoms simply overlap. For example, depression may deplete people from positive religious experiences and possibly even deprive people of a sense of religious trust. Induced or increased religious struggles could therefore be perceived of as expression of depression.
In a previous study among older adults (Braam et al., 2014), we described how persistent late-life depressive symptoms showed prominent associations with negative feelings toward God and negative religious coping. In that study, we used longitudinal data on depression, but only the last assessment cycle included aspects of God representation and religious coping, so that a change in God representation over time could not be modeled. For the current study, two more assessments have been added, including measures on feelings toward God and religious coping. This facilitates that both changes in levels of depressive symptoms and changes in specific affective aspects of religiousness could be observed and modeled. As far as the authors know, this has hardly or never been done in samples of older people. From a clinical point of view, the findings may help to substantiate information for clients with depression when experiencing religious struggle. For example, negative affective aspects of religiousness might tend to co-occur with depression and are possibly to a certain extent only temporal, decreasing during the recovery from depression.
The current study aims to describe how positive and negative aspects of religiousness, especially pertaining to various feelings toward God and religious coping, are related to late life depressive symptoms over a 6-year period. The following research questions are addressed:
Do positive aspects of religiousness show associations with decrease, emergence, or persistence of depressive symptoms over time? Do positive aspects of religiousness parallel concurrent lower levels of depressive symptoms over time? Do negative aspects of religiousness show associations with increase, emergence, or persistence of depressive symptoms? Do negative aspects of religiousness parallel concurrent higher levels of depressive symptoms over time?
Methods
Sample
The present study used data from the Longitudinal Aging Study Amsterdam (LASA), an interdisciplinary study on predictors and consequences of changes in autonomy and well-being in an aging population (Huisman et al., 2011). LASA is based on a random population-based sample of adults between the ages of 55 and 85, stratified for age, sex, and expected mortality 5 years into the study. Registries of eleven municipalities in the west of the Netherlands (mostly secularized, including Amsterdam), the northeast (predominantly Protestant), and the south (predominantly Roman Catholic) provided the sampling frame. Respondents were visited at home by specially trained and supervised lay-interviewers. Prior to the study, informed consent was obtained from all respondents. The procedures were approved by the Ethical Committee of the VU University in Amsterdam.
The number of respondents to the LASA baseline interview in 1992/1993 was 3,107. Every three or 4 years, all respondents in the baseline assessment were approached at follow-up assessments, in which generally, the same instruments and procedures were applied. Sampling details have been described in detail elsewhere (Deeg et al., 2002; Huisman et al., 2011).
In 2005, an additional postal questionnaire with questionnaires on God representations and religious coping was administered (Braam et al., 2014). This first, additional, measurement, served as “baseline” (T0y) for the present study. The subsample consisted of two groups: First, all respondents with high levels of depressive symptoms at one or more of the four previous LASA assessments between 1992/1993 and 2001/2002 (n = 306); second, a random selection of respondents without high levels of depressive symptoms at one of the previous four LASA assessment waves between 1992/1993 and 2001/2002 (n = 190, a sufficient number according to power calculations). The questionnaire was not administered to the full LASA sample, to reduce the risk of overdemanding respondents and to secure their continued cooperation in LASA. The response (N = 371) was 75%, with 354 respondents having complete data on depressive symptoms and on at least one of the scales on feelings about God or religious coping.
In 2008 (T3y), 223 respondents filled in the second questionnaire, and in 2011 (T6y), 163 respondents filled in the third questionnaire. Reasons for nonresponse were not collected, but information on the respondent status at the LASA assessment wave in 2011/2012 shows that 245 of the 354 respondents who had valid data on the first postal questionnaire in 2005 would still have been eligible in 2011. Meanwhile, 90 respondents had died, eleven refused, and eight were ineligible. The net response for the three questionnaires was therefore 67%.
In the analyses, all respondents in 2005 (T0y) were included if they had at least one follow-up depression assessment (N = 222), either after 3 years in 2008 (T3y) or after 6 years in 2011 (T6y). Depending on the concepts analyzed, the numbers of respondents included in the analyses varied. The sample size provided sufficient statistical power (0.8) to detect at least medium-sized associations between continuous variables (required N = 222). The significance level was adapted to alpha = .025 because of multiple comparisons, as five independent variables (five affective aspects of religiousness) were separately evaluated in their associations with depression.
Measures
Depressive Symptoms
Depressive symptoms were assessed using the Center for Epidemiologic Studies Depression Scale (CES-D) (Radloff, 1977). The CES-D was designed for use in population-based studies and has also been applied in gerontological and geriatric studies, showing consistently appropriate validity in screening for late life depression (Park & Lee, 2021). The CES-D consists of 20 items about depressive symptoms in the past week, with response categories ranging from 0 (“rarely or never”) to 3 (“mostly or always”). Four items about positive affect are reverse coded. All LASA face-to-face interviews included the CES-D, as did the postal questionnaires administered in 2005, 2008, and 2011. Internal consistency amounted to Cronbach α = .88 (T0y). The range of scale scores of the CES-D is 0–60.
CES-D scores of 16 or higher generally indicate clinically relevant depressive symptoms: For this cut-off criterion, high sensitivity (100%) and satisfactory specificity (88%) for late life major depression in the past month have been reported (Beekman et al., 1997). With respect to using the dichotomized scores in the present longitudinal study, emergence of depression was defined as a CES-D score < 16 at T0y and CES-D ≥ 16 at follow-up (T3y or T6y) with at least a five-point CES-D score increase (half a standard deviation), to rule out trivial changes, as have been applied in previous studies (Beekman et al., 2002; Braam et al., 1997; Phifer & Murrell, 1986). In turn, the persistence of depression was defined as an initial CES-D score ≥ 16, remaining ≥ 16 at T3y or T6y, or with less than five points, CES-D score decreases if a score fell below 16.
Feelings About God and Religious Coping
The Questionnaire God Representations (QGR) comprises a set of scales developed by Murken et al. (2011). From a psychodynamic point of view, the QGR aims to probe into object-relational representations, following Rizzuto's theory on the object-relational potential of “God images” (1979). Murken distinguishes two dimensions: feelings about God and the perception of God's actions. Schaap-Jonker et al. (2002; 2008) have translated the QGR into Dutch and arrived at a 33-item version. Schaap-Jonker and Vrijmoeth (2024) took care of further development of the six QGR subscales and arrived at a shorter 17-item version (cf. Sharp et al., 2021). They described adequate psychometric properties for both the total version and the 17-item version. Furthermore, principal component analyses resulted again in the three-factor solution, both in the general population and in a population of clients in mental health care. Structural validity appeared in their comprehensive validation study from associations of intermediate size (in the expected directions) between the subscales scores and measures on hope/meaning in life, identity, vitality, and psychopathology (Schaap-Jonker & Vrijmoeth, 2024). The current study focuses on the emotional aspects of religiousness and therefore only included the three subscales on feelings about God in the three assessments. The QGR items consist of brief statements (e.g., “When I think of God I experience … thankfulness”). Response categories ranged from 0 (“entirely not”) to 4 (“very strongly”). The three QGR subscales on feelings toward God comprise the following: “positive feelings toward God” (5 items: thankfulness, closeness, trust, security, and love; Cronbach α = .97); “anxiety toward God” (5 items: fear of being not good enough, fear of being punished, uncertainty, guilt, and shame‡; α = .83); and “discontent about God” (i.e., “feeling wronged by God”; 7 items: disappointment, anger, oppression‡, loneliness‡, need of more freedom‡, dissatisfaction, and desolation‡; α = .86). The items marked with “‡” belong to a larger, 52-item QGR version (e.g., Braam et al., 2008a) but were not part of the shorter standard, 33-item version (Schaap-Jonker et al., 2008; Schaap-Jonker & Vrijmoeth, 2024), as this has been developed later.
Religious coping was assessed with a ten-item version of the Brief RCOPE (Pargament, 1999). This ten-item version was slightly adapted and used for the current study, since it is considered to be less culture-sensitive than the fourteen-item version (Pargament et al., 2004). Response categories ranged from 0 (never) to 3 (very often). The positive religious coping scale included five items in the current study (concise content: work together with God as partners, look to God for strength, support and guidance, try to find lesson from God, confess sins, and focus on religion to stop worrying‡; Cronbach α = .94). The negative religious coping scale has four items (concise content: wonder whether God has abandoned me, question whether God exists, express anger at God, and question God's love for me‡; α = .73). The two items marked with “‡” were derived from the fourteen-item version of the Brief RCOPE and replaced two items with weaker factor loadings. One item of the negative coping subscale pertains to punishment appraisal (God's way of punishing for sins or lack of spirituality). However, in a pilot study among older people in The Netherlands (Braam et al., 2008a), this item did not load on the dimension of negative coping. Instead, it had a modest loading on the positive coping scale (Braam et al., 2010) and was not further used in the current study.
To substantiate the scale validity, a principal component analysis was carried out on a series of eleven scales on God representation and religious coping in the pilot study mentioned above (Braam et al., 2008a). These eleven scales included the six QGI subscales, two other scales on “God representation,” as well as the two brief RCOPE subscales on positive and negative religious coping. Three factors were identified: one covered the subscales with positive perceptions, one with critical perceptions, and one with perceptions about punishment. The RCOPE subscale on positive religious coping had a high factor loading (0.79) on the “positive perceptions” factor. Here, the QGR subscale on positive feelings toward God had the highest loading, 0.90. The subscale on negative religious coping had a high factor loading on the “critical perceptions” factor (0.63), together with the QGR subscales on “discontent about God” (loading 0.84), and “anxiety toward God” (loading 0.66).
Demographics and Other Measures on Religiousness
Age, sex, years of education, and marital status were included as demographic variables. With respect to other measures of religiousness, three items were included to describe the present Dutch sample. Assessed at the last LASA assessment prior to T0y (2001/2002) were religious affiliation (nonaffiliated, Protestant - mostly mainline Reformed/Calvinist - and Roman Catholic) and frequency of church attendance (five response categories, ranging between 1 “never/yearly or less” and 5 “weekly of more”). Frequency of prayer was included in the postal questionnaire in 2005, with eight response categories, ranging between 0 “never” and 7 “more than once a day.”
Statistics
First, descriptive statistics were computed for the demographic characteristics, the measures on religiousness, the affective religiousness variables (i.e., the three QGR subscales and Positive and Negative Brief RCOPE scales), and depressive symptoms. All variables were sufficiently normally distributed (acceptable to excellent skewness and kurtosis). Second, Pearson correlations were computed for the five affective religiousness variables and depressive symptoms at T0y.
Third, to study the associations between aspects of religiousness and depressive symptoms over time, mixed model analyses were applied. Because the independent (religiousness) variables (i.e., the three QGR subscales and Positive and Negative Brief RCOPE scales) and dependent variable (depressive symptoms scores) were time-dependent, it was possible to distinguish between within-subject effects and between-subject effects. This was done by performing both regular mixed model analyses and hybrid models, both using maximum likelihood estimation, with the latter including both the individual mean score and a deviation score as independent variables (Twisk & Vente, 2019). Although mixed model coefficients generally are expressed as unstandardized regression coefficients (B), also standardized coefficients (β) were computed to facilitate comparison between the types of religiousness variables. Separate analyses were carried out for each affective religiousness variable. Each analysis was adjusted for age and sex, because the initial sampling was weighted according to age strata by sex due to expected mortality.
For each religiousness measure, figures illustrate the longitudinal course patterns. These figures were based on marginal mean scores on the CES-D, adjusted for age and sex, computed by analyses of variance, which also served as post hoc tests. For each of the five religiousness subscales (QGR and RCOPE), the highest tertile was considered “high.” Six patterns were defined: (1) persistent-low scores (i.e., lowest two tertiles), (2) downward change (decreasing scores, no longer high), (3) upward change (increasing toward the highest tertile), (4) persistent-high scores, (5) low–high–low pattern, and (6) high–low–high pattern. The last two groups turned out to be very small but may be theoretically relevant. Two types of diagrams emerged: for two assessments T0y and T3y (N is about 222) and for all three assessments T0y, T3y, and T6y (complete scores, N is around 150). When specific differences in CES-D scores between groups are described, the comparison was made in post hoc tests with the “persistent-low” category of the religiousness subscale as reference group.
Fourth, a series of logistic regression analyses were applied to examine whether the religiousness measures predicted the emergence or persistence of high CES-D scores, indicative of clinically relevant depression. Finally, to compare the results with other studies (e.g., Li et al., 2016), the analyses were also carried out for two other measures of religiousness at T0: frequency of prayer and religious attendance. Regular mixed models were used for predicting depressive symptoms over time, and logistic regression analyses were used to predict the emergence or persistence of high depressive symptom scores. Analyses were performed using SPSS version 28.
Results
Characteristics of the Sample
As shown in Table 1, about two-thirds of the respondents were female. The average age in 2005 (T0y) was 76.3 years (standard deviation 6.3). Forty percent attended church on a weekly basis, and 58% of the sample prayed at least daily. One quarter of the sample was not or no longer affiliated to a church. The mean depressive symptom scores (CES-D) at T0y, T3y, and T6y varied between 14.6 and 14.9, with standard deviations varying between 7.4 and 8.7. The percentage of those who had a score of 16 and higher was between 40% and 46%. For those with initially low CES-D scores at T0y, the rate of emergent depression (CES-D ≥ 16, with an increase of five points or more) was 24%. For those with initially high CES-D scores, the rate of persistent depression (CES-D ≥ 16 or less than five points decrease beyond 16) was 71%.
Characteristics of the Sample, Including Respondents at Baseline and all Respondents With At Least One Follow-up Assessment After 3 Years or 6 Years (N = 222).
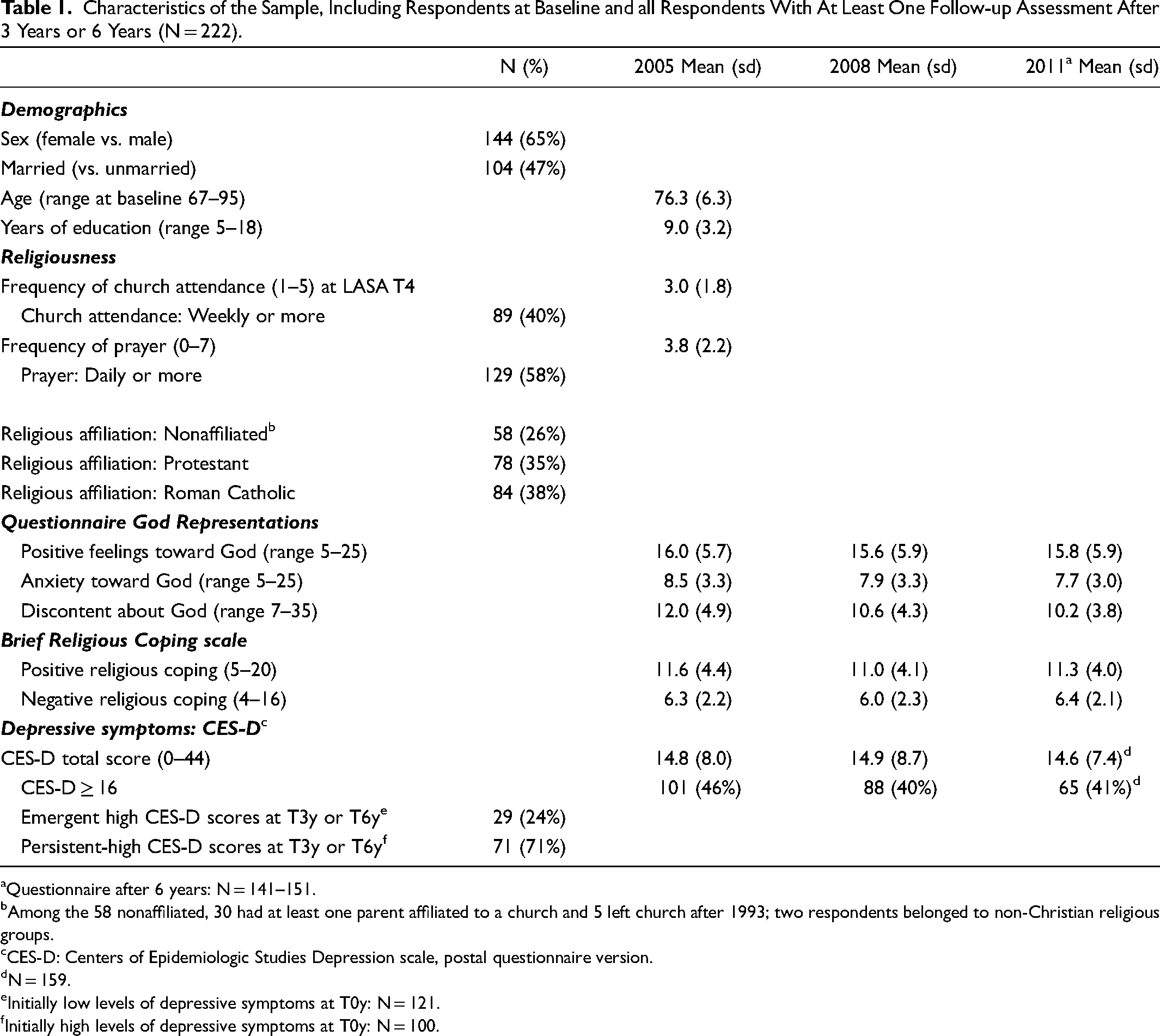
Questionnaire after 6 years: N = 141–151.
Among the 58 nonaffiliated, 30 had at least one parent affiliated to a church and 5 left church after 1993; two respondents belonged to non-Christian religious groups.
CES-D: Centers of Epidemiologic Studies Depression scale, postal questionnaire version.
N = 159.
Initially low levels of depressive symptoms at T0y: N = 121.
Initially high levels of depressive symptoms at T0y: N = 100.
The QGR and RCOPE subscales show several significant intercorrelations (shown for T0y in Table 2). The strongest is between “positive feelings toward God” and positive religious coping (rPearson = .82, p < .001). “Discontent about God” correlated positively with negative religious coping (r = .52, p < .001) and with “anxiety toward God” (r = .35, p < .001). “Anxiety toward God” had a weak, positive correlation with “positive feelings toward God” (r = .16, p = .020) and also with positive religious coping (r = .23, p < .001). “Positive feelings to God” had a weak association with lower depressive symptom scores (r = −.22, p < .001), whereas “anxiety toward God” (r = .30; p < .001), “discontent about God” (r = .41, p < .001), and negative religious coping (r = .25; p < .001) correlated significantly with higher CES-D scores.
Correlations at T0y (“Baseline”) Between Three Subscales of the Questionnaire God Representations (QGR), Positive and Negative Brief RCOPE Scores and Depressive Symptoms (CES-D).
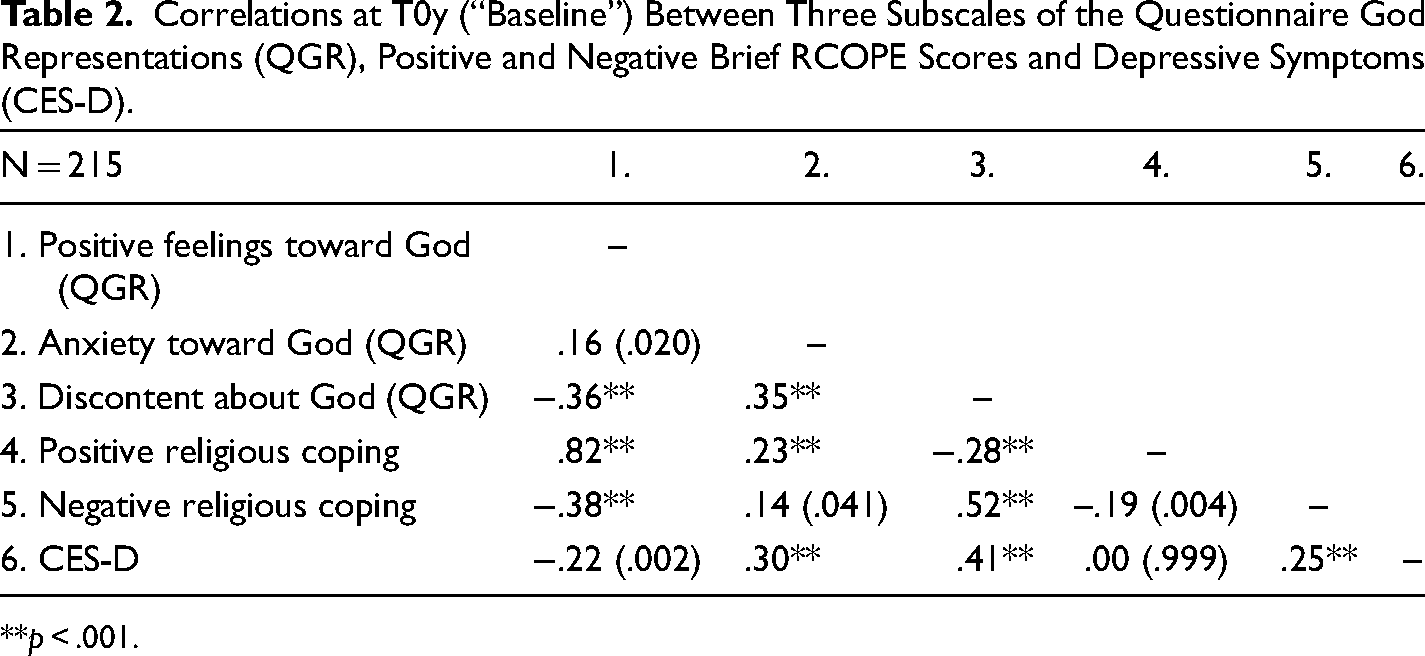
**p < .001.
Positive Aspects of Religiousness and Depressive Symptoms: Longitudinal Analyses
The “positive feelings toward God” scores (as independent variable) were negatively associated with depressive symptom scores over time (as dependent variable) according to the results of mixed model analyses. As shown in Table 3, this was especially apparent from the between-subject effect (β = −.25, p < .001). Hence, “positive feelings toward God” predicted lower levels of depression over time. Furthermore, there was a very small, borderline significant within-subject effect (β = −.06, p = .027): Upward changes in “positive feelings toward God” were associated with small, downward changes in depressive symptoms.
Associations Over 6-Years Between Affective Aspects of Religiousness (Questionnaire God Representations Subscales and Brief RCOPE Subscales) and Depressive Symptoms: Results From Linear Mixed Model Analyses, Adjusted for Age and Sex, with Depressive Symptom Scores as Dependent Variable (at Baseline, 3 Years and 6 Years; One Follow-up at Least, N = 222); Fixed Effects (Random Effects Included Intercept Only) for Mixed Models and Hybrid Models.
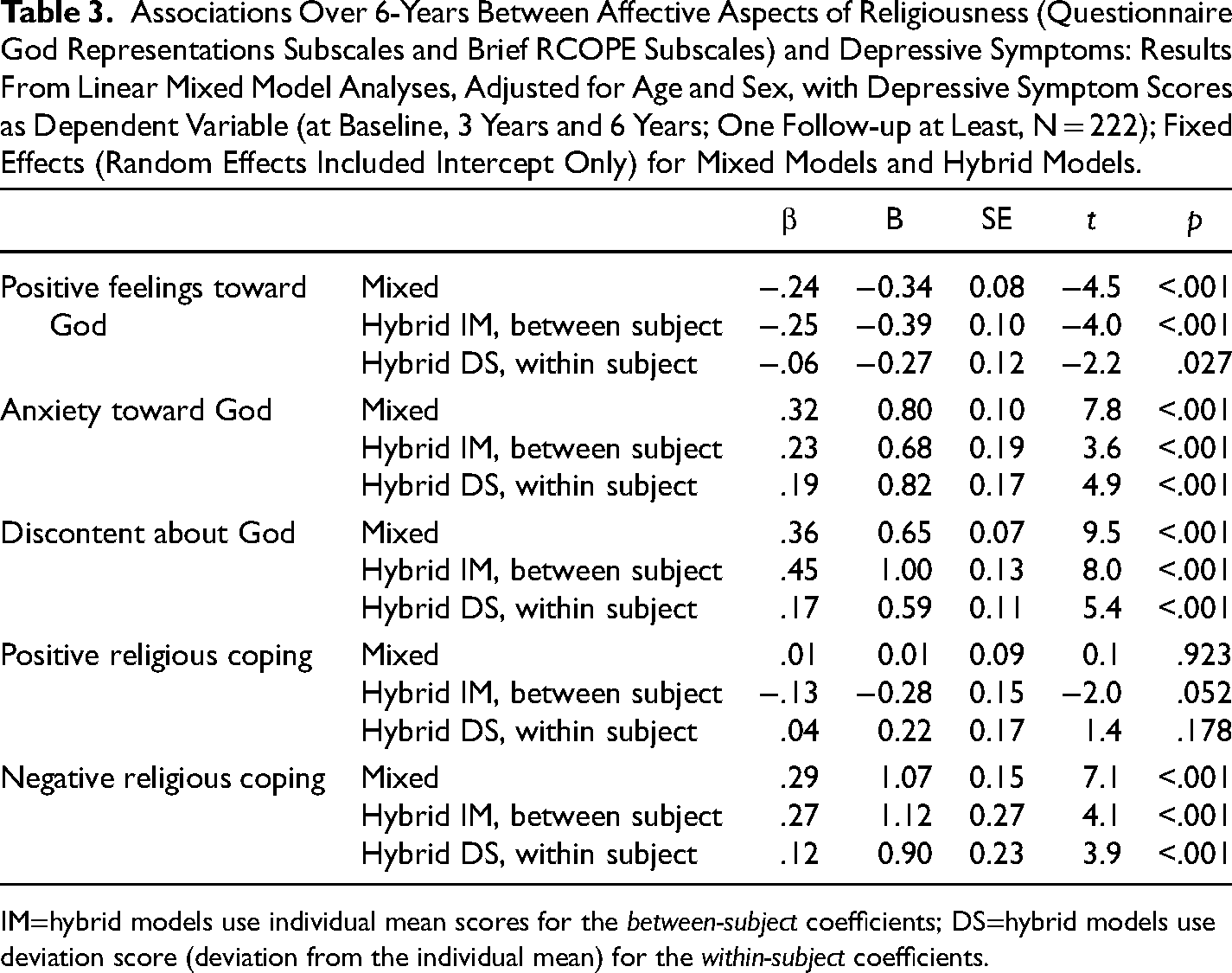
IM=hybrid models use individual mean scores for the between-subject coefficients; DS=hybrid models use deviation score (deviation from the individual mean) for the within-subject coefficients.
Figure 1 presents an illustration of the findings with respect to “positive feelings toward God,” based on analyses of variance at T0y, T3y, and T6y. For those with persistent-low levels of “positive feelings toward God” (solid black line), the CES-D scores were around 16, known as the criterion score for minor depression on the CES-D (Beekman et al., 1997). At follow-up, the CES-D scores for those with persistent-high scores were about five points lower (p = .009 at both T3y and T6y). The figure suggests that an upward change in “positive feelings toward God” (dashed, open line) aligned with lower levels of depressive symptoms (significant only at T3y, p = .019). However, for a downward change in “positive feelings toward God,” the pattern is less evident and nonsignificant.
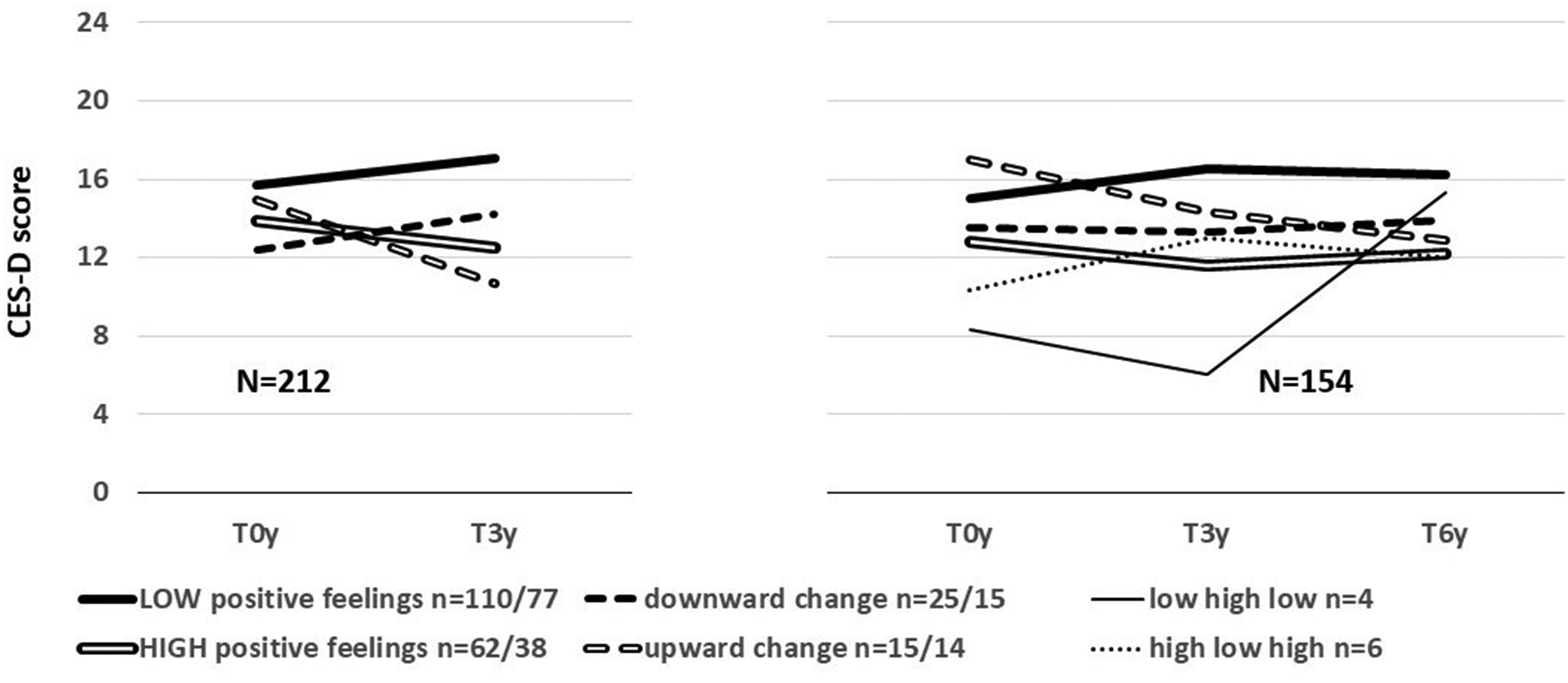
Mean CES-D depression scores for six course patterns on the Questionnaire God Representation for “positive feelings toward God” (highest tertile), adjusted for age and sex.
For the RCOPE subscale on “positive religious coping” (RCOPE), no significant associations with course of depressive symptoms could be demonstrated. The depression scores over time hardly differed for persistent-high and persistent-low “positive religious coping” scores (Supplemental Figure A).
Negative Aspects of Religiousness and Depressive Symptoms: Longitudinal Analyses
The results of the mixed model analyses regarding the QGR subscales on “anxiety toward God” and “discontent about God,” and the RCOPE subscale on “negative religious coping” (analyzed separately as independent variables) showed similar, positive associations between these subscales and depressive symptoms over time (as dependent variable). This was apparent from both between-subject effects and within-subject effects as shown in Table 3.
The most substantial between-subject effect was found for “discontent about God,” amounting to β = .45 (standardized coefficient; p < .001). As illustrated in Figure 2, CES-D scores among those with persistent-high scores on “discontent about God” were about 8–10 points higher as compared to those with persistent-low scores on “discontent toward God” (p < .001 in the post hoc analysis of variance, Supplemental Tables X and Y). Similar patterns pertained to “anxiety toward God” (between-subject β = .23, p < .001; illustrated in Supplemental Figure B) and the RCOPE subscale on “negative religious coping” (between-subject β = .27, p < .001; illustrated in Figure 3), with differences between persistently low and high scores around four to six points on the CES-D.
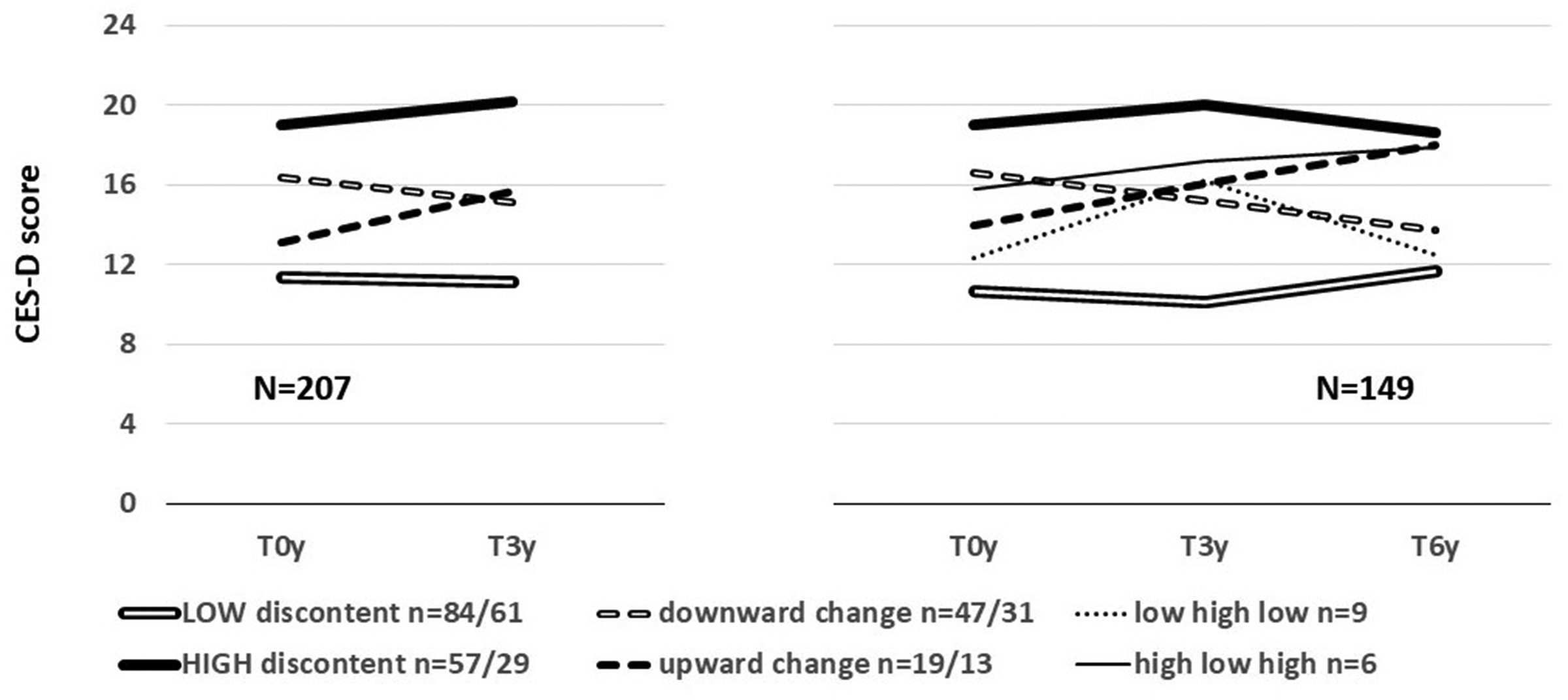
Mean CES-D depression scores for six course patterns on the Questionnaire God Representation for “discontent about God” (highest tertile), adjusted for age and sex.
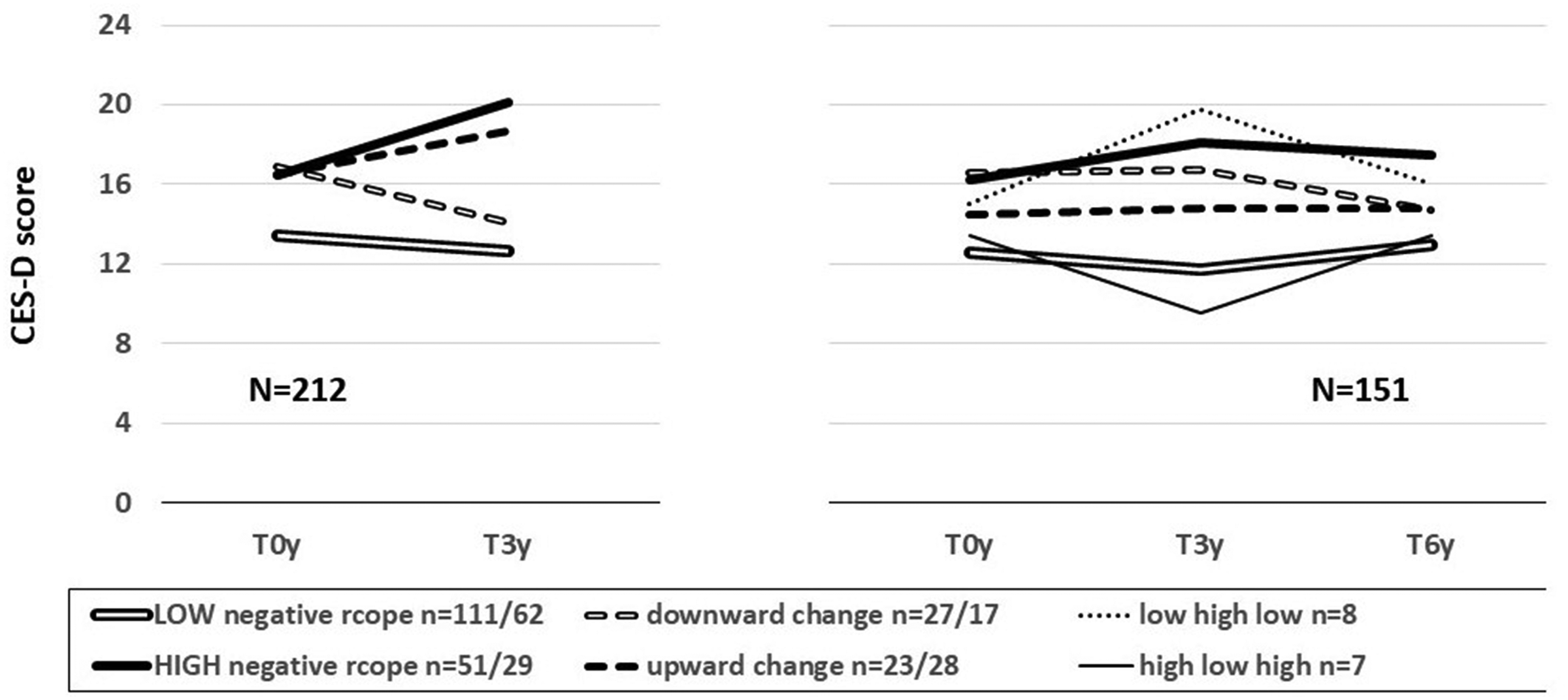
Mean CES-D depression scores for six course patterns on the RCOPE negative religious coping subscale (highest tertile), adjusted for age and sex.
The within-subject effects for the three subscales were modest (β between .12 and .19) but highly significant (p < .001). Upward changes in the three negative aspects of religiousness were associated with increases in depressive symptoms. Post hoc analyses of variance illustrate these associations. For example, for the QGR subscale on “discontent about God” (Figure 2), the CES-D scores at T0y for those with downward change were significantly higher compared to those with persistent-low scores (p < .001), but at T6y, this difference was no longer significant (Supplemental Table Y, p = .123). The opposite pattern was found for those with an upward change: The T0y CES-D scores did not significantly differ from those with persistent-low scores (p = .140), but at T6y, the CES-D scores are significantly higher (p < .001), a 4-point increase over time.
For “negative religious coping,” two very small, but indicative subgroups were those with changeable scores (low–high–low and high–low–high): the CES-D scores showed simultaneous, parallel change (Figure 3, right-hand part). Post hoc analyses of variance confirmed this pattern (Supplemental Table Y). For those with the low–high–low pattern (N = 8) on “negative religious coping,” the T0y and T6y CES-D scores differences with the persistent-low group were nonsignificant (T0y p = .381; T6y p = .149). However, at T3y, the low–high–low group has significant higher CES-D scores than the persistent–low group (p = .008). Similarly, the high–low–high group (N = 7) showed a difference at T3y when compared to the persistent-high group. There were no significant differences at T0y (−2.9, p = .387) or T6y (−2.7, p = .224), but at T3y, the high–low–high group had clearly lower CES-D scores (−8.4, p = .016).
Emergence and Persistence of High Levels of Depressive Symptoms
In the logistic regression analyses, “positive feelings toward God” and positive religious coping significantly predicted less emergence of high levels of depressive symptoms (Table 4, left-hand panel). The odds ratio for dichotomized scores (highest tertile vs. rest) on the subscale for “positive feelings toward God” emergent depression was 0.36 (95% CI 0.14–0.96; Wald 4.2; p = .040), a statistical trend. The odds ratio for dichotomized scores on the subscale for positive religious coping was 0.20 (95% CI 0.06–0.74; Wald 5.8; p = .016).
Predictions of Emergent or Persistent-High (≥16) CES-D Scores at T3y or T6y by Measures of Religiousness (in Separate Models) at T0y (Questionnaire God Representations Subscales and Brief RCOPE Subscales); Logistic Regression Analysis, Odds Ratios (RR) with 95% Confidence Intervals (95% CI), Adjusted for Effects by Age and Sex.
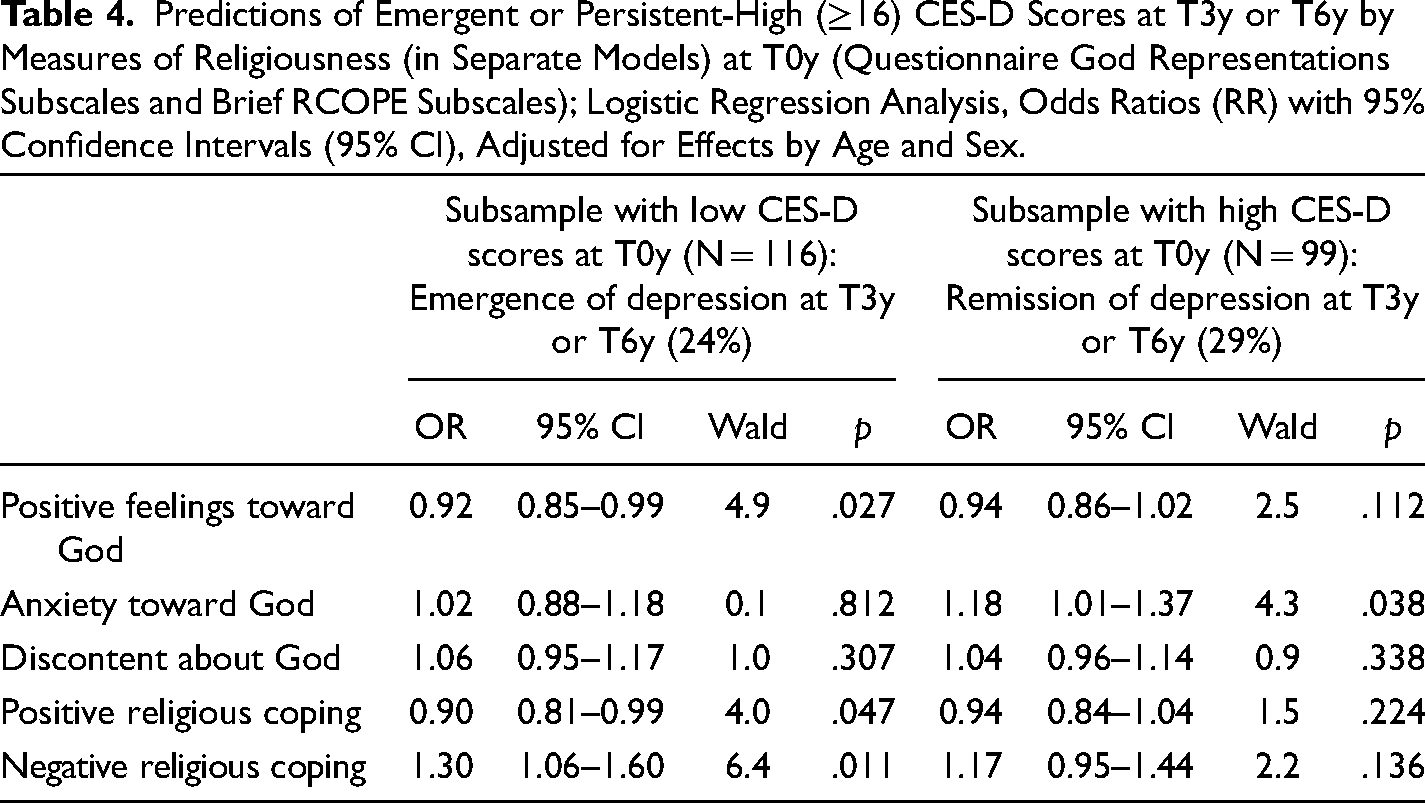
“Anxiety toward God” and “discontent about God” did not predict emergence of depression. However, negative religious coping showed a significant association with more emergence. For the dichotomized score (highest tertile vs. rest), the odds ratio amounted to 3.23 (95% CI 1.31–7.92; Wald 6.5, p = .011).
Persistence of high levels of depressive symptoms was only significantly predicted by “anxiety toward God” (Table 4, right-hand panel). However, the association with persistent depression for the dichotomized score of “anxiety toward God” (highest tertile) did not reach significance (OR = 2.19; 95% CI 0.88–5.43; Wald 2.9, p = .090).
Other Measures of Religiousness Predicting Course of Depressive Symptoms, Emergence, or Persistence
The mixed model analysis did not show a significant predicting effect on depressive symptoms of frequency of prayer at T0y (B = −0.23, SE = 0.16, β = −.06, p = .164). Frequency of religious attendance had a small but still nonsignificant predictive effect (B = −0.53, SE = 0.24, β = −.12, p = .031).
With respect to the emergence of high levels of depressive symptoms, the logistic regression analyses did not show predictive effects by the frequency of prayer or religious attendance (for details, see Supplemental Table Z). At trend level, the frequency of religious attendance predicted less persistence of depression (OR 0.77, 95% CI 0.59–1.02, Wald = 3.4, p = .066). For weekly church attendance (vs. yearly or less), this association reached significance (OR 0.22; 95% CI 0.07–0.76; Wald 5.7; p = .017).
Discussion
The current longitudinal study focused on associations between several affective aspects of religiousness and late life depressive symptoms over a 6-year period. Previously, very few studies have had access to data that allow longitudinal analyses necessary to test both more static and dynamic associations over time between these affective aspects of religiousness and late life depression. The measures of religiousness included scores on three types of feelings toward God as well as two main types of religious coping, positive and negative. Although there are conceptual differences between the five scales, two main patterns of results emerged.
The first pattern pertains to positive feelings toward God. Positive feelings toward God predicted lower levels of depressive symptoms over time, as well as less emergence of high levels of depressive symptoms. Furthermore, an increase in positive feelings toward God was associated, at trend level, with a decrease in depressive symptoms.
The second pattern of results pertains to negative feelings toward God (anxiety and discontent) and negative religious coping. These three scales can be regarded as measures that belong in the domain of so-called “religious/spiritual struggle” (Nieuw Amerongen-Meeuse et al., 2024; Pargament et al., 1998). These measures clearly predicted depressive symptoms over time: Those with persistent-high scores on the negative religiousness measures were more depressed, especially those with discontent about God. Furthermore, a general within-person change over time pattern was found, in which levels of religious struggle parallelled the course of depressive symptoms over time.
Persistent positive feelings toward God, therefore, seem to have a stable association with lower levels of depressive symptoms over time and are likely to represent a source of resilience. In turn, persistent-low levels of positive feelings toward God may add to vulnerability to depression. Whether these lower levels are acquired earlier in life is uncertain. Lower levels of positive feelings toward God may result from suffering from earlier depression and may show the disappointment with a previously presumed protecting potential as should have been offered by religion. However, recovery processes, earlier in life, may also have contributed to religious or spiritual coping abilities and spiritual growth or to discovering reasons to live for.
A complementary pattern relates to persistent religious struggle, being associated with higher levels of depression over time, reflecting an ongoing vulnerability to depression. Religious struggle, especially as measured with the negative religious coping scale, acted as a risk factor for emergent depression. Whether this points to a causal relationship is not certain. Although the participants were in old, even very old age, and dissatisfaction with religion may have developed during life (Nieuw Amerongen-Meeuse et al., 2024), even up to religious trauma (Slade et al., 2023), personality traits may play a role as well, as has been shown in some studies (e.g., Braam et al., 2008b).
The present study showed that a synchrony of change between religiousness and depressive symptoms was more prominent for religious struggle than for positive aspects of religiousness. Therefore, religious struggle may be conceived as overlapping with depressive symptoms. The items of the subscales reflecting religious struggle, however, hardly exhibit a literal content overlap with depressive symptoms. One may postulate that signs of religious struggle express existential concerns in persons suffering from depression. For example, a feeling of losing one's vitality, one's connection with others, as well as one's own future point to the personal and existential experience and suffering of depression. One might hypothesize that religious connotations to these existential concerns offer a vocabulary for religious people to express themselves. This religious, existential vocabulary may therefore serve as a frame of reference or attribution. Alternatively, these existential signs could precede depression as suggested by other studies (Pirutinsky et al., 2011).
A positive message of the current data and illustrations, possibly with clinical relevance, is that signs of religious struggle that simultaneously develop during depression are likely to decrease when depressive symptoms decrease. Regardless, ongoing religious struggles may deserve clinical attention during depression. Discussing them with the treatment staff, nurses in particular, was identified as a care need in a recent clinical study in the Netherlands (Nieuw Amerongen – Meeuse et al., 2020).
The present population-based study applied an oversampling of those with high levels of depressive symptoms at previous assessments. This may have led to a quasi-clinical sample with oversampling of depression, among whom levels of religious struggle are particularly high. These higher levels of depressive symptoms and religious struggle imply a higher potential of variability. Therefore, this oversampling might be considered a strength of this study, because in a less selective sample, associations between religiousness and depression might only have been substantiated at lower and less severe levels of depression, which are less clinically relevant.
One limitation of the study is that it does not address the themes of spirituality and sense of meaning and purpose in life, concepts that are likely to overlap with concepts of religiousness. In the past 10 years, more measures on spirituality and meaning in life have become available. Still, several measures, such as those with items on “spiritual well-being,” show content overlap with mental health, which inflates the associations studied. This problem has been coined as a tautological overlap (Garssen et al., 2016; Koenig, 2008). A similar concern can however be raised with respect to measures of religious struggle: A certain degree of general distress or depressive symptomatology may clearly be present in these measures.
Another limitation is that our study is performed in a partly Christian and partly secular population, so that the results may not be transferable to populations with other constellations of religious traditions. Furthermore, the sample size was limited, especially for demonstrating longitudinal associations between changes over time in religiousness and change in depressive symptoms. Similarly, for examining combinations of several types of feelings toward God or of both positive and negative religious coping in their associations with depressive symptoms, the statistical power of the study fell short. For a more accurate approach to describe temporal relationships, shorter intervals would have been more informative.
The employed religiousness measures presuppose a perceived, personal image of God. Other ways of imagining God are conceivable. In Western European studies in the psychology of religion and in empirical theology, support has been found for a “nonpersonal image of God” as well as an “unknowable image of God” that also had significant associations with psychological functioning such as with coping strategies (van Laarhoven et al., 2010). It might be worthwhile to include measures on these less personal representations of God in future studies. Furthermore, it is recommended for future studies to include other outcomes, such as anxiety and measures of loneliness. Moreover, personality characteristics, childhood attachment styles, and religious education may contribute to the explanation of our observed associations.
The present study elaborated on the affective dimension of religiousness, both from an object-relational point of view and from the perspective of coping strategies. Here, psychiatric epidemiology borders on the psychology of religion. The affective dimension of religion has been subject to speculations in the past. For example, historically, religious emotion has been considered a separate, unique type of affect, with either a sense of fear or awe, or a sense of trust and tender emotion, or a combination of these (e.g., Ribot, 1897). James (1902), an important early scholar in the psychology of religion, however advised against conceiving of one type of “religious sentiment” (p. 27). Nevertheless, he distinguishes one distinct characteristic of religion: “enthusiasm in solemn emotion” (p. 48). Pargament and Mahoney (2005) theorize about these positive feelings and describe how people tend to “sanctify” emotions in daily life, both theistically and nontheistically. In contemporary theories in positive or existential psychology, “meaning in life” sometimes serves as an overarching concept with respect to spirituality and religiousness. One core component of meaning in life, next to “purpose” and “coherence,” is “significance” (Martela & Steger, 2016). The experience of significance carries resemblance with a sense of awe, or awe of God, a construct that has been shown to correlate with practical wisdom (Krause & Hayward, 2014). The experience of significance such as a short bliss or sense of awe may be incidental, but significance may also manifest itself as an ongoing, basic emotional tune. In the current study, this basic emotional tune may coincide with positive feelings toward God. In coming generations in Western Europe, the explicit role of religion may diminish in matters of meaning in life. Therefore, further inquiry is needed into how to understand the basic, affective dimension of meaning in life and its relationship with resilience, mental health, and psychiatric vulnerability.
Supplemental Material
sj-docx-1-ahd-10.1177_00914150241297575 - Supplemental material for Affective Aspects of Religiousness and 6-Year Course of Depressive Symptoms in Aged Dutch Citizens
Supplemental material, sj-docx-1-ahd-10.1177_00914150241297575 for Affective Aspects of Religiousness and 6-Year Course of Depressive Symptoms in Aged Dutch Citizens by Arjan W. Braam and Joke C. van Nieuw Amerongen-Meeuse, Tjalling J. Holwerda, Hanneke Schaap-Jonker, Dorly J.H. Deeg, Aartjan T.F. Beekman, Martijn Huisman in The International Journal of Aging and Human Development
Footnotes
Acknowledgments
The data have been collected in the context of the Longitudinal Aging Study Amsterdam, funded primarily by the Netherlands Ministry of Health, Welfare and Sports. The current study has been supported by a grant from the Netherlands Organization for Health Research and Development (Zon-MW Grant 2003-05769). An earlier draft of the present study was presented at the 7th European Conference on Religion Spirituality and Health, May 27–28, 2021.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Research Data Access
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.