
Abstract
Measures of life outlook in older adults have been investigated in connection to pain, as both pain management and outlook are important factors of successful aging. We hypothesized that higher pain is associated with lower optimism among community-dwelling older adults. We utilized data from the UC San Diego Successful Aging Evaluation (SAGE), a prospective longitudinal cohort study initiated in 2010, to evaluate the relationship between pain and optimism in 378 community-dwelling adults aged ≥50 years. We used the revised Life Orientation Test (LOT-R) to measure optimism and three pain subscales–PROMIS Pain Interference, PROMIS Pain Intensity, and MOS 36-Item Short-Form Health Survey (SF-36)–as pain measures. Regression analyses reveal negative relationships between pain and optimism for all three pain scales, with regression coefficients of −0.277 (p < .0001), −0.246 (p < .0001), and 0.269 (p < .0001) respectively. This indicates value in considering physical and psychological elements in future intervention research to promote healthy aging.
Introduction
Both pain management and life outlook—an individual's feelings on their own life—are important factors for healthy aging (Barnes et al., 2021; Molton & Terrill, 2014; Ramos & Brown, 2020).. Chronic pain worsens socialization, sleep quality, physical activity, and mood in older adults, making it an essential symptom to understand and treat. In previous reports, measures of poor life outlook in older adults have been investigated in connection to pain. For example, depression has been reported to be strongly associated with higher pain levels and interference with daily activities (Molton & Terrill, 2014; Musich et al., 2019). Mood disorders, including depression, have also been found to correlate directly with lower optimism levels in a study of community-based adults, although depression does not equate a lack of optimism (Kim et al., 2019; Öcal et al., 2022). In regards to pain, in a study of aging women, participants with lower pain interference and higher activity levels reported increased optimism over a two-year study time span (Judge et al., 2019).
Studies have also shown that older adults respond to pain differently than younger adults, with the two groups using different levels of cognitive coping strategies as forms of pain management, although findings are not consistently agreed upon (Molton & Terrill, 2014). Hence, research up to this point agrees that outlook on life intersects with pain levels and responses in older adults. However, there is a lack of investigation addressing this relationship as a means to improve the understanding of clinical and psychological factors that predict healthy aging, especially in a large, randomized, and representative dataset.
With the significant influence pain has on aging adults and previous supportive findings, it is reasonable to predict a potential negative relationship between self-assessed positive life outlook and pain. Here, we test the hypothesis that higher pain levels are associated with lower optimism among community-dwelling older adults.
This study investigated the trends in self-reported pain and pain interference across different demographic groups and potential relationships between self-reported pain and optimism in a cohort of community-dwelling older adults from a prospective longitudinal cohort study.
Methods
Participants
Data from the University of California, San Diego Successful Aging Evaluation (SAGE), a prospective ongoing longitudinal cohort study initiated in 2010, was used to conduct a cross-sectional evaluation of the relationship between pain and optimism in 378 community-dwelling adults aged ≥50 years. All participants were initially recruited through random-digit dialing in San Diego County. Data was drawn from the 2015 SAGE questionnaire, which surveyed a total of 860 individuals. Forty-five percent of participants were included in this analysis, as 618 were aged ≥50 years, and 387 fully completed scales on pain, optimism, and resilience.
Pain
Three pain subscales were used in the 2015 SAGE survey and all three measures were separately analyzed in relation to optimism scores. Two Patient-Reported Outcomes Measurement Information System (PROMIS) scales were used, the Pain Intensity Short Form 3a and Pain Interference Short Form 8a. For the former, participants answered two questions inquiring about their pain in the last seven days on a scale from “no pain” to “very severe” pain (“How intense was your pain at its worst?” and “How intense was your average pain?”). The form included a third, final question asking about current pain (Instrument: PROMIS Pain Intensity—Short Form 3a V1.0, n.d.). Raw scores can range from 3 (lowest pain intensity) to 15 (highest pain intensity) and correspond to T-scores ranging from 36.3 to 81.8, respectively, as of the most recent grading scale (Pain Intensity Scoring Manual, 2021).
The PROMIS Pain Interference Short Form 8a included eight questions regarding the way pain interfered in the participant's day-to-day life over the past seven days (e.g., “How much did pain interfere with the things you usually do for fun?,” “How much did pain interfere with work around the home?”) (Pain Interference—Short Form 8a, n.d.). This scale was also analyzed using T-scores ranging from 40.7 to 77, which correlate to raw scores of 8 to 40, respectively (Pain Interference Scoring Manual, 2023).
The third pain measure used was two pain-related questions from the Medical Outcomes Study (MOS) 36-Item Short-Form Health Survey (SF-36), which consists of 36 items overall. In contrast to the PROMIS questions, the selected SF-36 questions asked participants to report both pain intensity and pain interference experienced over a longer period—over the past month. Additionally, the pain intensity question (“How much bodily pain have you had during the past 4 weeks?”) specified physical pain, while the interference question (“During the past 4 weeks, how much did pain interfere with your normal work (including both work outside the home and housework)?”) restricted the question to work-interference (Rand Corporation, 2019). For this measure, a higher score indicates lower pain, unlike the PROMIS scoring.
Optimism
The revised Life Orientation Test (LOT-R) was used to measure optimism. This measure provided a single score based on six items, three of which were reverse coded. The participant responded to 10 items on a scale of “Strongly Disagree” (coded as 0) to “Strongly Agree” (coded as 5), with four items serving as filler questions (Stanford University, n.d.). The LOT-R represents optimism through raw scores from 6 to 30, with higher scores indicating a higher propensity for optimism.
Data Analysis
To analyze potential relationships, Spearman correlations were conducted separately for all three pain measures and LOT-R. For the purpose of analysis, pain levels were considered as the independent variable and optimism levels as the dependent variable, although no analysis of causation was conducted. Median pain intensity, pain interference, and optimism levels were also calculated for sample subgroups based on demographics.
Results
Pain and Optimism
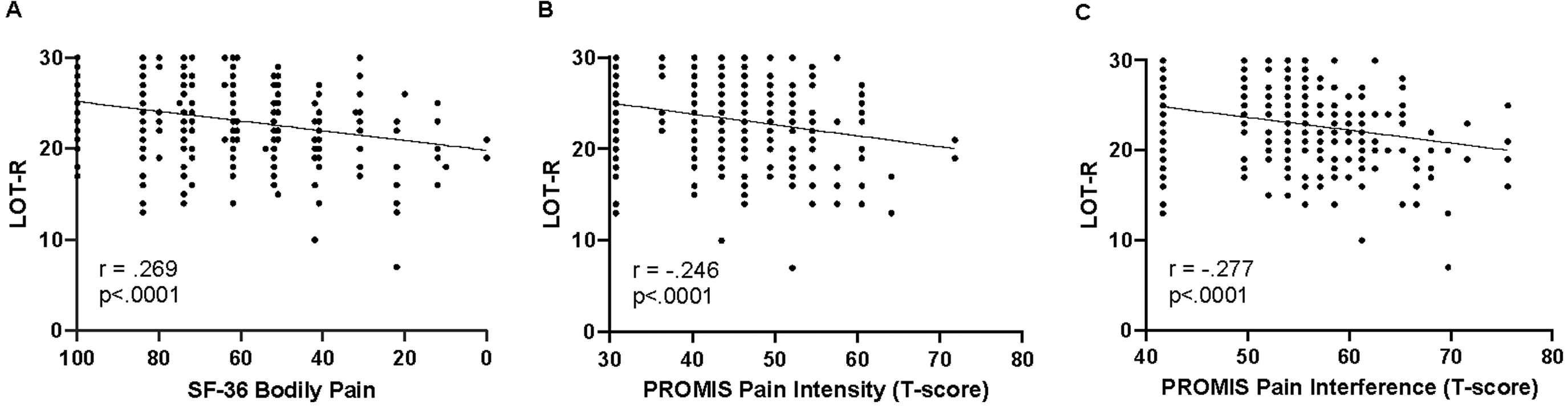
Negative correlations were found between all pain measures and optimism levels. Correlations between optimism and PROMIS Pain Intensity, PROMIS Pain Interference, and SF-36 were −0.246 (p < .0001), −0.277 (p < .0001), and 0.269 (p < .0001) respectively (see Figure 1). This correlation remained significant when adjusting for gender, age, education, marriage status, and household income (see Table 1). However, the correlation was not statistically significant among the non-Caucasian participants alone (n = 87) (p > .05), although the trend mirrored that seen in Caucasian participants (n = 300).
Spearman correlations of pain measures and LOT-R optimism.
Spearman Correlations of Pain Measures and LOT-R Optimism.
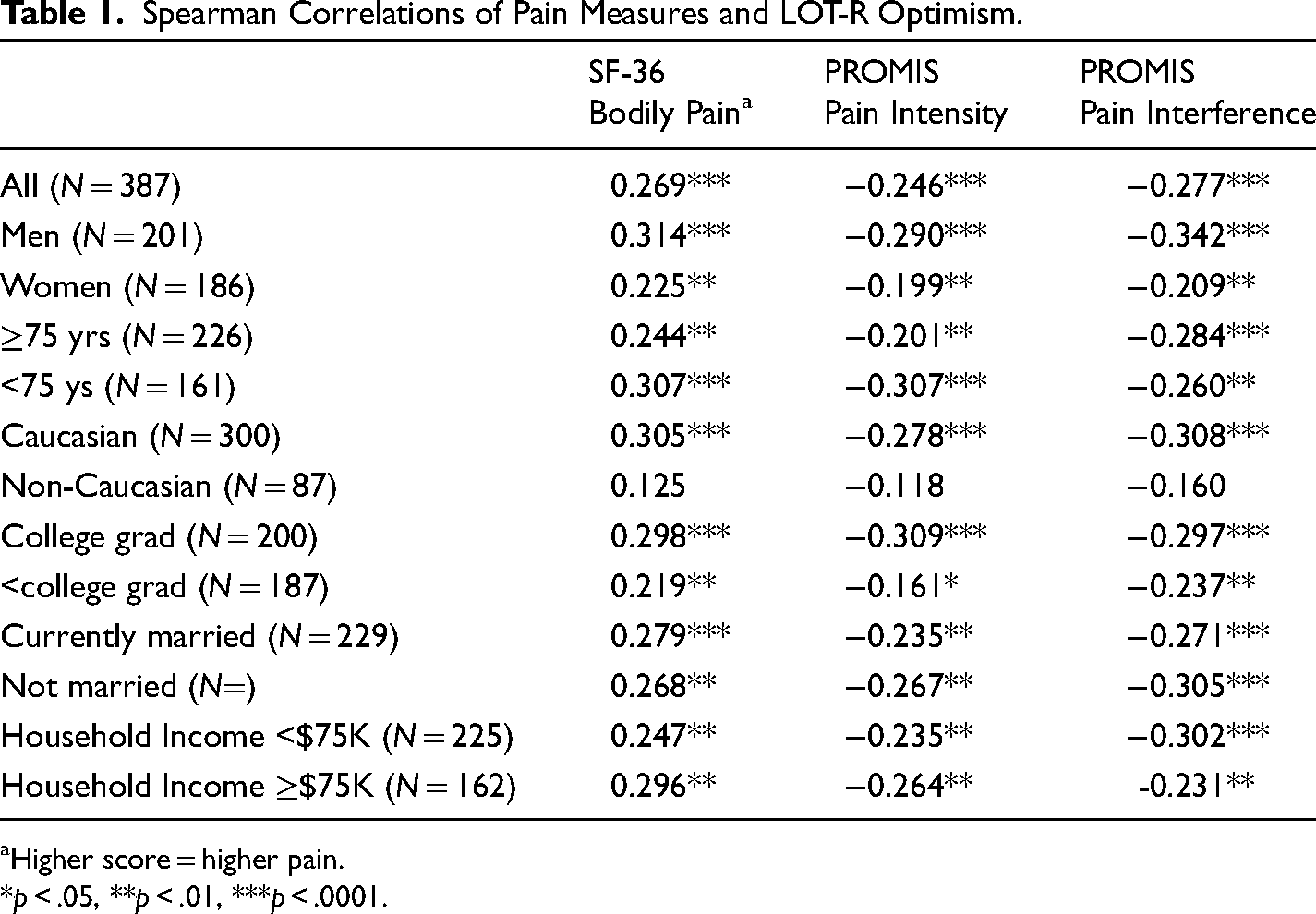
Higher score = higher pain.
*p < .05, **p < .01, ***p < .0001.
When analyzed by demographic groups, Spearman regression coefficients for correlations between pain interference and optimism were slightly stronger among men at −3.42 (p < .0001). Men also had slightly stronger regression coefficients for the relationship between SF-36 scores and optimism at 3.14 (p = .0001) (see Table 1). Regression coefficients for correlations between pain intensity and optimism were also slightly stronger for college graduates at −3.09 (p < .0001) in comparison to other groups.
Pain Prevalence by Demographics
Age
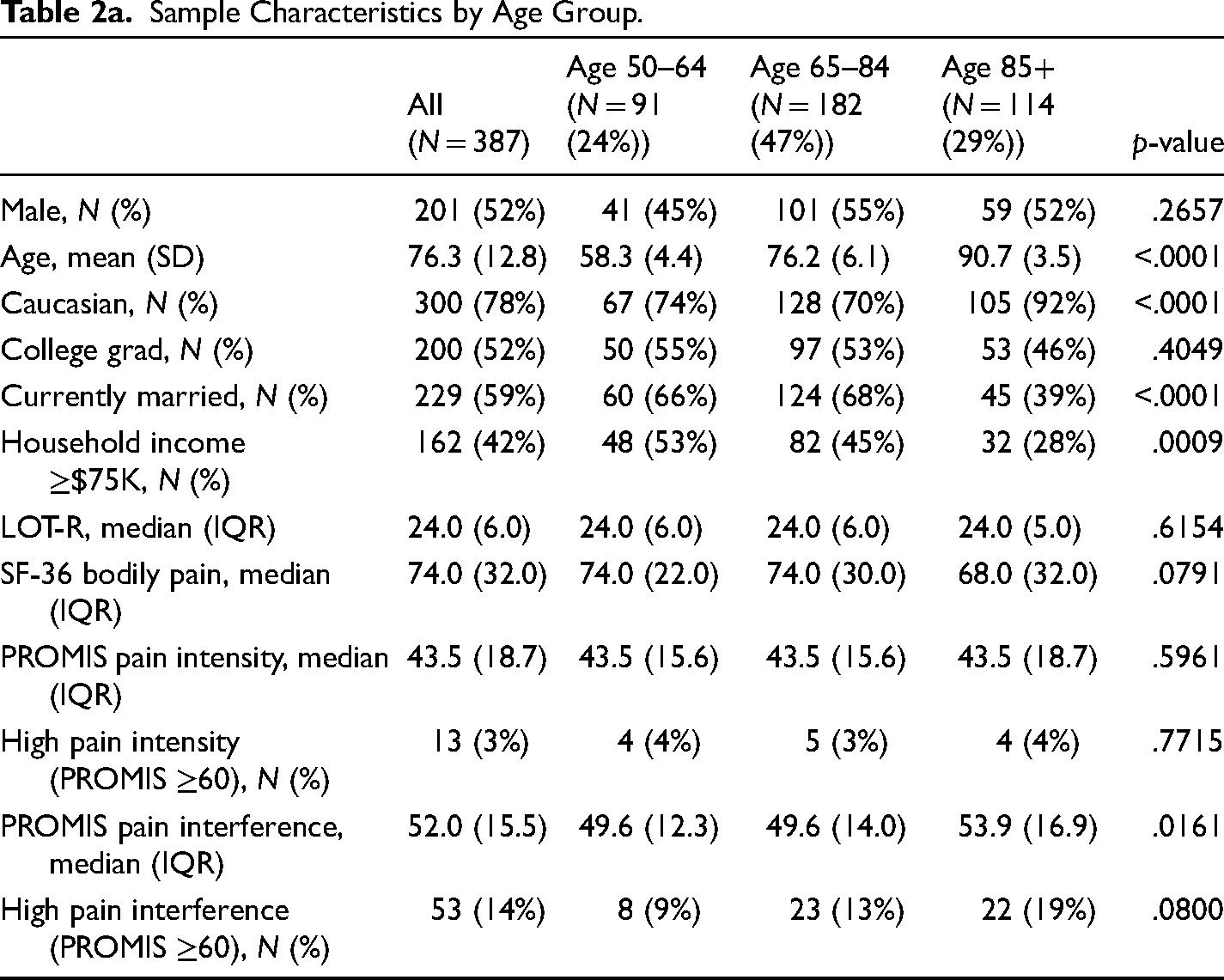
When separated by age range, pain interference as reported on the PROMIS Pain Interference scale was highest in those aged ≥85 years (n = 114) at a median T-score of 53.9 (p = .0161), versus median scores of 49.6 for both those aged 50–64 (n = 91) and those aged 64–84 (n = 182) (see Table 2). However, median pain intensity as reported on the PROMIS Pain Intensity scale, and median pain as measured by the SF-36 pain scale, did not vary by age group.
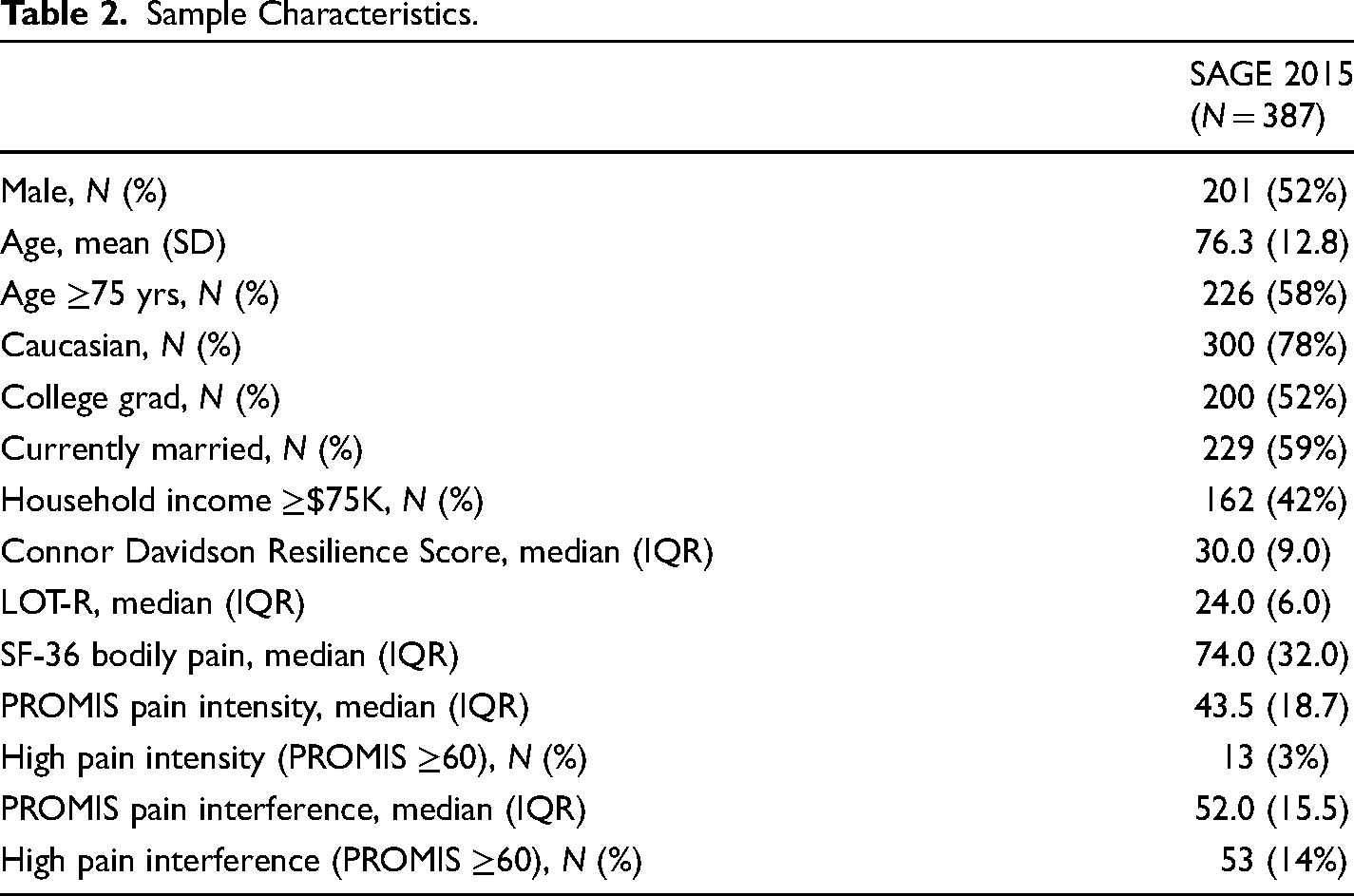
Sample Characteristics.
Sample Characteristics by Age Group.
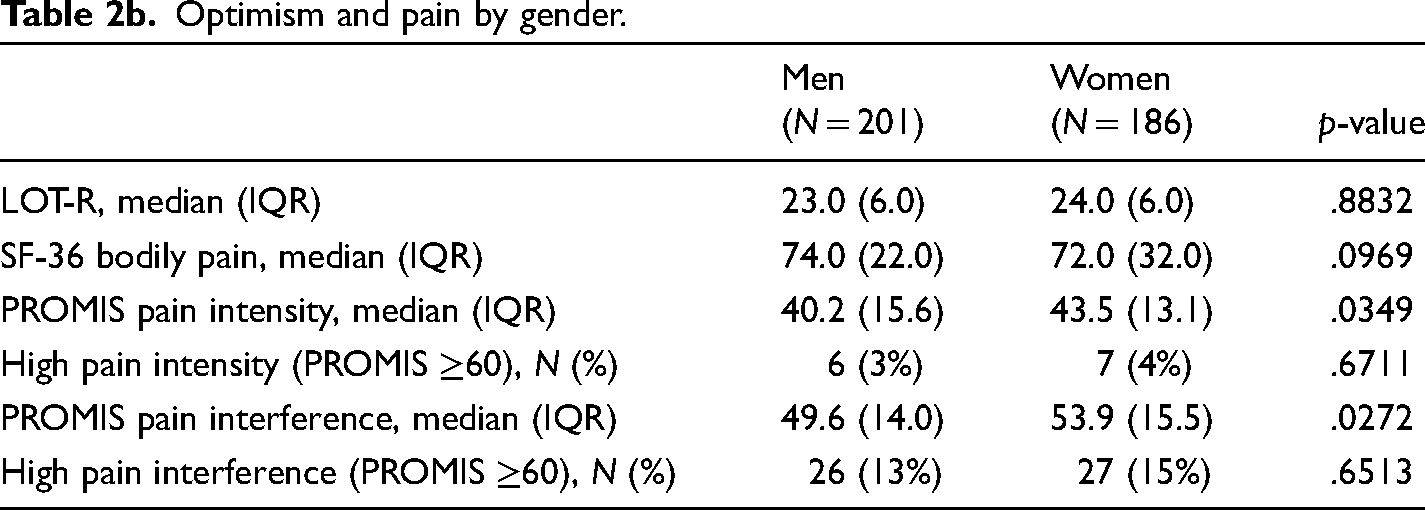
Optimism and pain by gender.
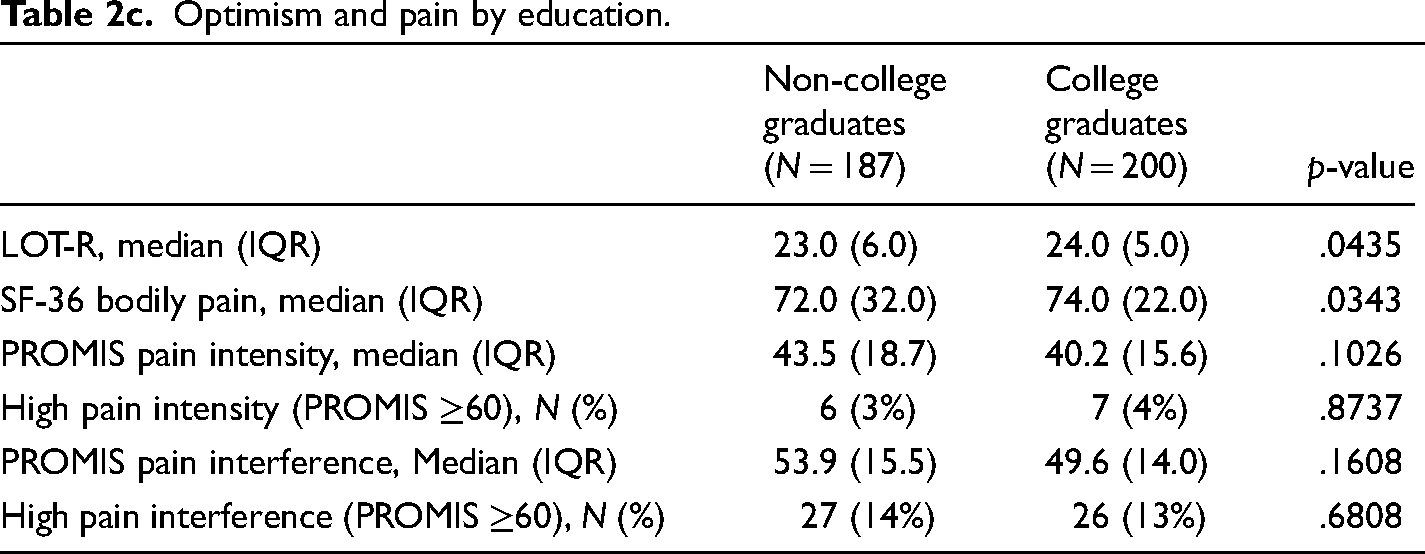
Optimism and pain by education.
Gender
On both PROMIS scales, women reported higher median pain levels than men (p = .0349 for intensity and p = .272 for interference). However, there was no difference in the percentage of individuals of each gender who reported high pain intensity and interference levels (see Table 2).
Education Level
Those without college education had lower pain, as reported on the SF-36, than those with college education (p = .0343). However, there was no statistically significant difference between the two groups’ pain and pain interference levels on the other scales (see Table 2).
Discussion
The negative correlation found between self-reported optimism and pain (intensity, interference, and a combination of both) indicates that the benefits of pain relief and positive life outlook for older adults are intertwined. This correlation was present across income levels, education levels, age ranges, gender, and marital status, indicating the generalizability of this relationship. The slightly stronger correlations for men and those with college education are intriguing considering that their respective counterparts (women and those without college education) were two groups who reported higher pain levels. Positive associations between optimism and the likelihood of maintaining healthy aging among adults without disabilities or chronic disease in a 2019 study were also stronger in men compared to women (Kim et al., 2019). This suggests a larger trend in the way optimism contributes to healthy aging among individuals of different genders that should be investigated further. Future research can investigate the way education levels and gender may play a role in older adults’ experiences with pain and low optimism.
It should also be considered that individuals experiencing chronic physical or psychological medical conditions may be more likely to be facing both worse pain and lower optimism, a concerning prospect in efforts to promote successful aging. Optimism is thought to potentially promote healthy aging through the promotion of health behaviors and biological means. Therefore, optimism is a valuable health promotion target for enhancing the health of older adults (Kim et al., 2019).
Understanding the relationships between optimism and pain can also help inform future intervention research in several ways. Although a causal relationship is not yet established, interventions can help determine whether higher optimism may lead to lower pain perception, and/or if lowered pain may result in higher optimism levels. Either potential result, or a bi-directional causal relationship, may inform interventions for improved pain management and psychological adjustment. For example, pain management programs for older adults could focus on optimism-building as a main goal, evaluating optimism as a potential mediator for pain reduction. Furthermore, if a causal relationship is established, older adults with depression may be key target populations for mental health support programs using optimism-focused work to potentially reduce both symptoms of physical pain and psychological distress.
The varying levels of pain reported by different demographic groups also provide insights into who might benefit most from interventions to improve healthy aging. Prior analysis of pain interference in community-dwelling adults aged ≥70 years using different pain scales also found that women and those with lower levels of education reported higher interference levels (Koren & Leveille, 2020). Those who report higher pain levels, such as women and those without college education, would benefit from targeted research, especially as these findings are also reflected in other studies.
Limitations
This study was limited by the underrepresentation of non-Caucasian participants (n = 87). This restricted statistical power and therefore likely contributed to the lack of statistical significance in correlations for this group. An emphasis on racially/ethnically diverse participants should be pursued in future research on the relationship between optimism and pain levels in older adults. This is especially pertinent as the older population in the United States continues to diversify, with racial/ethnic minorities projected to make up 34% of adults 65 and older by 2040 (2021 Profile of Older Americans, 2022).
Additionally, reliance on self-report survey data can also be problematic. Pain and life outlook can be difficult factors to measure objectively, especially when a participant is reflecting on their own levels. Older adults and those with multiple medical conditions may downplay aspects of their pain due to perceiving pain as reasonable for their age or less intense in relation to other experiences, respectively (Molton & Terrill, 2014). Furthermore, individuals may have different pain tolerances which impact their quantification of pain. “Pain” and “bodily pain” both may be interpreted differently by individuals, with some people excluding different types of pain from their responses. For example, one participant may include the interference their back pain has with their daily activities, but not the interference stemming from their migraines, while another participant considers both in their survey response. This variation was likely present despite the use of three pain measures in this study to help navigate the potential differences in how people report pain intensity compared to pain interference. Moreover, self-perceived views on how pain affects quality of life may not align with quantitative or biological measures.
In conclusion, pain and poor life outlook among community-dwelling older adults are interrelated contributors to quality of life for older adults. The negative correlation between optimism, pain intensity, and pain interference should be explored for potential causal relationships and to inform future intervention research to promote successful aging across a variety of demographic groups.
Footnotes
Acknowledgments
We thank all MADURA and SAGE staff, as well as SAGE participants.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The University of California San Diego MADURA ADAR program is supported by the National Institute on Aging (R25 AG066594; Steven D. Edland, P.I.). Data were supported, in part, by UC San Diego Sam and Rose Stein Institute for Research on Aging.