
Abstract
Fear of falling might result in overprotection by one's social environment. In turn, feeling dependent could increase fear of falling. However, the association between fear of falling and perceived overprotection and its temporal order is unknown. This longitudinal study explores this potential mutual longitudinal association. This study presents secondary analyses from a larger trial. We tested the association between fear of falling and perceived overprotection in a cross-lagged path model controlled for falls, health-related quality of life, age, gender, and trial condition. N = 310 participants (M = 70 years, range: 64–92) completed self-reports at Time 1, 7 (Time 2), and 11 weeks (Time 3) after baseline assessment. We found a positive association from fear of falling to perceived overprotection (β = .12, 95% CI[0.02, 0.21], p = .02; β = .10; [0.01, 0.18], p = .03). The reversed cross-lagged paths were not significant. Findings suggest higher fear of falling translates into perceived overprotection, which may in turn increase loss of independence in old age.
Introduction
Fear of falling is a serious concern in old age. It is described as a continuous concern that one might experience a fall (Tinetti & Powell, 1993). This fear may lead to the avoidance of activities, although these are still within the capabilities of an individual (Tinetti & Powell, 1993). Two in three older adults aged 60 years and older are afraid of falling and nearly 40% of them avoid activities as a consequence (Auais et al., 2017; Merchant et al., 2020). The restriction of activities due to fear of falling can indeed reduce falls (Rivasi et al., 2019). However, avoiding activities results in deterioration in physical functioning which in turn increases the risk of falls (Liu et al., 2020; Whipple et al., 2018). This process can lead to a downward spiral of immobility (Clemson et al., 2012) and may result in a loss of independence in the long term. Hence, activity programs for older adults should incorporate strategies to overcome fear of falling besides the promotion of physical abilities to counter the loss of independence (Steckhan et al., 2022). However, fear of falling in old age does not evolve independently of older adults’ social environment (Honaker & Kretschmer, 2014) and should be investigated taking this into account.
Fear of Falling Carries Over into Social Exchange Processes in Old Age: Overprotection
While individuals, who experience high fear of falling tend to overprotect themselves from perceived risky activities, these primarily individual concerns could carry over to well-intentioned support from the social environment, or origin from overprotection from the support network. Family, friends, and caregivers might tend to overprotect because they want to help older adults in coping with everyday life, possibly even more so, if they perceive their protégés to experience fear. Thompson and Sobolew-Shubin (1993) defined overprotection in adulthood as “a perception on part of the ill adult that he/she is overhelped, induced to be dependent, shielded from stress, and generally not treated as an adult” (p. 87). In other words, overprotection implies the underestimation of older adults’ abilities and consequently the needless support for activities and challenges older adults would still be capable to overcome themselves (Niemann-Mirmehdi et al., 2019). Overprotection can arise in different contexts, such as through family, friends, or significant others not only at home but also at care facilities. While social support is considered as positive, overprotection displays an unintended hindrance and could be understood as a maladaptive and problematic manner of receiving support (Thompson et al., 2002). In a qualitative study by Gallant et al. (2007), older adults reported discouragement of physical activity as one example of overprotection. Quantitative research extended this finding and revealed that overprotection is related to lower levels of activation and predicts a decline in physical functioning in the long term (Bertoni et al., 2022; Joekes et al., 2007).
Fear of Falling in Association with Overprotection in Old Age
Studies examining overprotection among older adults primarily investigated individuals with chronic illnesses such as cardiac or renal diseases (e.g., Bertoni et al., 2022; Jansen et al., 2014). In individuals with chronic diseases, higher levels of functional disability may be related to increased levels of perceived overprotection as shown in a study by Cimarolli et al. (2006) investigating older adults with visual impairment. Very little is known about overprotection in association with or as a consequence of fear of falling in old age. However, overprotection might particularly occur in the context of fear of falling due to safety concerns of the social environment. For instance, caregivers reported to alter their routine after a fall with the primary objective to monitor care recipients (Dow et al., 2013). In another study, caregivers overprotected their patients with the intention to prevent future falls (Ang et al., 2019). Overprotection of the social environment as extensive assistance with activities of daily living might lead to limited mobility (Yeom et al., 2008), which in turn could increase fear of falling among older adults. In addition, older adults are not just passive recipients of well-intentioned support (Gallant et al., 2007) and might internalize an overprotective social environment that could manifest itself in fear of falling or the will to comply with the intentions of significant others (in a sense of subjective norms as specified in the reasoned action approach; Fishbein & Ajzen, 2009). Having summarized preliminary findings on not only how fear of falling might elicit overprotection from the social environment but also how overprotection might increase fear of falling, the empirical question arises which association is stronger: the prediction of higher overprotective behavior by fear of falling or the prediction of higher fear of falling by an overprotective social environment. Therefore, we aim to investigate the reciprocity of the relationship between both concepts. This is of particular importance to gain insights into the possible origins and consequences of well-intentioned support from family, friends, and caregivers that might be perceived as overprotective by older adults. If individuals in the social environment of older adults tend to reinforce fear-related beliefs by reacting overprotective, raising awareness among family, friends, and caregivers is required. The social environment could be sensitized to the fact that extensive assistance might result in a loss of independence in old age.
Aim of the Study
As depicted in Figure 1, our study examines the relationship between fear of falling and perceived overprotection in a cross-lagged path model. The longitudinal study with three measurement points spanning three months allows to investigate the reciprocity of the relationship continuously over time to detect a consistent effect. Based on the studies mentioned above, we assumed a downward spiral between fear of falling and perceived overprotection. We hypothesized that higher fear of falling is associated with higher levels of perceived overprotection across all assessment points. Conversely, we hypothesized that the perception of higher overprotection of the social environment is related to higher fear of falling for all measurement points.
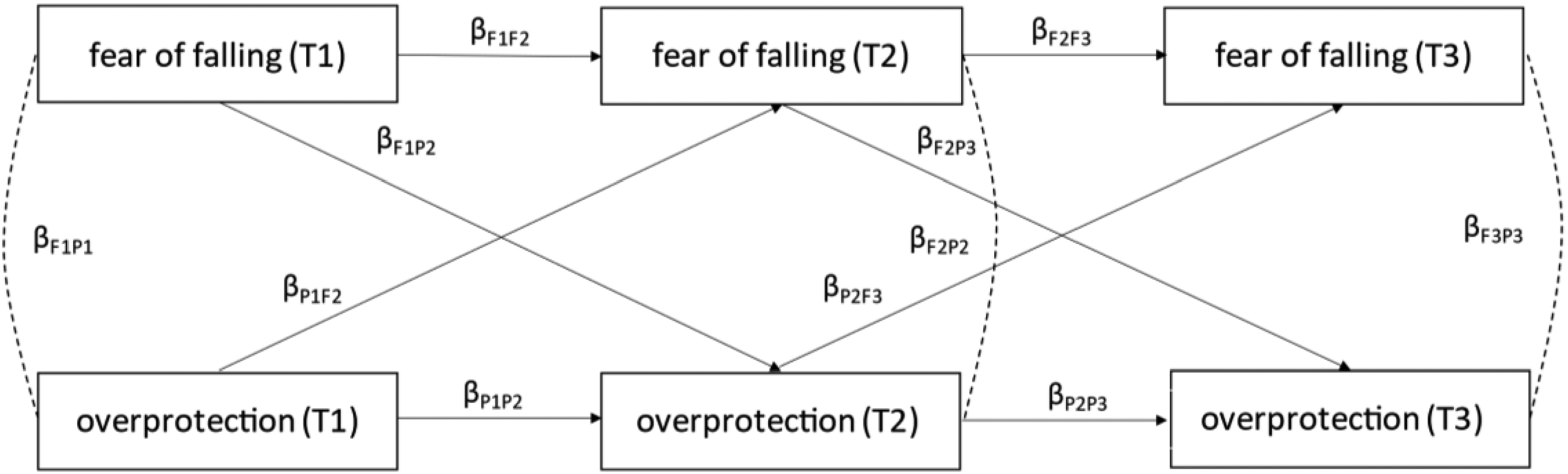
The conceptual cross-lagged path model covers four auto-correlations (βF1F2, βF2F3, βP1P2, and βP2P3), three cross-sectional correlations (βF1P1, βF2P2, and βF3P3), and four cross-lagged correlations (βF1P2, βF2P3, βP1F2, and βP2F3).
Methods
Participants and Procedure
This paper presents secondary analyses of data from the PREFER II trial. The trial was registered at www.clinicaltrials.gov (NCT01577134). The German Psychological Society granted ethical consent (DGPs-SW02-2012). Using newspaper articles, flyers, as well as advertisement letters sent to German health insurance companies, a sample of community-dwelling adults aged 64 years and above was recruited in Berlin, Germany. As an expense compensation, each participant received 25€. Within the randomized controlled trial (RCT) older adults were randomized into four groups: two intervention groups, an active control group, and a passive control group. The intervention groups comprised a three-hour face-to-face behavior change intervention with motivational and volitional behavior change techniques to increase physical activity in a group setting. The intervention session took place five weeks after Time 1 (T1). See Warner et al. (2014; 2016) as well as Wolff et al. (2014) for further details on study groups of the RCT and a flowchart of study participation.
Inclusion criteria were a minimum age of 64 years and exercising less than twice a week for 30 min. We excluded older adults who had an acute physical impairment, were disabled or cognitively impaired. N = 310 participants gave their informed consent and filled out the baseline paper-and-pencil questionnaire in Spring 2012. Participants received follow-up questionnaires via mail with prepaid return envelopes seven weeks (M = 6.95, SD = 1.57, Time 2 (T2)) after T1 and four weeks (M = 4.27, SD = 1.55, Time 3 (T3)) after T2. Due to inaccuracies in the autoregressive and cross-lagged estimates that are caused by unequal time intervals in cross-lagged path model (Newsom, 2015), we do not consider the fourth measurement point seven months (M = 27.99 weeks, SD = 2.31) after T3; 253 participants completed T2 (82% of T1) and 244 remained at T3 (79% of T1). Participants’ average age was 70.34 years (SD = 4.89, range = 64–92 years) at T1, and women were predominant (75%) in the sample; 53% of older adults were high-school graduates and 46% lived with a partner. Seven percent rated their health status as bad or very bad and a quarter (26%) experienced at least one fall in the past 12 months.
Measures
At T1, fear of falling was assessed with two items validated by Friedman et al. (2002)—“In the past 12 months, have you been afraid that you might fall?” and “Did you limit your activities at home or outside because you were afraid of falling?”. Both items were reassessed at T2 and T3 while adapting the time interval of the first item—“Since the last survey, have you been afraid that you might fall?”. Answers were given on a five-point scale from (almost) never (1) to (almost) always (5). In our sample, the correlation of the two items was rT1 = .75, rT2 = .72, and rT3 = .57.
Participants rated perceived overprotection at each measurement point on a four-point scale with answering options ranging from fully disagree (1) to fully agree (4). The following three items from Thompson and Sobolew-Shubin (1993) were used—“People from my family and circle of acquaintances…” “… no longer let me do things that I could do myself.”, “…want me to be dependent on them.”, “… keep me from doing things that might frustrate me”. Good internal consistency was shown in an earlier study by the authors of the scale comprising eight items (α = .88; see Thompson & Sobolew-Shubin, 1993). In our study, Cronbach's α was αT1 = .52, αT2 = .63, and αT3 = .71.
Covariates were falls, health-related quality of life, age, gender, and trial condition measured at T1. The question—“How often did you fall in the last twelve months?” was used to assess the number of falls. Health-related quality of life was measured with the item—“In general, how would you describe your health in the last 4 weeks?” (TNS Infratest Sozialforschung, 2011). Participants rated their answers on a six-point scale ranging from very bad (1) to excellent (6).
Statistical Analysis
Data analyses were performed using the lavaan package in R (version 4.1.1). With 79% of older adults who participated at T1 completing T3, withdrawal across time was acceptable. χ2 tests and t-tests were calculated to compare participants who dropped out with those who remained in the study on all measures included in these analyses. Results revealed no significant differences. Hospital admissions, major health problems, and time constraints were self-reported reasons for withdrawal. As approach to handle missing values, we used the full information maximum likelihood estimation in the longitudinal sample. To allow comparability of the paths in the cross-lagged path model, all metric variables were T-transformed (M = 50, SD = 10).
We tested the longitudinal associations between fear of falling and perceived overprotection using a cross-lagged path model with a two-variable three-wave design. As depicted in Figure 1, the cross-lagged path model covers four auto-correlations (βF1F2, βF2F3, βP1P2, and βP2P3), three cross-sectional correlations (βF1P1, βF2P2, and βF3P3) and four cross-lagged correlations (βF1P2, βF2P3, βP1F2, and βP2F3). The following fit indices were used to assess the model fit: Comparative Fit Index (CFI), the Tucker–Lewis Index (TLI), the root-mean-square error of approximation (RMSEA), and the standardized root-mean-squared residual (SRMR). The model was considered to have a good fit if CFI > 0.90, TLI > 0.95, RMSEA < 0.06, and SRMR < 0.09 (Hu & Bentler, 1999; Steiger, 2007). We statistically controlled the model for intervention condition at T2 and T3, respectively. Falls, health-related quality of life, age, and gender were taken into account when there was a significant bivariate correlation with fear of falling or perceived overprotection at T1, T2, or T3. The significant bivariate correlations are displayed in Table 1.
Descriptive statistics and bivariate correlations in the longitudinal sample (n = 310).
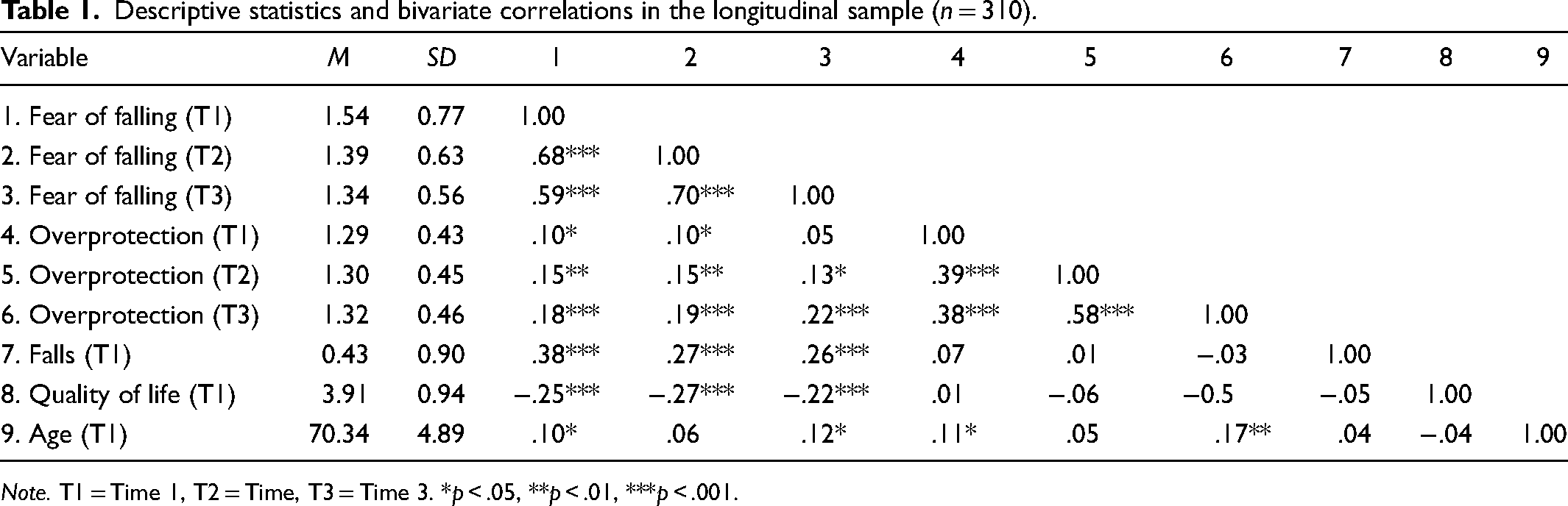
Note. T1 = Time 1, T2 = Time, T3 = Time 3. *p < .05, **p < .01, ***p < .001.
Results
Descriptive Results
Table 1 displays means, standard deviations, and bivariate correlations. Mean values indicate that perceived overprotection remained rather stable across measurement points.
Cross-Lagged Path Analysis
The model fit was good, CFI = 0.99, TLI = 0.98, RMSEA = 0.03, and SRMR = 0.02. At T3, 56% of the variance in fear of falling was explained, as well as 36% in perceived overprotection. At T2, 51% of the variance in fear of falling was explained, and 17% in perceived overprotection. Figure 2 depicts the results of the cross-lagged path model. Focusing on the cross-lagged paths, the paths from fear of falling to perceived overprotection were significant across all assessment points (fear of fallingT1 → overprotectionT2 β = .12; 95% CI [0.02, 0.21], p = .02; fear of fallingT2 → overprotectionT3 β = .10; 95% CI [0.01, 0.18], p = .03) and revealed a positive association. The cross-lagged paths from perceived overprotection to fear of falling were not significant (overprotectionT1 → fear of fallingT2 β = .02; 95% CI [−0.06, 0.08], p > .05; overprotectionT2 → fear of fallingT3 β = .01; 95% CI [−0.06, 0.07], p > .05). Regarding covariates, falls at T1 were positively associated with fear of falling at T1 (β = .36, p = .001) and T3 (β = .10, p = .015). Health-related quality of life at T1 was negatively related to fear of falling at T1 (β = −.22, p = .001) and T2 (β = −.10, p = .01). Furthermore, higher age at T1 showed a positive association with perceived overprotection at T1 (β = .10, p = .036) and T3 (β = .12, p = .007).
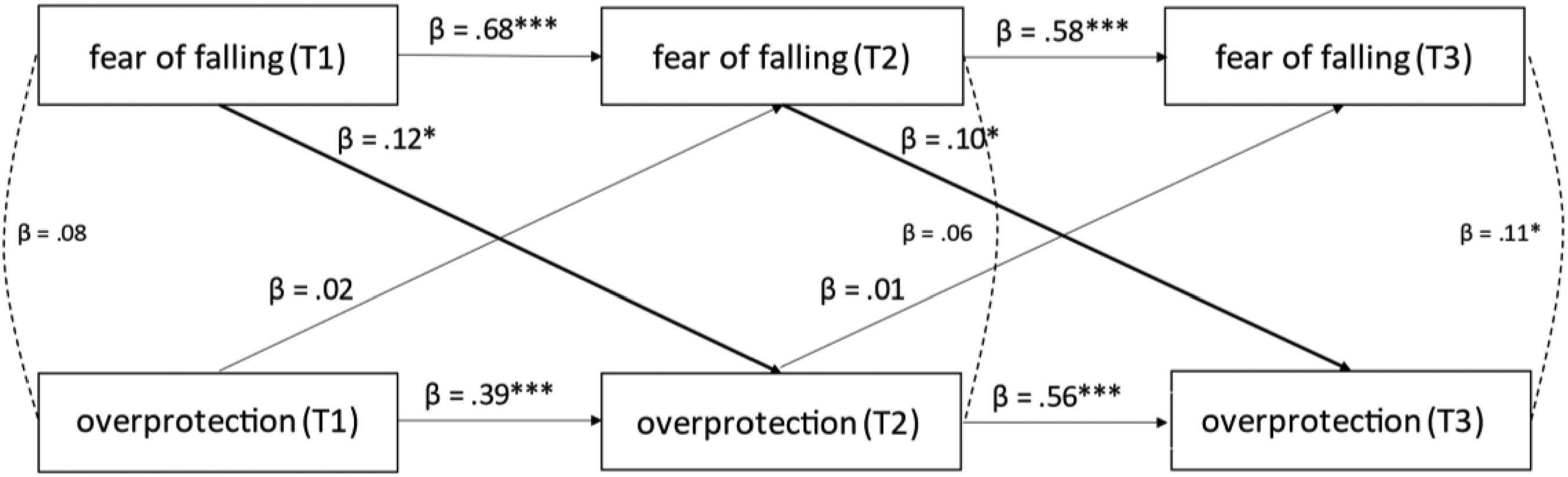
The cross-lagged panel model in n = 310 participants, fear of falling: R2 = .51 at time 2, R2 = .56 at time 3, perceived overprotection: R2 = .17 at time 2, R2 = .36 at time 3.
Discussion
The present study examined the association between fear of falling and perceived overprotection and their temporal order in a cross-lagged path model over three measurement points in time. Higher fear of falling predicted higher levels of perceived overprotection across all assessment points. The hypothesis that the perception of higher overprotection from the social environment carries over into higher fear of falling could not be confirmed for any of the measurement points. Overall, these results do not support the assumption of reciprocity or a downward spiral between fear of falling and overprotection but rather suggest that the individual's fear of falling is transferred to the perception of their social environment, which is perceived as overprotective over time.
These findings are in line with previous research that investigated fear of falling in association with perceptions of autonomy. For instance, a recent study indicates that individuals with higher fear of falling perceive lower levels of autonomy compared to participants with lower fear of falling (Singh et al., 2021). Another longitudinal study among adults with an average age of 65 years supports these findings by showing that fear of falling predicted lower levels of perceived autonomy three years later (Hajek & König, 2020). Our results revealed a positive association between fear of falling and overprotection. Individuals who feel overprotected might feel so because they perceive their autonomy to be restricted by their social environment.
Strengths and Limitations
Our study is among the first to document that older adults’ fear of falling carries over into perceived overprotection by the social environment over time. These findings add new insights to research on fear of falling, as we considered perceived overprotection as psychosocial factor rather than examining fear of falling in association with physical factors. A further strength of the current study is the survey period that comprised three points of measurement over three months.
However, several limitations must be addressed. On the one hand, we had a predominantly female sample. Previous studies showed that women are more likely to experience fear of falling in comparison to men (Hoang et al., 2017; Robert Koch-Institut, 2020). Future research should replicate our results with samples that are better balanced for genders. In contrast to the original scale by Thompson and Sobolew-Shubin (1993), the internal consistency of the overprotection construct was rather low in our study. We measured overprotection with three items of the original scale comprising eight items. In addition, perceived overprotection was assessed regardless of its source and quality. Gallant et al. (2007) showed that unwanted support particularly from family members is perceived as overprotecting as compared to support received from friends. The authors argue that friends might be more discrete, and their overprotective behavior could be refused more easily whereas social interactions with family members are less voluntary and often cannot be avoided. Future studies should also consider the perspective of older adults’ social environment and consider, for example, the perspective of close friends or the partner (e.g., type and quality of provided support, vicarious fear of falling).
Future Research
Based on our results, we cannot answer the question of whether overprotection is maladaptive in the context of fear of falling and increases loss of independence in old age. Cross-sectional studies suggest that overprotection of the social environment is significantly related to lower levels of activation (Bertoni et al., 2022; Sánchez-Garcia et al., 2019). In line with these cross-sectional results, a longitudinal dyadic study on patients surveyed after myocardial infarction revealed that perceiving a partner as overprotective predicted a decline in physical functioning nine months later (Joekes et al., 2007). In contrast, Wolff et al. (2013) investigated the balance of needed and received support and revealed that more support than needed is associated with a lower negative affect among older adults aged 68 and above. Thus, even though overprotection is associated with lower levels of activation and physical functioning it may not result in fear of falling. In addition, perceiving social support as overprotective depends on how older adults perceive their personal capabilities to perform a task without further help: If self-efficacy beliefs are high, receiving unsolicited support may threaten perceptions of autonomy (Warner et al., 2011). Perceptions of overprotective behavior could also be related to fear of dependency which describes older adults’ concern about accepting help from their social environment (Adams-Price & Ralston, 2018). Older adults might perceive social support as overprotective when they experience a higher fear of dependency. Future research should investigate under which conditions older adults perceive social support as being overprotective and when it imposes rather a concern about dependence which reflects a threat to autonomy.
In a study by Spitze and Gallant (2004), older adults reported to have an ambivalent attitude toward receiving assistance. The desire to remain independent competed with the need for support in areas of life that could no longer be handled autonomously. Therefore, it is important to identify forms of support that older adults receive by closer examining the conditions that determine whether it is perceived as positive or negative (Gallant et al., 2007). According to Crombie et al. (2004), a positive way of supporting older adults is to encourage them rather than to overprotect them. The authors demonstrated that encouragement by caregivers helped older adults to overcome fear of falling and to engage in physical activity (Crombie et al., 2004). Thus, supporting older adults’ autonomy can be understood as a positive way of support. Another study examining adherence to physical activity revealed that autonomy support is particularly relevant to older adults (Levy et al., 2008). Autonomy support implies acknowledging older adults’ views, meeting their requests, providing choices, and minimizing control (Williams et al., 2006). Whereas overprotection is described as an individuals’ perception of a social environment that induces dependence, averts stress, and does not interact with them as adults (Thompson & Shobolew-Shubin, 1993). Further elaborating on the fine line between support that not only helps solving the recipients’ problems but also protects their perceived autonomy and self-integrity will enable deducing advice on how to increase the adequacy of assistance from their social environment. Research with interventional designs might help to reduce overprotective behavior and promote an adequate fit of assistance to recipients’ needs.
Implications
Our findings emphasize the importance of investigating fall-related beliefs, as these are associated with perceptions of unwanted support from the social environment. To identify the needs of older adults it is important to focus on their resources instead of their disabilities (Sánchez-Izquierdo et al., 2019) and to acknowledge the ambivalence of dependency on support as well as the need for independence (Gallant et al., 2007). Interventions for caregivers and other members of the social network might raise their awareness of overprotective behaviors and to prevent often unintended restrictions of autonomy. A behavioral intervention comprising a weekly one-hour session over three weeks designed for caregivers showed initial success (Sánchez-Izquierdo et al., 2019). After completing the intervention, caregivers reported significant improvements in promoting autonomy behaviors among older adults (e.g., person-centered care). Another crucial aspect of these interventions may involve emphasizing positive perspectives on aging. When age is seen solely as a phase of cognitive and physical decline, it could limit the possibilities for older adults’ continued growth and development (Kornadt et al., 2019, Wurm et al., 2022). In addition to the social environment's views on aging, negative self-perceptions of aging may also inhibit autonomy in old age. Fear of falling is also associated with negative self-perceptions of aging (Ayalon, 2016) — the observed relationship of fear of falling and perceived overprotection as well as its possible link to loss of autonomy in old age might even be amplified if persons have pronounced negative perceptions of their own aging. For example, a recent meta-analysis points to the longitudinal association of negative self-perceptions of aging and higher physical and psychological impairments (Westerhof et al., 2023), which are known to jeopardize autonomy in old age.
Conclusion
Our study is among the first to document that individuals’ fear of falling carries over into perceived overprotection over time. However, our results do not support the assumption of reciprocity or a downward spiral between fear of falling and overprotection. This shows that social support perceived as overprotection does not always result in lower capability beliefs. It might also be counteracted in terms of a strong will to stay active and independent. Moreover, studies on fear-related beliefs and its potential carryover effects on social interactions are required, possibly also including recipients’ and providers’ perspectives. Future studies in this area might help to find a balance between offering adequate support where needed but at the same time promoting activities that help maintain independence and counteract fears.
Footnotes
Acknowledgments
The authors thank the German Centre of Gerontology and a team of highly motivated student assistants for helping to conduct the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The PREFER II study (Personal Resources of Elderly People with Multimorbidity: Fortification of Effective Health Behavior) was funded by the German Federal Ministry of Education and Research [grant number 01ET1001B].