
Abstract
The objectives of this study were to examine the prevalence of race-based disparities in cognitive problems, functional limitations (FLs), and activity of daily living (ADL) limitations between US Black and White older adults in 2008 and 2017, to explore how age, sex, income, and education attenuate these racial disparities, and to determine if Black–White health disparities are narrowing. Secondary analysis of the nationally representative American Community Surveys including 423,066 respondents aged ≥65 (388,602 White, 34,464 Black) in 2008 and 536,984 (488,483 White, 48,501 Black) in 2017. Findings indicate that Black–White racial disparities were apparent for all three outcomes in 2008 and 2017. Approximately half of the racial disparities was attenuated when adjustments were made for education and income. Racial disparities in cognition declined between 2008 and 2017 (p < .001) but persisted unabated in FLs and ADL limitations. Further exploration on the mechanisms of racial disparities is warranted.
Introduction
Racial disparities in health outcomes are pervasive across the lifespan in the United States (US) (National Center for Health Statistics, 2016). Despite efforts to address such differences among White and Black Americans, adverse health outcomes continue to disproportionately impact Black communities (Thorpe et al., 2016). Research suggests that initiatives to address these inequities have been efficacious. For example, the 2010 Affordable Care Act benefitted people of color substantially by improving their access to care, which should bring them closer to the standard of health of their White counterparts (Buchmueller et al., 2016).
The US is home to an increasingly aging population, with projections of the older adult population growing from 55.7 million in 2020 to 80.8 million by 2040 (Administration of Community Living, 2022). An increase in healthcare expenditure is expected to follow, in part due to rising disability-associated costs (Khavjou et al., 2020). Disability may better predict health and social service use than crude disease measures (i.e., incidence and prevalence) (Jette, 1996). Healthcare costs of persons with disabilities are almost triple that of their nondisabled counterparts (Khavjou et al., 2020). Three major forms of disability among older adults in the US include cognitive impairment, functional limitations (FLs), and impaired activities of daily living (ADLs) (U.S. Census Bureau, 2014).
There are several factors that may influence the development of cognitive impairment in later life. Higher educational attainment is associated with the delay of dementia onset, potentially owing to its role in building cognitive reserve in early life and adulthood (Lövdén et al., 2020). The degree to which this occurs varies across racial groups, with White populations benefitting more than Black populations from higher levels of education (Avila et al., 2021). Greater lifetime stress has also been correlated with poorer cognition in later life (Franks et al., 2021). One study following a small sample of Black Americans and White Americans found steeper declines in episodic memory among Black Americans, noting the disproportionate exposure to, and impact of, adverse life experiences for the Black American sample group (Zuelsdorff et al., 2020). For example, actual and perceived acts of discrimination—known correlates for cognitive decline—are higher among Black populations (Zahodne et al., 2019). This study aims to explore and better characterize these cognitive disparities in response to Manly & Mungas (2015) calls to action urging for efforts to “identify, understand, and reduce disparities in cognitive aging across ethnic, racial, and linguistic groups of older adults” (p. 1).
There has been less research investigating how racial differences manifest in FLs and in limitations in ADLs. FLs are the most common disability among older Americans, with more than 10 million older adults having trouble walking or climbing stairs (U.S. Census Bureau, 2014). A study comparing Black and White Americans with chronic conditions found that FLs onset earlier, progress more rapidly, and occur at a higher prevalence for Black Americans than White Americans (Kail et al., 2020). Another study using self-reported disability in ADLs found a higher incidence of FLs and impaired ADLs among Black individuals in comparison to White individuals (Liang et al., 2010).
While some studies indicate that racial disparities in disability persist independent of indicators like education (Avila et al., 2019), others suggest that the disparities are largely mitigated following adjustments for socioeconomic status (Goyat et al., 2016; Fuller-Thomson et al., 2009). There is a need for further research to examine the effects of education and socioeconomic status on racial disparities in disability, and to determine whether these disparities are declining. The theoretical underpinnings of this research is an intersectional framework that suggests that both class and race simultaneously influence the health and well-being of older Americans in a compounded manner (McAlpine et al., 2022; Moore-Berg & Karpinski, 2019; Moore-Berg & Karpinski, 2021).
Ultimately, racial disparities in health are associated with heightened morbidity among communities of color (Gee & Ford, 2011; Quiñones et al., 2019). With the added burden of age-related disabilities, it is important to explore how these issues intersect to affect the US older adult population.
This study aims to: (a) identify race-based disparities in cognitive impairment, FLs, and ADL limitations between US Black and White populations in both 2008 and 2017, (b) explore how other factors known to be predictors of disability—sex, income, and educational attainment—attenuate these outcomes, and (c) evaluate whether the magnitude of Black–White health disparities has decreased between 2008 and 2017. This study provides insight on trends in age-related disability prevalence when demographic (race and sex) and socioeconomic (education and income) factors are considered.
Methods
Sample
Data from the 2008 and 2017 waves of the American Community Survey (ACS) were used. Conducted by the United States Census Bureau, the ACS surveys a representative sample of individuals monthly to generate annual estimates. As has been described elsewhere (Fuller-Thomson & Ahlin, 2022; Fuller-Thomson, Ferreirinha & Ahlin, 2023), response rates were 98% in 2008 and 94% in 2017 (U.S. Census Bureau, 2019). Our sample was restricted to those aged 65 and older. The sample size was 423,066 (388,602 non-Hispanic White; 34,464 non-Hispanic Black) in 2008 and 536,984 (488,483 non-Hispanic White; 48,501 non-Hispanic Black) in 2017. The ACS sample includes individuals living in the community and group quarters (including nursing homes) and offers a nationally representative sample of older adults (≥65 years).
Study Design
Secondary analysis of two cross-sectional nationally representative surveys (ACS 2008 and ACS 2017).
Measures
The 2008 and 2017 iterations of the ACS use the same close-ended (yes/no) questions to gauge impairments in cognition (“Because of a physical, mental, or emotional condition, does this person have serious difficulty concentrating, remembering, or making decisions?”), FLs (“Does this person have serious difficulty walking or climbing stairs?”), and ADLs (“Does this person have difficulty dressing or bathing?”). These questions were identical for those living in the community and institutionalized settings. Surveys were completed independently by capable respondents, or by caregivers or nursing home staff members.
Sex was based on self-report (male, female). To generate prevalence estimates for bivariate analyses, age was categorized in 10-year periods (i.e., 65–74; 75–84; ≥85). In the logistic regression analyses, age was entered by each year categorically (except for those over age 95, who were top coded as 95+) with age 65 as the reference category. Treating each year of age categorically was done to address the nonlinear relationship between age and disabilities. Race and ethnicity were used interchangeably and indicate whether the respondent reported they were non-Hispanic White or non-Hispanic Black (hereafter referred to as White and Black).
For educational attainment, the ACS asks, “What is the highest degree or level of school this person has completed?” with the following categories: no schooling, some schooling but less than Grade 3 completed, then each year of education completed from Grade 3 through Grade 11, Grade 12 but no diploma, Grade 12 regular high school diploma, General Education Diploma (GED), some college but less than 1 year, 1 or more years of college but no diploma, associate's degree, bachelor's degree, master's degree, professional degree, and doctorate. All the above categories were entered categorically in the logistic regression analysis with doctoral degree as the reference category. Inclusion of this level of granularity in education was important for the logistic regression analysis because education is one of the factors most strongly associated with cognition and health outcomes. For clarity of presentation in the bivariate analyses, education attainment was grouped into five categories (no high school diploma, high school diploma or GED, associate's degree, bachelor's degree, Master, and/or doctorate degree).
The ACS measures an individual's household poverty status by comparing a household's total income against a predetermined income poverty threshold for households of that size and composition. The income variable was categorized into the following (<poverty line, 100–199%, 200–299%, 300–399%, 400–499%, 500% and more of the poverty line, and a missing data category).
Data Analysis
Descriptive analyses were provided, including unweighted frequencies and weighted percentages comparing the profile and prevalence of the three aforementioned disabilities among Black versus White older adults in 2008 and in 2017. Chi-square tests were reported.
Odds ratios (ORs) and 95% confidence interval (CI) of cognitive impairment, FLs, and ADL limitations were generated for Black versus White respondents using the 2008 ACS. Four separate logistic regression analyses were conducted for each of the three disability outcomes as follows: (a) unadjusted; (b) adjusted for age and sex; (c) adjusted for age, sex, and education, and (d) adjusted for age, sex, education, and income. These analyses were repeated with the 2017 ACS data. A p-value less than .05 was considered statistically significant.
To determine if the Black–White odds of each disability narrowed, widened, or remained consistent across the time period, an interaction term (year of data collection by race) was added to the logistic regression analyses including both the 2008 and 2017 data. Although the three logistic regression analyses are not shown, the p-value of the interaction terms for each of the three disabilities is reported.
All analyses were completed using IBM SPSS-26 (IBM Corp, 2019). All sample sizes are presented in their unweighted form. All analyses including prevalence, ORs, 95% CIs, and p-values were generated using a normalized weight by dividing the value of each respondent's statistical weight by the mean weight of the sample. The use of normalized weights is a widely accepted standard statistical method to correct for nonresponse bias while maintaining the original sample size (Hahs-Vaughn, 2005).
Results
As shown in Tables 1 and 2, the difference between Black and White respondents was statistically significant (p < .001) for cognitive impairments, FLs, and ADL limitations at both time points (2008 and 2017). Black respondents consistently had a significantly higher prevalence of each of these disabilities in comparison to White respondents. All other characteristics examined (i.e., age, sex, education, and income) were also statistically significantly different between Black and White respondents at both time points.
Sociodemographic and Health Characteristics of Non-Hispanic Black Versus Non-Hispanic White Respondents Age 65 and Older in the 2008 American Community Survey.
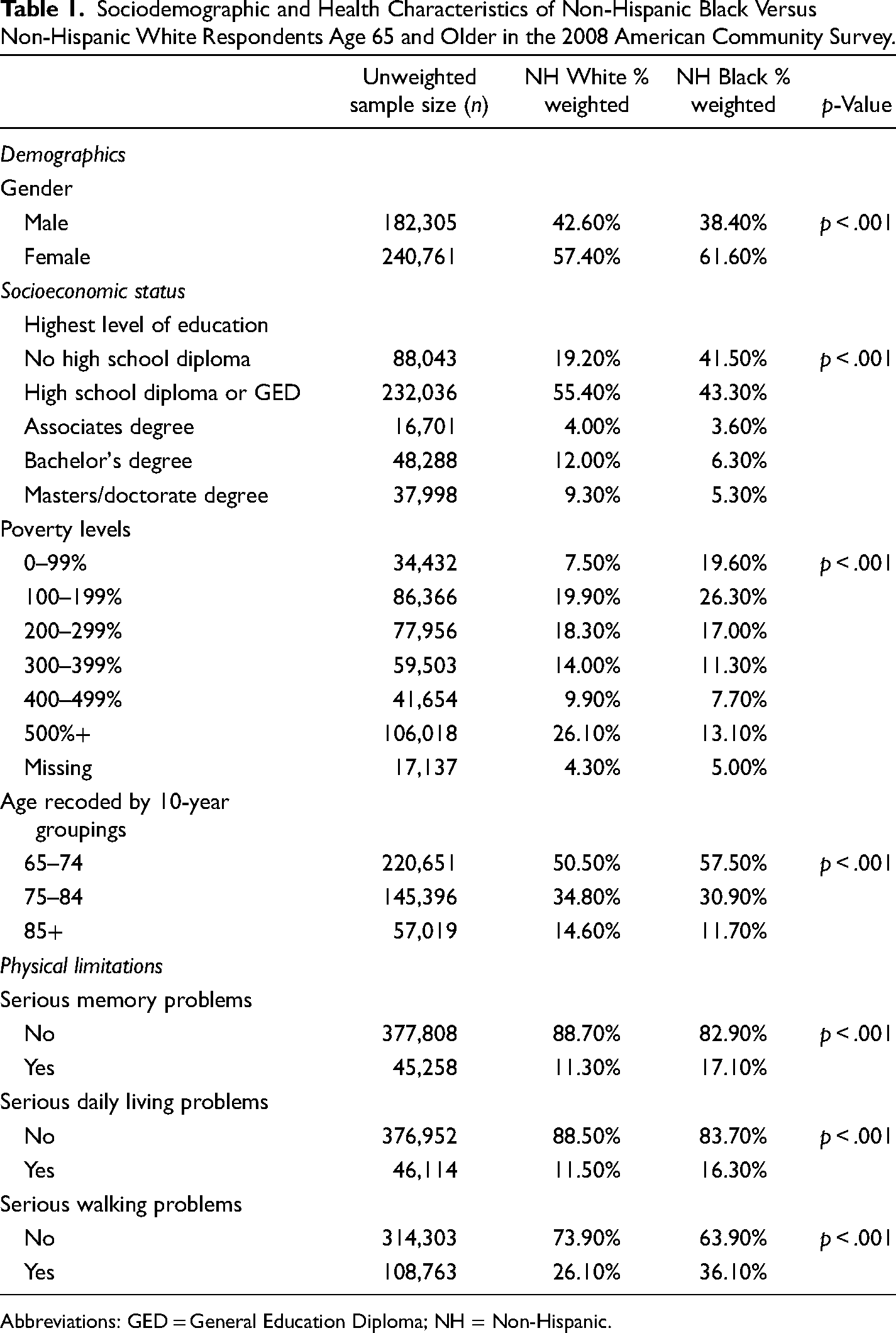
Abbreviations: GED = General Education Diploma; NH = Non-Hispanic.
Sociodemographic and Health Characteristics of Non-Hispanic Black Versus Non-Hispanic White Respondents Age 65 and Older in the 2017 American Community Survey.
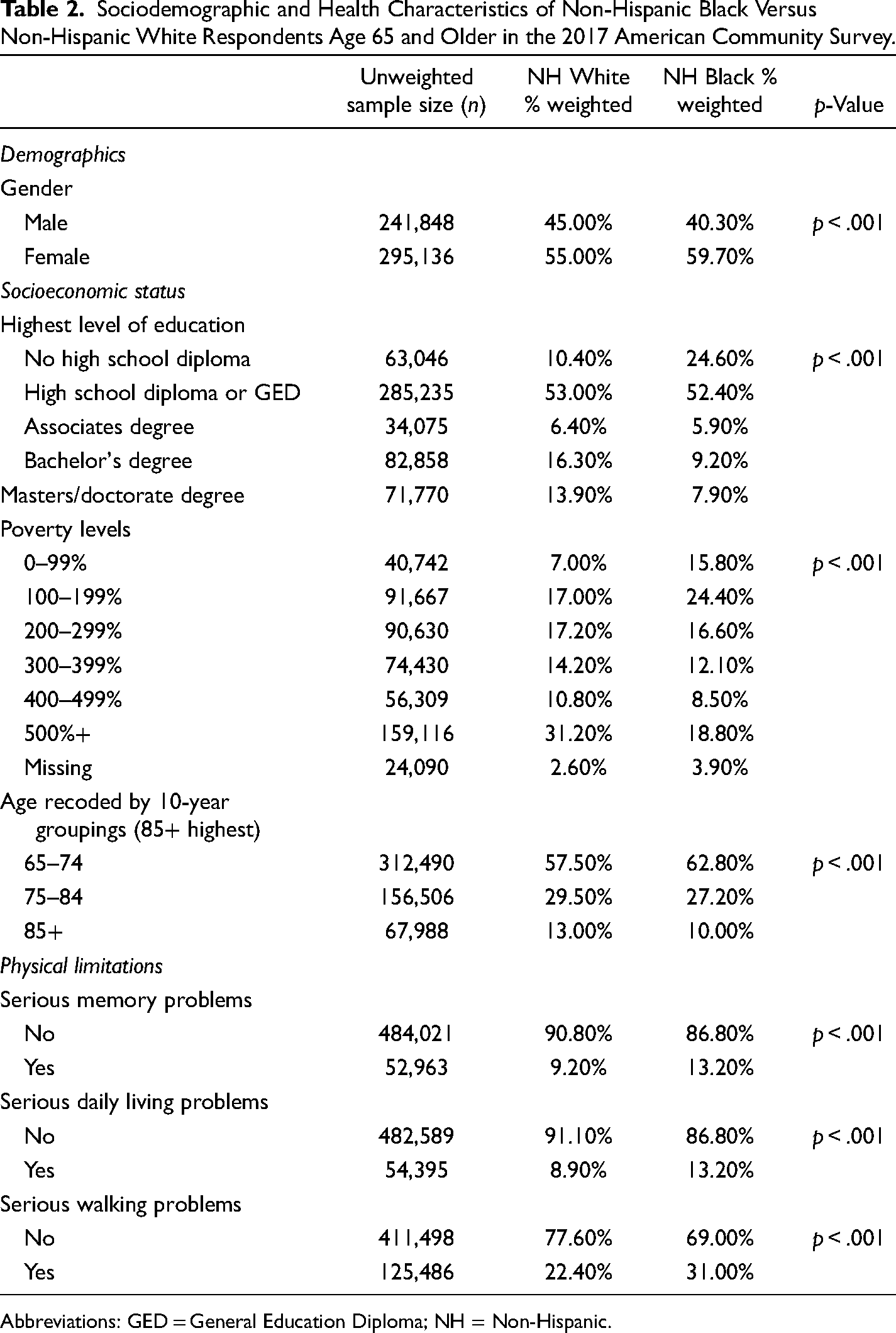
Abbreviations: GED = General Education Diploma; NH = Non-Hispanic.
In analyses not shown, we calculated the chi-square tests within each race to determine if the change over time was statistically significant. The prevalence of cognitive impairments, FL, and limitations in ADL declined significantly (p < .001) within each race over the decade (e.g., the decline from 2008 to 2017 in the prevalence of cognitive problems among White respondents from 11.3% to 9.2% and from 17.1% to 13.2% among Black respondents, respectively, was statistically significant.)
To determine the degree to which Black–White disparities in the odds of each type of disability are attenuated once age, sex, education, and income were taken into account, we conducted logistic regression analyses, shown in Table 3. For each of the three outcomes and at both time points, inclusion of the above-mentioned factors partially attenuated the association, but a significant racial disparity remained. The age–sex adjusted ORs ranged from 1.70 to 1.89, while the age–sex–education–income OR ranged from 1.29 to 1.42. Inclusion of education level provided the greatest attenuation of the association between Black–White disparities and each of the three disability outcomes.
Odds Ratios and 95% Confidence Interval (CI) of Cognitive Problems, Functional Limitations, and Limitations in Activities of Daily Living for Non-Hispanic Black Versus Non-Hispanic White Respondents Using the American Community Survey (ACS) 2008 and 2017, Including Community Dwelling and Institutionalized Older Adults.
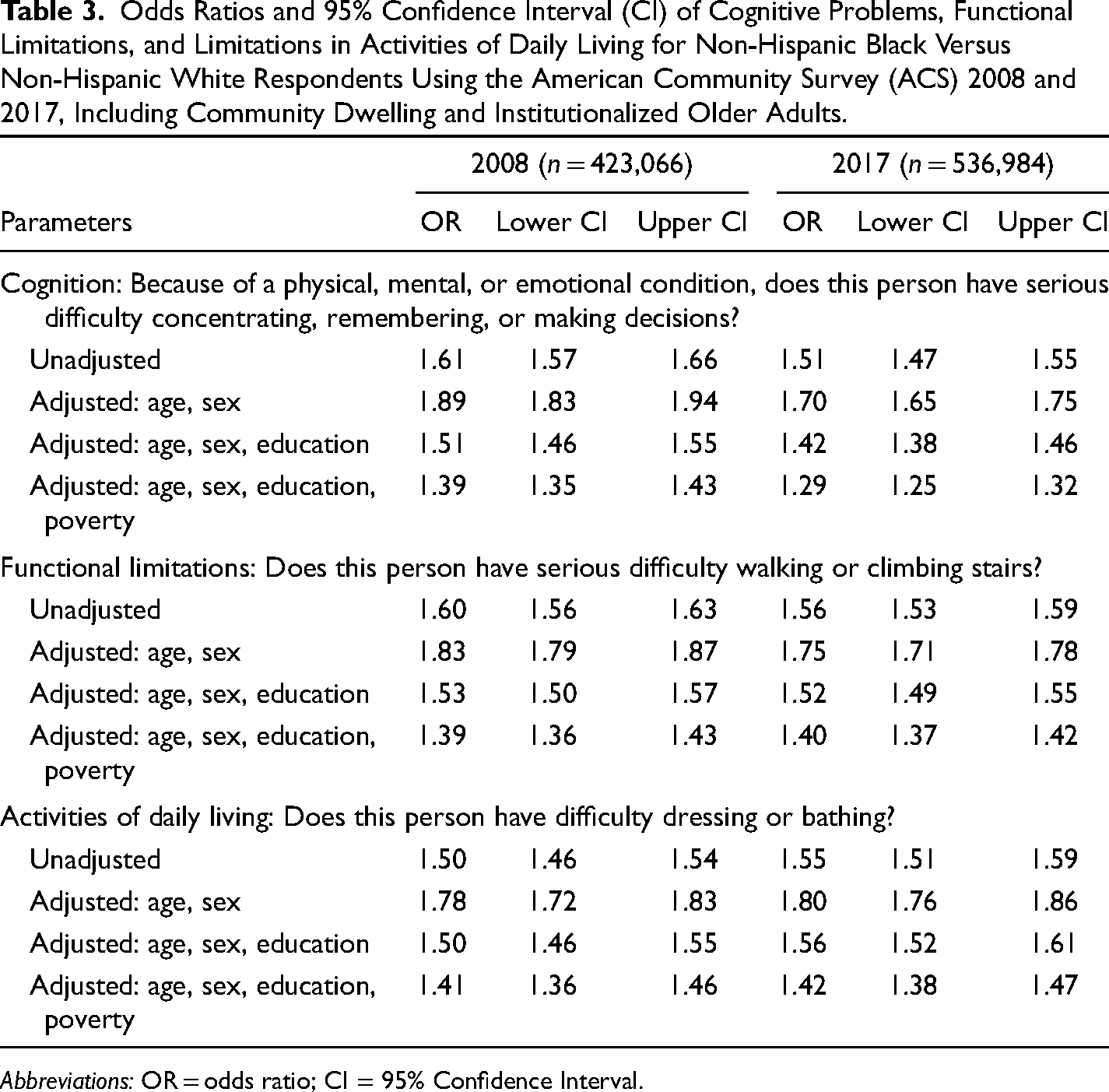
Abbreviations: OR = odds ratio; CI = 95% Confidence Interval.
A major question of interest is whether the racial disparity narrowed, widened, or stayed the same between 2008 and 2017. The interaction between race and year of data collection was statistically significant for serious memory problems (p < .001), indicating that the magnitude of the disparities between Black and White Americans for this condition had significantly narrowed over the decade.
In contrast, the race-by-year of data collection interaction effects were not statistically significant for ADL limitations (p = .53) nor FLs (p = .13), indicating that the magnitude of the Black–White disparities did not change between 2008 and 2017 for either of these limitations.
Discussion
The findings of this study provide robust evidence that Black–White racial disparities in disabilities among older adults were present in both 2008 and 2017.
Over the decade, racial disparities in cognitive impairment declined significantly, from 39% higher odds to 29% higher odds of cognitive impairment for Black older adults compared to White respondents, once age, sex, education, and income were considered. Racial disparities persisted unabated in FLs and ADL limitations between 2008 and 2017.
In this study, racial disparities were substantially attenuated when education and income were accounted for. In both 2008 and 2017, half of the observed disparities across all three disability measures were attributable to socioeconomic disadvantage. That is, much of the difference in the odds of self-reported cognitive impairment, FLs, and limitations in ADLs between Black and White respondents can be explained by the former having less education and lower income, on average, than the latter.
That socioeconomic factors account for such an appreciable portion of racial disparities is unsurprising. Previous research has found that higher educational attainment and occupational cognitive demands are strongly correlated with better cognition, greater cognitive reserve, and reduced dementia risk in older adulthood, with its effects tied to education quality (Brewster et al., 2019). Higher educational attainment is also associated with better grip strength, a proxy for physical frailty, and hence, disability status (Ihle et al., 2017). Education and income are closely related; lower education levels tend to restrict individuals to entry-level or blue-collar positions, employment with lower wages, less job security, and increased precarity (Ihle et al., 2017). Such occupations may also be more deleterious to one's long-term health due to increased physical demands, contributing to later life disability. Probable mechanisms underlying this relationship beyond occupational factors include lifestyle risk factors, healthcare access and level of use, and physiological responses to stress. Importantly, educational attainment does not always translate into occupational outcomes. For example, despite educational achievements, Black men dealing with racial discrimination reflective of systemic inequities may face barriers to occupational or professional advancements (Lövdén et al., 2020).
Members of older cohorts were likely educated during segregation (in place until 1954) and the years following desegregation, calling into question the quality of education received by Black respondents compared to their White counterparts (Avila et al., 2021). Thus, differences in access to quality education may indicate that similar education levels among Black and White respondents may not be truly equivalent. Notably, unequal quality of, and access to, education remains a reality in the US, with students of color and those facing poverty being disproportionately disadvantaged (Darling-Hammond, 1998; Gee & Ford, 2011). Against the background of present-day disparities in education, this finding indicates that concerted efforts to improve education outcomes for Black Americans, such as raising high school completion rates and increasing access to postsecondary education, are a promising avenue to explore to potentially promote further reductions in cognitive disparities.
Overall, general improvements in the prevalence of cognitive impairment, FLs, and ADL limitations among older adults are promising from a population health perspective. However, with limited progress made to address racial disparities between Black and White Americans, this area continues to require attention and appropriate intervention. Importantly, interventions such as Obamacare (also known as the Affordable Care Act), which had higher uptake in Black Americans, were expected to help narrow racial disparities. However, due to an appreciable period of latency for the development of disabilities, even if Obamacare is found to make a difference, it will likely be years, if not decades, until the tangible benefits of these improvements may become apparent with respect to disability outcomes in older adults.
These findings highlight the importance of considering the intersectionality of class and race, rather than overemphasis on either category when identifying and subsequently addressing disparities. Closing the racial gap related to education and economic opportunities may also provide long-term benefits in reducing racial health disparities in later life as well as reducing economic disparities earlier in life. We hypothesize that racial disparities in disability in older adulthood may be curbed to an appreciable degree by earlier-life interventions to improve education and standard of living. These are targetable and achievable goals. Though there remains much to do, providing such initiatives are promising strategies to reduce health inequities.
Racial disparities in cognition narrowed between 2008 and 2017, even after education and income were considered, suggesting that factors other than socioeconomic characteristics may be playing a role. We hypothesize that greater improvements in air pollution exposure and cardiovascular risk factors among Black versus White respondents may be relevant. Both White and Black Americans experienced improvements in the prevalence of cognitive problems across the decade, but it appears that the improvements were more substantial among Black older adults in comparison to their White peers.
Differential exposures to environmental toxins may also help explain some of the decline in disparity. For example, lead is a known neurotoxin, with high levels of exposure associated with cognitive decline. In the late 1970s, 23% of Black Americans had blood lead levels above 20 μg/dL compared to 14% of White Americans (Pirkle, 1994). Although the phase-out of leaded gasoline in the USA beginning in the 1970s reduced the overall population's exposure to environmental lead, it would have led to greater reductions among Black Americans in comparison to White Americans. Further, exposure to pollutants from emissions such as fine particulate matter (PM) can have neurodegenerative effects on older adults (Block et al., 2012). A study following a cohort of older American women found that those living in areas with PM2.5 levels higher than the approved standard had an 81% and 92% increased risk of developing global cognitive decline and all-cause dementia, respectively (Cacciottolo et al., 2017). One study found that the racial disparities in residential proximity to PM-emitting facilities (used as a proxy for exposure) disproportionately impacted Black Americans, who shouldered a PM2.5 burden 1.54 times higher than the population average (Mikati et al., 2018). This pattern was consistent nationally across most states and counties and was more pronounced than the poverty-based disparity (1.35 times higher than the average). Although absolute PM2.5 burden declined for all subgroups under consideration, proportional burdens remained (Mikati et al., 2018). This could be another contributing factor for which despite an observed decline, racial disparities in cognition continue to endure.
Changes in the prevalence of known cardiovascular risk factors associated with dementia (such as hypertension, smoking, and stroke incidence) may also contribute to the observed decline in disparity in cognition (Leritz et al., 2011). One study examining trends in Black–White disparities in heart disease mortality between 1968 and 2015 found that while both groups experienced decreases in mortality, the rate for Black Americans was slower (Van Dyke et al., 2018). It is not until 2005 when the Black–White mortality ratio began to steadily decrease annually by 0.7% (Van Dyke et al., 2018), which is in keeping with our observations in this study demonstrating a decrease in disparity in cognition during a similar timeline. Further research is needed to determine which factors are influencing this beneficial trend in reduced racial disparities in cognitive problems among older adults, and to explore how to further accelerate these improvements.
Racial disparities persisted unabated in FLs and ADL limitations. In contrast to the improvements evident in racial disparities related to cognitive problems, Black–White disparities in functional and ADL limitations saw no improvement across the decade examined in the current study. While the prevalence of such limitations decreased overall within each racial group, the rate of improvement was comparable between the races and thus, the disparities between Black and White Americans did not decrease during the study period. This finding has important implications for quality of life in older adulthood and is consistent with reports that Black Americans spend more of their lives with disabilities than their White peers (Crimmins & Saito, 2001).
One of the reasons for this observation could be due to disease burden. The presence of comorbidities drives disability development, with more health conditions contributing to higher rates of disability. Black Americans are more likely to have higher rates of chronic diseases than their White counterparts, such as diabetes, cardiovascular disease, hypertension, and malignant cancers, all of which contribute to mobility limitations (Bakk et al., 2017; Owens et al., 2021; Verbrugge et al., 1989). Also, these two forms of disability are closely related, since FLs may precede ADL limitations, resulting in older adults with progressively worsening FLs subsequently developing ADL impairments (Barnes & Bennett, 2014).
Differences in self-reporting may also contribute to this finding. The ACS relies on self-reported measures, and perceived disability is influenced by an individual's social context. Access to assistive devices and features of the built environment such as home modifications, which are known to differ across racial and socioeconomic groups, may influence respondents’ self-perception of their disability status (Bakk et al., 2017). Respondents with access to assistive devices are less likely to perceive themselves as disabled. The impact of disease burden compounded with inaccessible physical environments often causes worsening morbidity over time. This is known to disproportionately impact older Black Americans due to the increased likelihood of experiencing poverty, limiting their ability to modify their home environments accordingly or to live in communities with accommodations that meet their health needs (Owens et al., 2021).
Further, communities of color are more likely to have lower health literacy, receive poorer quality care, and are less likely to have private insurance (Buchmueller et al., 2016; Egede, 2006; Eichner & Vladeck, 2005). Therefore, Black older adults may have less access to primary disease prevention and may experience suboptimal care of their chronic diseases (Population Reference Bureau, 2021). Following injury, hospitalization, or any process that may increase frailty, rehabilitation can be restorative to an older adult's health. However, access to rehabilitation via physical therapy is often restricted to individuals with private insurance. One study examining an Ohio community found that medically underserved adults faced a host of barriers in accessing physical therapy services (McCallum, 2010). Similarly, a national study investigating physical therapy access following rotator cuff surgeries found that patients relying on Medicaid insurance had significantly more difficulty accessing these services than those with private insurance (Rogers et al., 2019).
This outcome is consistent with previous research that found even following adjustments for factors associated with disability and race (e.g., age, gender, comorbidities, and health behaviors), older Black Americans fare worse than their White counterparts at all stages of the disablement process that sees disease eventually progress to disability (Ostchega et al., 2000; Kelly-Moore & Ferraro, 2004). Thus, although not accounted for here, there are a complex set of interrelated issues to be considered in future literature examining racial disparities that go beyond socioeconomic differences. Examining how access to opportunities, social networks and support, occupational factors, exposure to pollution, differences in nutrition, systemic racism and discrimination-related stress, neighborhood social and material disadvantage and social segregation, and other interrelated factors could help further clarify the relationship between SES and disability (Population Reference Bureau, 2021).
Limitations
The questions used to determine the outcome of all three categories of disability were based on self or proxy report using a binary outcome (yes/no) and not upon more objective measures such as a medical examination or review of medical charts. This is major limitation of the study. Future research would benefit from the use of medical charts. However, it is important to note that these disability questions have great relevance nationally and are used to guide US Federal policy in order to “identify vulnerable populations that may be at disproportionate risk of experiencing limitations in health care access, poor health quality, and suboptimal health outcomes.” These items are also used federally to identify “housing needs of disabled persons. State and Local government grantees receiving formula block grant funds from the Community Development Block Grants, HOME Investment Partnership Program, Emergency Solutions Grant and Housing Opportunities for Persons with AIDS programs, are required by law to report these needs.” They are also used “for transit service planning, where some geographic areas may need to be targeted for special public transportation service such as para-transit service” (U.S. Census Bureau, n.d.). Thus, understanding how the Black-White disparities have narrowed (or not!) over the decade is relevant to program administrators and policy designers.
There are important limitations to the use of racial categories in research. While race is often conflated with ethnicity, even in the ACS, individuals may belong to multiple racial categories, making it more difficult to interpret the effects of race on outcomes in research (Egede, 2006). For the purposes of this paper, the analyses were restricted to respondents who identified as solely Black or White. Also, while people of color typically report greater morbidity (Egede, 2006), it is impossible to draw conclusions about the degree of impairment experienced by each group because the measures of disability are binary outcomes (yes/no). Furthermore, the ACS data did not provide information on sexual orientation, which is another important social categorization that may contribute to discrimination and disadvantage, and therefore we are missing a key element in the intersectionality framework. Future research should address this limitation.
The means through which the ACS is disseminated (i.e., by mail or by phone) exclude individuals without stable housing. This may not impact this study to a great extent since the proportion of older adults experiencing homelessness is low given social safety nets (e.g., older adults’ subsidized housing, Medicaid, Social Security, and Supplemental Security Income) and an unfortunately low life expectancy (<65 years) for individuals who are homeless (National Coalition for the Homeless, 2009). It is however important to consider for future studies as more older adults are expected to be among those experiencing homelessness as time progresses.
Implications for Research, Practice, and Policy
Study outcomes have implications on the direction of future research on this topic. Mainly, further exploration is warranted to determine the mechanisms underlying racial differences in disability among older adults. This will inform how interventions can be tailored to account for intersectionality among older adults, especially given the impacts of structural racism, economic oppression, and other forms of injustice that may be compounded. While this study focuses on White and Black populations, there are several other racial groups in the United States for which trends in disability prevalence should be investigated in future studies. Examining within-group differences (e.g., geography, ethnicity, and immigration status) among racial groups may facilitate more appropriate characterization of subgroups of older adults at higher risk of disability, so that focused interventions may be developed. These groups can be prioritized in older adulthood and in earlier life stages to proactively reduce inequities that manifest in older adulthood. Finally, outcomes from this study present a unique opportunity to explore how the inequities of racism, sexism, ageism, ableism, and economic oppression converge to impact population health, and underline the lack of substantial progress attained in recent years in FL and ADL prevalence. Greater understanding of the reasons why progress was seen in decreasing cognitive health disparities among Black versus White older Americans is an important topic for future research.
Footnotes
Acknowledgments
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.