
Abstract
It is unclear whether racial or nativity health disparities exist among older Canadians and what social and economic disadvantages may contribute to these differences. Secondary analysis of data collected from respondents aged 55 and older in the Canadian General Social Survey 27 was performed. The outcome variable was self-reported physical health. Compared to racialized immigrants, white immigrant and Canadian-born respondents had approximately 35% higher odds of good health. Among racialized older adults, the odds of good health were better if they were younger than 75, more affluent, better educated, had a confidant, had not experienced discrimination in the past five years, and were more acculturated. Racialized immigrants are at a health disadvantage compared to white groups in Canada; however, greater acculturation, social support, and lower experiences of discrimination contribute to better health among racialized older adults.
Fifty years ago, only 2% of Canadians were racialized individuals (Statistics Canada, 2013). By 2016, more than one in five Canadians (22.3%) were from racialized groups, representing 7.67 million Canadians, a 15-fold increase since 1971 (Statistics Canada, 2019c). Of the 1.4 million racialized Canadians aged 55 and older in 2016, 96% had been born abroad (Statistics Canada, 2019c), and the majority had arrived in Canada as adults. Some of these older adults arrived as immigrants while others were forced to flee their home countries as refugees. Health research, to date, has not well examined the intersecting identities of racialized status and immigrant or refugee status among older adults in Canada. Existing research tends to focus on newly arrived younger immigrants and refugees and fails to examine how these groups fare later in life. It is unclear whether racial health disparities exist among older Canadians, and whether these differences derive from socioeconomic disadvantage, discrimination, immigration status, inadequate social support, English or French language proficiency, and/or acculturation.
This study is informed by two quite divergent theoretical frameworks: the Healthy Immigrant Effect (HIE) and the intersectionality framework. For immigrants, there appears to be a HIE such that those who migrate tend to be healthier than individuals born in Canada (Kennedy et al., 2015), and this appears to be the case for both white and racialized immigrants. A 15-year prospective study of 2.57 million Canadians from the 1991 census showed strong evidence of a HIE with respect to age-adjusted mortality (Omariba, 2015). Canadian immigrants were studied as a group and separate analyses were conducted for South Asians, Chinese, Vietnamese, and Western Europeans immigrants. When compared with their Canadian born peers, each of these four immigrant groups and the overall grouping of immigrants had significant lower mortality risk in total premature, unavoidable, and avoidable mortality. However, research has also suggested that as the length of time in Canada increases, there is an attenuation in the magnitude of the health advantage experienced by immigrants (De Maio & Kemp, 2010; Subedi & Rosenberg, 2014). Unfortunately, the HIE has seldom included the role that identity factors, such as discrimination or refugee status, play in health outcomes post-migration.
Conceptually, an intersectionality framework (Crenshaw, 2018), which highlights the need to consider multiple overlapping and intersecting identities as potential sources of discrimination, can shed important light on health disparities (Wiebe, 2015). Individuals may be placed at a disadvantage and/or discriminated against because of their race, immigrant or refugee status, English or French language proficiency, accent, gender, and/or socioeconomic position (Wiebe, 2015). These simultaneous but distinct identities may influence health status. Older adults may have had many decades of exposure to the discrimination associated with these social positions, and the accumulation of this disadvantage may be more evident in their current health status when compared with younger individuals, who have had fewer years of exposure to the pernicious effects of discrimination (Dannefer, 1987).
Although the HIE framework suggests there is often a health advantage among immigrants, the intersectionality framework hypothesizes that there may be a health disadvantage among racialized immigrants due to experiences of discrimination. It is important to ascertain the experiences and health of racialized immigrants and refugees coming to Canada, to better inform health providers of unmet needs, and to explore the validity of these competing theoretical frameworks.
A refugee is a person who is forced to flee their country of origin due to fear of harm or punishment based on their religion, race, political views, social group membership, or nationality (Immigration and Refugee Protection Act, 2001). Comparatively, immigrants arrive in Canada under two different programs, categorized as: (1) economic class (e.g., worker and business programs, provincial and territorial nominees); or (2) family class (Statistics Canada, 2019b). The eligibility of economic class immigrants is determined by a point system that takes into account the applicant's English or French language ability, age, education, and employment experience (Government of Canada, 2019). All immigrants and refugees in Canada are also required to complete the Immigrant Medical Exam, which screens newcomers for potential medical inadmissibility for health conditions that may cause an excessive burden on the health care system (Gushulak & Williams, 2004). For refugees, but not immigrants, there is an exemption to “excessive demand regulations” where refugees are permitted to remain in Canada regardless of excessive health problems (Gushulak & Williams, 2004). Therefore, it may be that refugees have, on average, more physical health problems when they arrive in Canada in comparison to other immigrants. Furthermore, any disparity in health status between refugees and immigrants may be partially due to the fact that many refugees experience severe persecution, physical harm, and/or incarceration premigration (Yun et al., 2016).
Canada welcomed over 28,000 refugees in 2018 (UNHCR, 2018), and over 300,000 immigrants in 2018/2019 (Statistics Canada, 2019a). Sociodemographic characteristics of refugees often differ from other immigrant groups. For example, refugees are much less likely to hold a university degree compared to economic or family class immigrants (<20%, 81%, and 34%, respectively) (Prokopenko, 2018). In comparison, 28.5% Canadian-born individuals, aged 25–64, reported having a bachelor's degree or higher (Statistics Canada, 2017a). Further, the analyses of employment data show that among refugees, men have higher rates of employment than women. For example, when employment five years after arrival was examined, men from 10 of 13 source countries had greater than 60% employment compared to women from only 4 of the 13 countries (Picot et al., 2019). Additionally, refugees are 40% more likely than other immigrants to live in poverty during their first year in Canada and are 12% less likely to leave poverty in subsequent years in comparison to immigrants (Picot et al., 2008). Although there is a wide variation in earnings among refugees depending on country of origin, after 15 years in Canada refugees were still at a disadvantage, earning between 35% and 90% of the income of economic immigrants (Picot et al., 2019). Finally, the majority of recent refugees in Canada are married or common-law and living with dependent children, as is the case with economic and family class immigrants (Prokopenko, 2018). The majority of Canadian-born individuals (∼75%) are living married or common law (Statistics Canada, 2019d), but just over one half (51.1%) of these couples are living with dependent children (Statistics Canada, 2017b).
To date, research findings on the health of refugees have been inconsistent. Over the past decade, research has noted poorer health (Marshall et al., 2016; Taylor et al., 2014) and more limited health care access (McKeary & Newbold, 2010; Tuck et al., 2019) of newly arrived refugees. In contrast, a Canadian systematic review in this area reported a health advantage for all-site cancer and mortality from chronic diseases (e.g., heart disease, diabetes, respiratory conditions, etc.) among refugees, compared to the Canadian born (Vang et al., 2015). A health advantage among refugee women, but not men, was found for health conditions such as back pain, high blood pressure, migraines, ulcers, arthritis, and asthma when compared with Canadian-born individuals (Lu & Ng, 2019). The Canadian study also found that the odds of chronic health conditions, such as diabetes, cancer, Crohn's disease, and heart disease, were comparable for refugees and those born in Canada (Lu & Ng, 2019). Given these discrepant findings, there is a need for more population-based research on the long-term health outcomes of refugees as they age in Canada and an improved understanding on how their outcomes compare to other immigrants (Gabriel et al., 2011).
In Canada, racialized groups may experience greater physical health disadvantages. One Canadian study investigated health differences among Caribbean Black and non-Black individuals living in Canada in relation to Canadian-born white and racialized individuals and found that reported diabetes, hypertension, and cardiovascular disease was most prevalent among those of Caribbean origin compared to Canadian-born whites (Lacey et al., 2021). Further analysis also revealed that ethnic and racial minority groups had a greater risk for any cardiovascular disease (e.g., diabetes, stroke, heart disease, hypertension) than their white Canadian-born counterparts (Lacey et al., 2021). Participants who were Caribbean non-Black were also more likely to rate their health as poor, in comparison to white Canadians (Lacey et al., 2021). Additionally, in a Canadian survey that included individuals with histories of cancer, it was found that racialized individuals were significantly more likely to self-report poorer health as compared to white respondents (Abdel-Rahman, 2021).
Social support, discrimination, and other social determinants may impact the health of older adults across the life span. Compared to Canadian-born individuals, refugees may experience a higher prevalence of social isolation and loneliness, which are factors associated with poorer physical and mental health outcomes (Johnson et al., 2019). A recent large study of Canadians aged 45 and older found that refugees were much less likely than immigrants and those born in Canada to have a confidant, someone to advise them in times of crisis, and someone to show them love and affection (Lin et al., 2020). In addition, a study using data from the 2009 General Social Survey (GSS) found that among the 15% of respondents who had experienced discrimination in the past five years, the most common form was based on race or ethnicity/culture (Du Mont & Forte, 2016). Experiencing discrimination was significantly associated with poorer self-reported health (Du Mont & Forte, 2016). The authors also found that there was poorer health among those who indicated experiencing discrimination during health care access (Du Mont & Forte, 2016).
The current study aims to examine whether race or immigrant or refugee status is independently associated with self-reported health status among middle-aged to later life Canadians. Our first aim is to determine whether racialized immigrants differ significantly in self-reported health from other groups in Canada. In this paper, we seek to determine whether refugees and Canadian-born individuals who are racialized differ in respect to their self-reported health compared to racialized immigrants. We also examine whether whites in all groups (immigrants, refugees, and Canadian-born) differ in their self-reported health compared to racialized immigrants. Our second aim is to examine the factors that are associated with self-reported health among racialized Canadians in mid to later life. To this end, we will assess the independent contributions of refugee or immigrant status, gender, socioeconomic status (income and education), discrimination, and acculturation, and whether they are associated with health status among racialized Canadians.
Methods
Sample
Data were drawn from the 27th GSS, a nationally representative survey conducted by Statistics Canada in 2013. The survey collected information on sociodemographic characteristics, immigration history, racialized status, well-being, social identity, social networks, and social engagement. There were 9011 respondents age 55 and older who had complete data on all of the variables included in the analyses. Of these, 6777 were whites born in Canada, 44 were racialized individuals born in Canada, 104 were white refugees, 110 were racialized refugees, 1277 were white immigrants, and 699 were racialized immigrants. First Nations Canadians were excluded from the analysis. In the three age groups, 4288 were aged 55–64; 2772 were aged 65–74; and 1950 were aged 75 and older.
Measures
The outcome measure was self-reported health in response to the question “In general, would you say your health is excellent, very good, good, fair, or poor.” Responses were dichotomized as “fair or poor” versus “good to excellent.” Hereafter, we will refer to these categories as poor health and good health, respectively. Research has suggested a high predictive validity for self-rated health measures on a variety of health outcomes, and it is a strong and accurate predictor of mortality (Schnittker & Bacak, 2014).
Racialized identity was based upon self-report as “Caucasian and/or White versus non-Caucasian in race and non-white in color” (Statistics Canada, 2013). If individuals self-identified as both white and racialized they were defined as racialized by Statistics Canada. Respondents born outside Canada were asked “Under which of the following broad immigration programs did you become a landed immigrant in Canada?” Response categories included (1) “The refugee program,” (2) “The program of re-unification with a family member already in Canada,” (3) “The points system (skilled workers and professionals, investors, entrepreneurs, and self-employed persons),” and (4) “other.” Categories 2, 3, and 4 were grouped together as “immigrants” and group 1 was defined as “refugees.” The key variable of interest combined racialized status and immigration status. It included six categories (whites born in Canada, racialized individuals born in Canada, white refugees, racialized refugees, white immigrants, and racialized immigrants).
Sociodemographic characteristics included sex (male or female), age group (55–64, 65–74, and 75 or older), total household income (less than $50,000, $50,000-less than $100,000, and $100,000 or more), and a missing category. Education level was divided into three categories (less than or equal to high school diploma, bachelors or college degree or diploma and master's or other graduate degree). Marital status was categorized as either married or common law versus single, widowed, divorced, or separated.
Individuals were asked about how trusting they are of people in general, and responses were dichotomized into “you cannot be too careful dealing with people” and “most people can be trusted.” Individuals were asked “How would you describe your sense of belonging to Canada” and responses were dichotomized into very strong versus somewhat strong, somewhat weak, very weak, or no opinion. Participants also responded to: “How many close friends (non-relatives) do you have that you feel at ease with, can talk to about what is on your mind, or call on for help?” Responses were dichotomized “none” versus “one or more.” Language spoken at home was dichotomized into English or French versus other languages. Level of participation in associations (e.g., professional or union), groups (e.g., religious or neighborhood/ community), or formal organizations (e.g., political party) in the past 12 months were dichotomized into none versus one or more. Individuals were asked if they had experienced any forms of discrimination in Canada in the past five years (i.e., based on race or skin color, ethnicity or culture, physical appearance (other than skin color), language, sex, religion, sexual orientation, age, physical, or mental disability) dichotomized into “no discrimination in any form” or “discrimination in any form.”
In our analyses restricted to the racialized subsample, two additional questions were included: (1) The percentage of friends contacted in the past month who were from a visibly different ethnic group, and; (2) the percentage of friends contacted in the past month who had the same mother tongue. Responses to these questions were dichotomized into “half or more” or a “none to a few.”
Statistical Analysis Plan
In the full sample of 9011 adults aged 55 and older, bivariate analyses based on Chi-square tests using adjusted weights were conducted to describe the sample with respect to racialized status (Table 1) and with respect to self-reported health status (Table 2). Adjusted odds ratios (aOR) were calculated using binary logistic regression analyses to examine the association between racialized/immigrant status and self-reported physical health, while adjusting for the covariates, described above, which were entered simultaneously. In the subsample of 853 respondents who were racialized, aOR were calculated using binary logistic regression analyses to examine the association between immigrant and refugee status and self-reported physical health while adjusting for covariates. All analyses were completed using SPSS Version 26 (IBM). The weights provided for the GSS27 were normalized to produce population-representative estimates corrected for the sample size.
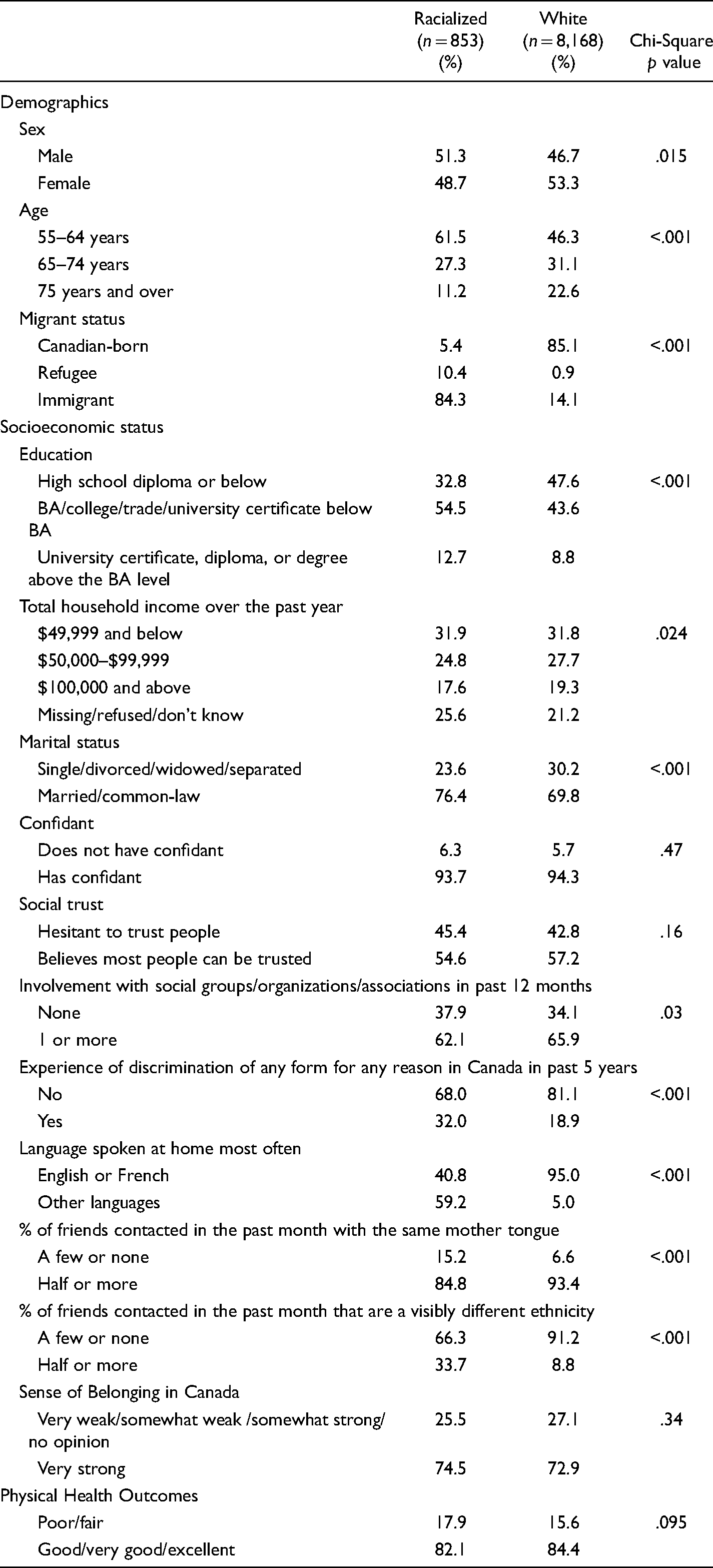
Sample Characteristics by Racialized status (General Social Survey, n = 9011).
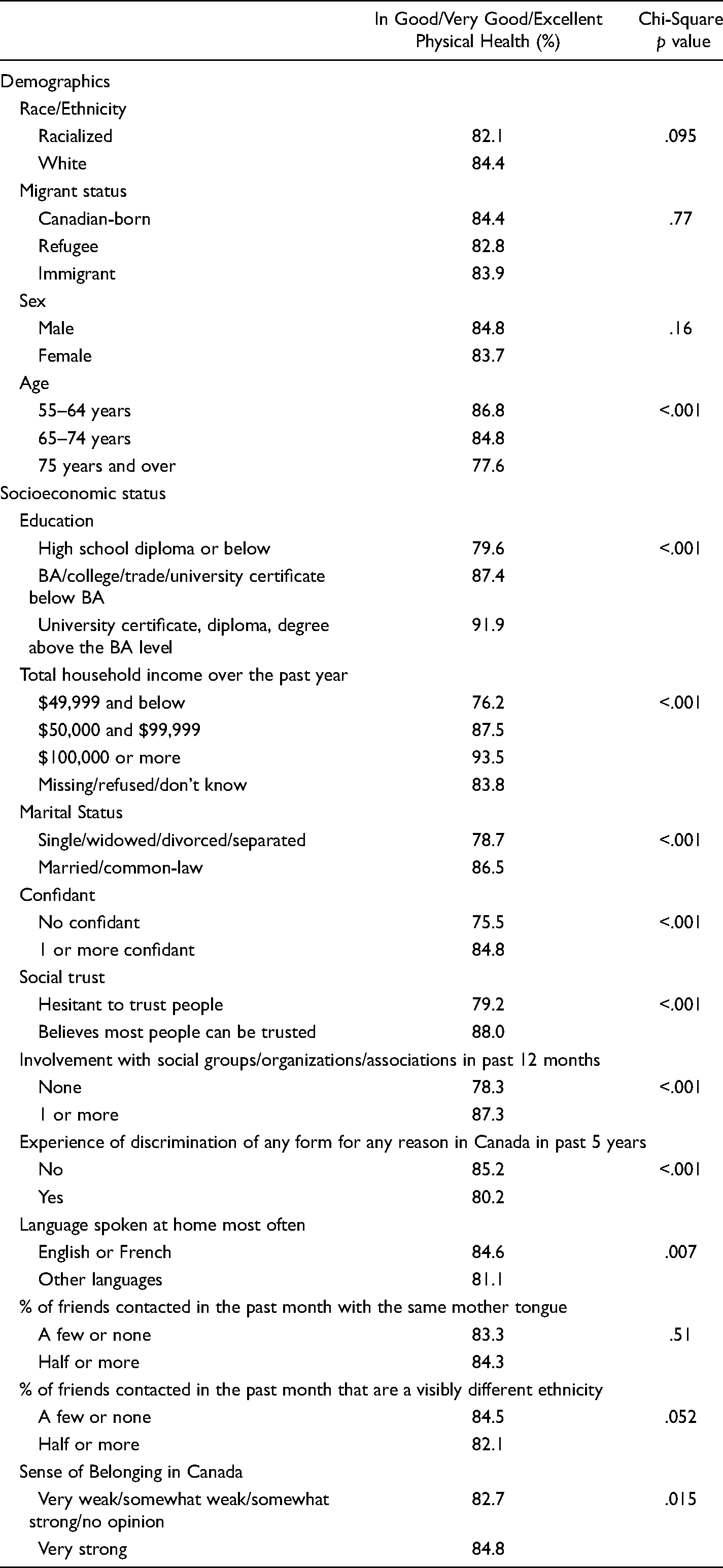
Sample Characteristics by Physical Health status (General Social Survey-27; n = 9011).
Results
As shown in Table 1, the bivariate results indicate that those who were racialized were more likely to be male, younger, university graduates, married, to have experienced discrimination (32.0% vs 18.9%), speak a language other than English or French at home (59.2% vs 5%), and to have one half or more of their friends be of a different ethnicity (33.7 vs 8.8%). In addition, a much lower percentage of racialized individuals, in comparison to whites, were born in Canada (5.4% vs 85.1%). Household income is hard to compare since racialized members were more likely to choose not to disclose their income. Racialized respondents were less likely to have participated in an association or organized group in the preceding year and were less likely to report having one half or more friends who spoke their mother tongue (84.8% vs 93.4%).
The duration of residence in Canada varied substantially by group: The prevalence of respondents who had arrived in Canada before 1980 was greatest for white immigrants (84%), followed by white refugees (69%), racialized immigrants (47%), and racialized refugees (16%) (p < .001) (analysis not shown in the table).
As shown in Table 2, bivariate analyses examining health status indicated that the percentage of respondents with good health was significantly higher among the following: younger age cohorts, those with more education, those with higher incomes, married respondents, those with at least one confidant, those who believed that most people could be trusted, those who participated in at least one association or group, those who spoke English or French at home, and those who had a very strong sense of belonging to Canada.
In the bivariate analyses, self-reported health status was not significantly associated with sex, racialized status, whether the respondent was born in Canada or was a refugee or immigrant, or whether the respondent socialized primarily with friends who had the same mother tongue. However, the percentage of respondents with good health was significantly lower among those who reported that they had been discriminated against in the last five years in Canada. Although those who socialized primarily with those of their same ethnicity had a marginally higher prevalence of good health than those who primarily socialized with friends of different ethnicity, this trend failed to reach statistical significance (p = .052).
Table 3 provides the results of the logistic regression analyses on the full sample of 9011 respondents when all variables, identified a priori, were entered simultaneously. This allows for the identification of the independent contribution of each variable while holding the other variables constant. In comparison to racialized immigrants, white immigrants had 35% higher odds of reporting good health while white older adults born in Canada had 34% higher odds of reporting good health. Racialized immigrants did not significantly differ with respect to self-reported health status compared to racialized refugees, those born in Canada who are racialized, or white refugees. An additional analysis including all the same variables in the analysis presented in Table 3 was conducted, but with Canadian-born whites as the reference category. Only racialized immigrants had significantly lower odds of good self-reported health.
Adjusted Odd Ratios (OR) of Good Physical Health by Race/Immigration Status and Other Sample Characteristics in the Whole Sample of GSS (n = 9011).
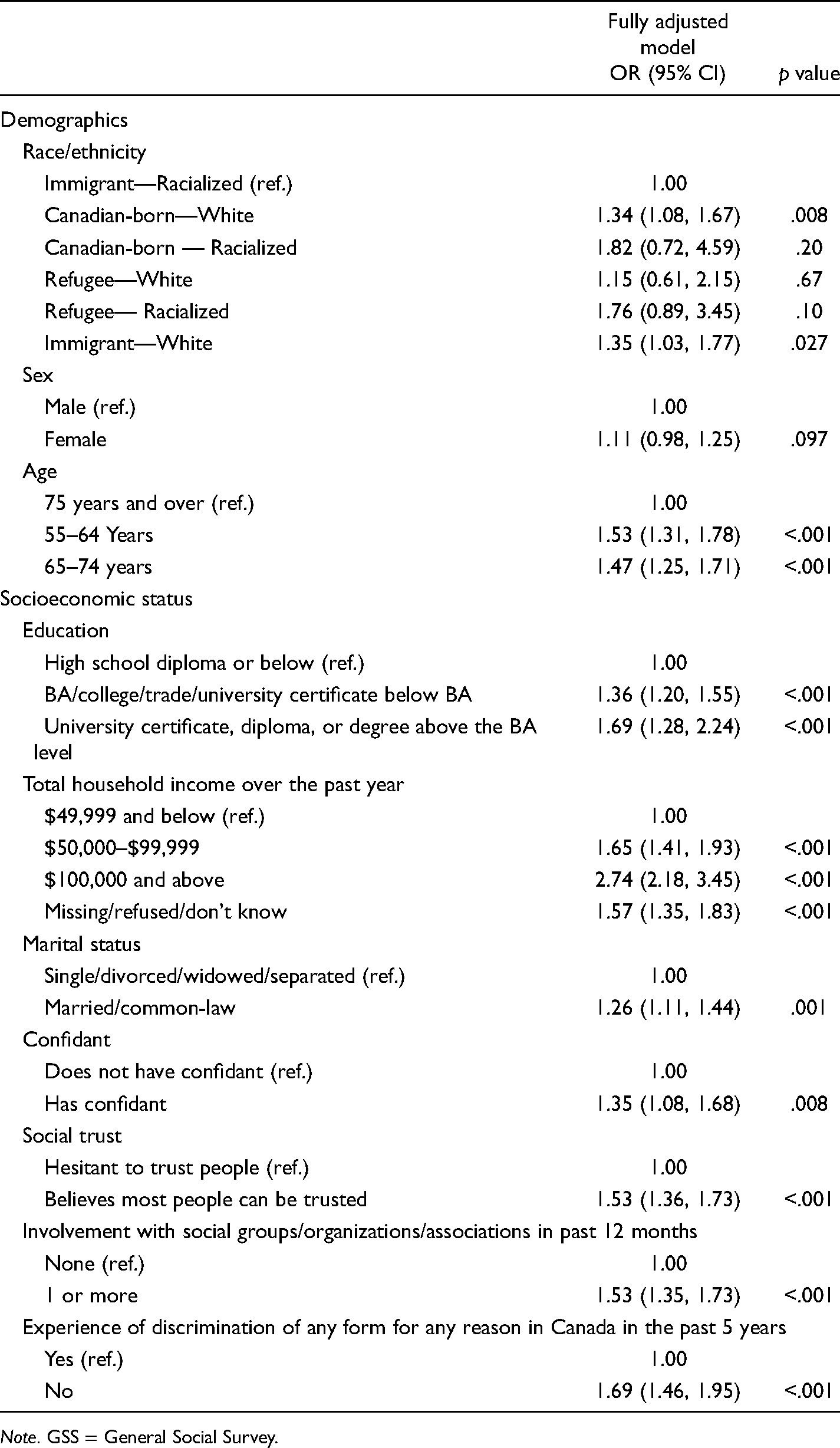
Note. GSS = General Social Survey.
In comparison to those aged 75 and older, the odds of reporting good health were 53% higher for those 55–64, and 47% higher for those aged 65–74. Higher household income, married individuals, those with a confidant, those who believe that most people could be trusted, and those who belong to at least one organized group or association had higher odds of reporting good health (aORs range from 1.26 to 1.53). Compared to those who had experienced discrimination in the past five years, those who had not experienced discrimination had 69% higher odds of reporting good health.
Table 4 presents the results from a logistic regression analysis with the 853 racialized respondents aged 55 and older in the GSS-27 data set. All three racialized groups (refugees, immigrants, those born in Canada) had comparable odds of reporting good health. In comparison to racialized members aged 75 and older, the odds of reporting good health were more than four-fold for those aged 55–64, and more than double for those aged 65–74. In comparison to those with a high school diploma or lower, individuals with a Master's degree or higher had more than seven-fold higher odds of reporting good health. In comparison to those whose household income was under $50,000 a year, those whose household income was above $100,000 had three times the odds of good health. Those with a confidant had twice the odds of good health in comparison to those with no confidant. When compared with those who had experienced discrimination in Canada in the past five years, those who had not experienced discrimination had 52% higher odds of good health. Individuals who report that the majority of their friends speak a language other than the respondent's mother tongue had twice the odds of good health.
Adjusted Odd Ratios (OR) of Good Physical Health by Race/Immigration Status and Other Sample Characteristics Among Visible Minorities in the GSS (n = 853).
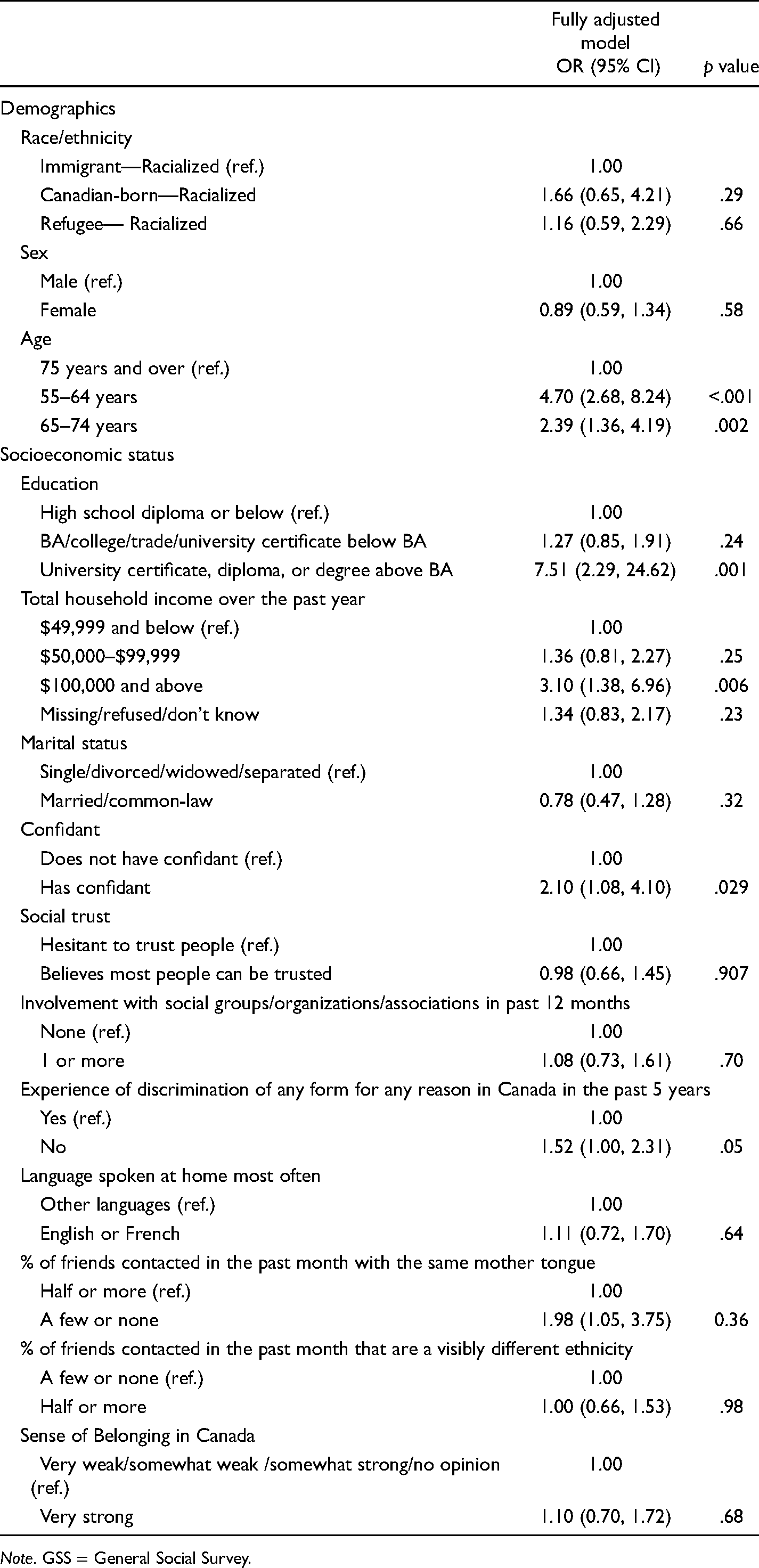
Note. GSS = General Social Survey.
Discussion
In this large, nationally representative survey of older Canadians, it appears that neither immigrant nor refugee status is driving health disparities; rather, it seems that race is the more important factor. In comparison to racialized immigrants, Canadian-born whites, and white immigrants both had approximately 35% higher odds of good self-reported health, even when statistical adjustments were made for a wide range of demographic, socioeconomic, social engagement, and social support variables. In contrast to our expectations, racialized refugees and white refugees did not have worse health than either racialized immigrants or whites born in Canada. Almost 70% of white refugees had arrived prior to 1980, so it is possible that any health disadvantage in that group may have been offset by access to Canada's universal health system in the years after their arrival in the country. In addition, the lack of a significant health disparity for racialized refugees, more than 80% of whom arrived since 1980, may also be partially due to their access to Canada's universal health system; however, further research is needed to explore the reasons for this finding.
When examining other factors associated with health disparities in the full sample, once race and nativity were taken into account, there was strong evidence of an association with lower social class, as measured by income and education, but, surprisingly, no evidence for sex disparities. The lack of association with sex may be partially due to the fact that income and education were taken into account. That is, the pathway between sex and health outcomes may be mediated by disadvantages or advantages in education or income, and therefore may no longer be statistically significant when socioeconomic characteristics are included in the analysis.
Several other factors were strongly associated with better health in the full sample of Canadians aged 55 and older: greater social support (which includes having a confidant and being married); a measure of social trust; and community involvement. However, taking into account all these factors did not attenuate the disparities associated with racialized status, suggesting that factors not explored in this study may be at play.
In the full sample, older adults who had not been discriminated against in the past five years had 69% higher odds of good health compared to those who reported they had been discriminated against. Approximately one-third of racialized older adults (32%) reported they had been discriminated against in the past five years, compared to one-fifth (18.9%) of white respondents. Previous research on immigrants, refugees, and racialized individuals have found that the experience of discrimination has a negative impact on self-rated health (Kim et al., 2013; Paradies et al., 2015; Siddiqi et al., 2017; Ziersch et al., 2020), and mental health (Beiser & Hou, 2017; Paradies et al., 2015; Szaflarski & Bauldry, 2019). Thus, discrimination can be considered a common stressor that may impact racialized older adults, regardless of their immigrant status. However, taking discrimination into account did not attenuate the association between racialized status and health status, underlining the need for further research including a wider range of other potential risk factors.
When we restricted our sample to racialized Canadians, those with the highest level of education (Master's degree or higher) and the highest income ($100,000 or more) were much more likely to be in good health compared to their less educated and less affluent peers. Canada's immigration system is based upon a point system that gives more points to those with more educational credentials (Government of Canada, 2019). This policy is reflected in the profile of the GSS sample of older adults, where almost one-half of white respondents had only a high school diploma or less, compared to only one-third of racialized respondents. In this way, the point system may contribute to the “healthy immigrant effect” as it “selects” highly educated and employable skilled workers who tend to have better health than their less educated peers.
In addition, respondents who had at least one confidant were twice as likely to be in good health, compared to those with no confidant. This finding speaks to the importance of reducing social isolation among aging immigrants, refugees, and the Canadian-born. A scoping review of older immigrants and refugees in Canada suggested that social isolation among this population was related to feelings of loss, living alone, having a living arrangement that restricts socialization with nonrelatives, having limited English language ability, being financially dependent, having family conflict, and a having lack of knowledge about available services and supports (Johnson et al., 2019). As social isolation is known to have negative impacts on mental and physical health, the authors suggested that older immigrants and refugees may cope with social isolation through joining support groups or involvement in religious activities (Johnson et al., 2019). However, in this study, the rather crude measure of social involvement (participating in at least one association or organization in the past year) was not associated with health status when other measures such as having a confidant were taken into account. Our bivariate findings indicated that racialized members, compared to white respondents, were less likely to have participated in a group, organization, or association in the past 12 months, suggesting the need for improved access to and/or creation of initiatives and programs that can improve social connectedness among these groups.
There were mixed findings on the three factors that were believed to indicate acculturation. It was hypothesized that acculturation would be stronger among those who reported that less than one half of their friends spoke the respondent's mother tongue. This group represented 15% of the racialized sample. In the logistic regression analysis, this group had double the odds of good physical health in comparison to racialized respondents who spoke the same mother tongue of more than half their friends. These findings may be biased toward the null for those racialized members who speak English or French as a mother tongue (e.g., African Canadians from French-speaking countries). It was also hypothesized that racialized older adults who spoke English or French at home, and those who reported that at least one half of their friends were of a different ethnicity would be more acculturated. Only 41% of racialized members versus 95% of white respondents spoke English or French at home. One-third of racialized members reported that more than half their friends were of different ethnicity. In the logistic regression analyses on the racialized sample, neither language spoken at home nor percentage of friends of different ethnicity were significantly associated with health status.
Research has found that acculturation among immigrants is related to having English fluency and not being newly arrived (Baek Choi & Thomas, 2009). Being able to speak English fluently may have facilitated respondent's ability to form social connections with Canadian peers, find appropriate employment, and access health care. Although a measure of English or French fluency was not included, the GSS was only administered in English or French, so it is fair to assume that all respondents had relatively good working knowledge of one of the charter languages. Further, greater length of time since immigration provides respondents with more opportunity to gain English or French fluency and build social networks, and these factors, among others, may promote good health outcomes. There was variation in the recency of arrival by race. Whites were much more likely than racialized respondents to have arrived in Canada prior to 1980. Discrimination may impede physical well-being. Racialized older adults who had no experience of discrimination in the preceding five years had 50% higher odds of good health compared to those who had been discriminated against.
Limitations
There are several important limitations to this study that must be considered. Firstly, other forms of intersectionality, such as sexual orientation and religion (Wiebe, 2015) were not included in our analyses, thus we cannot determine whether the health of our sample was associated with discrimination related to these identities. In addition, the context in which discrimination was experienced, the frequency or severity of the discrimination, or the form of discrimination was not included in the analyses. Research among refugees and racialized groups has reported discrimination during interactions with health care providers (McKeary & Newbold, 2010; Paradies et al., 2014; Wahoush, 2009), which may impact health care access and partially explain poorer health among those who are racialized. Last, the GSS-27 did not include information on many aspects salient to health status including health behaviors such as alcohol and other substance dependence, smoking history, nutrition (Moffat et al., 2017), food insecurity (Lane et al., 2019), obesity, and use of preventive health care (Pottie et al., 2007). Furthermore, our study was cross-sectional. As was discussed in the introduction, there is a selection bias that excludes ill immigrants through the medical examination system at the time of immigration. It may also be that immigrants who develop health problems after immigration return to their country of origin, thereby providing a further selection bias toward health immigrants. Longitudinal research would be beneficial to untangle these effects and determine whether the health of immigrants is declining over time. Future research should address these important gaps in the current study.
Conclusion
The intersections between racialized and socioeconomic status matter in the physical health outcomes of older adults in Canada. Findings from the present study indicate that racialized status and socioeconomic status are strongly associated with health status among older Canadians, but that sex, and immigrant and refugee status are not. Among racialized older adults, higher income and education, greater levels of social support, and lower levels of discrimination are associated with better self-reported health. Unfortunately, the findings do not provide insights into why these health disparities exist. Qualitative research would be helpful to further explore these disparities among racialized older adults. Such research would also provide important guidance as to how community-based services and programs could best facilitate the construction of social networks for racialized older adults to address the negative impact of social isolation. It might also shed light on the salience of cultural competence and language training for health care and other social care professionals to address discrimination and other structural barriers to health care access (World Health Organization, 2018).
Footnotes
Acknowledgment
This work was supported by the Social Science and Humanities Research (Grant number 435-2020-0177). The authors would like to thank the GSS-27 for providing the data for this analysis.
Authors’ Note
Conceptualization, A.M., U.G., K. K., E.F.T.; methodology, E.F.T.; formal analysis, E.F.T.; writing—original draft preparation, A.M., E.F.T.; writing—review and editing, A.M., U.G., K.K., E.F.T., supervision, E.F.T., funding acquisition, U.G., K.K., E.F.T. All authors have read and agreed to the published version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Social Sciences and Humanities Research Council of Canada (grant number 435-2020-0177).
Supplemental Material
Supplemental material for this article is available online.