
Abstract
Dementia represents a substantial threat to the self. However, to date, there is no reliable way to measure how threatened people feel by dementia. This article reports on two online studies. In Study 1, 248 participants rated statements about dementia according to their threat to well-being. In Study 2, 99 participants (all students at the University of the West of England) completed the emerging scale (the Threat of Dementia Scale or ToDS). We validated this by examining its associations with conceptually related measures, including the revised Fraboni Scale of Ageism and the Fear of Alzheimer’s Disease Scale. Study 1 yielded 13 statements that were highly intercorrelated and comprised a single factor. In Study 2, the ToDS demonstrated good construct validity and acceptable test–retest reliability. Higher levels of distancing predicted lower scores on the ToDS. The ToDS is a reliable and valid instrument that is the first statistically validated method of examining the extent to which dementia threatens well-being.
Introduction
Dementia involves numerous changes to the body and mind, including a progressive loss of control over daily functioning, leading to death (Martens et al., 2005; O’Connor & McFadden, 2012). These changes occur incrementally and gradually over the course of the illness. There is no cure for any form of dementia; the risk of developing it increases exponentially with age, roughly doubling every 5 years after the age of 65 (Corrada et al., 2010).
Recently, it has been suggested that contact with people living with dementia may promote an awareness of one’s own mortality and the inevitability of aging and, ultimately, death (Cheston & Christopher, 2019; McKenzie et al., 2017). Thus, reading about older people with dementia provokes more anxiety among younger participants than does reading about older people who are in good or unknown health (O’Connor & McFadden, 2012). Prior theory and evidence indicate that contact with older adults with dementia can serve to remind younger people of the inevitability of aging and, by extension, their own death (Martens et al., 2005). Indeed, even thinking about dementia is associated with heightened accessibility of death-related thoughts (O’Connor & McFadden, 2012) and increased levels of anxiety about death. In a similar way, fears about developing dementia oneself intensify as people grow older or as they gain personal experience with dementia (Cutler & Hodgson, 1996; Kessler et al., 2012)—for instance, from caring for a relative living with the illness (Cutler & Hodgson, 2001).
In order to reduce the anxiety that contact with dementia (and by extension with their mortality) may induce, people draw on a number of different strategies (Greenberg et al., 1990). For example, younger adults may avoid the company of older adults (Chonody et al., 2014) or characterize them as being forgetful, incompetent, and unproductive—in essence as being unlike younger adults’ representations of themselves (Cuddy et al., 2005; North & Fiske, 2012). From a social–psychological perspective, then, ageist attitudes such as these forms of distancing serve to protect the self against the anxiety that would otherwise arise from being reminded of the inevitability of illness, aging, and mortality (Popham et al., 2011). Although younger people may be able to reduce their anxiety by distancing themselves from older people living with dementia, these strategies may become less effective as people age. Consequently, they may need to draw on other psychological mechanisms to reduce their exposure to anxiety. Along these lines, Cheston et al. (2020) have shown that older, but not younger, participants recalled fewer highly negative statements about dementia when these were directed at them, rather than at another person. This form of selective forgetting is termed the mnemic neglect effect (Sedikides & Green, 2009; Sedikides et al., 2016) and acts to decrease the level of anxiety that would otherwise arise from proximal threats to the self.
Given the frequent contact of staff working in health and social care with people living with dementia, it is reasonable to assume that they too will draw on strategies to reduce anxiety. Indeed, a study of 94 nursing students showed that reading about a hypothetical older patient with dementia led to higher levels of death anxiety (McKenzie & Brown, 2017) compared to either younger patients or to patients with other conditions.
There is strong evidence then to suggest that contact with dementia (either through providing care or by reading about it) represents a psychological threat to self-functioning and activates the use of strategies aimed at reducing anxiety. Thus, distancing strategies may assuage the existential threat that old age and dementia represent to younger generations (Martens et al., 2005), while a process of selective forgetting enables older people to negate some of the anxiety arising from more self-threatening aspects of dementia (Cheston et al., 2020). If researchers are to understand better the psychological processes underlying people’s response to dementia, then they ought to be able to determine the extent to which dementia is experienced as a threat. Currently, however, no reliable way to measure dementia threat exists. Although it is possible to measure someone’s fear of developing dementia (e.g., through the Fear of Alzheimer’s Disease Scale or FADS; French et al., 2012), these two constructs relate to distinct psychological processes. For example, it is possible to have relatively little fear of developing dementia personally, whilst also experiencing the potential impact of the illness on oneself as very threatening. Whereas the former relates to an enduring concern, the latter is a situation-specific response. Developing a means of assessing the level of threat that dementia represents to the self would, therefore, open up possibilities for research into social attitudes toward dementia.
Research Aims
The goals of the current research were to (1) develop a scale with good psychometric properties for assessing the level of threat associated with dementia, and (2) test the scale’s construct validity.
Study 1: Development of the Threat of Dementia Scale (ToDS)
Method
Materials
The study received ethical approval. 1 RC collected descriptive statements of dementia from materials that are widely available in the UK (e.g., information leaflets published by the Alzheimer’s Society 2 and the NHS Choices website 3 ) and that were designed to be read by people with dementia. The statements were then screened for duplicates and coherence by ED and GC, with the remaining 64 statements forming the basis of an online survey, which we administered through Qualtrics.
The statements fell into one of three areas. The first area was Kitwood’s (1997) description of personhood, comprising: three statements related to security (e.g., “Even with your illness you can be reassured”), three related to continuity (e.g., “Your plans for the future might change, but the illness doesn’t change who you are”), two related to belonging (e.g., “The impact of the illness depends on the support available to you”), two related to purpose (e.g., “You will still be able to find answers for yourself”), and four related to fulfillment (e.g., “With the illness there is still much that you can enjoy in life”). The second area was the six cognitive domains of dementia identified in the Diagnostics and Statistics Manual of Mental Disorders, 5th Edition (American Psychiatric Association, 2013): five statements related to learning and memory (e.g., “The illness will mean that you cannot always remember things you have heard”), three related to language (e.g., “The symptoms that you may experience can include problems with communication”), five related to complex attention (e.g., “As a result of the illness, you may have problems reasoning”), four related to executive functioning (e.g., “The illness may make you feel confused”), and three related to perceptual—motor (e.g., “The illness may make you fidget constantly”). The third and final area constituted six other categories that are widely identified as key features of dementia (British Psychological Society, 2016): nine statements related to progression (e.g., “Your illness is progressive”), four related to treatments (e.g., “Drug treatments may slow down the speed at which your symptoms get worse”), two related to variability (e.g., “The symptoms of your illness can vary greatly from one person to another”), six related to causation (e.g., “Your illness develops when the arteries in your brain become blocked”), six related to behaviors (e.g., “You may forget and ask the same question over and over”), and three related to affective responses (e.g., “The illness can make you feel depressed”).
Participants
We recruited participants from three sources: undergraduates at the University of the West of England (UWE Bristol) who completed the study for course credit; postgraduate students, academics, and administrative staff at UWE Bristol who learned about the study through the University newsletter; and members of the public (including health, social, and voluntary sector staff) who engaged via social media. All participants were aged over 18. Otherwise, we had no inclusion or exclusion criteria. In all, 248 participants completed both the online consent stage and the questionnaire. Of these, 190 were female and 58 were male, with their occupations split roughly evenly between undergraduate students (95) and staff (94) with the remaining 59 participants having a range of other occupations. Participants largely identified themselves as white (231) with 15 self-identifying as from Black, Asian, and Minority Ethnic (BAME) communities with two not recording their ethnicity. Participants had an average age of 39.01 years (SD = 15.86).
Procedure
Participants rated each statement (1 = not at all, 6 = very much) according to how serious its consequences were for well-being.
Results
Factor Structure
We analyzed the data using IBM SPSS version 24 for Macintosh (IBM Corp, 2016). An initial screening analysis did not identify any potential observations that might adversely affect an exploratory factor analysis solution (Chatterjee et al., 1991), and we therefore sought such a solution using principal axis factoring with oblique rotation to aid interpretability. We used both parallel analysis and Velicer’s Minimum Average Partial (MAP) test (Cota et al., 1993; Glorfeld, 1995, Hayton et al., 2004; Velicer, 1976; Zwick & Velicer, 1986) to decide on the number of factors to retain. An inspection of the bivariate correlation matrix indicated a set of 13 items that were positively intercorrelated. The parallel analysis identified a single factor that comprised the same 13 statements. Velicer’s MAP strongly indicated a single component (
Cronbach’s α (Cronbach, 1951) for the putative scale was 0.911, with all 13 items having a high corrected item–total correlation (0.5 < r < 0.8), and the sample value for α continuing to be robust to item deletion (α > 0.899, if any item deleted). Table 1 provides the Threat of Dementia Scale (ToDS) factor loadings, item means, standard deviations, and item–total correlations.
ToDS Factor Loadings, Content Item Means, Standard Deviations (SD), and Item–Total Correlations in Study 1.
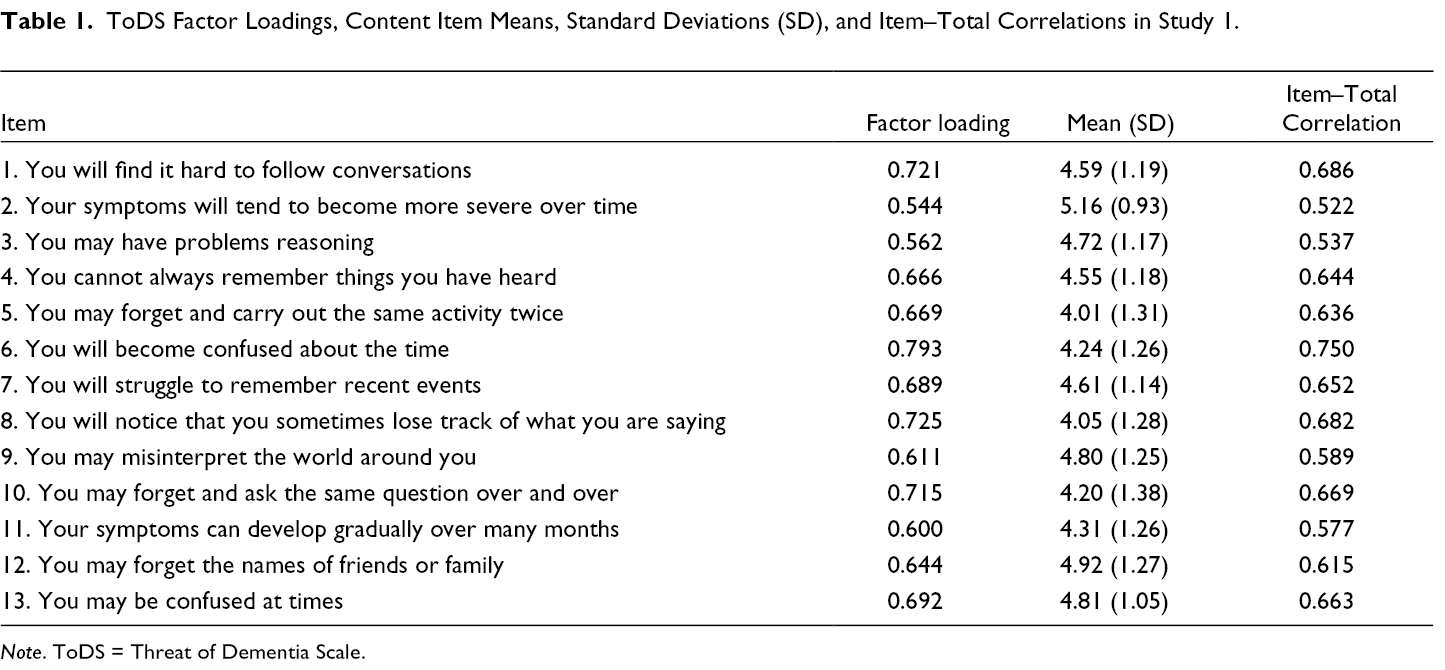
Note. ToDS = Threat of Dementia Scale.
In summary, our analysis produced 13 statements (given in Table 1) that were positively intercorrelated. Attempting to force other statements into this set of items did not improve the solution, with item–total correlations for these forced items being generally low. Consequently, these 13 items comprised the ToDS. In Study 2, we examined the scale’s construct validity.
Study 2: Construct Validation of the Threat of Dementia Scale (ToDS)
Social attitudes serve, at least in part, to reduce self-threat (Martens et al., 2005; O’Connor & McFadden, 2012). Thus, we would expect that a measure of dementia threat would be associated with a range of attitudes toward both dementia and, more generally, aging. More precisely, as ageism amongst younger people is believed to result (at least in part) from a wish to distance themselves from older people, who are perceived as embodying the aging process—and by extension mortality (Chonody et al., 2014; Cuddy et al., 2005; Greenberg et al., 1990, 2002)—increased psychological distance would act to reduce the threat of dementia. We therefore hypothesized that the ToDS would be negatively predicted by ageism, as measured by the Fraboni Scale of Ageism-Revised (FSA-R; Rupp et al., 2005), and in particular by the Separation subscale of the FSA-R, which is closely aligned to the distancing aspects of ageism.
We also expected that the extent to which people feel threatened by dementia would be related to their understanding of the risk of developing dementia themselves. Fears about developing Alzheimer’s or other forms of dementia (the phenomenon of “dementia worry”) have been reported to be increasingly widespread (Kessler et al., 2012, 2014), and may reduce performance on clinical outcomes, including those assessing executive functioning (Fresson et al., 2017). We therefore tested the relationship between the ToDS and the Fear of Alzheimer’s Disease Scale or FADS (French et al., 2012). We expected to find a positive correlation between the ToDS and the overall score on the FADS. Specifically, we hypothesized that there would be a positive correlation between the ToDS and the Catastrophic Attitudes subscale of the FADS, which is most clearly identified with threat.
Finally, we tested whether the threat of dementia could be distinguished from fears of developing dementia through their relationship with anxiety. There is a key distinction to be made between experiencing specific symptoms of dementia as a potential threat and a fear that one might develop dementia or Alzheimer’s disease: whereas the former is a situation-specific response, the latter is an emotional reaction that involves a calculation of risk. We hypothesized that, although the fear of developing dementia (as assessed by the FADS) would be associated with increased anxiety (as measured by the Anxiety subscale of the Hospital Anxiety and Depression Scale or HADS-A; Zigmond & Snaith, 1983), the threat of dementia would not be associated with anxiety. We therefore also hypothesized that the (positive) correlation between the FADS and the HADS-A would differ significantly from the correlation between the ToDS and the HADS-A (Zigmond & Snaith, 1983).
Method
Participants
Ninety-nine undergraduates (89 females, nine males, and one participant of unknown sex) at UWE Bristol participated for course credit. 4 Participants had an average age of 21.86 years (SD = 6.17) with 82 identifying themselves as white and seven self-identifying as from different BAME communities.
Design and Procedure
The study consisted of two parts, accessed online via two separate Qualtrics surveys. As in Study 1, participants provided consent online before completing both surveys. In the first survey, participants supplied background demographic information (e.g., age, gender, ethnicity). Before completing the ToDS, they were then provided with the following instructions:
Please read the following statements, all of which are symptoms of dementia or Alzheimer’s Disease. Imagine that these descriptions are real, and that they apply to you. Please rate the extent to which your sense of well-being would be threatened by each statement by circling the appropriate response.
Participants rated each of the 13 statements on a scale ranging from 1 (not at all) to 7 (very much). Finally, participants completed three other questionnaires: the FSA-R, FADS, and HADS-A. To assess test–retest reliability, participants completed a second survey after 4 weeks, which included only the ToDS.
Measures
The FSA-R (Rupp et al., 2005) measures both affective and cognitive components of attitudes to aging. The revision of the original FSA (Fraboni et al., 1990) involves a new factor structure corresponding to three subscales. Response options for the 23-item FSA-R range from 1 (strongly disagree) to 4 (strongly agree). The Stereotypes subscale consists of 10 items that are similar to the original FSA Antilocution factor, and measures the cognitive component of ageism. It includes statements such as “Old people are stingy and hoard their money and possessions.” The Separation subscale consists of eight statements that are comparable to the FSA Avoidance factor, and includes items such as “It is best that old people live where they won’t bother anyone.” The Affective Attitudes subscale consists of four items that are reflective of positive attitudes toward older people (e.g., “The company of most old people is quite enjoyable”) and one item that is reflective of negative attitudes toward older people (“I personally would not want to spend much time with an old person”). We reversed the positively worded items, and then averaged the five items to create an index of negative attitudes toward older people. The FSA-R has good construct validity and high internal reliability.
The FADS (French et al., 2012) is a reliable measure of dementia worry or anticipatory fears about developing dementia. Response options for the 30-item FADS range from 0 (never) to 4 (always). It comprises three subscales: General Fear (17 items; e.g., “When I think about the possibility of developing Alzheimer’s disease, I become nervous or anxious”), Physical Symptoms (eight items; e.g., “Thinking about Alzheimer’s disease makes me feel fatigued”), and Catastrophic Attitudes (five items; e.g., “I would rather die than develop Alzheimer’s disease”). The FADS has good construct validity and is correlated with measures of state and trait anxiety.
The HADS (Zigmond & Snaith, 1983) is a widely used measure of anxiety and depression. We administered only the seven-item Anxiety subscale (HADS-A) that instructs participants to rate their feelings of anxiety (e.g., “I feel tense or wound up”) over the previous week (0 = not at all, 3 = most of the time).
Results
The mean score on the ToDS was 68.30 (SD = 12.14) out of a maximum of 91, with participants’ average total score on the FSA-R being 41.31 (SD = 7.35; Stereotypes subscale, M = 19.98, SD = 3.82; Separation, M = 12.44, SD = 2.94; and Affective Attitudes, M = 8.89, SD = 1.80). Only 98 participants completed the remaining scales, with an average total score on the FADS of 35.06 (SD = 18.16; General Fear, M = 25.41, SD = 13.53; Physical Symptoms, M = 2.83, SD = 3.19; and Catastrophic Attitudes, M = 6.83, SD = 3.80) and with an average score on the HADS-A of 10.07 (SD = 4.74).
Internal Consistency
Cronbach’s α for the ToDS was 0.913. The removal of any of the 13 individual items did not improve this score.
Construct Validity
We calculated Pearson product–moment correlations for the ToDS, FSA-R, FADS, and HADS-A (and subscales; Table 2). All tests were two-sided and we took a p level of less than .05 to indicate statistical significance.
Pearson Inter-Item Correlation Matrix (and Significance Levels) for Scales and Subscales in Study 2 (N = 99).
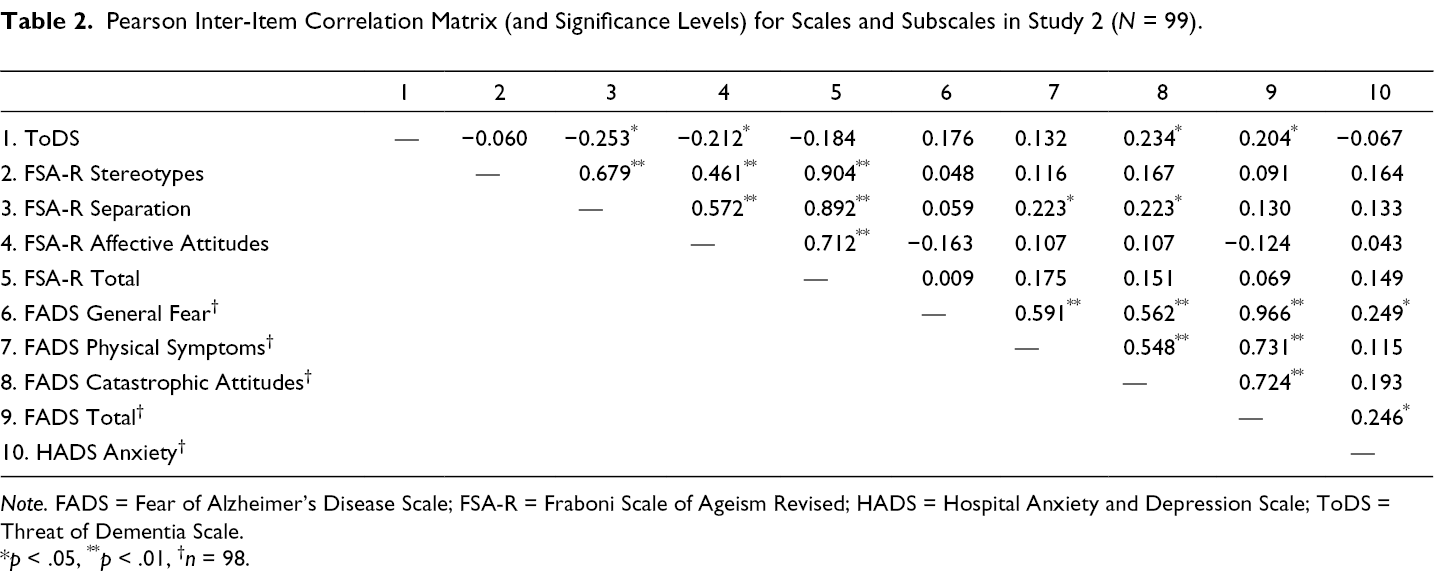
Note. FADS = Fear of Alzheimer’s Disease Scale; FSA-R = Fraboni Scale of Ageism Revised; HADS = Hospital Anxiety and Depression Scale; ToDS = Threat of Dementia Scale.
*p < .05, ** p < .01, † n = 98.
The FSA-R: As hypothesized, scores on the ToDS were negatively correlated with the Separation subscale of the FSA-R (r = −0.253, p < .05). Additionally, the ToDS correlated negatively with the Affective Attitudes subscale (r = −0.212, p < .05), but was not significantly correlated with the total score or the Stereotypes subscale.
The FADS: Consistent with our hypothesis, scores on the ToDS were positively correlated with the overall score on the FADS (r = 0.204, p < .05) and the FADS Catastrophic Attitudes subscale (r = 0.234, p < .05), which, as mentioned before, is most clearly identified with threat.
The HADS: We hypothesized that scores on the FADS would be positively correlated with scores on the HADS-A, and that this correlation would be stronger than the one between ToDS and HADS-A. This was indeed the case. Whereas the overall FADS score was positively correlated with HADS-A (r = 0.246, p < .05), the correlation between ToDS and HADS-A was not significant (r = −0.067). Moreover, the difference between these two correlations was significant, as indicated by a Williams’ test (Weaver & Wuensch, 2013) for comparing dependent correlations, t(95) = 5.31, p < .001.
Relationship Among Variables
To test whether anxiety, ageism, or fear of developing dementia best predicted the threat of dementia, we conducted a stepwise linear multiple regression. The ToDS was the dependent variable. Anxiety (HADS-A), the three FADS subscales (General Fear, Physical Symptoms, and Catastrophic Attitudes), and the three FSA-R subscales (Separation, Affective Attitudes, and Stereotypes) were the independent variables. The overall model was significant (F[7, 90] = 2.98, p = .007) with an R 2 of 0.19. The variance inflation factors for the seven variables were between 1.10 and 2.38, indicating a low risk of multicollinearity (Table 3). The FSA-R Separation negatively predicted ToDS scores, whereas the FADS Catastrophic Attitudes positively predicted the ToDS scores, corroborating the above-reported univariate analyses.
Multiple Regression Analysis Predicting ToDS Scores.
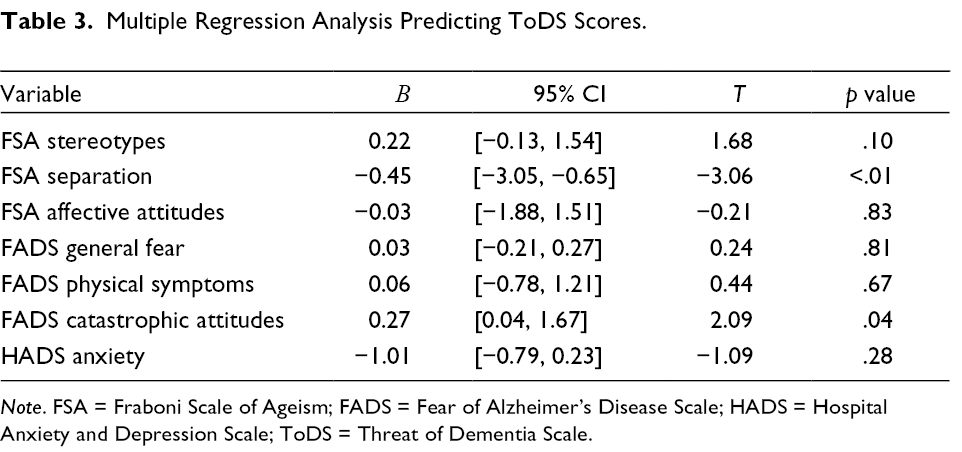
Note. FSA = Fraboni Scale of Ageism; FADS = Fear of Alzheimer’s Disease Scale; HADS = Hospital Anxiety and Depression Scale; ToDS = Threat of Dementia Scale.
Analysis of Demographic Responses
Neither the difference in the ToDS scores between women and men (t[97] = 1.06, p = .29) nor between younger (aged 18 to 24) and older (aged 25 to 64) participants (t[97] = 0.99, p = .32) was statistically significant. However, participants from the BAME communities (M = 62.82, SD = 13.56), (t[97] = −2.08, p = .04, d = 0.54) scored significantly lower on the ToDS than did white participants (M = 69.43, SD = 11.59). Furthermore, participants from the BAME communities scored significantly higher on the Separation (M = 14.24, SD = 3.38 vs. M = 12.07, SD = 2.72; t[97] = 2.86, p < .01, d = 0.71) and Affective Attitudes (M = 9.94, SD = 1.48 vs. M = 8.67, SD = 1.79; t[97] = 2.74, p < .01, d = 0.77) subscales of the FSA-R, but not on any other variables.
We tested whether the BAME participants’ lower perceived threat of dementia (as assessed by the ToDS) was mediated by their higher levels of ageism (as indexed by the Separation and Affective Attitudes subscales of the FSA-R). We implemented the joint-significance test (Yzerbyt et al., 2018), which involves testing the individual components of the indirect or mediated effect. The first component was the link between the independent variable (i.e., ethnicity) and the postulated mediator (i.e., ageism). The second component was the link between the mediator and the dependent variable (i.e., ToDS), controlling for the independent variable. To demonstrate mediation, both components of the indirect effect needed to be statistically significant (i.e., joint significance).
Consistent with the idea that distancing (as indexed by Separation) serves a self-protective function, the BAME participants’ lower perceived threat of dementia was mediated by Separation. Supporting the first component of this indirect effect, the BAME (compared to white) participants scored higher on Separation (see above). Supporting the second component, when controlling for ethnicity, Separation predicted lower ToDS scores, b = −0.87, t(96) = −2.08, p = .040. Results did not support possible mediation by Affective Attitudes. Although the BAME (compared to white) participants scored higher on Affective Attitudes (indicating more negative attitudes toward older adults; see above), Affective Attitudes did not significantly predict ToDS scores when controlling for ethnicity (i.e., the second component of the indirect effect was not significant), b = 1.14, t(96) = −1.65, p = .103.
Test–Retest Reliability
Ninety-one participants completed the ToDS for a second time. The mean period between completing the ToDS initially and retesting was 31 days (SD = 8.85). The ToDS scores at both time points were significantly correlated (n = 91, r = 0.62, p < .001). Test–retest reliability was good, with an intra-class correlation between the retest and test of 0.74, 95% CI [0.58, 0.83].
General Discussion
We developed and tested the psychometric properties of a scale designed to measure the threat associated with dementia—the ToDS. Study 1 involved the identification of scale items. Results revealed a single-factor solution of 13 items assessing the threat that dementia poses to well-being. All 13 items had a high corrected item−total correlation and were robust to item deletion. We assessed construct validity in Study 2 by examining the relationship between the ToDS and three related measures: the FSA-R, FADS, and HADS-A (including their subscales).
The Relationship Between Dementia Threat and Ageism
Ageism, and especially distancing, provides a way of protecting oneself from threat (Chonody et al., 2014; Cuddy et al., 2005). We therefore anticipated that scores on the ToDS would be negatively associated with our measure of ageism, the FSA-R, and especially the Separation subscale of the FSA-R. This contains items such as “I personally would not want to spend much time with an old person” and measures the extent to which participants seek to distance themselves from older people.
Overall, our findings point to a relationship between threat and the distancing component of ageism. First, the ToDS was significantly and negatively correlated with the Separation and Affective Attitudes subscales of the FSA-R, but was uncorrelated with the total FSA-R and the Stereotypes subscale. Second, scores on the Separation subscale (but not other FSA-R subscales) negatively predicted ToDS scores. Third, Separation scores mediated the BAME (compared to white) participants’ lower perceived threat of dementia.
The Relationship Between Dementia Threat and Fear of Developing Dementia
Our findings also cast light on the relationship between dementia worry and threat. Prior research has generally indicated that a personal experience of dementia is associated with higher levels of fear of developing illnesses such as Alzheimer’s disease (Cutler & Hodgson, 1996, 2001; Kessler et al., 2012, 2014). We confirmed our hypothesis of a positive relationship between the ToDS and the total FADS score. This correlation was primarily driven by a significant positive correlation between the ToDS and the Catastrophic Attitudes subscale (rather than between the ToDS and the other FADS subscales). Indeed, this subscale (but none of the others) positively predicted threat. Additionally, although the total FADS score was significantly correlated with anxiety (as measured by HADS-A), scores on the ToDS were not associated with anxiety. Further, these correlations differed significantly.
These findings support our argument that the ToDS and the FADS measure separate but overlapping constructs. Whereas a person’s fear of developing dementia—their dementia worry—is related to levels of anxiety, the extent to which the self is threatened by dementia is only predicted by the extent to which the person catastrophizes about the risk of having dementia themselves.
The Relationship Between Dementia Threat and Demographic Variables
Neither gender nor age was associated with the ToDS scores despite consistent findings that both factors are linked to other cognitive processes around dementia including the development of attitudes (Cuddy et al., 2005; Martens et al., 2005; North & Fiske, 2012). However, the BAME participants scored lower on the ToDS than white participants. Although we acknowledge that Study 2 included only a small (n = 17) and selective (undergraduates) sample of individuals from the BAME communities, this is consistent with some other findings in the literature. First, previous research has indicated that some BAME participants have less positive person-centered views toward those living with dementia (Cheston et al., 2016) and sometimes have higher levels of stigma toward dementia (MacKenzie, 2006; St. John, 2004). At the same time, qualitative findings suggested that some individuals from the BAME communities do not see dementia as an illness that affects them (Baghirathan et al., 2020). For example, in a UK study, members of Black African and Caribbean communities characterized perceptions of memory problems with the phrase “we don’t do dementia” (Berwald et al., 2016). In line with this literature, we found that distancing (as measured by the FSA-R Separation subscale) mediated the lower levels of threat experienced by the BAME participants. The small sample size of BAME participants in our study necessarily limits the conclusions that we can draw; nevertheless, the role of distancing in shaping perceptions of dementia among society as a whole including people from the BAME communities merits further attention.
Strengths and Limitations
The ToDS is a reliable and valid instrument. It is the first to assess the extent to which dementia represents a threat to the self. The process of development and validation of the ToDS does, however, have several limitations. For example, whether or not participants had any experience with dementia, and if so in what context, is unknown. Thus, all participants in Study 2, and over a third of those in Study 1, were undergraduates, typically studying psychology. Although most students would have attended lectures on neurological conditions, their knowledge of dementia, including their personal experiences of it, is unverified. Moreover, there is evidence that attitudes toward old age change over time (Cheston et al., 2016, 2019). Whereas adults of all ages distance themselves from their future and older selves, and thus insulate themselves from anxiety about their mortality, this strategy is likely to be less effective for older people (Levy, 2009). Thus, the relationship between perceived threat of dementia and distancing may only hold for younger people, including the undergraduate population that we tested in Study 2. In order to establish whether the psychometric properties of the ToDS are consistent across all age ranges and cultures, the measure needs to be evaluated in different samples and with other forms of construct validity, such as predictive and concurrent validity. For instance, the relationship between threat and specific protective strategies, such as distancing, needs to be tested directly.
Summary and Conclusion
The ToDS scale is a valid measure of the extent to which an individual feels threatened by dementia. It has good psychometric properties, including acceptable test–retest reliability after 1 month. Our analysis of the construct validity of the ToDS points toward the threat of dementia being a psychological process that is related to, but distinct from, both ageism and the fear of developing dementia. When participants were able to distance themselves from older people, they manifested a reduced level of dementia threat. Similarly, although the threat of dementia was positively predicted by the Catastrophic Attitudes subscale of the FADS, it differed from other aspects of dementia worry. For instance, whereas the fear of developing Alzheimer’s disease was correlated with anxiety, there was no such relationship between anxiety and the threat of dementia.
Our findings cast light on gerontological constructs including the formation of attitudes toward dementia and people living with this condition. On a societal level this is important, as global estimates suggest that 66 million will be living with dementia by 2030, and 115 million by 2050 (Alzheimer’s Disease International, 2013). In anticipation of these demographic changes, many countries, and in particular those within the G20 economic zone, have begun to develop and enact plans to address dementia as a national priority (Rosow et al., 2011). A key element of such policies has been to build dementia-friendly communities, and to reduce the stigma that people with dementia face. It is, therefore, important to understand the mechanisms that contribute to the formation of social attitudes to dementia. Hitherto, the role that dementia threat plays in this process has been largely neglected. The development of a psychometrically sound measure of dementia threat will enable further exploration of how personal experience of dementia, age, gender, or ethnicity contribute to wider social attitudes toward people living with dementia (Cheston et al., 2018) An improved understanding of these processes may contribute toward a more nuanced approach to the development of dementia-friendly communities.
Additionally, understanding more about the role of dementia threat may facilitate an improved understanding of how emotions (and their avoidance) impact dementia care. Just as there is evidence to suggest that thinking or reading about dementia promotes anxiety within the general population, and that this is reduced by strategies such as distancing, similar processes seem to take place amongst people caring for those with dementia (McKenzie & Brown, 2017). In order to prevent the emergence of anxiety, it has been suggested that professionals working in dementia care draw on a number of experiential avoidance strategies (McKenzie et al., 2017)—thoughts, memories, or behaviors that reduce the anxiety that they would otherwise experience. McKenzie et al. (2017) go as far as suggesting that these avoidance strategies may be associated with more frequent involvement in task-oriented forms of care that enable carers to avoid emotional engagement with the person for whom they are caring, and less use of person-centered forms of care. Although further work is clearly required to substantiate such claims, research in this area has been undermined by the absence of a reliable way of measuring the threat. The development of the ToDS will therefore facilitate a future examination of whether psychological mechanisms that protect the self against anxiety have an impact on attitude formation and care practices.
Footnotes
Acknowledgments
We thank participants in both studies. We recognize the contribution of the three Alzheimer Society monitors: Julia Burton, Louise Gillam, and Andra Houchen. Finally, we acknowledge the work of India Hart, who provided maternity cover for the trial coordinator, and Dr. Tony Ward, who chaired the study steering group.
Authors’ Note
Neither the funder nor the sponsor played any role in the research, and did not influence the formulation of the research questions, choice of study design, data collection, data analysis, or the decision to publish.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Alzheimer Society (Grant No. AS-PG-2013-13).
Notes
Author Biographies