
Abstract
This study is on the effects of spousal loss among older adults who continue to live independently after bereavement. Little longitudinal studies focus on this group, which is of special interest, since in many countries, care policy and system reform are aimed at increasing independent living among older adults. Using longitudinal data from a Dutch public data repository, we investigate the effects of spousal loss on psychological well-being, perceived quality of life, and (indication of) yearly health-care costs. Of the respondents who had a spouse and were living independently (N = 9,400) at baseline, the majority had not lost their spouse after 12 months (T12, n = 9,150), but 2.7% (n = 250) had lost their spouse and still lived independently. We compared both groups using multivariate regression (ordinary least squares) analyses. The results show that spousal loss significantly lowers scores on psychological well-being and perceived quality of life, but we found no effect on health-care costs.
Many Western populations are aging and therefore policy in many countries is currently aimed at extending independent living and postponing institutionalization among older adults, as is the case in the Netherlands (e.g., Ministry of Health Welfare and Sports, 2005; Organisation for Economic Co-operation and Development, 2011). Even after the death of a spouse, who is often also a source of informal care and support, older adults are supposed to continue to (want to) live independently, despite the fact that the death of a loved one is known to be one of the most stressful of all life events and the partner who stays behind is often vulnerable as well (Gallagher, Thompson, & Peterson, 1981; Holmes & Rahe, 1967). First, older spouses are often highly dependent on each other, as informal help provided by the spouse is very common among older adults (Timmermans, 2003). Second, older spouses have often had a relationship over a long time with a long history together and their lives are closely interwoven, for instance, due to traditional gender role division and dependency on help with daily tasks (Wolff & Wortman, 2006). Third, social support during the grieving process can be sparse because social networks of older adults are changing and contact frequency is often decreased (Cornwell, Schumm, Laumann, Kim, & Kim, 2014; van Tilburg, 1998), and in this life phase, health and mobility are often reduced which may be a barrier for participation and maintaining social contacts. Finally, spousal loss in late life may be very difficult as it often happens during a life phase in which not only social but also financial and adaptive resources are declining (Wolff & Wortman, 2006; Wortman & Silver, 1990).
Previous Research
Previous studies have shown that spousal loss in late life is associated with adverse outcomes. First, bereavement is associated with more physical health problems, depressive symptoms, and anxiety (e.g., Bennett, 1998; Stroebe, Schut, & Stroebe, 2007; Wingen & Otten, 2009); increased mortality risk (Boyle, Feng, & Raab, 2011); and greater use of medication and poorer health ratings (Thompson, Breckenridge, Gallagher, & Peterson, 1984). Also, it seems related to higher health-care costs and higher health service use (Prigerson, Maciejewski, & Rosenheck, 2000; Rolden, van Bodegom, & Westendorp, 2014; Wong, Elderkamp-de Groot, Polder, & van Exel, 2010). Health-care costs are higher among older adults who lost their spouse particularly because healthy years seem to be replace by years with chronic diseases (van den Berg, Lindeboom, & Portrait, 2011). Based on previous findings, we also expected that bereavement has an adverse association with psychological well-being and quality of life (Bond, Clark, & Davies, 2003; Fry, 2001). In sum, investigating the consequences of widowhood among community-dwelling older adults is of importance as spousal loss can have a major impact on health, well-being and health-care utilization, and cost of health care. As well as individual consequences, insight into the impact of spousal loss is of special interest for prevention and policy aiming at increasing participation and postponing institutionalization of community-dwelling older adults. What do they need and what should policymakers and formal and informal caregivers bear in mind in dealing with this growing group within society? Given the ongoing trend in which more seniors are living independently, it is important to have insight into their quality of life and well-being, especially for recently bereaved individuals.
Except for studies focusing on the effects of spousal loss on health-care costs, most studies on spousal loss among older adults usually have a cross-sectional research design and are based on small samples (Carr, Nesse, & Wortman, 2006). This limits studying the direct effects of widowhood over time and restricts causal inferences about the impact of loss of a spouse. Like stated by, for instance, Schaan (2013), the only way to investigate the effects of losing a spouse is to use data that observe the same individuals over time and compare the mental health status of people before and after becoming widowed with that of their (still) married counterparts. In addition, the fact that most studies are retrospective, that is, spousal loss has already occurred at the time of study, is troublesome because both selection and recall bias (i.e., a change in the memory of a given past distressing event) might occur. As highlighted by Carr et al. (2006), people who have lost their spouse might overestimate the effect of spousal loss on their feelings of anger and anxiety retrospectively, or more generally, changes in the level of grief over time might moderate the memory of past grief (Field, Thompson, & Gallagher-Thompson, 2006). Moreover, the vulnerability of bereaved people makes it less likely that they are willing to participate in research and also makes it ethically challenging to approach them for research participation, which may lead to selection biases in study designs (Stroebe, Sroebe, & Schut, 2003). This selection bias matters particularly when it is dependent upon the variable of interest/the object of the study, that is, the effects of bereavement. In sum, it is difficult to clearly unravel the consequences of spousal loss in a cross-sectional, retrospective study.
In the Netherlands, to our knowledge, limited studies have been conducted into the consequences of spousal loss specifically among community-dwelling older adults in a large sample and longitudinal design. Based on a large sample, but in a cross-sectional study design, Wingen and Otten (2009) found that recent widowhood among older adults was associated with poor psychological health. A longitudinal study based on Dutch health-care insurer data found an increase in health-care expenditure after widowhood among older adults (Rolden et al., 2014) but paid no attention to the psychological consequences. We add to this knowledge and focus on the Netherlands, as an interesting country to study because in terms of demographics, the incidence of widowhood, and the presence of an informal caregivers (social) network, Dutch older adults score fairly average compared with other European older adults (Verbeek-Oudijk, Woittiez, Eggink, & Putman, 2014). Although focusing on people aged more than 50 years living independently, Verbeek-Oudijk et al. (2014) show that, for instance, the age profile of the Dutch older population roughly matches with the rest of Europe. For the incidence of spousal loss, they conclude that “the Netherlands is in the large group around the European average” (p. 60) as roughly a fifth of all over-50s have (ever) dealt with the death of a partner. For some other relevant characteristics, they found that just under 70% of over-50s living independently in the Netherlands have a family network they can (potentially) rely on (the average across the countries studied is 66%), and that one in five only has a (potential) care network outside the household (for instance, adult children living away from home)—which is again around the average for the other European countries. Also, compared with other countries, the study of Verbeek-Oudijk et al. shows that the Netherlands spends an average percentage of gross domestic product on nonresidential long-term care. Considering this, findings among community-dwelling Dutch older adults might also apply to this population in other European countries.
In this study, we use existing data from the Dutch public data repository, the Older Persons and Informal Caregivers Survey Minimum Dataset (TOPICS-MDS; www.topics-mds.eu; Lutomski et al., 2013). This is a pooled data set combining longitudinal data of 32,210 older (65 and older) adults and 3,940 informal caregivers. The data set has previously been used, for instance, to assess the influence of ethnicity on frailty of community-dwelling older adults (Franse et al., 2018) and a study in which frailty profiles of older persons were developed (Looman et al., 2018). This large data set allows to study the effects of spousal loss among community-dwelling older adults because data are available before and after spousal loss. We compare older adults who lost their spouse and those who did not during the past year on diverse domains, namely, psychological well-being, perceived quality of life, and health-care costs. Based on previous findings and theories, we expect that health-care costs will increase and perceived quality of life and psychological well-being conversely will be lower due to spousal loss. We reduce the potential influence of selection and recall bias because of the longitudinal design (information on psychological well-being, perceived quality of life, and health-care costs is gathered both on T0 and T12) and by the use of the MDS that consists of studies originally collected for different research questions than the one we address on the effects of spousal loss.
Method
Data and Selection Criteria
We used data from the Older Persons and Informal Caregivers Survey Minimum Dataset (TOPICS-MDS). This pooled minimum data set was developed under the umbrella of the National Care for the Elderly Program of the Dutch Ministry of Health, Welfare, and Sports to promote research on physical, mental, and social health and well-being among older persons. TOPICS-MDS contains some standardized measures on, among other things, health status demographic information, morbidity, quality of life, functional limitations, mental health, social functioning, and health service utilization of the older persons for several data points in time (Lutomski et al., 2013). A total of 41 research projects contributed data to the pooled data set of TOPICS-MDS. Data were collected between the end of 2009/2010 and 2013 and the primary studies varied in study design, sampling method, data collection moments and frequency, and survey mode. For more information regarding the development and characteristics of the data set, see Lutomski et al. (2013). Regarding research ethics, at the moment of data collection, studies using TOPICS-MDS fell outside the remit of the Medical Research Involving Human Subjects Act (in Dutch WMO; Wet Medisch Wetenschappelijk Onderzoek met mensen). Therefore, such studies may be carried out in the Netherlands without additional approval by an accredited research ethics committee.
For our analyses on the effects of spousal loss on psychological well-being, perceived quality of life, and health-care costs, we selected respondents aged 65 years and older, with available data on baseline (T0) and at least one follow-up measurement after 12 months (T12). As studies varied in their start date and thus also follow-up date (after 12 months), so does the exact year-period covered in the different studies. For instance, whereas in some studies, the first moment of data collection (T0) was at the beginning of the year 2010 (and then again at the beginning of 2011, T12) in other, later studies, the first data collection took place at the end of 2012 (T0) and follow-up was at the end of 2013.
Next, respondents were selected when they reported they had a spouse at baseline (either married (96.6%, n = 9,091) or cohabiting/unmarried (3.4%, n = 319)) and who were not institutionalized at T0 nor between baseline and follow-up (T12). After applying the selection criteria and checks for validity and consistency between T0 and T12 (for instance, on age and/or gender), the study sample consisted of N = 9,400 community-dwelling older adults aged 65 to 97 years of which we have information available on T0 and T12.
Measures
Our dependent variables are psychological well-being, perceived quality of life, and indication of health-care costs. Psychological well-being was measured with the Rand-36 Mental Health subscale (van der Zee & Sanderman, 2012). The subscale consisted of five items asking respondents how often in the past 4 weeks they have felt (1) very nervous, (2) calm and peaceful, (3) downhearted and blue, (4) a happy person, and (5) down in the dumps so that nothing could cheer them up. Response categories varied from all of the time to none of the time. Scores were averaged and rescaled to produce an overall score between 0 and 100 with higher scores indicating a more positive emotional state (for more details, see Lutomski et al., 2013). Respondents’ perceived quality of life was assessed with a modified version of Cantril’s (1965) Self Anchoring Ladder: What score would you give your life at this moment (ranging from 0 to 10). Information about health-care costs in the past 12 months was gathered as follows: number of hospital admissions, length of hospital stay, number of urgent care visits to the general practitioner (GP; during evenings, weekend, or out-of-hours consultation in hospital), and number of hours receiving home care assistance. We calculated an indication of yearly health-care costs by multiplying use of hospital, urgent GP visits, and home care with the reference tariffs. We used reference tariffs from a Dutch standardized method for economic evaluation studies (Hakkaart-van Roijen, Tan, & Bouwmans, 2010). It should be noted that the measure we used for health-care costs is not as objective as, for instance, that used by Rolden et al. (2014) as, first, it is based on respondents’ own recall on how often and how long they utilized these health-care services and second, it only includes, for instance, urgent GP visits and no normal ones. For these reasons, we labeled this measure as an indication of yearly health-care costs. When respondents only indicated having used certain care but did not report the quantity, the indication of yearly health-care costs was coded as missing.
As gender, age, socioeconomic status, and ethnicity are supposed or known to influence or intervene with the effects and responses to spousal loss (e.g., Carr et al., 2006; Collins, 2018; Horwitz, White, & Howell-White, 1996), we control for several of these variables. Demographic information included in the analyses is as follows: age, gender (man/woman), education level (low, intermediate, and high), country of origin (the Netherlands, or another country), and multimorbidity, which was defined as having two or more chronic conditions. Finally, spousal loss during the last year (i.e., between T0 and T12) is operationalized as yes or no.
Statistical Analyses
Our study objective is to investigate whether spousal loss has a negative effect in itself on older adults’ psychological well-being, perception of quality of life, and the indication of health-care costs, that is, does spousal loss in the past year yield (more) negative effects on those health measures compared with among older adults who did not lose their spouse? Or can no such clear effect be distinguished and are previous reported results merely the result of a so-called recall effect or selection/small sample sizes? We investigate this question based on longitudinal data on 250 older adults who did and 9,150 people who did not experience the loss of a spouse during the last year, and control for age, gender, education level, multimorbidity, and country of origin.
First, descriptive analyses were conducted to describe the study sample at baseline (T0) and follow-up (T12), irrespective of spousal loss. Next, three pairs of multivariate regression (Ordinary Least Squares) analyses were conducted for each of our dependent variables. In Model 1, we test the effects of initial scores (T0) for psychological well-being, perceived quality of life, and indication of health-care costs on respondent’s scores on these variables at T12. Because answers to subjective measures such as psychological well-being and perceived quality of life might also reflect general state of mind, it is important to account for the baseline values of such measures. The same holds for the indication of yearly health-care costs, which might have increased for particular respondents, regardless of spousal loss. This controlling for baseline values is an additional added value of conducting longitudinal research, as we really capture the change and not merely general differences between people in this respect. In Model 2, we control for age, gender, education level, multimorbidity, and country of origin at T12. Finally, in Model 3, spousal loss (yes/no) is added to see whether there is an additional and independent effect on the change in the dependent variables compared with those who did not experience spousal loss in the previous year. Analyses were conducted using STATA version 15.1.
Results
Descriptive Results
Of the total study sample (N = 9,400), a total of n = 250 (2.7%) older adults had lost their spouse within 12 months and n = 9,150 did not. Background characteristics of the study sample are shown in Table 1. As displayed in Table 2, the average age of older adults who are confronted with spousal loss is higher compared with the nonbereaved older adults and also higher compared with the mean age of the total study sample. An independent t test shows that respondents who lost their spouse are indeed slightly older (statistically significant compared with participants who did not, p = .000, not in table). In addition, gender is not equally distributed among the bereaved versus nonbereaved, as more women experienced spousal loss compared with men (4.3% vs. 1.4%). This is in line with the fact that women have a higher life expectancy than men and are therefore surviving men. Intermediate- and high-educated people are less often widowed than the low-educated people. No differences between country of origin (Netherlands or other country) in the occurrence of spousal loss were found nor with respect to multimorbidity.
Background Information for the Total Study Sample.
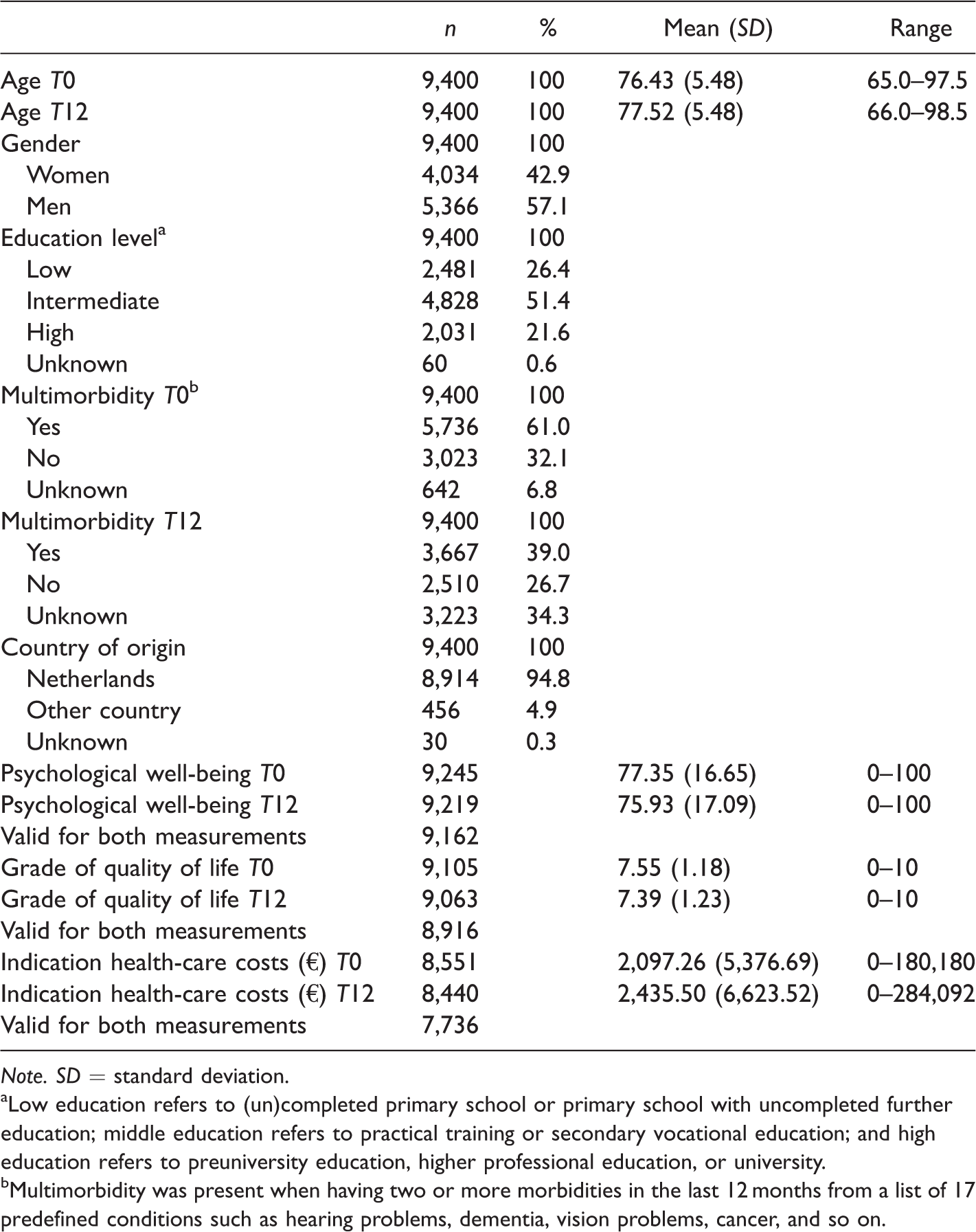
Note. SD = standard deviation.aLow education refers to (un)completed primary school or primary school with uncompleted further education; middle education refers to practical training or secondary vocational education; and high education refers to preuniversity education, higher professional education, or university.bMultimorbidity was present when having two or more morbidities in the last 12 months from a list of 17 predefined conditions such as hearing problems, dementia, vision problems, cancer, and so on.
Background Variables of Older Adults Who Had Lost Their Spouse (T12) and Those Who Had Not.
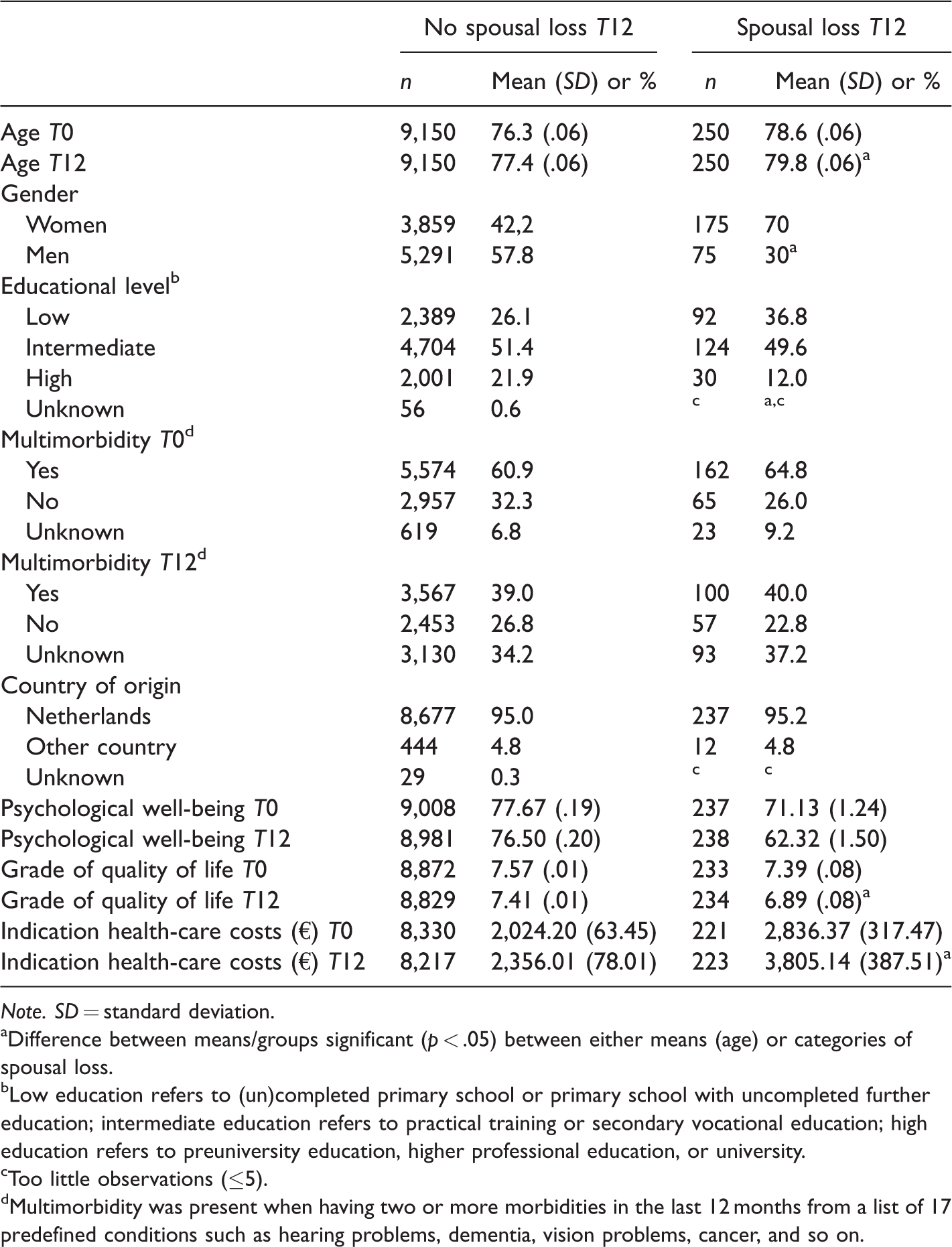
Note. SD = standard deviation.aDifference between means/groups significant (p < .05) between either means (age) or categories of spousal loss.bLow education refers to (un)completed primary school or primary school with uncompleted further education; intermediate education refers to practical training or secondary vocational education; high education refers to preuniversity education, higher professional education, or university.cToo little observations (≤5).dMultimorbidity was present when having two or more morbidities in the last 12 months from a list of 17 predefined conditions such as hearing problems, dementia, vision problems, cancer, and so on.
Both the scores for psychological well-being and grade of quality of life diminish more among respondents who did loss their spouse compared with those who did not. Likewise, health-care costs increase. Although, for instance, psychological well-being was already lower among older adults facing spousal loss in the upcoming year (possible due to the burden of care tasks or worries about a sick partner), the difference of 71.13 versus 62.32 is still striking.
Multivariate Regression Analyses (Ordinary Least Squares) Results
Results of the multivariate regression analyses are presented in Table 3. As might be expected, psychological well-being at T0 strongly predicts well-being a year later. This probably can be best characterized as someone’s general state of mind, which does not change much over time. The second model includes the control variables. Both age and gender (being a women) negatively effect psychological well-being. In other words, as older people age, their well-being generally decreases and women score worse in terms of psychological well-being than men. In a similar vein, the prevalence of multimorbidity has a negative effect on psychological well-being among older adults, while older adults with an intermediate or higher educational level score higher on psychological well-being compared with their low-educated counterparts. In Model 3, adding spousal loss during the last 12 months showed that this has an additional negative effect on psychological well-being among those who experienced such a loss. Compared with those who did not lose their spouse, those who did score significantly lower on psychological well-being, holding other things constant. The effect of spousal loss on psychological well-being (β = −.08, p < .001) is comparable with multimorbidity in magnitude, which is generally recognized as having a persistent effect on psychological well-being. Although it increased only modestly in the last model, the variance explained is high (R2 = .45).
. Results of Ordinary Least Squares Regression Analyses (β Values).
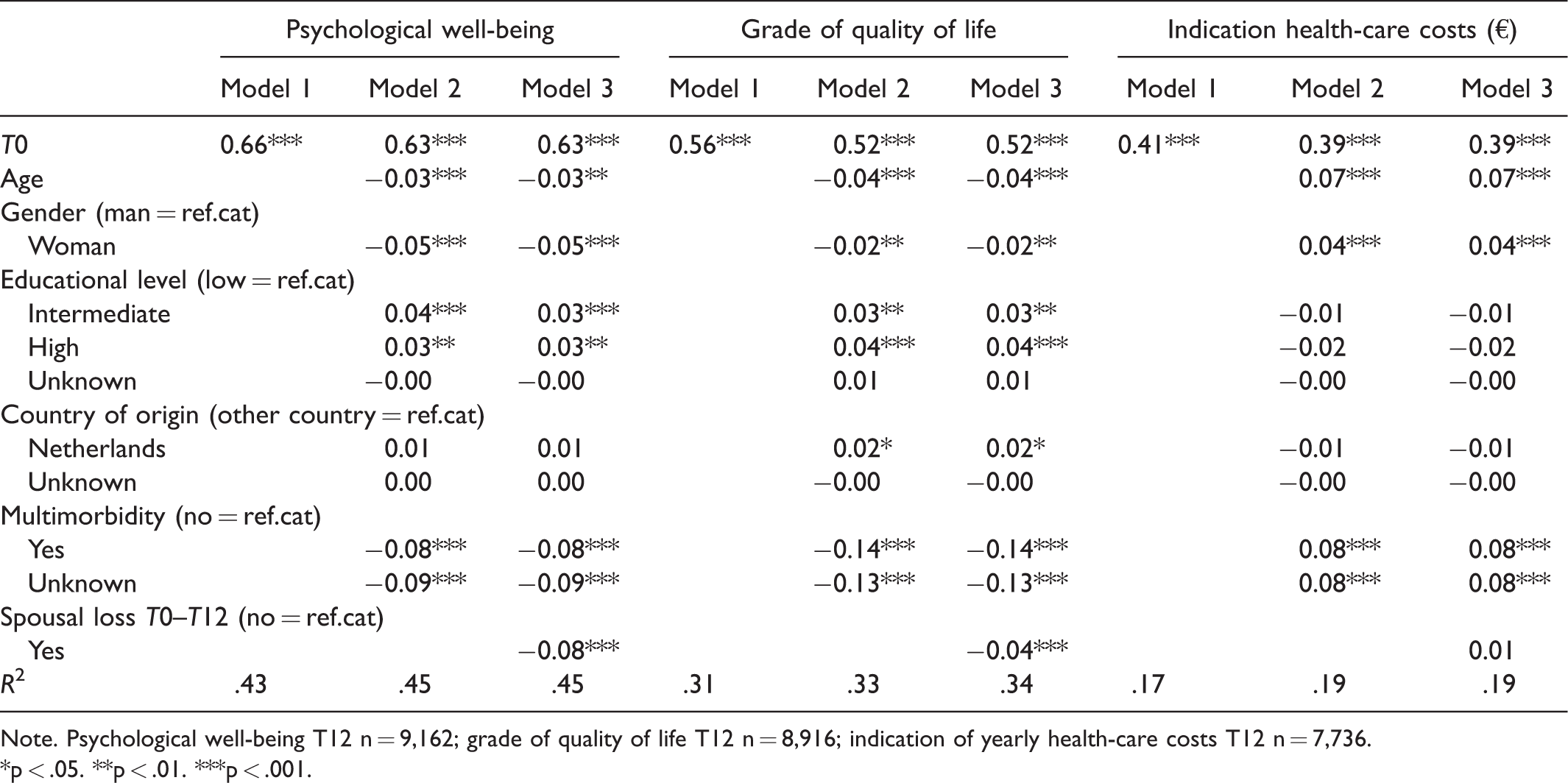
Note. Psychological well-being T12 n = 9,162; grade of quality of life T12 n = 8,916; indication of yearly health-care costs T12 n = 7,736.*p < .05. **p < .01. ***p < .001.
Also, the respondents’ perceived quality of life at T0 was a significant indication for the perceived quality of life 1 year later (Table 3, grade of quality of life, Model 1). Older respondents, women, lower educated respondents, and respondents from other countries of origin than the Netherlands graded their quality of life significantly lower. Also, respondents who reported multimorbidity scored lower on perceived quality of life than those who did not (Model 2). From the third model, it becomes clear that respondents who lost their spouse during the previous year also reported a lower perceived quality of life at T12 compared with respondents who were not confronted with spousal loss. The explained variance in the respondents’ own grade of their quality of life is quite good as well (31% in Model 1 and 34% in Model 3).
Finally, for the indication of yearly health-care costs, first of all, it should be noted that the R2 is relatively low compared with the models for psychological well-being and perceived quality of life (Table 3, indication health-care costs [€], Model 1 R2 = .17 and Model 3 R2 = .19). This implies that we are less able to predict any change in the indication of yearly health-care cost in the year after bereavement compared with the other two outcome variables. Again, indication of health-care cost at T0 was a strong predictor for the yearly health-care costs 1 year later. In the second model, including the control variables, it was found that age and gender (being a women) were associated with higher health-care costs. In other words, older respondents and women have higher health-care costs compared with their younger and male counterparts. Not surprisingly, multimorbidity was also related to higher health-care costs at T12. In the third model (Table 3, indication health-care costs [€], Model 3), for the additional effects of spousal loss on the (indication) of health-care cost, we find no significant effects of the costs made at T12, which implies that contrary to psychological well-being and perceived quality of life, we do not find an effect of spousal loss on the indication of health-care costs in the year after the loss of the spouse. In addition, interactions between gender and spousal loss were tested for psychological well-being, perceived quality of life, and indication of health-care costs and were not significant.
Discussion
As expected, community-dwelling older adults who were confronted with spousal loss in the last year reported lower psychological well-being and perceived quality of life compared with older adults who did not lose their spouse. This was in line with previous findings from predominantly cross-sectional and small-scale research that bereavement is related to diverse psychological reactions and the grieving process may cause mental disorders or complications (e.g.,; Bennett, 1998; Stroebe et al., 2007; Wingen & Otten, 2009). The effect of spousal loss on physical health problems and use of medical services has been found in other studies (e.g., Stroebe et al., 2007; Thompson et al., 1984). The fact that we found rather small effects in magnitude might be because we do not suffer from recall bias (due to memory bias), which appears to be particularly important when studying older people (because older people are worse in recalling). Not dealing with this might provide slightly larger effects (Carr et al., 2006; Knäuper et al., 2016). Contrary to what we expected based upon previous research (Prigerson et al., 2000; Rolden et al., 2014; Wong et al., 2010), spousal loss did not appear to have an effect on the indication of health-care costs. However, this finding should be considered in the light of some limitations in the measure we used for indication of health-care costs. As mentioned, first, we used self-reported data on health-care utilization instead of data from databases of, for instance, health insurance companies or other official national registries which are more complete and objective. Second, our measure of health-care costs was limited to hospital admission, urgent care visits by the GP, and home care assistance; thus costs of normal GP visits, paramedical care, medication, and long-term care were not taken into account. Especially, long-term care utilization might be related to spousal loss (Wong et al., 2010). Hence, our finding that spousal loss did not have an effect on health-care costs should be interpreted with caution. Also, Rolden et al. (2014) found changes in health-care expenditure 42 months after loss of a spouse, so maybe our time span simply was too short to find any effects.
Strengths and Limitations
The longitudinal data of 9,400 community-dwelling older adults and the comparison between those who were and who were not confronted with spousal loss made it possible to study the causal effect of spousal loss based on a large sample. In contrast to most studies in this field, we were able to investigate the changes instead of retrospectively asking about changes in subjective factors such as psychological well-being and perceived quality of life. The use of a large data set which was initially collected for different purposes limits the risk of so-called recall and self-selection bias in which a respondent’s decision to participate might be related to the topic of the research. Finally, instead of focusing on just one possible effect of spousal loss, we were able to investigate three outcome measures at the same time.
However, this study has limitations as well. First, the TOPICS-MDS is a pooled data set and the collection and contribution of date was mandatory on all the primary studies. Most researchers in the primary studies did not use the TOPICS-MDS data themselves, which may have caused less attention to be given to the quality of the data. Although administrators of the TOPICS-MDS data recovered some mistakes and inconsistencies, we were still confronted with data errors. During the screening stage of the data, selection of the study sample, and checking data, we took conservative stands; in the event of any doubt, we excluded cases or coded values as missing. Related to using secondary data of this kind, we did not have any information about loss of follow-up and reason for dropout. Nevertheless, the distribution of gender, marital status, and living situation among the respondents is in line with the distribution in the overall Dutch population aged 65 years and older. Another limitation was that we had no information about the exact time spousal loss occurred, that is, it could have occurred anytime during the year of data collection. Consequently, we were not able to control for the exact time since spousal loss. Finally, we were not able to consider the circumstances and context preceding spousal loss, whereas it is known that when evaluating the effect of spousal loss, it is important to consider the social context and condition (for instance, quality of the relationship) preceding this loss (Carr et al., 2006). Spousal loss may be sudden or anticipated at the end of a long period of stressful caregiving, which play a role in the consequences (Carr, House, Wortman, Nesse, & Kessler, 2001).
Implications
Regarding policy implications, the results of this study highlight the importance of monitoring community-dwelling older adults who have recently lost their spouse, as this group is found to be vulnerable for physical and psychological health problems. In the Netherlands, nurses from home care organizations are limited in their time and are restricted to care for older adults who have an official indication for a need for frequent medical care. When a sick spouse has deceased, the remaining partner might not fulfill the criteria to be eligible for home care anymore. However, a promising option might be for the home care organization involved in the care of the deceased spouse to continue to support the remaining spouse after the bereavement, as these professionals may already have established a relationship with the widowed spouse. The existing community organizations previously known to older adults might also be used for bereavement support (Bellamy, Gott, Waterworth, McLean, & Kerse, 2014). In addition, the informal network is increasing important in providing older people the care they need in order to keep living independently. Also, in the Netherlands, a country with “high public spending and low family responsibility, p. 12,” the focus is shifting toward more informal care by the family, the social network, and the community (Verbeek-Oudijk et al., 2014). This increased rely on informal care in turn causes concerns about the sustainability of the care system and caregivers’ subjective well-being and overload (Verbakel, Metzelthin, & Kempen, 2016). Knowledge of effective interventions that enhance resilience or prevent problems among older adults who have lost their spouse and their social network is of importance. Finally, qualitative research can add to current knowledge as it may provide insight into the feelings and emotions of older adults who have lost their spouse and the circumstances and context in which bereavement and grieving occur.
Conclusion
In line with previous findings and our expectations, we found that spousal loss among older adults had a negative effect on psychological well-being and perceived quality of life. Contrary to previous findings, we did not find an effect of spousal loss on health-care costs. However, we cannot be conclusive about this finding due to limitations in the measure we used for health-care costs. Although using a pooled secondary data set comes with some challenges and limitations, we were able to study causal effects of spousal loss on three different outcomes among a large sample (N = 9,400) of community-dwelling older adults. The findings of our study underline the vulnerability of community-dwelling older adults who are confronted with spousal loss and the potential effects spousal loss can have on physical and psychological health.
Footnotes
Acknowledgments
This study makes use of data generated by the Older Persons and Caregivers Survey Minimum Dataset (TOPICS-MDS). A full list of the investigators is available from ![]() . Funding for the TOPICS-MDS project was provided by the National Care for the Elderly Program on behalf of the Organization of Health Research and Development (ZonMW—the Netherlands, Grant Reference 633.400.011).
. Funding for the TOPICS-MDS project was provided by the National Care for the Elderly Program on behalf of the Organization of Health Research and Development (ZonMW—the Netherlands, Grant Reference 633.400.011).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Netherlands Organization for Health Research and Development (ZonMW—the Netherlands Grant Reference: 60–63300-98–505).