
Abstract
Objective
This narrative review examines the intersection of serial infidelity, coercive control, and psychological abuse as an under-recognised form of betrayal trauma.
Methods
Guided by PRISMA principles, a systematic search of four databases (PsycINFO, PubMed, Scopus, and Web of Science) identified 47 peer-reviewed studies published between 1990 and 2025 that met inclusion criteria. Studies were included if they examined repeated infidelity within intimate relationships, associated patterns of coercive control, gaslighting (defined here as psychologically manipulating a person into questioning their own perceptions, memory, or sanity), or the psychological sequelae of sustained relational betrayal. Data were analysed using a narrative synthesis approach to identify convergent theoretical, clinical, and diagnostic themes.
Results
Findings indicate that serial infidelity frequently co-occurs with coercive and gaslighting behaviours, producing psychological effects consistent with trauma responses observed in intimate partner violence. Despite these effects, relational betrayal involving sustained deception and control remains largely absent from psychiatric nosology, contributing to diagnostic blind spots and therapeutic misclassification.
Conclusion
This review highlights the distinction between moral judgement of behaviour and the clinical recognition of trauma-based harm. An evidence-informed framework is proposed for identifying betrayal trauma within diagnostic and clinical settings, emphasising trauma-informed assessment and intervention rather than behavioural or personality-based explanations.
Keywords
Introduction: When Infidelity Becomes Abuse
Infidelity within intimate relationships is most often conceptualised as a moral, relational, or interpersonal issue rather than a potential source of psychological trauma. Existing literature has examined predictors of infidelity, relationship dissatisfaction, and post-affair repair, yet comparatively little attention has been given to the conditions under which repeated infidelity may operate as a mechanism of psychological abuse.1-3 As a result, individuals presenting with trauma-related symptoms following sustained relational betrayal are frequently misclassified diagnostically, minimised clinically, or conceptualised through maladaptive personality or attachment frameworks rather than recognised as trauma-exposed patients.4-6
It is important to distinguish between infidelity as a relational rupture and infidelity as a form of psychological harm. Not all infidelity constitutes abuse. Situational or isolated infidelity may occur in the context of unmet relational needs, impaired communication, developmental transitions, or relational conflict and does not inherently result in trauma-related psychopathology.1-3 However, emerging evidence indicates that serial infidelity combined with deception, power imbalance, coercive control, and psychological invalidation may produce psychological effects consistent with recognised trauma syndromes.7-10
What Counts as Infidelity? Expanding the Clinical Definition
Traditional clinical definitions of infidelity have focused primarily on violations of sexual exclusivity. Contemporary relational dynamics, however, increasingly involve emotional infidelity, digital infidelity, and concealed parallel relationships that may not involve physical sexual contact but nonetheless constitute sustained breaches of trust.11-13 From a trauma-informed perspective, the defining feature is not the sexual act itself, but the pattern of deception, concealment, and manipulation of reality imposed on the non-offending partner.7,9
Serial infidelity becomes clinically significant when embedded within a relational context characterised by repeated lying, gaslighting, intermittent reinforcement, blame-shifting, and threats of abandonment. In such cases, betrayal is not a discrete event but a chronic relational condition that progressively erodes epistemic trust and psychological safety. Individuals exposed to these dynamics may experience persistent hypervigilance, emotional dysregulation, cognitive confusion, and a destabilised sense of self, reflecting adaptations to ongoing relational threat.
Diagnostic Blind Spots in Relational Trauma
Despite substantial evidence linking coercive control and psychological abuse to trauma-related outcomes, psychiatric diagnostic frameworks continue to prioritise overt physical or sexual violence as qualifying stressors.10,14-16 Consequently, individuals exposed to sustained relational betrayal are often diagnosed with adjustment disorders, anxiety disorders, or personality disorders, particularly borderline personality disorder, rather than trauma-related conditions. This diagnostic pattern risks pathologising adaptive survival responses to chronic relational harm.
Trauma scholars have cautioned against the reification of diagnostic categories when they obscure underlying mechanisms of injury. Rather than advocating for the creation of a new diagnostic entity, contemporary trauma models support the recognition of relational betrayal involving coercive control as a qualifying traumatic stressor within existing frameworks. In particular, ICD-11’s conceptualisation of Complex PTSD provides a clinically appropriate structure for understanding the cumulative psychological impact of sustained relational deception and control.17-19
Aims of the Present Review
The present narrative review synthesises peer-reviewed literature examining serial infidelity in conjunction with coercive control, gaslighting, and psychological abuse. The review has three primary aims. First, it seeks to differentiate non-abusive infidelity from patterns of relational betrayal associated with trauma-related outcomes. Second, it examines how sustained relational deception produces psychological effects analogous to those observed in intimate partner violence. Third, it explores diagnostic and clinical implications, with a particular focus on preventing misdiagnosis and improving trauma-informed assessment and intervention.
Methods
Design
This study employed a PRISMA-guided narrative review to synthesise existing literature examining serial infidelity in the context of coercive control, gaslighting, and psychological abuse. A narrative review methodology was selected to allow integration of heterogeneous empirical findings with established trauma, attachment, and coercive control frameworks, while maintaining transparency and methodological rigour consistent with PRISMA principles.
Search Strategy
A systematic literature search was conducted across four electronic databases: PsycINFO, PubMed, Scopus, and Web of Science. Searches were limited to peer-reviewed articles published in English between 1990 and 2025. Search terms were developed iteratively and combined keywords relating to infidelity, betrayal trauma, coercive control, gaslighting, psychological abuse, and trauma-related outcomes. Boolean operators and database-specific subject headings were used to maximise sensitivity and relevance.
Search Strategy and Study Selection Summary
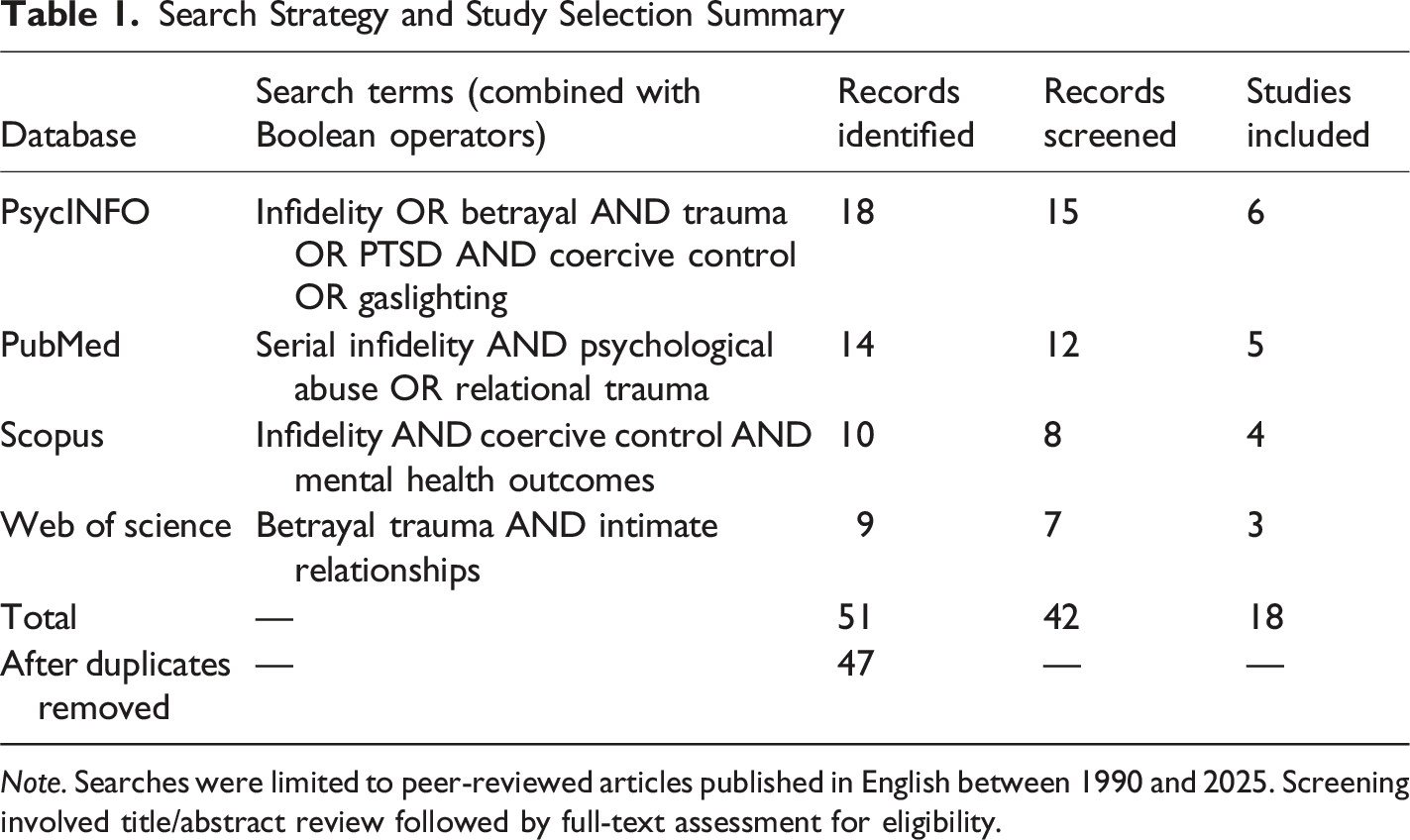
Note. Searches were limited to peer-reviewed articles published in English between 1990 and 2025. Screening involved title/abstract review followed by full-text assessment for eligibility.
Eligibility Criteria
Studies were eligible for inclusion if they met one or more of the following criteria (a) examined repeated or serial infidelity within intimate partner relationships; (b) investigated psychological, emotional, or trauma-related outcomes associated with relational betrayal; (c) addressed mechanisms such as deception, gaslighting, coercive control, or power imbalance; or (d) provided clinically relevant theoretical or empirical insights into betrayal trauma or relational abuse.
Studies were excluded if they focused exclusively on single-incident infidelity without relational context, non-intimate relationships, or moral, cultural, or sociological discussions of infidelity without psychological or clinical relevance.
Study Selection
The initial database search identified 47 records meeting the inclusion criteria following removal of duplicates. Titles and abstracts were screened for relevance, followed by full-text review to confirm eligibility. The study selection process is summarised in a PRISMA-style flow diagram (Figure 1). Eighteen studies were included in the narrative synthesis. PRISMA-style flow diagram of study selection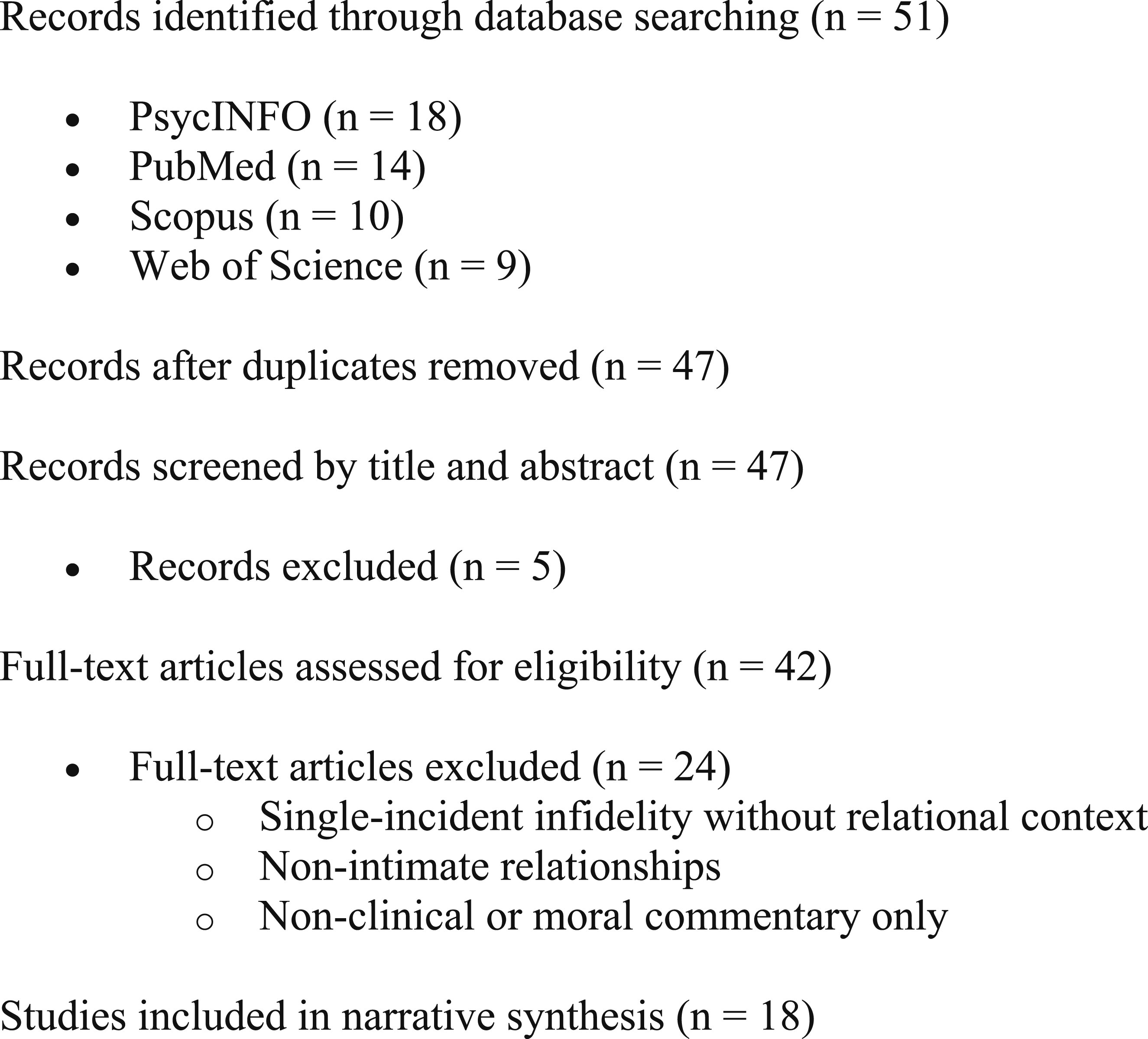
Data Extraction
Data were extracted manually and included author(s), year of publication, study design, population characteristics, primary focus (eg, infidelity patterns, coercive dynamics, trauma outcomes), and key findings relevant to betrayal trauma and psychological harm. Given substantial heterogeneity in study designs, outcome measures, and analytic approaches, quantitative meta-analysis was not appropriate.
Quality Appraisal
Included studies were appraised using the Critical Appraisal Skills Programme (CASP) tools appropriate to study design. Quality indicators included clarity of aims, methodological coherence, relevance to the review question, and transparency of findings. Studies were not excluded solely based on quality appraisal; rather, appraisal outcomes were used to contextualise the strength and limitations of evidence within the narrative synthesis.
Summary of Quality Appraisal Using CASP Criteria
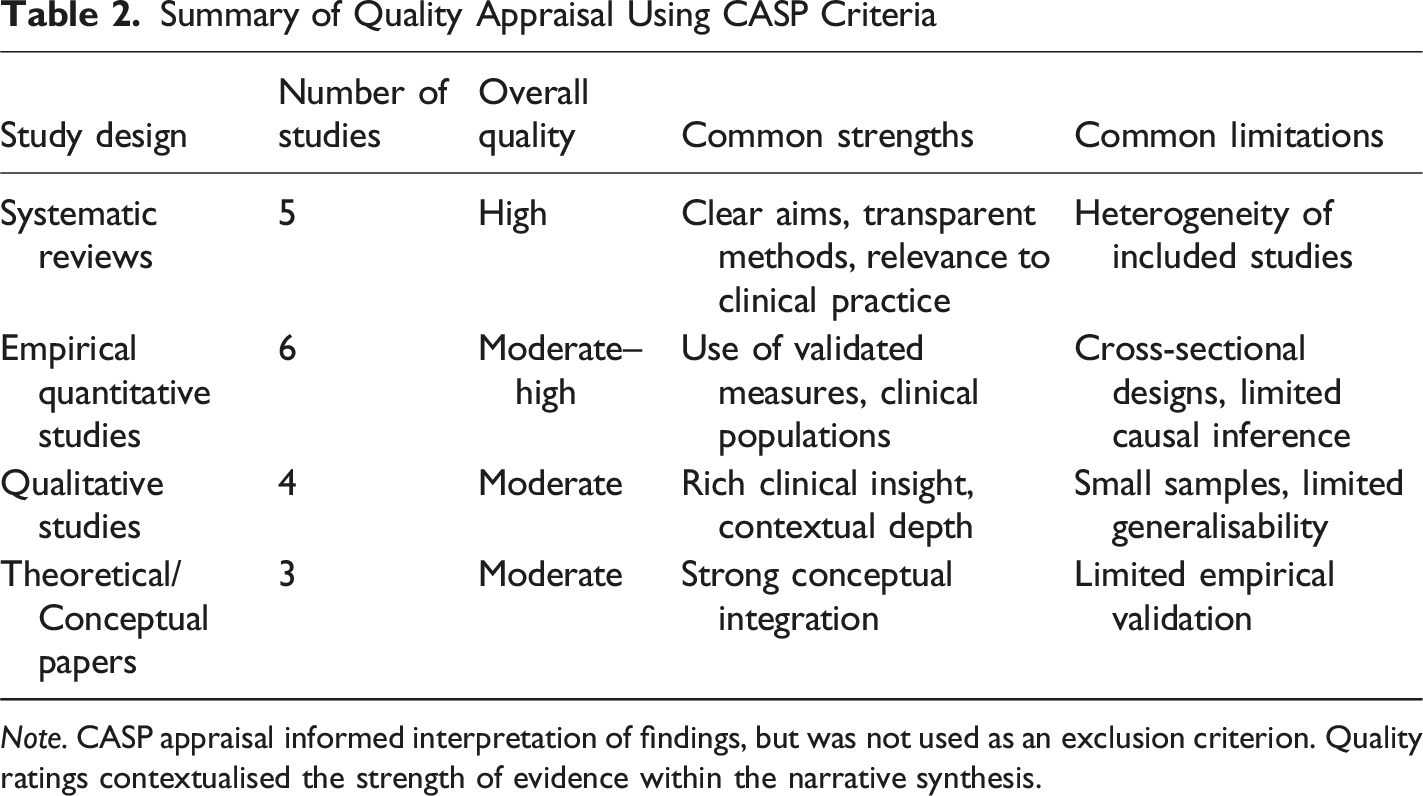
Note. CASP appraisal informed interpretation of findings, but was not used as an exclusion criterion. Quality ratings contextualised the strength of evidence within the narrative synthesis.
Data Synthesis
A narrative synthesis approach was employed to integrate findings across included studies. Extracted data were coded thematically, and recurring patterns were identified through iterative comparison. Themes were refined through repeated review and clustered into higher-order conceptual domains reflecting mechanisms of harm and clinical impact.
Thematic Synthesis of Findings Across Included Studies
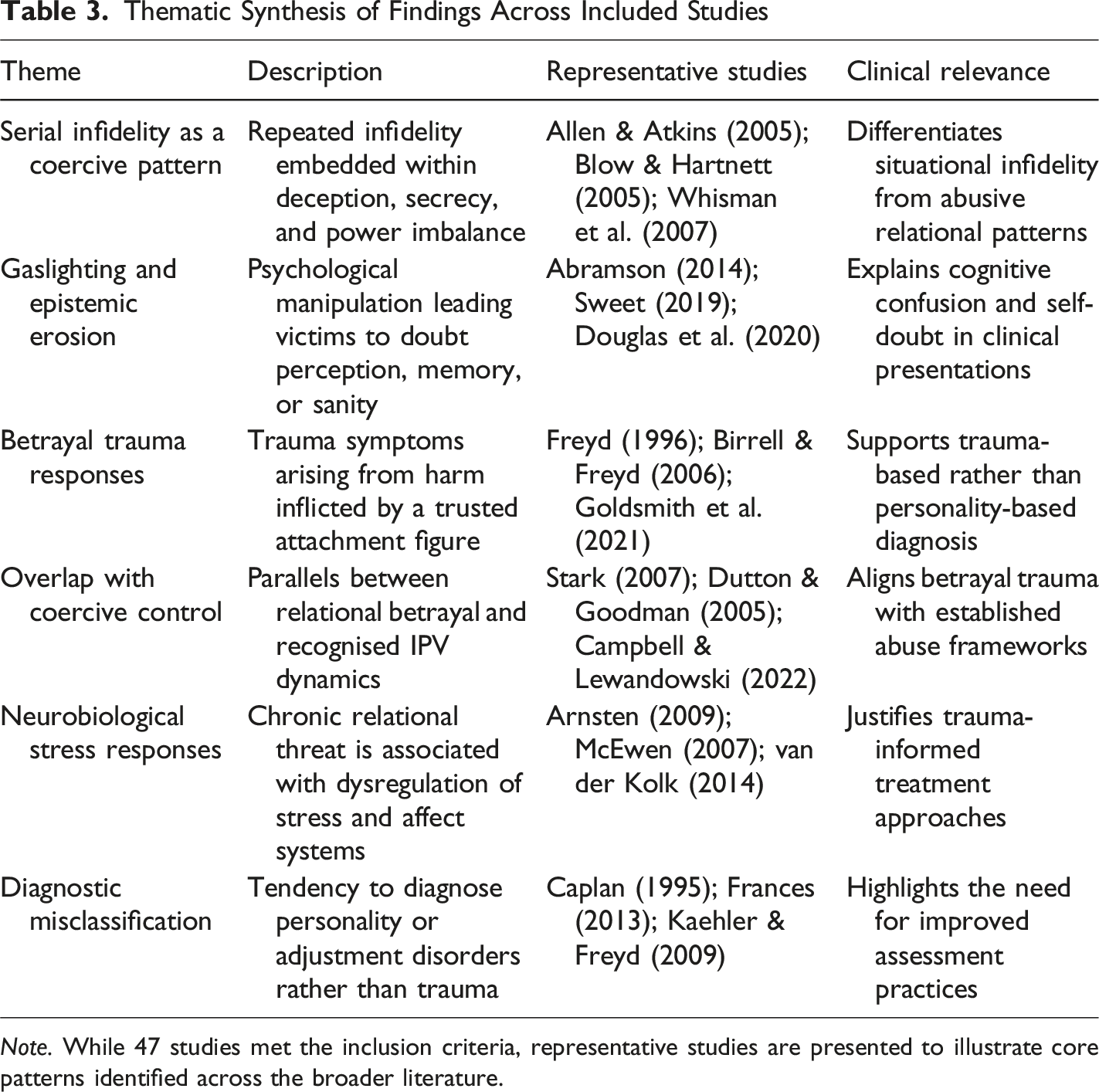
Note. While 47 studies met the inclusion criteria, representative studies are presented to illustrate core patterns identified across the broader literature.
Results
The narrative synthesis of the 47 included studies identified six interrelated themes describing the psychological impact of serial infidelity when embedded within patterns of deception, coercive control, and psychological abuse. While the included literature varied in design, population, and methodological approach, convergent findings across empirical, theoretical, and clinical studies revealed consistent mechanisms of harm and clinically significant outcomes.1,3,7,10,14
Serial Infidelity as a Coercive Relational Pattern
Across the literature, serial infidelity was distinguished from situational or isolated infidelity by its repetitive, concealed, and relationally destabilising nature. Multiple studies indicated that when infidelity occurred alongside persistent deception, secrecy, and power imbalance, it functioned less as a discrete relational transgression and more as an ongoing coercive pattern. This distinction was evident in relationship-focused studies identifying chronic betrayal as qualitatively different from single-incident affairs, particularly in its association with psychological distress and relational trauma.1-3,20
These findings support the position that serial infidelity should be evaluated within its broader relational context rather than assessed as a stand alone behaviour. Representative studies illustrating this pattern are summarised in Table 3.
Gaslighting and Erosion of Epistemic Trust
A prominent theme across studies was the role of gaslighting in amplifying the psychological impact of serial infidelity. Gaslighting behaviours—including denial, minimisation, blame-shifting, and distortion of events—were repeatedly associated with erosion of epistemic trust, whereby individuals became uncertain of their own perceptions, memories, and reasoning. Philosophical, sociological, and clinical studies converged in identifying gaslighting as a mechanism that transforms relational betrayal into a psychologically destabilising experience.21-23
Victims exposed to sustained gaslighting commonly reported confusion, self-doubt, hypervigilance, and cognitive disorganisation, symptoms frequently misattributed to anxiety or personality pathology. These findings reinforce the importance of assessing psychological manipulation when evaluating post-infidelity distress.10,21,23
Betrayal Trauma Responses
The synthesis revealed strong alignment between experiences of serial infidelity within coercive relationships and betrayal trauma theory, which conceptualises trauma arising from harm inflicted by a trusted attachment figure. Studies grounded in betrayal trauma theory demonstrated that victims may suppress awareness of harm to preserve relational attachment, particularly when emotional, financial, or familial dependencies are present.24-27
Across clinical and empirical studies, betrayal trauma was associated with symptoms consistent with post-traumatic stress, including intrusive thoughts, affect dysregulation, dissociation, and impaired self-concept. These outcomes were not contingent on physical or sexual violence, underscoring the relevance of relational context in trauma exposure.24,26,27
A substantial subset of studies identified parallels between serial infidelity and recognised forms of coercive control. Patterns of surveillance, intermittent reinforcement, emotional withdrawal, and threats of abandonment mirrored dynamics observed in intimate partner violence literature. These findings support the conceptualisation of serial infidelity, when embedded within coercive dynamics, as a form of psychological abuse rather than a purely relational or moral issue.14,28-30
This overlap provides a clinically and theoretically coherent framework for understanding why individuals exposed to sustained relational betrayal may present with trauma-related symptoms comparable to those observed in survivors of other forms of intimate partner abuse.
Neurobiological Stress Responses
Several studies examined the neurobiological correlates of chronic relational stress, indicating that sustained exposure to relational threat may disrupt stress-regulation systems, including prefrontal cortical functioning and limbic reactivity. Although neuroimaging studies specific to infidelity were limited, convergent evidence from trauma and stress literature supports the plausibility of neurobiological dysregulation in individuals exposed to prolonged relational betrayal.31-35
These findings lend biological credibility to clinical observations of hyperarousal, emotional dysregulation, and impaired executive functioning reported by patients following sustained betrayal.31,32,35
Diagnostic Misclassification and Clinical Consequences
Across the literature, a recurring concern was the misclassification of betrayal trauma responses as personality disorders, adjustment disorders, or mood disorders. Several studies highlighted a tendency to attribute emotional instability, interpersonal sensitivity, or identity disturbance to intrinsic pathology rather than contextual trauma exposure.36-39
This diagnostic pattern carries significant clinical consequences, including inappropriate treatment planning, invalidation of lived experience, and delayed trauma-informed intervention. The findings underscore the need for assessment frameworks that account for relational context, coercive dynamics, and cumulative betrayal when evaluating psychological distress.36,38,40
Discussion
The findings of this narrative review indicate that serial infidelity, when embedded within patterns of deception, coercive control, and psychological manipulation, can function as a clinically significant form of relational trauma. Across diverse study designs and theoretical frameworks, convergent evidence suggests that the psychological sequelae associated with sustained relational betrayal are comparable to trauma responses observed in other forms of intimate partner abuse.7,10,14,28-30 These findings challenge prevailing assumptions that infidelity-related distress is inherently transient, moral, or relational in nature rather than trauma-based.
A central contribution of this review is the clarification that not all infidelity constitutes abuse. Situational or isolated infidelity, while often emotionally distressing, does not consistently produce trauma-related psychopathology.1-3 In contrast, trauma-relevant outcomes emerge most reliably when infidelity is serial, concealed, and reinforced through coercive or gaslighting behaviours.7-10,21-23 This distinction is clinically critical, as failure to differentiate between these patterns risks both over-pathologising relational conflict and under-recognising genuine psychological harm. The evidence supports a contextual rather than behavioural approach to assessment: it is not the act of infidelity itself that predicts trauma outcomes, but the relational environment in which it occurs, particularly the presence of power asymmetry, epistemic invalidation, and chronic psychological threat.14,21,36
Across the reviewed literature, gaslighting emerged as a pivotal mechanism through which serial infidelity becomes psychologically injurious. By systematically undermining an individual’s trust in their own perceptions, memories, and reasoning, gaslighting erodes epistemic agency and contributes to cognitive disorganisation, self-doubt, and emotional dysregulation.21-23,36 These effects align closely with contemporary trauma models emphasising disruption to meaning-making, identity coherence, and affect regulation.24-27,31 Within this context, symptoms frequently interpreted as emotional instability or personality dysfunction may more accurately reflect adaptive responses to sustained relational threat, underscoring the importance of assessing psychological manipulation and epistemic injury when evaluating post-infidelity presentations.36-39
The review also highlights a consistent pattern of diagnostic misclassification among individuals exposed to sustained relational betrayal. Personality disorder diagnoses, particularly borderline personality disorder, appear disproportionately in clinical contexts where relational harm is minimised or conceptualised as mutual conflict rather than coercive abuse.36-39 This tendency reflects broader diagnostic blind spots within psychiatric nosology, which continues to privilege overt physical or sexual violence as qualifying traumatic stressors.14,17-19 Consistent with contemporary trauma scholarship, the present findings do not support the creation of a new diagnostic category. Rather, they support the application of existing trauma frameworks—most notably ICD-11 Complex PTSD—to presentations involving prolonged relational betrayal accompanied by coercive control.17-19,24,31 Conceptualising such presentations as trauma-related avoids pathologising adaptive survival responses and facilitates more appropriate treatment planning.
Substantial overlap was observed between serial infidelity within coercive relationships and established models of coercive control. Patterns such as intermittent reinforcement, emotional withdrawal, surveillance, and threats of abandonment closely parallel dynamics documented in the intimate partner violence literature.14,28-30 Recognising this overlap allows relational betrayal to be situated within a coherent abuse framework rather than treated as a peripheral or purely relational issue. This integration also provides a practical bridge between trauma research and clinical practice, offering clinicians a structured lens through which to evaluate relational dynamics that may otherwise be dismissed or normalised.
Taken together, the findings underscore the importance of trauma-informed assessment approaches that attend to relational context, power dynamics, and psychological manipulation. Failure to recognise betrayal trauma risks invalidating patient experiences, delaying effective intervention, and reinforcing self-blame.36,38,40 Conversely, accurate conceptualisation of sustained relational betrayal as a potential traumatic stressor supports more precise diagnosis, targeted treatment, and improved clinical outcomes.
Clinical Applications
The findings of this review have direct implications for clinical assessment, diagnosis, and treatment across psychiatry, psychology, and primary care settings. Patients presenting with distress following serial infidelity are frequently encountered in practice, yet the underlying mechanisms of harm may be overlooked when infidelity is conceptualised solely as a relational or moral issue.7-10 A trauma-informed approach requires clinicians to attend to relational context, patterns of control, and psychological manipulation rather than focusing narrowly on behavioural disclosure.14,28,36
Clinicians should assess patterns rather than isolated events. Indicators that serial infidelity may constitute a form of psychological abuse include repeated deception, concealment of parallel relationships, denial of verifiable evidence, blame-shifting, intermittent reinforcement, and efforts to undermine the patient’s confidence in their perceptions or memory.21-23,28-30 Inquiry should extend beyond sexual behaviour to include emotional withdrawal, surveillance, threats of abandonment, and manipulation of reality. Assessment frameworks commonly used in intimate partner violence may be adapted to relational betrayal contexts, particularly those evaluating coercive control, epistemic invalidation, and dependency dynamics.14,28,30 Failure to conduct such an assessment risks misdiagnosis and inappropriate treatment planning.36-39
Diagnostic formulation should prioritise trauma-based conceptualisations when criteria are met. Presentations characterised by hypervigilance, affect dysregulation, dissociation, negative self-concept, and relational avoidance are consistent with trauma-related diagnoses, particularly ICD-11 Complex PTSD when exposure is prolonged and relational.17-19,24,31 Where appropriate, clinicians may specify formulations such as PTSD with prominent betrayal trauma features or Complex PTSD associated with relational coercion, maintaining diagnostic precision without unnecessary diagnostic proliferation.
Treatment planning should prioritise trauma-informed interventions rather than relationship repair strategies alone. While couples therapy may be appropriate in cases of non-coercive infidelity, its use in contexts involving deception, gaslighting, or control may risk further harm.28-30 Individual trauma-focused therapies, including trauma-focused cognitive behavioural therapy, sensorimotor psychotherapy, and phase-based approaches for Complex PTSD, are likely to be more appropriate when coercive dynamics are present.31,33,34,40 Pharmacological interventions may be indicated for comorbid mood or anxiety symptoms, but should not substitute for addressing the underlying trauma exposure. Psychoeducation also plays a critical role in validating patient experiences and reducing self-blame.24,36
Recognition of betrayal trauma has implications for risk assessment and patient safety. Individuals exposed to sustained relational deception may experience significant psychological distress, impaired decision-making, and erosion of self-trust.24-27 Validating the reality of relational harm is therefore a therapeutic intervention in itself, counteracting epistemic injury and supporting recovery. Clinicians should remain alert to the potential for re-traumatisation when patients are encouraged to minimise harm, reconcile prematurely, or assume shared responsibility for abusive dynamics. Consistent with established trauma-informed care principles, clinical work requires careful pacing, explicit boundaries, and prioritisation of psychological safety.41,42
Study Limitations and Future Directions
Several limitations of this review should be acknowledged. First, although guided by PRISMA principles, the review employed a narrative synthesis approach rather than a full systematic review or meta-analysis, limiting the ability to quantify effect sizes or establish causal relationships. This reflects the heterogeneity of the existing literature on serial infidelity and relational betrayal. Second, the included studies varied widely in design, population, outcome measures, and conceptual frameworks. While this diversity enabled integrative thematic analysis, it also introduced variability in the strength and specificity of conclusions. Notably, relatively few studies examined serial infidelity explicitly within trauma or coercive control frameworks, highlighting a gap in the empirical literature.
Publication bias must also be considered. Research on infidelity and relational harm is dispersed across multiple disciplines, and negative or null findings may be underrepresented. Much of the available literature relies on self-report data, which may be influenced by recall bias or contextual factors. In addition, although convergent evidence supports the conceptualisation of serial infidelity with coercive dynamics as a potential traumatic stressor, betrayal trauma is not deterministic. Individual outcomes are influenced by moderating factors such as attachment history, social support, prior trauma exposure, and access to validating clinical care.24-27 Serial infidelity alone is insufficient to infer trauma-related harm without careful contextual assessment.
Future research should prioritise longitudinal designs examining trajectories of psychological outcomes following relational betrayal, particularly in cases involving deception and coercive control. Development and validation of structured assessment tools to differentiate situational infidelity from abuse-associated betrayal would enhance clinical utility. Neurobiological and psychophysiological studies specific to relational betrayal may further clarify mechanisms underlying observed trauma responses.31-35
Conclusion
This narrative review examined serial infidelity in the context of coercive control, gaslighting, and psychological abuse, highlighting its potential to function as a clinically significant form of relational trauma. Across diverse literatures, convergent evidence indicates that sustained relational betrayal—particularly when embedded within deception, power imbalance, and epistemic invalidation—can produce psychological effects consistent with trauma responses observed in other forms of intimate partner abuse.7,10,14,24-30
The findings underscore the importance of distinguishing situational infidelity from coercive betrayal patterns and caution against diagnostic formulations that obscure relational harm. By situating serial infidelity within existing trauma frameworks, particularly ICD-11 Complex PTSD, this review advances a clinically coherent approach that prioritises contextual assessment, trauma-informed care, and appropriate intervention. Improved recognition of betrayal trauma has implications for diagnostic accuracy, patient validation, treatment planning, and ethical clinical practice, and may reduce misdiagnosis while supporting recovery for individuals whose experiences of relational trauma have historically gone unrecognised.
Footnotes
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Disclaimer
All views expressed are those of the authors and do not necessarily reflect the positions of James Cook University or any affiliated institutions.