
Abstract
Objective
Repetitive transcranial magnetic stimulation (rTMS) is an established treatment for comorbid post-traumatic stress disorder (PTSD) and major depressive disorder (MDD). However, there are no universal protocols regarding the type of rTMS recommended, including among military and first responders. This study aimed to describe high frequency rTMS applied to the left dorsolateral prefrontal cortex (DLPFC) administered to inpatients with comorbid PTSD and MDD at Ward 17, Austin Health in Melbourne, Australia.
Method
Retrospective review of patient files was undertaken for adult inpatients admitted between 01/01/2017 and 01/12/2024 with PTSD and MDD who received ten or more rTMS treatments during admission. Paired t-tests were used for statistical analysis.
Results
Among 65 patients and 118 admissions, the majority received high frequency rTMS to the left DLPFC (n = 106, 89.8%), followed by rTMS applied to the right DLPFC (n = 8, 6.8%). The group who received left-sided rTMS had an average of 6 fewer treatments and admission length that was 10 days shorter, but almost half required readmission for further rTMS treatments. The most common side effects reported were pain, fatigue, light-headedness or dizziness, and increased anxiety. Left-sided rTMS was associated with significant improvements in MADRS (Cohen’s D = 1.36, 95% CI = 1.06-1.65, P < .001), PCL-5 (D = 1.18, 95% CI = 0.72-1.63, P < .001), HoNOS (D = 1.20, 95% CI = 0.94-1.46, P < .001), and MoCA scores (D = −0.56, 95% CI = −0.81 to −0.31, P < .001).
Conclusions
High frequency left-sided rTMS is generally well tolerated and may reduce both depressive and PTSD symptoms. Further research to assess rTMS subtypes and target specific symptomatology would support standardization of care and inform future protocol guidelines.
Keywords
Introduction
Repetitive transcranial magnetic stimulation (rTMS) uses non-invasive brain stimulation that involves passing an electric current through a magnetic coil, which generates a time-limited high intensity magnetic field over the scalp. This results in the excitation or inhibition of underlying brain area, depending on the type of rTMS treatment. 1 rTMS may be used to treat psychiatric disorders such as major depressive disorder (MDD) and post-traumatic stress disorder (PTSD). 2 Approximately half of people with PTSD may also meet MDD criteria 3 and comorbid MDD and PTSD may be more difficult to treat compared to MDD alone 4 and present with more long-term functional impairment. 5 These comorbid conditions are particularly relevant among first responders and military personnel, and point prevalence is up to 14.6% for MDD and up to 14.2% for PTSD among police personnel. 6 Comorbidity rates are similarly increased among military personnel and is associated with reduced cognitive functioning and quality of life, alongside greater anxiety, suicidal ideation, self-harm, and mental health service utilization, compared to PTSD or MDD alone. 7
Treatments for comorbid PTSD and MDD may include psychotherapy and/or antidepressant medication, however greater treatment attrition and poorer prognosis have been observed in the setting of psychiatric multimorbidity. 3 Individuals who experience both PTSD and MDD symptoms often show reduced or delayed treatment responses. 5 rTMS has shown evidence for improving comorbid MDD and PTSD, 8 including presentations that have failed to respond to alternative treatment. For instance, rTMS has been assessed in refractory MDD and PTSD within the military population and demonstrated clinical benefits in terms of Beck Depression Inventory (BDI) and PTSD checklist (PCL) scores. 9
In relation to mechanism of action, effective rTMS treatment may result in neuroplasticity and connectivity changes between key brain areas. 8 The prefrontal asymmetry theory proposes there may be underactivity in the left DLPFC and overactivity in the right DLPFC among people who experience depression. 10 High frequency left-sided rTMS and low frequency right-sided rTMS may therefore reduce depressive symptoms and normalize brain activity through stimulation of the left DLPFC and inhibition of the right DLPFC. 10 High frequency rTMS over the left DLPFC and low-frequency rTMS over the right DLPFC shows evidence for MDD alone 11 as well as comorbid MDD and PTSD. 10 Similarly, low frequency rTMS may be effective for PTSD due to inhibition of right DLPFC hyperactivity. 12 In contrast, animal studies have shown an association between hypothalamic-pituitary-adrenal (HPA) axis hypoactivity in PTSD and right hypofrontality of the brain. 10 Activation of the right DLPFC through high frequency rTMS may excite the HPA axis and subsequently improve autonomic responses and suppress amygdala activation in PTSD.10,13
There are no universal recommendations or protocols regarding the type and frequency of rTMS treatment recommended for comorbid MDD and PTSD. 10 Furthermore, it is unclear whether first line treatment for comorbid MDD and PTSD should be low or high frequency, or target the left or right DLPFC. Right DLPFC targeted treatment may be more effective compared to left-sided DLPFC treatment for PTSD14-16 and PTSD with prominent depressive symptoms. 10 A double blinded placebo controlled trial demonstrated significant mood improvements following high frequency left-sided rTMS but a significant reduction in anxiety and core PTSD symptoms after high frequency right-sided rTMS. 15 Left-sided rTMS shows potential for reducing both PTSD and MDD comorbid symptoms 10 but there is currently limited evidence available.
There are currently no recommended rTMS protocols for comorbid MDD and PTSD, and further research is needed to inform guidelines. 10 Given the absence of standardized protocols and limited real-world inpatient data, this study aimed to describe the tolerability, clinical outcomes, and treatment characteristics of high-frequency left-sided rTMS in an inpatient population with comorbid PTSD and MDD.
Materials and Methods
Setting and Participants
This was a retrospective cohort study which included electronic patient files of psychiatric inpatients admitted to Ward 17 at Austin Health, a metropolitan tertiary public hospital in Melbourne, Victoria. Inclusion criteria included adult inpatients who were eligible for Psychological Trauma and Recovery Services (PTRS) and admitted between 01/01/2017 and 01/12/2024 with a diagnosis of PTSD and MDD determined by a consultant psychiatrist as per the Diagnostic and Statistical Manual of Mental Disorders, 5th Edition (DSM-5) criteria, 2 who received ten or more rTMS treatments during hospitalization. A minimum of ten sessions was selected to ensure sufficient treatment exposure to assess early clinical response. Exclusion criteria included outpatients, patients without primary diagnoses of MDD and PTSD, or patients who received less than ten rTMS sessions. Patients who experienced comorbid substance use issues such as high alcohol use were included if they were able to complete detoxification.
PTRS is a statewide service which offers specialized treatment for people with trauma-related mental health conditions that are compensable. This includes emergency services personnel, veterans and current military personnel, workplace injury or road traffic accident survivors, and victims of crime. rTMS was introduced to PTRS in 2017 and referrals are from private psychiatrists/psychologists, general practitioners, PTRS outpatient clinics, or patients. Safety protocol screening is undertaken pre-admission by a medical doctor to confirm there are no contraindications to rTMS such as active epilepsy, or electrical stimulation devices or metallic elements in the brain. rTMS is provided as unilateral or bilateral treatment using a flat figure 8 coil. An acute rTMS course is commenced with daily treatments that are gradually increased to twice daily based on tolerability. The number of treatments provided is based on clinical response as assessed by the lead consultant psychiatrist and funding provisions as a compensation-based tertiary service. Treatment response is evaluated by regular clinical reviews led by the consultant psychiatrist alongside weekly psychometric outcomes. These include the Montgomery and Asberg Depression Rating Scale (MADRS) 17 and Post Traumatic Stress Disorder Checklist for DSM-5 (PCL-5), 18 both of which demonstrate acceptable reliability and validity for monitoring depressive 19 and PTSD symptoms respectively. 20 Adverse effects are monitored through regular psychiatric and nursing reviews, and cognition is evaluated weekly using the Montreal Cognitive Assessment (MoCA), a screening tool with high specificity and sensitivity for detection of mild cognitive impairment. 21 The Health of the Nation Outcome Scales (HoNOS) are completed at admission and discharge and similarly demonstrate acceptable validity and reliability in assessing overall health and social functioning, as well as changes over time. 22
Design and Data Collection
Admission and progress notes, rTMS records, and discharge summaries for each eligible patient file were reviewed by a trained medical doctor. Outcomes of interest were demographic and clinical characteristics and types of rTMS treatment administered. This included left-sided rTMS, which was defined as rTMS treatment applied to the left DLPFC, and right-sided rTMS which described rTMS applied to the right DLPFC. Bilateral rTMS was defined as rTMS applied to both left and right DLPFC. rTMS was further subtyped into high frequency (10 Hz) or low frequency (1 Hz) treatment. Data was extracted and recorded in deidentified format on secure servers.
Statistical Analysis
IBM SPSS Statistics (Version 27) was used for descriptive and analytical statistics, and paired t-tests were used to assess if there were statistically significant differences in MADRS, PCL-5, MoCA, and HoNOS scores before and after left-sided rTMS treatment. 23 Descriptive statistics included all eligible admissions which occurred between 01/01/2017 and 01/12/2024, including readmissions. Statistical analysis only included index admissions, and admissions which had the complete outcome measure data available. Significance level was set at P < .05.
Ethics
This study was approved by the local hospital ethics committee, and a waiver of consent was obtained.
Results
Demographic and Clinical Characteristics
There were 70 patients who received rTMS through PTRS, Austin Health between 01/01/2017 and 01/12/2024. Of these, 1 patient was excluded as they did not have primary diagnoses of MDD and PTSD, 1 outpatient was removed, and 3 patients who received less than 10 treatments were excluded. Overall, 65 inpatients and 118 admissions were included. Of these, 40 (61.54%) patients had single rTMS admissions and 25 (38.46%) patients had 2 or more admissions for rTMS.
Characteristics of Admissions for Inpatients With Comorbid PTSD and MDD Who Received Left-Sided or Right-Sided rTMS Treatment
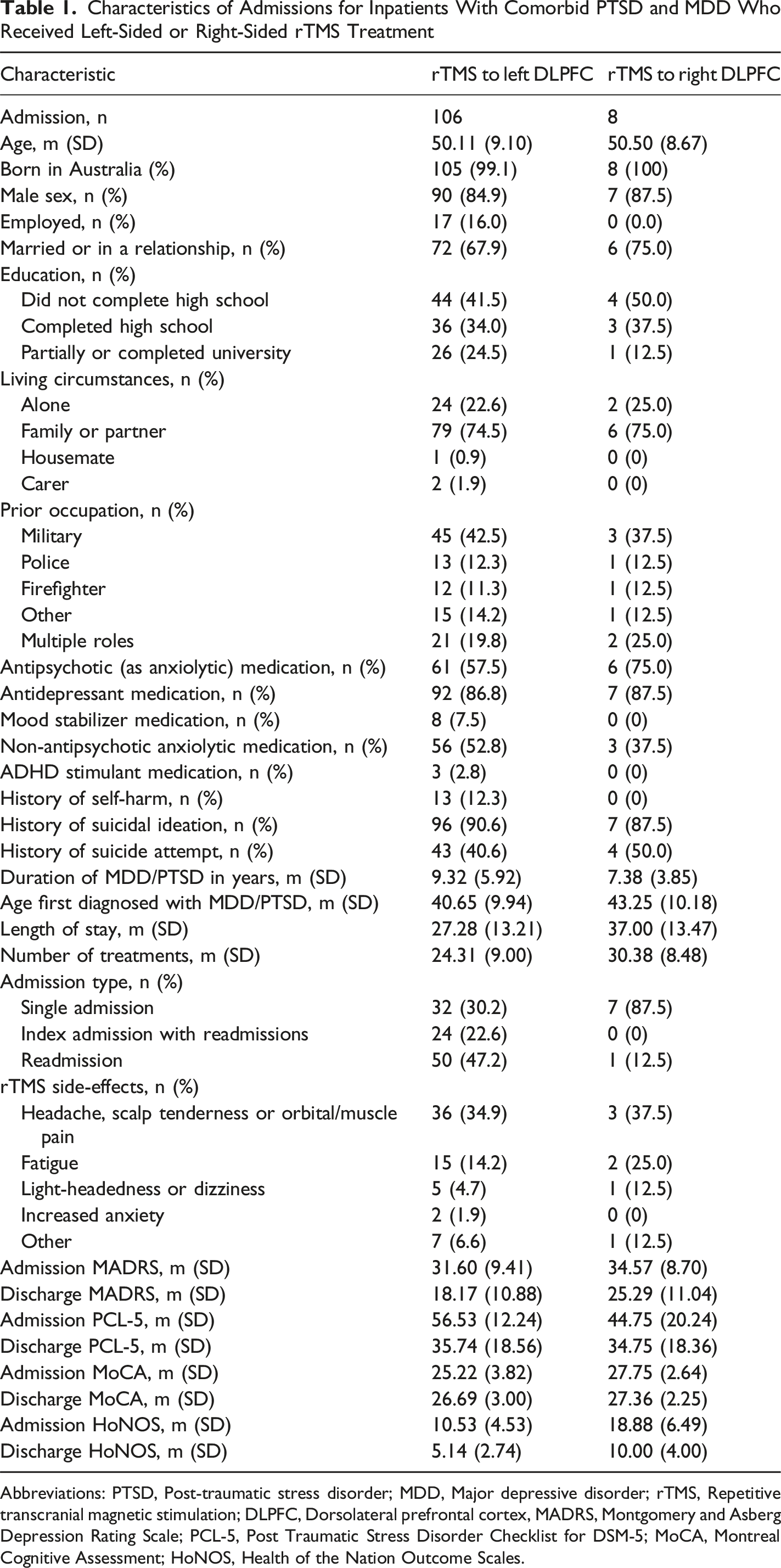
Abbreviations: PTSD, Post-traumatic stress disorder; MDD, Major depressive disorder; rTMS, Repetitive transcranial magnetic stimulation; DLPFC, Dorsolateral prefrontal cortex, MADRS, Montgomery and Asberg Depression Rating Scale; PCL-5, Post Traumatic Stress Disorder Checklist for DSM-5; MoCA, Montreal Cognitive Assessment; HoNOS, Health of the Nation Outcome Scales.
Sample Characteristics of Admissions for Inpatients With Comorbid PTSD and MDD Who Received rTMS Treatment
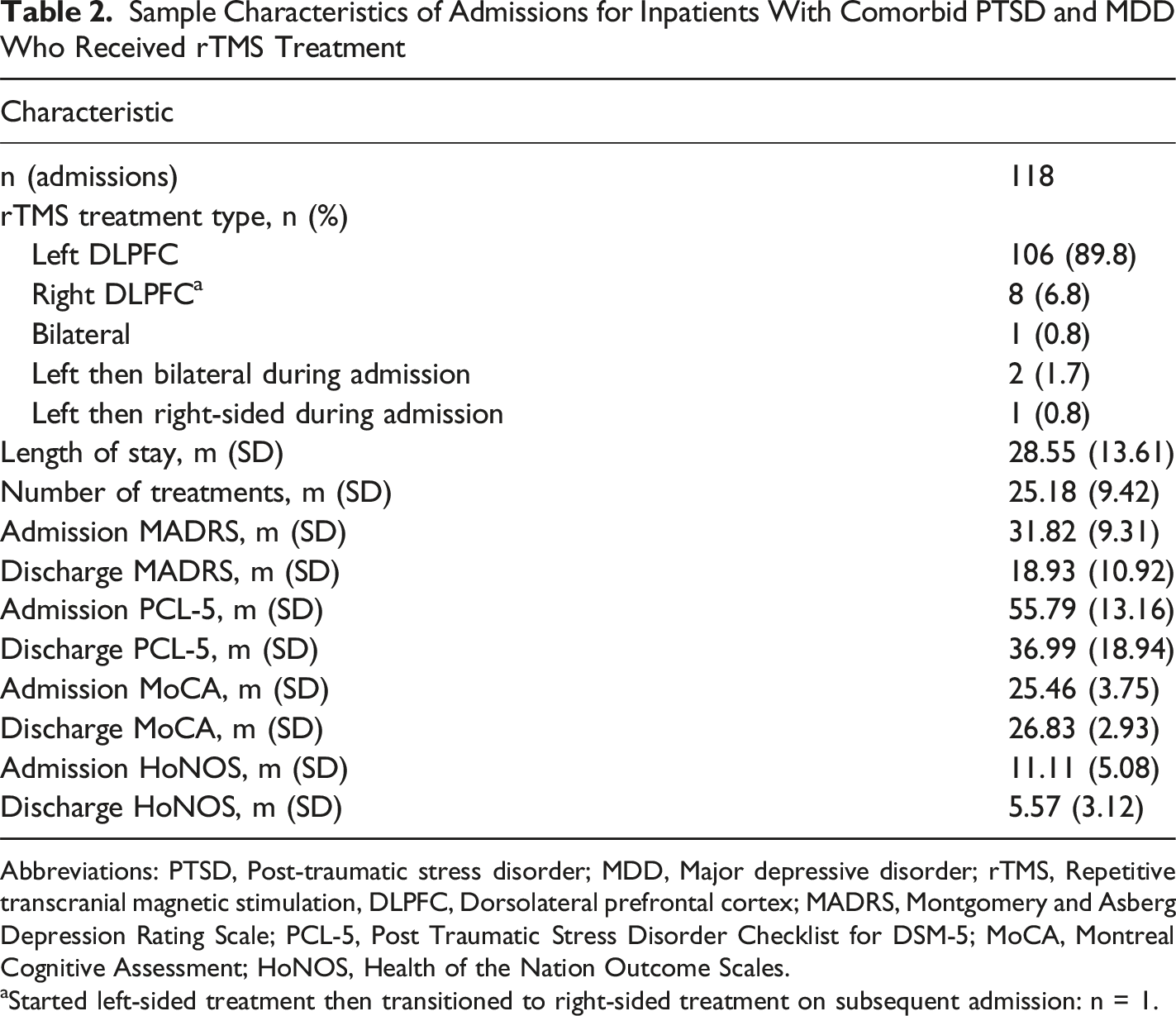
Abbreviations: PTSD, Post-traumatic stress disorder; MDD, Major depressive disorder; rTMS, Repetitive transcranial magnetic stimulation, DLPFC, Dorsolateral prefrontal cortex; MADRS, Montgomery and Asberg Depression Rating Scale; PCL-5, Post Traumatic Stress Disorder Checklist for DSM-5; MoCA, Montreal Cognitive Assessment; HoNOS, Health of the Nation Outcome Scales.
aStarted left-sided treatment then transitioned to right-sided treatment on subsequent admission: n = 1.
The average number of rTMS treatments received was 25.18 (SD = 9.42) (Table 2). In terms of descriptive statistics, the group who received left-sided rTMS had a length of stay that was 10 days shorter compared to right-sided rTMS, and required approximately 6 fewer treatments. Almost half of patients who received left-sided rTMS required hospital readmission for further rTMS treatment, whereas most individuals who received right-sided rTMS were not readmitted at W17. The most common side effects included pain, fatigue, and light-headedness or dizziness (Table 1). Other side effects were reported from 7 patients who received left-sided rTMS (irritability, mild nausea, blurred vision, or increased frequency of nightmares with sleep improvement), and 1 patient who received right-sided rTMS (self-reported short-term memory issues). For both left and right-sided rTMS treatment, improvements in MADRS, PCL-5, and HoNOS scores were observed (Table 1).
Outcome Measures Before and After rTMS Treatment to the Left DLPFC for Comorbid PTSD and MDD
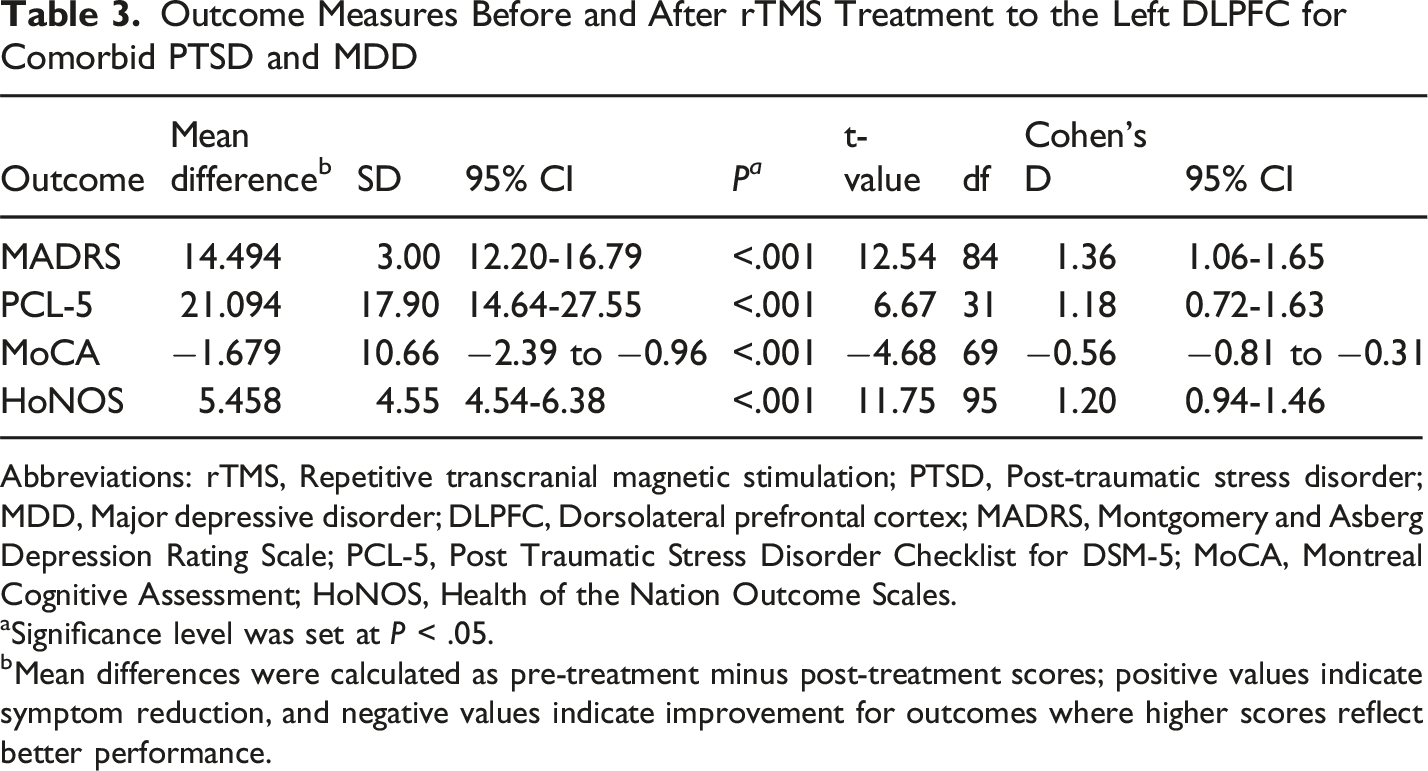
Abbreviations: rTMS, Repetitive transcranial magnetic stimulation; PTSD, Post-traumatic stress disorder; MDD, Major depressive disorder; DLPFC, Dorsolateral prefrontal cortex; MADRS, Montgomery and Asberg Depression Rating Scale; PCL-5, Post Traumatic Stress Disorder Checklist for DSM-5; MoCA, Montreal Cognitive Assessment; HoNOS, Health of the Nation Outcome Scales.
aSignificance level was set at P < .05.
bMean differences were calculated as pre-treatment minus post-treatment scores; positive values indicate symptom reduction, and negative values indicate improvement for outcomes where higher scores reflect better performance.
For left-sided rTMS, the majority of treatment was administered at high frequency as 10 Hz (n = 104, 98.1%), and per a treatment, 40 pulses in a train (n = 100, 94.3%), 75 trains (n = 100, 94.3%), and 3000 pulses in total (n = 101, 95.3%). At discharge, the RMT percentage was most frequently 120% (n = 93, 87.7%). For right-sided rTMS, all treatment was administered as low frequency at 1 Hz and per a treatment, most patients had 8 (n = 3) or 1 (n = 2) pulses in a train, the number of trains were 225 for half (n = 4), and the total number of pulses was 1800 for all patients. At discharge, all received treatment at RMT percentage of 110%.
Discussion
In this cohort of 65 inpatients who received rTMS for comorbid PTSD and MDD at Ward 17, Austin Health in Melbourne, Victoria, Australia, there were 118 admissions between 01/01/2017 and 01/12/2024. The majority of admissions were for high frequency rTMS treatment applied to the left DLPFC, which was generally well tolerated. Only a small proportion of patients reported increased activation and anxiety, necessitating a change to low frequency right-sided treatment. These findings demonstrate that left-sided rTMS primarily administered as high frequency treatment was overall well tolerated and may be associated with some clinical benefit for comorbid PTSD and MDD.
Left-sided rTMS was significantly associated with overall improvements in psychometric outcomes. MADRS scores improved from approximately 31 points, indicative of moderate depressive symptoms, to approximately 18 points, which suggests mild symptoms. 24 PCL-5 scores improved from approximately 56 points to 35 points, although this remained within the cutoff range that is suggestive of active PTSD symptoms. HoNOS scores similarly halved from admission to discharge, which suggested clinically significant change in terms of general mental health and wellbeing. 25 MoCA scores before and after left-sided rTMS improved by approximately 1 point, and this improvement met the minimum score for the normal range for cognitive functioning. 21
These results are consistent with previous findings that rTMS may improve PTSD, 13 anxiety, and MDD symptoms. 10 Both high and low frequency rTMS may reduce PTSD symptoms 13 but high frequency treatments may be more effective for trauma-related disorders 16 and comorbid PTSD and MDD. 12 In relation to the MoCA score improvements observed in this study, current literature has demonstrated mixed findings in terms of whether rTMS may improve cognition in MDD.26,27 Currently there is limited research available which assesses the impact of rTMS on cognition in comorbid MDD and PTSD. Further investigation is needed to explore whether rTMS has the potential to improve cognitive functioning independently of mental health treatment.
Not all participants improved with left-sided rTMS in our study and the average MADRS and PCL-5 scores at discharge were indicative of ongoing MDD and PTSD symptoms, suggesting symptom reduction rather than remission. This may represent the difficulties in treating comorbid and long-term MDD and PTSD, as well as the nature of patients who require rTMS treatment. The sample was primarily comprised of inpatients who had trialed multiple interventions including medications and psychotherapy prior to admission, with limited benefits. As rTMS has been implicated in neuroplasticity, it has been suggested that rTMS could augment other interventions to potentially improve clinical outcomes. 12 Some studies have shown that rTMS combined with psychotherapy may be more effective for PTSD treatment than psychotherapy alone. 12 Additionally, PTSD may present with different symptomatology between patients. These PTSD subtypes may differ in their functional connectivity patterns and benefit from different forms of psychotherapy. Similarly, some patients may improve with 1 type of rTMS but deteriorate with another. 12 It has been proposed that low frequency rTMS may reduce re-experiencing 12 and depressive 13 symptoms in PTSD whereas high frequency rTMS may reduce core PTSD symptoms 13 alongside avoidance and hyperarousal symptoms. 12 As these symptoms may be more or less prevalent among different individuals, targeting the type of rTMS to the prevailing presentation is an important consideration in clinical practice. 13
In terms of descriptive findings, it was noted that admissions for left-sided rTMS were on average shorter and required fewer treatments compared to right-sided rTMS. However, almost half of patients who were treated with left-sided rTMS required readmissions for further rTMS treatment. This is consistent with previous findings that approximately half of individuals successfully treated with rTMS for depression may relapse by 1 year. 28 The highest risk of relapse is often several months following an acute course. 29 Despite these findings, there are currently no recommendations in relation to when maintenance rTMS should be introduced as part of treatment and relapse prevention. Psychometric monitoring and clinical follow up during and after acute treatment could inform models of care to guide rTMS protocols in the future. Our findings further emphasize the need for standardization of rTMS treatment protocols recommended for individuals who experience comorbid PTSD and MDD.
Strengths and Limitations
Strengths of this study included the clinical relevance of the findings, which contribute to the limited evidence available regarding left-sided rTMS treatment for comorbid PTSD and MDD. The patient sample was primarily comprised of first responders and military personnel, a clinically important population in terms of mental health needs. Limitations included the retrospective nature of the study, which relied on available documentation. In relation to psychometric scores, statistical analysis only included admissions with complete data available, which may have impacted statistical power and limits the generalizability of these findings. Generalizability may also be limited due to the demographic characteristics of the cohort, which primarily included inpatients who were male and middle-aged. Additionally, this retrospective study did not control for potential confounders such as medication changes or other inpatient therapeutic interventions. However, during rTMS admissions at Ward 17, treatment is predominantly focused on rTMS, and additional interventions are infrequent. The absence of a control or comparison rTMS protocol nonetheless limits causal inference. Further limitations included the sample size, as only index admissions were included in statistical analysis to prevent resampling bias. Descriptive results may have also been further impacted by the proportion of readmissions. Future studies would benefit from sample size estimation, prospective patient recruitment, and analytical comparison to other forms of rTMS such as right-sided or bilateral treatment. Further stratification by stimulation frequency, including low- and high-frequency protocols, may also provide further insight in relation to treatment effects.
Conclusions
High frequency rTMS administered to the left DLPFC may be an effective and primarily well-tolerated treatment for comorbid PTSD and MDD, including among military personnel and first responders. High frequency left-sided rTMS may reduce both depressive and PTSD symptoms and is therefore an important intervention to consider for psychiatric multimorbidity and complex patient populations. Further prospective, controlled research is required to support the development of evidence-based guidelines and treatment recommendations, including optimization of rTMS to target specific symptom profiles. Improved standardization of rTMS protocols may enhance consistency in clinical practice and overall quality of patient care.
Footnotes
Ethical Considerations
This study was approved by the local ethics committee and a waiver of consent was obtained.
Author Contributions
Natalie Seiler was involved in conceptualization, data curation, methodology, and manuscript writing and revision. Thomas Nguyen led the formal analysis and investigation, and was involved in data curation and manuscript review. Amy Coelen was involved in data curation and manuscript review. Benjamin Newham and Timothy Rolfe led the conceptualization, manuscript review, and supervision.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author, Natalie Seiler, upon reasonable request.