
Abstract
Objective
This study described the prevalence of and correlates of depression and anxiety in adult patients with hemophilia A and B.
Methods
In this cross-sectional study, we investigated patients with hemophilia who were being seen at an adult hemophilia center in Turkey. Participants were screened for depression and anxiety during their annual clinic visit, which included administration of the Beck Depression Inventory and State-Trait Anxiety Scale.
Results
Of the 90 patients, 22 (24.4%) met criteria for significant depressive symptoms and 67 (74.4%) met criteria for significant anxiety symptoms. There were no significant associations between depression and any psychosocial or clinical characteristics or adherence to hemophilia prophylaxis, except for educational status. No association was found between state and trait anxiety scores and psychosocial and clinical characteristics other than hemophilia type. After adjusting for confounding factors, multivariable analysis showed that high school education level was associated with depression (OR: 1.87, CI: 1.31–2.36, P = .010) and type B hemophilia was associated with anxiety (OR: 1.32, CI: 1.09–1.75, P = .042).
Conclusion
Depression and anxiety are major psychiatric comorbidities in patients with hemophilia in Turkey. Routine evaluation for mood and anxiety disorders are important in the routine care of patients with haemophilia.
Keywords
Introduction
Hemophilia is an inherited, life-threatening disorder caused by a deficiency of clotting factors VIII (hemophilia A) and IX (hemophilia B). It is characterized by spontaneous and post-traumatic bleeding events in the joints, muscles, and other soft tissues. 1 In the past, patients were likely to die in the first couple of decades. However, with advances in diagnosis and the development of safe and effective treatment modalities, individuals have an almost average life expectancy. 2
Despite evolving from a deadly disease to a chronic disorder, hemophilia still causes significant morbidity, with numerous daily and long-term challenges for patients and their families. Patients with hemophilia must deal with the consequences of bleeding episodes, frequent hospital admissions, chronic arthropathy, functional disability, dependence on blood transfusions, and an increased risk of virus transmission through blood products, which may result in depression, anxiety, and social isolation.3–5 The prevalence of depression and anxiety has been found to increase in patients with hemophilia.6–9 As the prevalence of mood disorders varies among different countries, 10 we aimed to describe the rate and possible risk factors for depression and anxiety in adult population with hemophilia that was followed up at a single center in our country.
Method
Patients and data
Adult patients aged ≥18 years with a diagnosis of hemophilia who were followed up at a single adult hemophilia center were enrolled in this study. All consecutive patients who completed the participant report forms were included in the study. Patients with acquired hemophilia; a history of psychosis, bipolar disorder, severe cognitive impairment, or antidepressant drug utilization before being diagnosed with hemophilia; and incomplete files were excluded. Several sociodemographic and laboratory features were evaluated: sex; serologic results for hepatitis B virus (HBV), hepatitis C virus (HCV), and human immunodeficiency virus (HIV); level of education; marital status; family history of hemophilia; employment status; type and severity of hemophilia; and estimated number of bleeding episodes in the past 12 months. Data extracted from the questionnaires were matched with those collected during clinic visits, which were written into patients’ files by doctors or nurses. Serology test results of the patients were obtained from medical record systems and patient files.
Definitions
The most widely used method to classify the severity of hemophilia is based on plasma procoagulant factor levels (factor VIII or IX), with individuals with <1% normal factor defined as severe, 1–5% normal factor as moderate, and 5–40% normal factor as mild. 11 Compliance with hemophilia prophylaxis was calculated as follows: adherence (%) = total prescribed International Unit (IU)/total estimated IU × 100. The estimated IU was defined as the IU required to comply with treatment between the first and last prescriptions. Objective adherence was divided into two groups: adherence ≥75% (good = adherent patients) and adherence <75% (bad = non-adherent patients). 12
Assessment of depression and anxiety
All patients completed the Beck Depression Inventory (BDI) and State-Trait Anxiety Inventory (STAI). The BDI was published by Beck et al, and Tegin validated the Turkish version of the BDI-II in 1980.13,14
The BDI, a 21-question multiple-choice self-report inventory, is one of the most widely used and validated psychometric tests for screening, diagnosing, and measuring the severity of depression; a cutoff score for depression has been suggested to be ≥ 17.15–18 Patients accepted as having depression (≥17 in BDI) were provided free counseling and referred to a psychiatry clinic.
The STAI is a self-reported anxiety instrument considered the most reliable standard for anxiety evaluation. The State Anxiety Scale (STAI-S) evaluates the current state of anxiety, asking how respondents feel “right now,” using items that measure subjective feelings of apprehension, tension, nervousness, worry, and activation/arousal of the autonomic nervous system. STAI adaptation and validation studies have been performed in the Turkish population.19,20 The Trait Anxiety Scale (STAI-T) evaluates relatively stable aspects of “anxiety proneness,” including general states of calmness, confidence, and security. The STAI comprises 40 items, with 20 items allocated to each subscale. The range of scores for each subtest is 20–80, with higher scores indicating greater anxiety. For the STAI-S and STAI-T, the cutoff points for detecting clinically significant symptoms on the anxiety scales were 40 and 44, respectively.21,22
Ethical approval was obtained from the local instutional ethical committee (Ege University, Faculty of Medicine, Clinical Research Ethics Committee, Approval date and number: 21/04/2016 – 15-9.1/7).
Statistical analysis
Statistical analyses were performed using the IBM SPSS for Windows® version 20.0 software (IBM Corp., Armonk, NY, USA). Descriptive statistics are presented as mean ± standard deviation for continuous variables and as number and frequency for categorical variables. Data distribution was assessed using a one-sample Kolmogorov-Smirnov test. The chi-square test was used to compare categorical variables, and the independent sample t test or Mann–Whitney U test was used for continuous variables. Correlations were assessed using Pearson’s chi-square test.
Results
During routine clinic visits for 12 months, 116 patients received the sociodemographic questionnaire, BDI, and STAI I-II. All consecutive patients were male. A hundred and sixteen patients completed the forms and were enrolled in this study. Twenty-six patients were excluded because of incomplete responses to the questionnaire (Figure 1). Data analysis was done for the 90 participants with completed forms. Flow-chart of patient selection.
Medical and demographic data of the patient population by depression and anxiety.
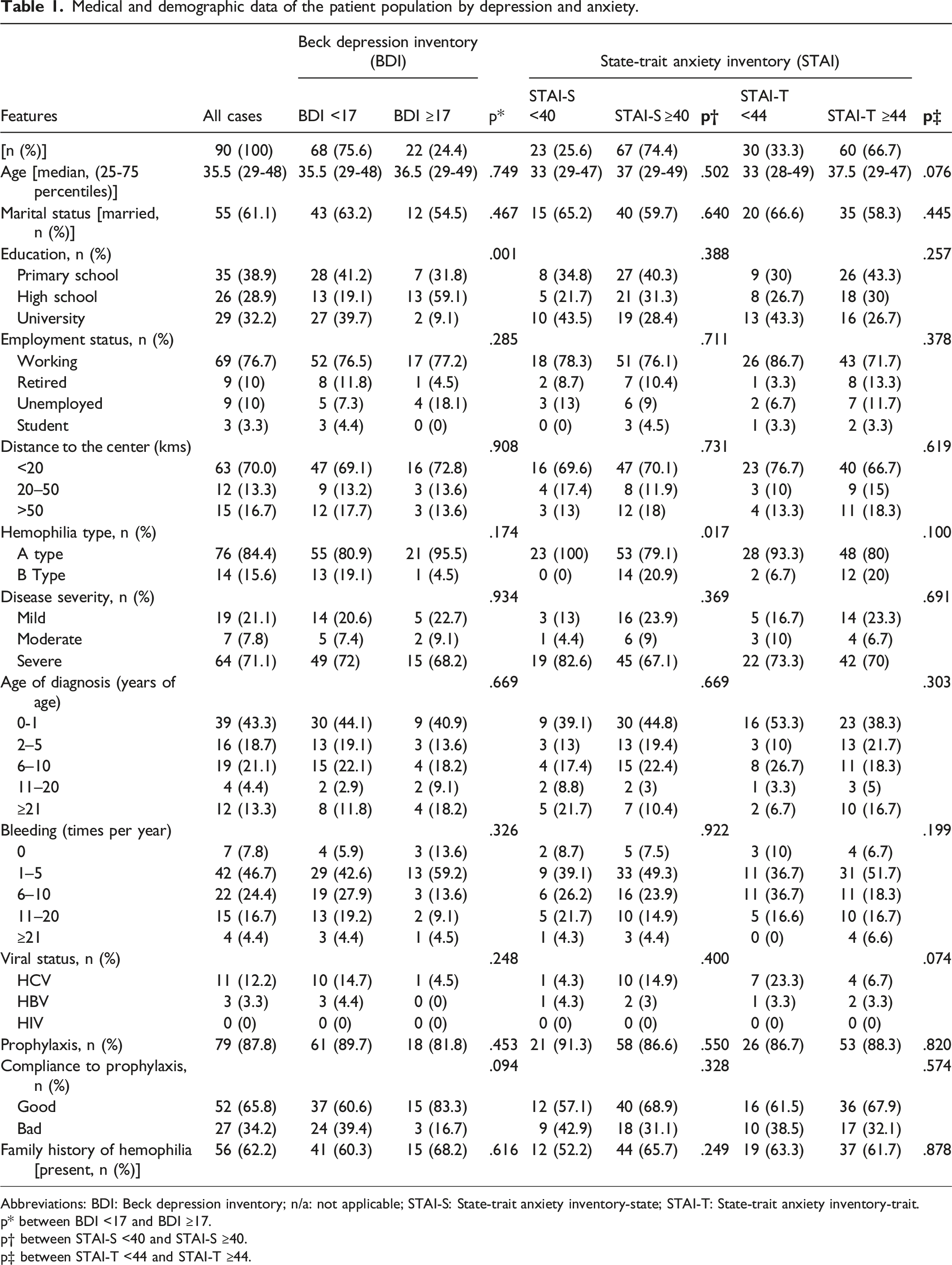
Abbreviations: BDI: Beck depression inventory; n/a: not applicable; STAI-S: State-trait anxiety inventory-state; STAI-T: State-trait anxiety inventory-trait.
p* between BDI <17 and BDI ≥17.
p† between STAI-S <40 and STAI-S ≥40.
p‡ between STAI-T <44 and STAI-T ≥44.
The median age of the patients was 35.5 years. Most patients had severe hemophilia A. Family history of hemophilia was present in 62.2%. Patients experienced frequent bleeding episodes, mostly 1–5 times per year. The prophylaxis rate was 87.8% (79/90), and good compliance to prophylaxis rate was 65.8%. Among the 90 patients, anti-HCV and anti-HBV seropositivities were found in 11 (12.2%) and 3 (3.3%) patients; there was no HIV seropositivity (Table 1).
Depression and anxiety Scores of patients According to their Depression and anxiety Status.
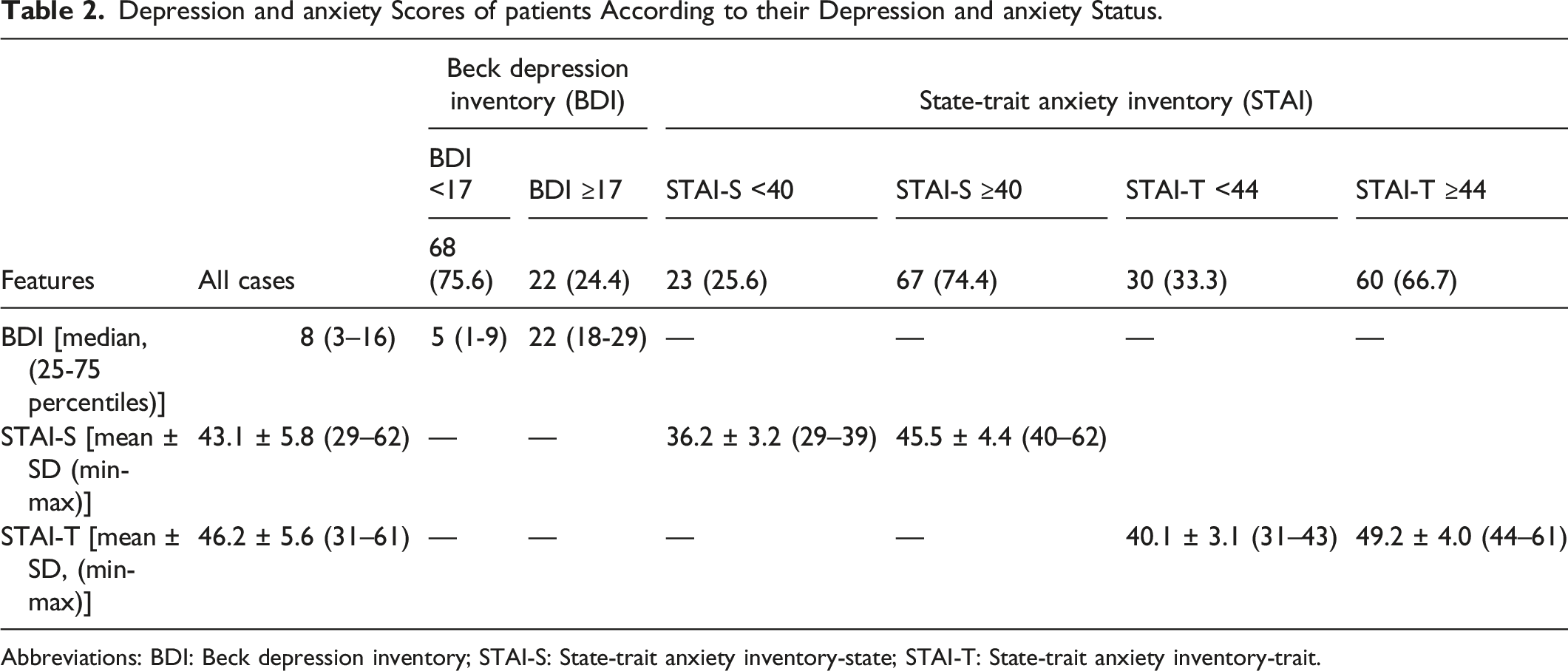
Abbreviations: BDI: Beck depression inventory; STAI-S: State-trait anxiety inventory-state; STAI-T: State-trait anxiety inventory-trait.
The mean STAI-S score was 43.1, lower than the mean STAI-T score. High STAI-S and STAI-T scores were found in 74.4% and 66.7% of the patients, respectively (Table 2). Patients with hemophilia B had higher STAI-S scores than those with hemophilia A (P = .017). No other factors were associated with increased anxiety scores (Table 1).
Multivariable analysis showed that high school education level was associated with depression (OR: 1.872, CI: 1.312–2.356, P = .010) and type B hemophilia was associated with anxiety (OR: 1.319, CI: 1.089–1.745, P = .042).
The median number of bleeding episodes was 5.5 per year (25th and 75th percentiles of 3.0 and 9.25, respectively). There was no correlation between the number of bleeding episodes and the BDI, STAI-S, and STAI-T scores (Table 1).
Discussion
Our study showed that, first, a significant proportion of patients with hemophilia met the criteria for depression (24.4%) and anxiety (74.4%). Second, patients with a higher educational status had a higher rate of depression. Third, patients with hemophilia B were more anxious than those with hemophilia A.
It is well known that chronic illnesses are associated with a higher risk of depression;3,4,23 hemophilia, a chronic and lifelong disease with significant morbidity, is no exception. Previous publications have reported the rate of depression in patients with hemophilia to be up to 50%.5,7,9,24–30 The methodology of the studies varied significantly, and several different questionnaires, self-report papers, and face-to-face interviews were used. There are also marked demographic, sociopolitical, and cultural differences between countries (eg, the variability between countries in population ageing, health care access, work–life balance, job insecurity, and the increase of living costs). 10
A study in China demonstrated that the rates of anxiety and depression in patients with hemophilia were 60% and 43.7% in China and other countries (Algeria, Argentina, Canada, China, France, Germany, Italy, Spain, the United Kingdom, and the United States of America), respectively. 31 In another study, Iannone et al 7 showed that the prevalence of depression in hemophilia patients was 37%. Data from our center revealed that the rate of depression in adult patients with hemophilia was 24.4%. Although lower than that in some countries, the rate of depression was still comparable with the data in the literature.
Educational status was the only variable related to depression in patients with hemophilia. Almost half of the patients who had graduated from high school were affected, whereas the rate of depression was lower among less-educated and university graduates. Education and related socioeconomic status seem to act as complex factors in developing depression among patients with hemophilia. We postulated that thriving on the choice of career and uncertainties about coping with such future stress among patients with hemophilia may contribute to the higher rates of depression among high school graduate.
Anxiety is common in patients with hemophilia.32,33 In a recent comprehensive meta-analysis evaluating 2926 patients with hemophilia, it was shown that the prevalence of anxiety can reach up to 46%. 34 In our study, the state and trait anxiety rates were 74.4% and 66.7%, respectively. However, no relationship was found between the rate of anxiety and features studied in patients with hemophilia. The only exception was the hemophilia type; state anxiety was higher in patients with hemophilia B. Although not statistically significant, a similar trend was observed for trait anxiety. Other factors may not have been considered in this study. In contrast to our findings, Kihlberg et al 35 did not observe any difference in quality of life in patients with hemophilia type A and B in their study of 126 patients. Although it does not seem possible to attribute the fact that hemophilia type B patients are more anxious than type A patients to a reason with our cross-sectional study, this interesting issue needs to be investigated with more comprehensive cohort studies. According to our clinical experience from face-to-face interviews, most patients followed up at our center had anhedonia and anxiety. They were anxious about many situations, such as social activities, emotional relationships, being disabled, and losing financial and social support. Their future expectations were nebulous because of fear of bleeding, disability, and death anxiety. There are few important studies in the literature that agree with these observations. Witkop et al 36 showed that hemophilia has a negative impact on physical activity and social relationships (eg friends, peers, colleagues and employers). In another study, it was observed that people with hemophilia were worried about relationships, sexuality, sports activities and the future. 37
Infections with HIV, HBV, and HCV significantly impact the mortality of patients with hemophilia. 38 Various factors influencing the quality of life have been reported in patients with hemophilia. HCV infection has been shown to reduce the quality of life in patients with hemophilia. 39 Patients with hemophilia may experience disease-related distress due to HIV, HCV, and HBV infections related to chronic health conditions. 40 In addition, interferon treatment may cause serious side effects, including depression, and should be withheld if there is severe pre-existing depression. 38 This situation is even worse for HIV. 41 Despite its probable effects on depression, we did not find any significant association between the viral serological status and depression or anxiety in our study group, which may be related to the relatively small number of serologically positive cases in the population.
Bleeding is one of the most critical factors affecting the course of hemophilia. Almost half of the patients experienced 1–5 bleeding episodes yearly in the studied population. Although it is a suspected risk factor for altered mood, there was no relationship with depression and/or anxiety. The number of bleeding episodes was not correlated with the scores of the studied inventories. Patients become accustomed to bleeding, so they may not experience adverse emotional effects.
People with chronic and/or life-threatening disorders tend to be more anxious and experience intense, excessive, persistent worry and fear in everyday situations. However, patients struggle with this lifelong disease since childhood, try to harmonize with the social environment, and may not identify as patients. Patients may have a positive image of their status since childhood, despite the fear of bleeding. Therefore, the rate of depression in our study population may have been low. In addition, the fact that our patient population was young may explain this observation.
Study limitations
Our study had several limitations. First, we did not include a control group to compare patients with hemophilia with healthy individuals. Second, we randomly applied the BDI, STAI-S, and STAI-T to every patient who visited the clinic over 12 months. Third, the small number of patients enrolled in the study may have limited the ability to detect associations between the variables and depression and anxiety. Fourth, some variables that were significant predictors of depression and anxiety, such as income, persistent pain, and joint impairment, were not considered. The main limitation of our study is that although our sample size was sufficient considering the prevalence of hemophilia, caution should be exercised regarding the results’ generalizability since it is a cross-sectional, single-center analysis. Despite these limitations, we believe this study is of particular importance as it provides national data on the rates of depression and anxiety among patients with hemophilia.
Conclusions
This study found that depression and anxiety are important comorbidities in patients with hemophilia. Mental health screening of this patient population for depression and anxiety should be considered by clinicians in Turkey, and possibly outside Turkey as well. In addition to competently and thoroughly treating their medical condition, the diagnosis and treatment of mental health problems in patients with hemophilia could make a major contribution to their quality of life. Larger studies, particularly prospective studies, are needed to assess the true impact of this blood disorder on mental health.
Footnotes
Acknowledgements
This study was not funded by any foundation. The patients did not gain any profit. All work was conducted at Ege Adult Hemophilia Center in Ege University/Izmir.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval was obtained from the local instutional ethical committee (Ege University, Faculty of Medicine, Clinical Research Ethics Committee, Approval date and number: 21/04/2016 – 15-9.1/7).
Informed consent
All patients signed written informed consent and gave permission for being included in this study and publication of it.
Research involving human and animal participants
All procedures were according to the ethical standards of the responsible committee on human experimentation and with the Helsinki Declaration of 1964 and its modifications.