
Abstract
Objective
This study examined the prevalence and correlates of depression, anxiety, insomnia, and dysmenorrhea in stressed fingolimod-treated women with multiple sclerosis.
Methods
This cross-sectional study recruited female patients diagnosed with multiple sclerosis and high stress scores from Al-Bashir Hospital in Jordan. Depression was assessed by the Patient Health Questionnaire (PHQ-9); anxiety by the Generalized Anxiety Disorder (GAD-7) scale; insomnia by the Insomnia Severity Index (ISI-A) scale; and dysmenorrhea severity by a measure assessing working ability, location, intensity, days of pain, and miscellaneous dysmenorrhea symptoms (WaLIDD).
Results
A total of 129 patients were recruited for the study. Severe depression was reported in 55.8%, severe anxiety in 62.0%, severe insomnia in 36.4%, and severe dysmenorrhea in 23.3%. Multivariate analyses revealed that depressive symptoms were associated with dysmenorrhea (OR = 3.55, 95% CI = 1.56–8.12, p = 0.003); anxiety symptoms with “not using dysmenorrhea analgesics” (OR = 2.74, 95% CI = 1.16–6.46, p = 0.02) and dysmenorrhea symptoms (OR = 4.74, 95% CI = 1.94–11.59, p = 0.001); insomnia symptoms with age above 30 years (OR = 4.34, 95% CI = 1.64–11.51, p = 0.003); and dysmenorrhea symptoms with the presence of chronic diseases (OR = 4.21, 95% CI = 1.28–13.92, p = 0.02), anxiety symptoms (OR = 3.03, 95% CI = 1.18–7.73, p = 0.02), and insomnia symptoms (OR = 3.00, 95% CI = 1.18–7.64, p = 0.02).
Conclusion
Stressed women with multiple sclerosis in Jordan experience high rates of depression, anxiety, insomnia, and dysmenorrhea. Characteristics related to these conditions may help clinicians to identify those at risk. Longitudinal studies are needed to determine the causal nature of these associations.
Introduction
Multiple sclerosis (MS) is a chronic immune-mediated disease characterized by inflammation, demyelination, and axonal degeneration of the central nervous system (CNS), with relapsing-remitting MS (RRMS) as the most common form. 1 The incidence of MS has increased dramatically between the ages of 20 and 40 years and is three times more common in women than men, especially those of reproductive age. 2 Disease-modifying therapies (DMTs) such as fingolimod, interferons, and monoclonal antibodies are the mainstay for RRMS. Fingolimod is a sphingosine-1-phosphate (S1P) receptor agonist and a natural bioactive sphingolipid that plays an important role in the inflammation and repair of the cell membrane structure.3–5 Clinically, fingolimod is of particular importance, as it is an oral, effective, and convenient agent used in the treatment of RRMS. 3
The chronic nature of the disease, the uncertainty of the cure, and the stressful treatment journey put women with MS at high risk for mental health disturbance. It is estimated that 70% of MS patients reported high-stress levels during the disease course compared to healthy subjects.6–8 Chronic and uncontrolled psychological stress could lead to depression, anxiety, insomnia, and pain symptoms.9–12
The prevalence of depression symptoms was previously studied in patients with MS of both sexes. It has been established that the prevalence of depression is higher compared to that of the normal population. 13 Several cross-sectional cohort studies recruiting different numbers of patients have estimated that 30–50% of patients diagnosed with RRMS reported depression symptoms, of which 50% are untreated.14–16 Fewer studies focused on depression symptoms among women, with one interesting study reporting that 25% of women with RRMS reported depressive symptoms. 17
The prevalence of anxiety, defined as a state of fear or tension from existing or future events, has also been studied in MS; according to some reports,18,19 anxiety could reach 30% among RRMS patients and is estimated to be 29% in women with RRMS. 17
Insomnia is considered an important sleep disturbance associated with fatigue among MS patients. The prevalence of sleep disorders in individuals with MS is 3–5 times higher compared to the general population. 20 According to the literature, insomnia symptoms have been reported in 12.5%–78% of patients with RRMS.21,22
The most commonly reported symptoms are difficulty falling asleep, maintaining sleep, or waking up too early, all of which can lead to significant fatigue, the most common and disabling symptom of MS. Furthermore, fatigue and insomnia could exacerbate other psychological and physical symptoms. 23
Dysmenorrhoea is one of the most common menstrual cycle-related disorders among females, characterized by painful menstrual cramps with a prevalence ranging from 30% to 94%.24,25 The severity of dysmenorrhoea is tightly related to family history, menarche before 12 years, body weight, smoking, and stress,26–28 although cross-talk between MS and the menstrual cycle has also been established.29,30 For instance, MS exacerbations are usually evident during the premenstrual period due to low levels of estrogen and progesterone.31,32 However, the prevalence of dysmenorrhoea severity is rarely studied in women with RRMS.
In developing countries, the mental health status of women diagnosed with disabling diseases is emerging. In addition, only a small amount of literature has highlighted the importance of the mental health status of women diagnosed with RRMS. The estimation of the rates of depression, anxiety, insomnia, and dysmenorrhoea symptoms among women with MS and the identification of potential risk factors for these symptoms helps clinicians to improve the patient’s mental health status and wellbeing.
Therefore, the objective of the present study is to explore the rates of depression, anxiety, insomnia, and dysmenorrhoea symptoms in stressed fingolimod-treated women with multiple sclerosis and to investigate whether the patient demographics and health factors are associated with these symptoms.
Materials and methods
Study design and settings
This is part of a larger cross-sectional study. The study was approved by Yarmouk University IRB committee (16/2022). MS patients attending the MS clinic at Al-Bashir Hospital were approached and then assessed for their eligibility to participate in the study according to pre-determined inclusion criteria.
Inclusion criteria
Female RRMS patients were diagnosed according to the 2017 McDonald criteria, 1 receiving fingolimod for at least one year, free of relapses and experiencing “near normal walking ability” according to the Arabic version of the patient-determined disease steps (PDDS-A) in people with multiple sclerosis. 33 In addition, all participants exceeding the threshold for stress according to the Perceived Stress Scale (PSS) Arabic version were included. The Arabic version of the PSS was used to screen the participants (MS patients and controls) for stress before enrolment. The PSS was developed by Cohen and Williamson 34 and included 14 items that are designed to measure individual stress for the last 30 days using a cut-off score of 14 reflecting clinically significant stress.
Covariates
A self-administered structured online questionnaire was employed to cover the participants’ demographic and clinical data, including marital status (single/married), age (below 30/30 and above), education (high school/university degree), employment (no/yes), smoking status (no/yes), the presence of chronic diseases (no/yes) and over the counter analgesics used to control dysmenorrhoea symptoms. To ensure the accuracy of data collection, both the generic name, the brand name, and the picture of the medication pack were all presented and checked out by the patients. The medication list used by the study participants included the following options: acetaminophen, non-steroidal anti-inflammatory drugs (NSAIDs), herbs, and “no analgesics.”
Outcome variables
Depression
The Patient Health Questionnaire-9 (PHQ-9) Arabic-validated version was used. The PHQ-9 is a short, self-administered scale based on the nine Diagnostic and Statistical Manual of Mental Disorders-IV criteria for diagnosing depression. 35 The PHQ-9 was previously used in Arab-speaking MS patients, with a cut-off score of above 14 to indicate severe depression symptoms as in previous literature.36–38
Anxiety
The General Anxiety Disorder-7 (GAD-7) is a short, self-administered scale with a cut-off point of 10 that has a sensitivity of 89% and a specificity of 82% for diagnosing generalized anxiety disorder. 39 The GAD-7 has previously been used in Arab-speaking MS patients with a cut-off score of above 14 to indicate severe anxiety symptoms as in previous literature.36,37,40
Insomnia
The insomnia severity index-Arabic version (ISI-A) was used to evaluate sleep quality. The ISI consists of 7 questions with Likert-type answers and a score range from 0–28, where a score above 14 indicates clinically significant insomnia, as in. 37 The ISI has been validated for use in the Arabic language.41,42
Dysmenorrhoea
The severity of dysmenorrhoea was assessed using the scale-type survey (working ability, location, intensity, days of pain, dysmenorrhoea [WaLIDD] score) was used 43 with a cut-off score of 8 for severe dysmenorrhoea.
Data Analysis
Data were analyzed using SPSS software version 21. The rates of depression, anxiety, insomnia, and dysmenorrhoea were analyzed using frequencies and percentages. To study which factors are associated with each of the outcome variables, four separate univariate analysis models were run, and potential confounding variables showing a cut-off value of p < 0.10 were included in the subsequent multivariate models. Then, these variables were used to build four backward step-wise multiple regression models for depression, anxiety, insomnia, and dysmenorrhoea to determine what covariates are independently associated with the outcome variables; only covariates with p < 0.05 were kept in the final model. The confidence intervals were set at 95% and significance at a p-value of 0.05.
Results
Study sample characteristics
From the total group of approached patients (n = 175), 129 patients consented to participate and fulfilled all of the inclusion criteria and no exclusion criteria. Most of the study participants were above 30 years old (n = 88, 68.2%), a total of 74 (57.4%) were married, and 92 (71.3%) were non-smokers. The dysmenorrhoea self-medications were as follows: 44 (34.1%) reported using herbals, 33 (23.6%) reported not using analgesics, 28 (21.7%) reported using acetaminophen, and 24 (18.6%) reported using NSAIDs.
Prevalence of depression, anxiety, insomnia and dysmenorrhoea
The participants demographics and details (n = 129).
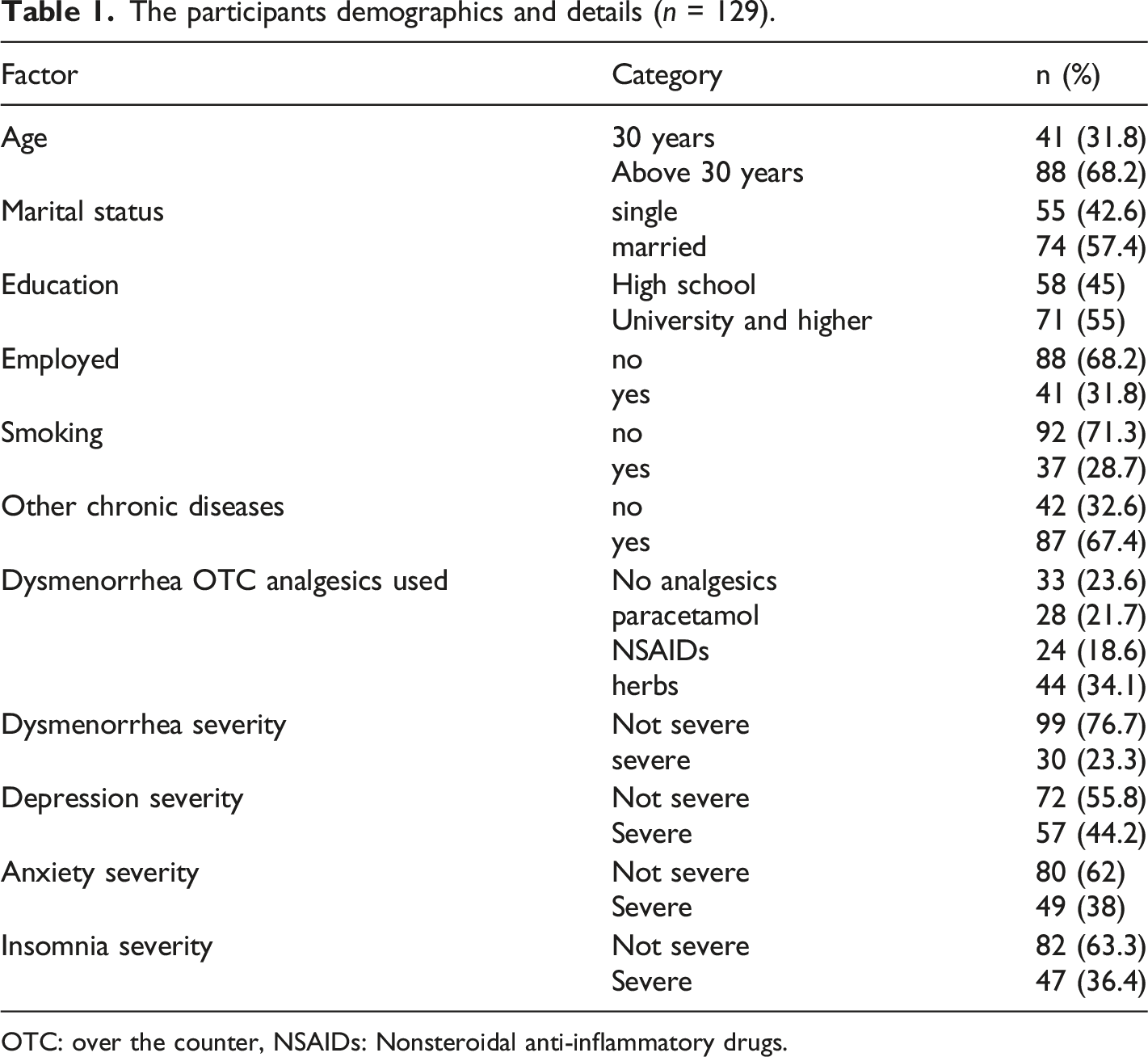
OTC: over the counter, NSAIDs: Nonsteroidal anti-inflammatory drugs.
Univariate analysis models
Four different univariate regression analysis for each of the outcome variables (depression, anxiety, dysmenorrhea, insomnia).
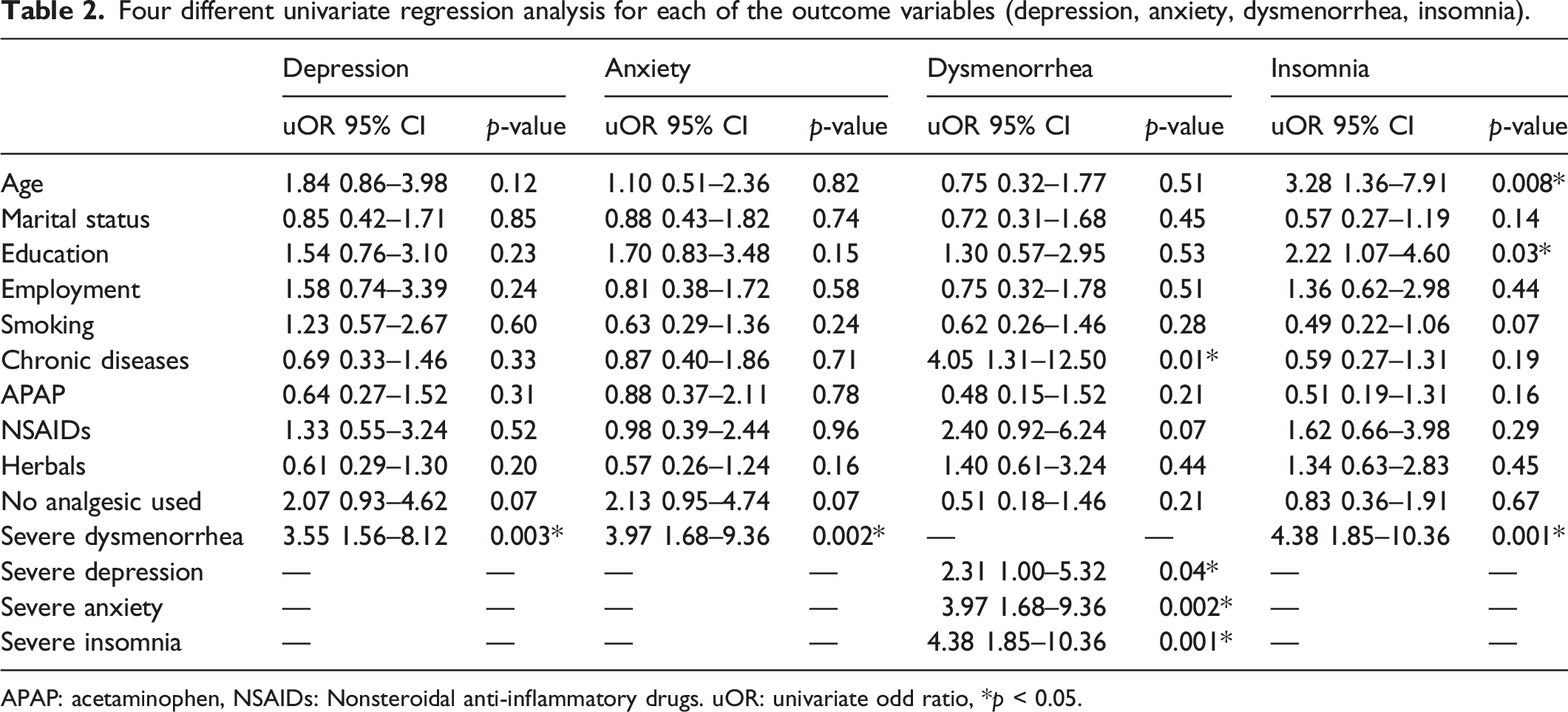
APAP: acetaminophen, NSAIDs: Nonsteroidal anti-inflammatory drugs. uOR: univariate odd ratio, *p < 0.05.
Multivariate analysis models
Four different multivariate logistic regression analysis for each of the outcome variables (depression, anxiety, insomnia and dysmenorrhea).
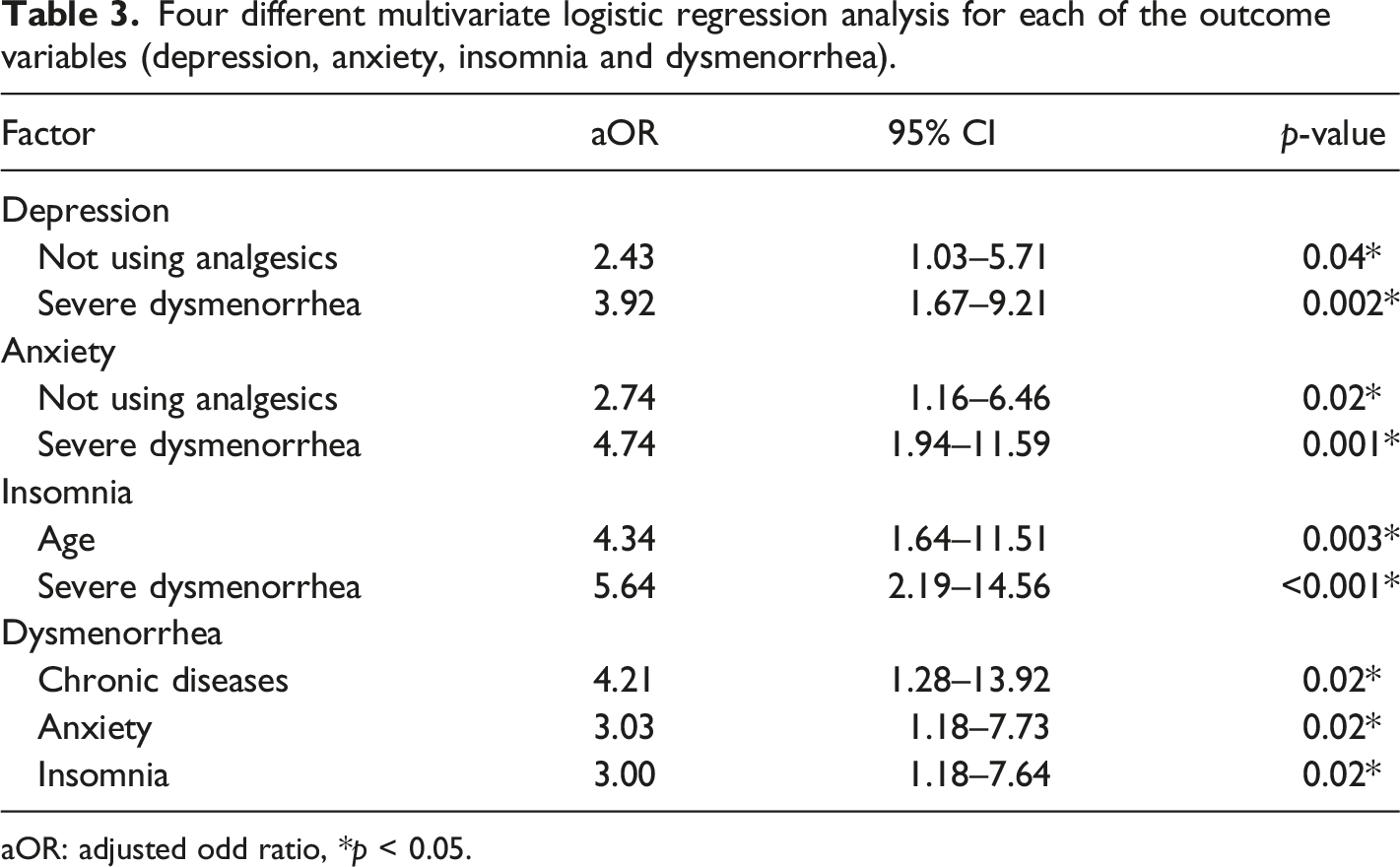
aOR: adjusted odd ratio, *p < 0.05.
Discussion
The present study aimed to explore the prevalence of depression, anxiety, insomnia, and dysmenorrhoea symptoms among a cohort of stressed fingolimod-treated women with MS and also to investigate which patients’ demographics and health factors are associated with these symptoms.
Severe depression symptoms were reported in 55.8% of the study sample, although this rate is considered high compared to the normal population; however, it is consistent with the existing literature showing similar prevalence rates of depression in MS patients, including males and females. For example, several studies reported depression in 50% of MS patients;15,44 however, the rate of depression in the current study is higher than that of the rate found in other women with MS. For example, a similar study that examined depression symptoms in a cohort of 111 women with MS stated that 25% presented with depression. 17 This difference may be associated with many social, environmental, and cultural factors and different coping mechanisms;45,46 also, the scales used in the studies could result in variation in the outcome. In our study, women with severe dysmenorrhoea and women who did not use dysmenorrhoea analgesics were at a higher risk for severe depression.
Although the complete underlying mechanism has not yet between uncovered, the association between dysmenorrhoea and depression has been established. 47 Experiencing monthly repeated menstrual pain could increase the risk of depression; also, depression could increase pain sensitivity and therefore enhance pain perception.48,49 Therefore, dysmenorrhoea cannot be explained only in the context of uterine inflammation; however, the psychological aspect that exacerbates psychological distress is of paramount importance, especially in vulnerable women. 50
The present study reported a high rate of anxiety of 62%. Our results confirm previous studies demonstrating that anxiety in MS is higher than in healthy individuals. Although several studies in Norway concluded that anxiety prevalence in MS ranged between 14% and 41%,7,51 few results examined anxiety rates in women with MS, while one study reported the anxiety rate to be 30% (Dahl). The high anxiety rate in our study could be a result of the fact that women are anxious about the nature of the disease and the healthcare quality service provided (i.e., patients with MS have to wait for several months to get a neurologist visit or MRI scan in the public sector). Also, this high rate of anxiety could be due to the lack of mental health support services in some developing countries, a service that is faced with many social and cultural obstacles such as stigma. 52 Our results indicate that, as in depression, severe anxiety symptoms were related to dysmenorrhoea and a lack of analgesia. This is confirmed by previous studies where anxiety in MS patients was tightly related to chronic pain. 53 According to the literature, women with pelvic inflammation and pain, including dysmenorrhoea, were at a higher risk of anxiety compared to pain-free controls. 14 This could be explained by central sensitization of the central nervous system for abdominal pain, thus leading to intense pain sensation. 54 In addition, chronic monthly pain is also an emotional experience that can aggravate anxiety. 50
Severe insomnia symptoms were reported in 36.4% of our study sample and were related to dysmenorrhoea. It has been agreed that insomnia prevalence in MS patients is higher than that in controls. 20 Sleep disturbances are common in MS, where published studies indicate insomnia prevalence to be from 12.5% to 78% in MS patients of both sexes. One cross-sectional study recruiting more than 800 women with MS reported that 26% described initiating and maintaining sleep (Bamer 2008).
Previous studies have indicated that women with primary dysmenorrhoea have low sleep quality.55,56 It has been suggested that poor sleep during menstruation is related to enhanced pain sensitivity.57,58 Almost one-third of women with significant dysmenorrhoea symptoms experienced insomnia symptoms during the menstrual period. 59
We report severe dysmenorrhoea symptoms in 23.3% of women with MS, which is related to diagnosis with other chronic diseases, anxiety and insomnia, although the cross-talk between MS and the menstrual cycle is established.29,30 For instance, MS exacerbations are usually evident during the premenstrual period due to the low levels of estrogen and progesterone;31,32 moreover, MS relapses were seen to subside during pregnancy. 31 To the best of our knowledge, no previous studies have investigated dysmenorrhoea prevalence in women with MS.
The association between anxiety, insomnia, and dysmenorrhoea is bidirectional. Women reporting severe dysmenorrhoea are at a higher risk of suffering from mood disturbances such as anxiety, depression, and insomnia.60–63
Psychiatric distress plays a role in the regulation of reproductive hormones, and the hypothalamic-pituitary-adrenal (HPA) axis is activated during stress. 64 Women diagnosed with anxiety and insomnia had a lower threshold for pain and more severe somatic symptoms such as dysmenorrhoea. 65 Although the exact mechanism underlying this association is still undetermined, hormonal fluctuations and patient awareness are possible explanations. 66 Also, the diagnosis of chronic diseases was associated with dysmenorrhoea. Dysmenorrhoea is mainly characterized by pain due to inflammation and is best treated by anti-inflammatory drugs;28,67 at the same time, inflammation is implicated in many chronic diseases such as hypertension, diabetes, and psychological distress, such as anxiety and insomnia.68–70 Therefore, damping the inflammatory pathways could improve dysmenorrhoea symptoms and its associated risk factors.
Mental health studies focusing on vulnerable women with disabling diseases in developing countries are limited. This work contributes to the existing literature by reporting the prevalence of depression, anxiety, insomnia, and dysmenorrhoea in stressed fingolimod-treated women with multiple sclerosis and by identifying the demographics and health factors that are associated with these symptoms. However, the lack of psychiatric assessment was a limitation, but this has been overcome by using a validated scale for all outcome measures and using rigorous inclusion criteria.
Conclusion
In conclusion, the reported rates of depression, anxiety, insomnia, and dysmenorrhoea are considered high and require medical and psychiatric attention to improve the well-being of these vulnerable patients.
Footnotes
Acknowledgments
The corresponding author would like to thank Suzi, Nour, and Yasmina for their support.
Declaration of conflicting interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Yarmouk University.
Ethics statement
This is a part of a larger cross-sectional study. The study was approved by Yarmouk University IRB committee (16/2022).