
Abstract
Objective
Premenstrual syndrome (PMS) and premenstrual dysphoric disorder (PMDD) are experienced in the luteal phase among women of reproductive age and are known to affect quality of life. This study sought to determine the prevalence and correlates of PMS and PMDD in women aged 18‐25 in Turkey.
Method
A cross-sectional study was conducted between December 2022 and May 2023, which recruited 1125 female college students. A personal information form, the International Physical Activity Questionnaire, and the Premenstrual Syndrome Scale (PMSS) were administered. Participants who met criteria for PMS during three consecutive menstrual cycles based on the ACOG and PMSS scores were diagnosed as having PMS. Participants who met the criteria for PMDD during three consecutive menstrual cycles based on the DSM-V were diagnosed as having PMDD. Logistic regression analysis was used to determine correlates of PMS and PMDD.
Findings
PMS was found in 49.2% and PMDD in 48.0% of the participants. Women having a blood group type B compared to those with blood group type A were more likely to have PMS (OR = 151.8, 95% CI = 54.5-422.6). In addition, women with PMS were less likely to be physically active based on the metabolic equivalent of task score (OR = 0.99, 95% CI= 0.98-0.99). Menstrual cycle duration was also longer among those with PMDD (OR = 1.47, 95% CI= 1.25-1.72), as was daily caffeine intake (OR = 1.01, 95% CI= 1.00-1.01). PMDD score was also found to be associated with major depressive disorder (OR = 1.06,95% = 1.05-1.07).
Conclusions
PMS and PMDD among young women in Turkey were associated with blood groups, MET scores, and other clinical characteristics that may help clinicians to identify these conditions.
Keywords
Introduction
Premenstrual Syndrome (PMS) is a recurrent cluster of physical and psychic symptoms during the luteal phase of the menstrual cycle. 1 The etiology of PMS is uncertain. Since PMS symptoms co-occur with the hormonal fluctuations of the menstrual cycle, hormonal disproportion like estrogen surplus and progesterone deficiency have been proposed. Symptoms are also associated with serotonin to link as a key etiological factor. 2 Premenstrual symptoms are prevalent, affecting about half of women of reproductive age worldwide. However, prevalence rates vary widely in different studies and countries depending on the characteristics of participants, personal attitudes, lifestyle, stressors, socio-cultural factors, environmental conditions, and different diagnostic criteria.3–5 Although the meanings attributed to menstruation vary between societies, it is reported that there are many taboos and myths related to this period, especially in low and middle-income countries. Women who faced negative attitudes experience body dysfunction and perceive themselves as “dirty” and as a result, isolate themselves in their work/school and social lives.6–8
For diagnosing of PMS, the most commonly used diagnostic criteria are those of American College of Obstetricians and Gynecologists (ACOG).3,9 ACOG has published 10 diagnostic criteria for PMS. PMS is diagnosed when at least one of the six affective (depression, angry outbursts, anxiety, irritability, confusion, and social withdrawal) and at least one of the four somatic symptoms (breast tenderness, abdominal bloating, headache or swelling of extremities) are experienced in the luteal phase of three consecutive cycles and disappeared within four days of the onset of bleeding. 9
Premenstrual Dysphoric Disorder (PMDD) is more severe at the end of the PMS spectrum that is characterized by the cyclic recurrence of psychological manifestations, including irritability, nervousness, agitation, anger, insomnia, difficulty in concentrating, severe fatigue, depression, anxiety, and confusion. 10 In order to diagnose PMDD, at least five of the seven criteria (A through G) in the Diagnostic and Statistical Manual of Mental Disorders-V (DSM-V) must be present and at least one of them must be one of the first four (A through D) criteria.1,10
This study aims to determine the prevalence and correlates of PMS and PMDD in women aged 18-25.
Method
This cross-sectional descriptive study included 1125 women from Istanbul Medipol University, between December 2022 and May 2023. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) checklist was used in planning, implementation, and reporting of the study design. 11
The minimum sample size required in the study was decided by power analysis (G*Power Version 3.1.9.2). The effect size was calculated according to the data obtained from previous studies.3–5 Accordingly, the effect size was taken as 0.40, and type 1 error rate (α) = 0.05 and study power (1- β) 0.95 (Type II error = 0.05) were used. The minimum sample number was calculated as 356 in total.
An announcement regarding the research was made to the female students at Istanbul Medipol University and participants were recruited between October 2022 and November 2022. The research announcement was delivered to a total of 2188 female students. The number of participants who were not included in the study due to refusal was 263. One hundred 60 participants were excluded from the study because they stated that they were not in the luteal phase at the time of the announcement of the study, and 48 participants were excluded because they stated that their cycles were irregular. Furthermore, 12 participants were excluded because they were not in the specified age range, 10 were excluded because they were pregnant, and five were excluded because they were obese. Three hundred-seven participants were excluded since they only met the ACOG 9 criteria, and 200 were excluded because they did not meet the diagnostic criteria for PMS in the second or third menstrual cycle. 12 participants were excluded from the study because of using oral contraceptives, four were using psychiatric drugs, 33 were smoking, and nine were using alcohol. After excluding 800 people, 1125 voluntary participants were included in the study.
The factors confirmed to be the common associated factors for PMS and PMDD in the literature were considered when determining the inclusion and exclusion criteria for the participants.1,3,9 In this way, it was aimed to focus on associated factors that are not commonly known.
Inclusion Criteria
In three consecutive menstrual cycles, those who met the ACOG 6 diagnostic criteria for PMS and the criteria for the Premenstrual Syndrome Scale 12 (min: 110 points), 18–25 years old, with regular cycle and regular bleeding time (21–35 days, 3–10 days bleeding time), who did not smoke or did not consume alcohol, did not have a history of pregnancy or current pregnancy, and did not use oral contraceptives and psychiatric drugs were included in the study.
Exclusion Criteria
Those who took vitamin or hormone supplements until three months before participating in the study, who were obese (BMI >30 kg/m2), who experienced stressful life events (marriage, divorce, birth, loss-death, surgical intervention) until three months before participating in the study, who had chronic diseases (thyroid diseases, diabetes mellitus, hypertension, hyperlipidemia, cardiovascular system diseases, endocrine diseases, autonomic nervous system diseases, psychological diseases, or gynecological diseases), who had a shorter or longer menstrual cycle than necessary (<24 or >35 days), who had a shorter or longer bleeding time than necessary (<3 or >10 days), who meeting the diagnostic criteria of only ACOG 9 or only PMSS, 12 who did not meet the diagnostic criteria of both measurement tools for PMS during three consecutive menstrual cycles were excluded from the study.
Data Collection Tools
In data collection, the Personal Information Form (including characteristics of participants, PMS symptoms, and deterioration in daily premenstrual activities, ACOG’s 9 diagnostic criteria for PMS, and DSM-V diagnostic criteria for PMDD 1 ), Premenstrual Syndrome Scale 9 and International Physical Activity Questionnaire13,14 were used.
Personal Information Form
The personal information form consists of personal data, PMS symptoms, and deterioration in daily premenstrual activities.4,5 The first part of the form is focused on age, height, weight, age at menarche, blood group, menstrual pattern, duration of menstrual bleeding (in days), amount of bleeding, family history of PMS, physical activity, smoking, and daily caffeine intake. Additionally, the data related to sociodemographic and obstetric information, such as physical activity status, are questioned. The second part includes items related to the ACOG 9 diagnostic criteria for PMS and DSM-V diagnostic criteria for PMDD. 1 The self-reported Personal Information Form was completed by the participants for at least three consecutive menstrual cycles.
Since students at this college involve in clinical practice, they have routine blood tests done every year. The blood groups of the students were obtained from these test results.
Premenstrual Syndrome Scale (PMSS)
It is used to examine the physical, psychological, behavioral, and social symptoms of PMS and how they affect the daily lives of women with this condition. PMSS is a scale developed by Gençdoğan 12 according to DSM III and DSM IV, aiming to measure the severity of premenstrual symptoms. This scale, widely used in our country, is a 5-point Likert-type scale consisting of nine sub-dimensions and a total of 44 items, which the individual marks by taking into account the “being in the period one week before the period”. The minimum score from the scale is 44, the maximum score is 220, and above 110 points are considered “have PMS”. A high PMSS score indicates more severe premenstrual symptoms. The total Cronbach’s alpha coefficient of the scale is 0.75, and its sub-dimensions range from 0.75 to 0.91. 12 In this study, Cronbach’s alpha coefficient was determined as 0.82.
International Physical Activity Questionnaire Short Form (IPAQ Short Form)
It was developed to determine participants’ physical activity levels between the ages of 15–65. 13 The validity and reliability study was carried out by Saglam et al. 14 There are four short and four long versions of the form. The IPAQ Short Form has seven questions that provide information on time spent walking, moderate-intensity, vigorous activities, and sitting. Calculating the total score includes the sum of time (minutes) and frequency (days) of walking, moderate-intensity activity, and vigorous activity. The energy required for activities is calculated with the Metabolic Equivalent Task (MET)-minute score. Standard MET coefficients have been established for these activities. These are sitting (1.5 MET), walking (3.3 MET), moderate-intensity activity (4.0 MET), and vigorous physical activity (8.0 MET). With the MET score collected, individuals can be evaluated as inactive, minimally active, and very active. 14
Data Collection Method
After the research announcement was made, the Personel Information Form and PMSS were filled in by face-to-face interview method with the participants who met the criteria for inclusion in the research. Participants who scored above 110 on the PMSS and met ACOG's 9 diagnosis criteria for PMS were informed that they would be followed up for three consecutive menstrual cycles. At the same time, participants who scored above 110 on the scale were also evaluated in terms of meeting DSM-V 1 diagnosis criteria for PMDD.
Statistical Analysis
Research data were analyzed with SPSS 28.0 (IBM SPSS Statistics for Macintosh, Version 28.0.). Frequency, percentage, mean, and standard deviation statistics were used to determine the descriptive characteristics of the participants. Relationships between continuous variables were examined through Pearson correlation analysis. Chi-square and independent groups t test analyses were used to determine the variables associated with the participants’ presence of PMS and PMDD. Logistic regression analysis was applied to determine the factors affecting PMS and PMDD.
Ethical Considerations
Ethics committee approval was obtained from the local ethics committee (the approval number: 1054, the date of approval:08/12/2022). The study was conducted under the Declaration of Helsinki and followed the ethical standards of the country of origin. Written permission was obtained from the university where the research would be conducted. Written informed consent was obtained from all participants before enrolment in the study.
Results
The mean age of participants (n = 1125) was 20.9 ± 1.2 years (range 19–25 years), the mean PMSS score is 115.8 ± 37.7 (range 51–217), the mean number of DSM-V symptoms was 4.7 ± 3.9 (range 0–11). As a result of the analysis made to evaluate the ACOG and PMSS criteria together, PMS was defined in 49.2% (n = 553) of the participants. As a result of the analysis based on the DSM-V criteria, PMDD was found in 48% (n = 540), and 77.80% (n = 436) of the participants diagnosed with PMS also had PMDD.
There was a significant difference between the participants’ PMS status and blood groups (p = 0.00), family history of PMS (p = 0.00), and MET score (p = 0.00), while no statistically significant difference was found with the Rh factor, age at first menstruation, cycle period, cycle duration, BMI, and caffeine intake (p > 0.05). In the logistic regression analysis performed to determine the factors associated with the presence of PMS, it was determined that having the B, AB, and 0 blood groups increased the presence of PMS compared to the A blood group (OR = 151.8, 95% CI = 54.5- 422.6; OR = 76.7, 95% = 27.0- 217.3, and 1.97, 95% CI = 1.16-3.34, respectively). An increase in MET score decreased the presence of PMS (OR = 0.98, 95% CI = 0.98- 0.99).
Comparison of Descriptive Characteristics by PMDD Status (DSM-V) (N = 1125).
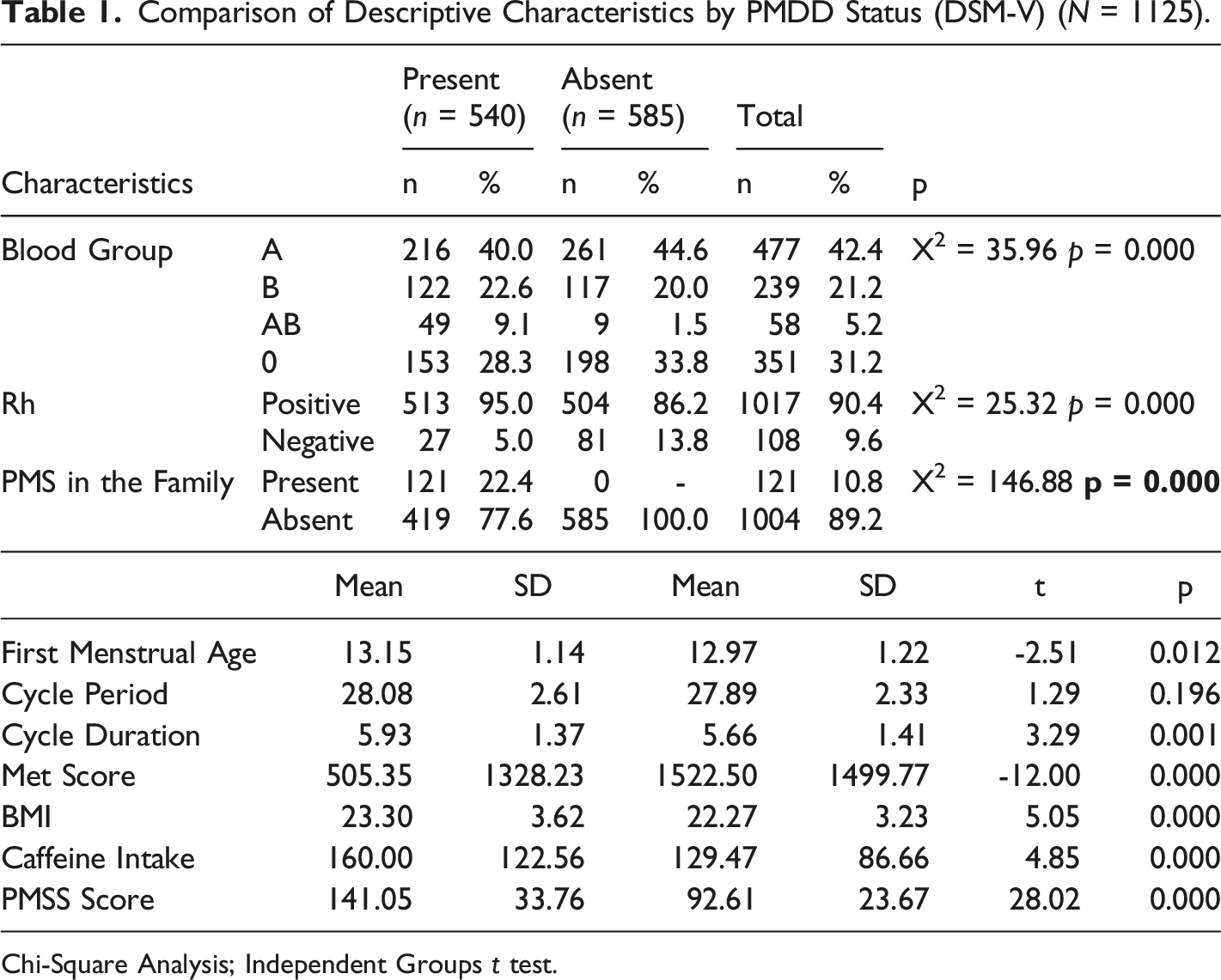
Chi-Square Analysis; Independent Groups t test.
Logistic Regression Analysis for Factors Associated with PMDD.
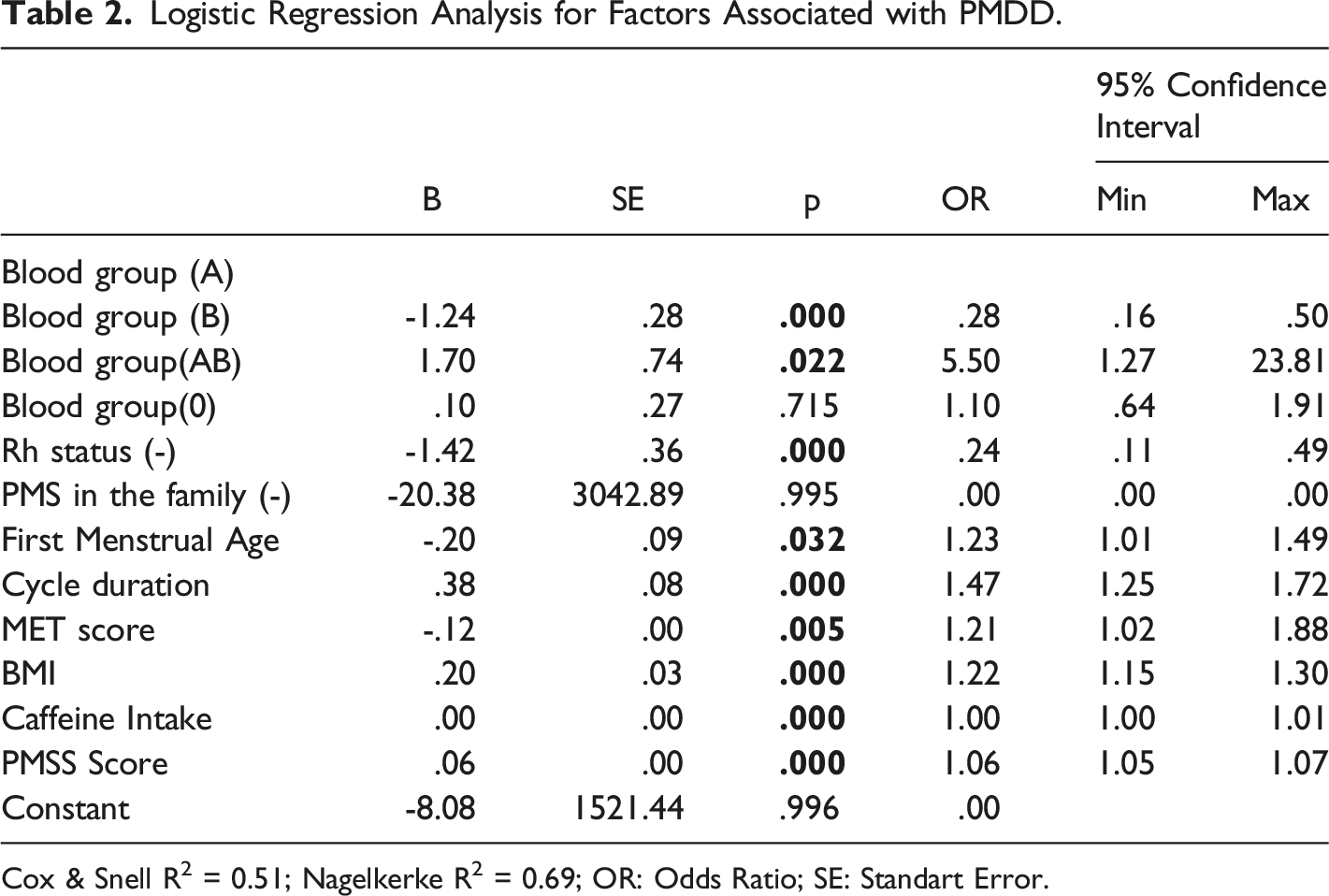
Cox & Snell R2 = 0.51; Nagelkerke R2 = 0.69; OR: Odds Ratio; SE: Standart Error.
Discussion
As a result of studies conducted in different ethnic groups and countries, it has been reported that 90% of women of reproductive age experience at least one or two mild symptoms of PMS. 20 to 40% of these women experience severe PMS symptoms that affect their social lives.3,4 In this study, the prevalence of PMS was 49.2% among women aged 18-25. The estimate using the PMDD 1 checklist in this group was 48.0%. The different results regarding the prevalence of PMS in the literature may be due to different measurement tools. In this study, the ACOG 9 criteria and PMSS 12 are used for the diagnosis of PMS to evaluate the PMS objectively. As noted in the methods section, only those meeting the PMS diagnostic criteria for a single measurement instrument (n:307) were excluded from the study. This result shows us that there may be differences between measurement tools. An important point here is that the use of the ACOG diagnostic criteria results in more PMS diagnoses.
Lifestyle factors such as physical activity had a significant association with PMS. 15 A study from Egypt revealed a positive correlation between PMS and excess intake of sweet food. It also showed that other factors, such as junk food and coffee intake, were significantly associated with PMS. Hence, making it evident that lifestyle factors have a significant association with PMS and PMDD. 15 Another study among women university students to assess the factors associated with PMS revealed that dietary factors such as consumption of fast food, drinks containing sugar, and deep-fried foods, and lifestyle factors such as less habitual exercise and poor sleep quality are significantly associated with PMS. 16 A study with medical students showed that lifestyle factors such as sleep, physical activity, and total tea/coffee consumption were significantly associated with PMDD. 17 In the current study, it was deduced that while the amount of daily caffeine intake did not affect PMS, it increased PMDD by 1.007 times. In addition, it was determined that physical exercise was effective on PMS and PMDD consistent with the literature, and PMS and PMDD decreased as physical activity increased.
Recent studies have focused more and more on the genetic factor that causes menstrual irregularity. The results of our study are in accordance with the previous study, which indicated an association between menstrual disorders and blood type distribution.18,19 In a study conducted with medical students, PMS symptoms were mainly seen in A and B blood groups, similar to our results, while they were found the least in AB blood groups. 20 Hence, further studies are needed to determine the relationship between blood groups and PMS.
Limitations
This is a cross-sectional study that involved a “convenience” sample of college students from a single university in Turkey. The study had multiple exclusion criteria that limit the generalizability of the current findings only to those women fulfilling inclusion criteria, which is a rather restricted sample of college students. Future longitudinal studies are needed to determine the direction of causation in the correlates identified in this study.
Conclusions
The results of the research showed that PMS status is associated with blood groups, family history of PMS, and MET score, and PMDD status is associated with blood groups, Rh factor, family history of PMS, age at first menstruation, cycle duration, MET score, BMI, caffeine intake, and PMSS score. It is common knowledge that the symptoms experienced in PMS and PMDD negatively affect women’s life quality. Knowing the associated factors of women with these symptoms by health professionals and providing counseling accordingly can improve women's quality of life.
Footnotes
Author Contributions
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The name of the ethics committee: Istanbul Medipol University Clinical Research Ethics Committee.