
Abstract
Objective
This study examined the perception of dental pain and its relationship to pain anxiety, dental anxiety, and mental pain.
Methods
This cross-sectional study was conducted on 328 patients referred to dental clinics in Kermanshah (Iran) from 2020 to 2021. The instruments used in this study included scales assessing pain anxiety, dental anxiety, mental pain, and pain perception.
Results
There was a significant relationship (p = .001) between pain perception with dental anxiety (r = .38), pain anxiety (r = .45), and mental pain (r = .25).
Conclusion
Psychological factors are associated with the perception of dental pain. Given the importance of dental care to overall health, psychological interventions may help to reduce the perception of dental pain and fear of seeing dentists in Iran.
Introduction
The International Association for the Study of Pain (IASP) defines pain as an unpleasant emotional experience related to actual or potential risk. Pain is a symptom of many diseases and appears in different ways. 1 Many factors contribute to the formation and exacerbation of pain. Biomedical factors and nerve stimulation are the most critical factors in forming pain. Researchers have recently shown that psychological factors affect the continuity and worsening of pain.2,3
A person’s experience of pain and how to interpret it plays an essential role in the perception of it. The part of this experience is only related to physical factors. 4 However, considering the multidimensional role of pain, psychological factors also affect pain perception. Research in medicine focuses on investigating biomedical factors and their relationship with the body.4,5
Patients with a homogeneous level of damage to body organs present different levels of pain intensity. This can indicate different perceptions and interpretations of pain. 6 It is possible that a person endures the most severe injuries and fractures and complains of less pain than expected, and another person reports a lot of pain in the case of minor damage to the body.7,8 Such an experience is harrowing and is one of the main reasons for visiting a dentist.
Medical researchers have investigated the role of psychological factors in pain.9,10,11 Research has shown that psychological distress affects aggravating diseases such as chronic pain, cancer, and rheumatism.10,12,13 Turk et al.’s study (2002) pointed out the importance of psychological factors to deal with and improve the quality of life in patients with chronic pain. The evaluation of symptoms, their ability to self-manage pain, and their pain fear are also crucial in the patient's perception of pain. 14
Dentistry is one of the pain-related fields. People usually go to the dentist to treat pain. 15 Dental pain is one of the reasons for patients avoid receiving dental services. Therefore, a comprehensive examination of pain in dentistry is necessary. The common cause of dental pain is damage to the tooth's nerves. 16 People usually benefit from repair and denervation services for pain relief. In some patients, the intensity of the pain report is more than the amount of damage, and when receiving services, patients exaggerate their perception of pain. 17 Other patients still complain of pain after specialized interventions and express pain without organic damage.18,19 This can be due to psychological factors such as anxiety and depression and their effect on causing sensitivity to pain.
Pathological anxiety gradually causes these patients to show anxiety about their pain. As a result, pain anxiety is created. 20 Greenberg and Byrne (2003) classified pain anxiety as a specific type of fear. 21 Avoiding being in painful areas and predicting the recurrence of pain can be mentioned as the main symptoms of pain anxiety. 20 Patients with dental pain predict the occurrence of severe pain by mentally imaging the dental setting and equipment and reviewing their previous experiences and others' reports.22,23 The result of these images and extreme thinking about pain is mental rumination, worry, and obsessive thoughts about the experience of pain.22,24,25,26,27 If this process continues, pain anxiety about dental services will develop. Pain anxiety can lead to hypervigilance about pain stimuli, making patients anxious and worried about past and future painful symptoms. 17 Finally, this unpleasant experience causes patients to avoid receiving medical services and, as a result, become more disabled.
Studies have shown that pain anxiety plays a vital role in pain perception, and paying more attention to it in dentistry is necessary. In their research, Strahl et al. examined the role of pain anxiety, coping, and self-efficacy in the functioning of rheumatoid arthritis patients. The results showed that the predictor variables explained between 9 and 38 percent of the variance of the criterion variable. 28 Studies have shown that pain anxiety plays a fundamental role in pain perception, and paying more attention to it in dentistry is necessary.
Based on previous studies, Dental pain is not only caused by nerve damage; part of it includes the psychological suffering experienced by the patient.29,30,31 Mental pain is one factor that plays a role in the perception and exacerbation of pain.32,33 In the research literature, mental, emotional, psychological, and psychological pain are used interchangeably and refer to a typical structure. The central theme of mental pain is suffering and despair. 34 According to Cassel’s (1999) view, mental pain is a type of psychological experience of suffering, and it does not only belong to the physical and physical condition. 35 The report of specialists indicates that such incidents are seen in patients who refer to dental clinics, and it seems necessary to investigate the extent of its impact on the perception of pain. In a study, Raiisi et al. investigated the relationship between pain anxiety, mental pain, and pain perception in musculoskeletal patients. The results showed that mental pain is a mediating variable to pain anxiety and perception. 36 Studies have shown that mental pain plays an essential role in pain perception, and paying more attention to it in dentistry is necessary.
Another psychological variable that most research focuses on is dental anxiety. Dental anxiety includes fear or stress about the dental intervention.37,38 Things like needles, drills, or the dental setting, can trigger dental anxiety. Some of the symptoms of dental anxiety to conceal pressure comprise sweating, suffering from tachycardia, having the symptoms of crying or panic, retreating, and using aggressiveness.39,40
The etiology of dental anxiety is not well-known because dental anxiety is a multiple and complex phenomenon.41,42 Some factors that cause and develop this kind of anxiety include personality characteristics, pain fear, pain sensitivity, fear of injury and blood, and coping styles.43,44 Moreover, the painful and damaging experience of dentistry, especially conditional experiences during childhood in the dental settings, and observational learning via observing fear of pain by family members are the other factors causing this anxiety. 45 Various studies have investigated the relationship between dental anxiety and pain perception.46,47 In a study, Sanikop et al. (2011) investigated the relationship between dental anxiety and pain perception during scaling. The results showed a significant association between dental anxiety and pain perception. 46 As studies have shown, dental anxiety plays an essential role in pain perception, and paying more attention to it in dentistry is necessary.
Also, anxiety can manifest itself in various forms, including pain anxiety and mental pain, and such experiences may manifest themselves in dental settings. The space and place where dental interventions are performed can also intensify the patient’s anxiety and suffering. Therefore, examining the association between dental anxiety and pain anxiety, mental pain, and pain perception seems necessary. Finally, the present study analyzed the relationship between the perception of dental pain and pain anxiety, mental pain, and dental anxiety in the Iranian sample.
Materials and Methods
The method of the present study was a cross-sectional study. The statistical population included all people referred to dental clinics in Kermanshah (Iran) city in the last six months of 2020 and the first quarter of 2021. Two researchers participate in collecting questionnaires. Krejcie and Morgan's table was used to determine the sample size and the convenience sampling method. Considering the average number of patients in the Kermanshah (Iran) dental clinics, at least 300 people were needed for the statistical analysis. Finally, 449 patients met the study inclusion criteria. The inclusion and exclusion criteria in the current study are as follows:
Inclusion criteria: (1) receiving dental services, (2) being able to read and write, (3) having informed consent to complete the questionnaires, and (4) not using analgesics and palliatives for a long time.
Exclusion criteria: (1) random response and bias in answering the questionnaires, and (2) incomplete completion questionnaire.
According to the inclusion criteria, 350 participants filled out the questionnaires used in this study. Afterward, the information of the participants was evaluated by exclusion criteria, and the data of 22 of them were excluded from the research process. Finally, the information from 328 participants was analyzed. The sampling process was carried out by two master's students in clinical psychology in person at dental clinics. Figure 1 shows the flowchart of the research sampling process. The flowchart of the research sampling process.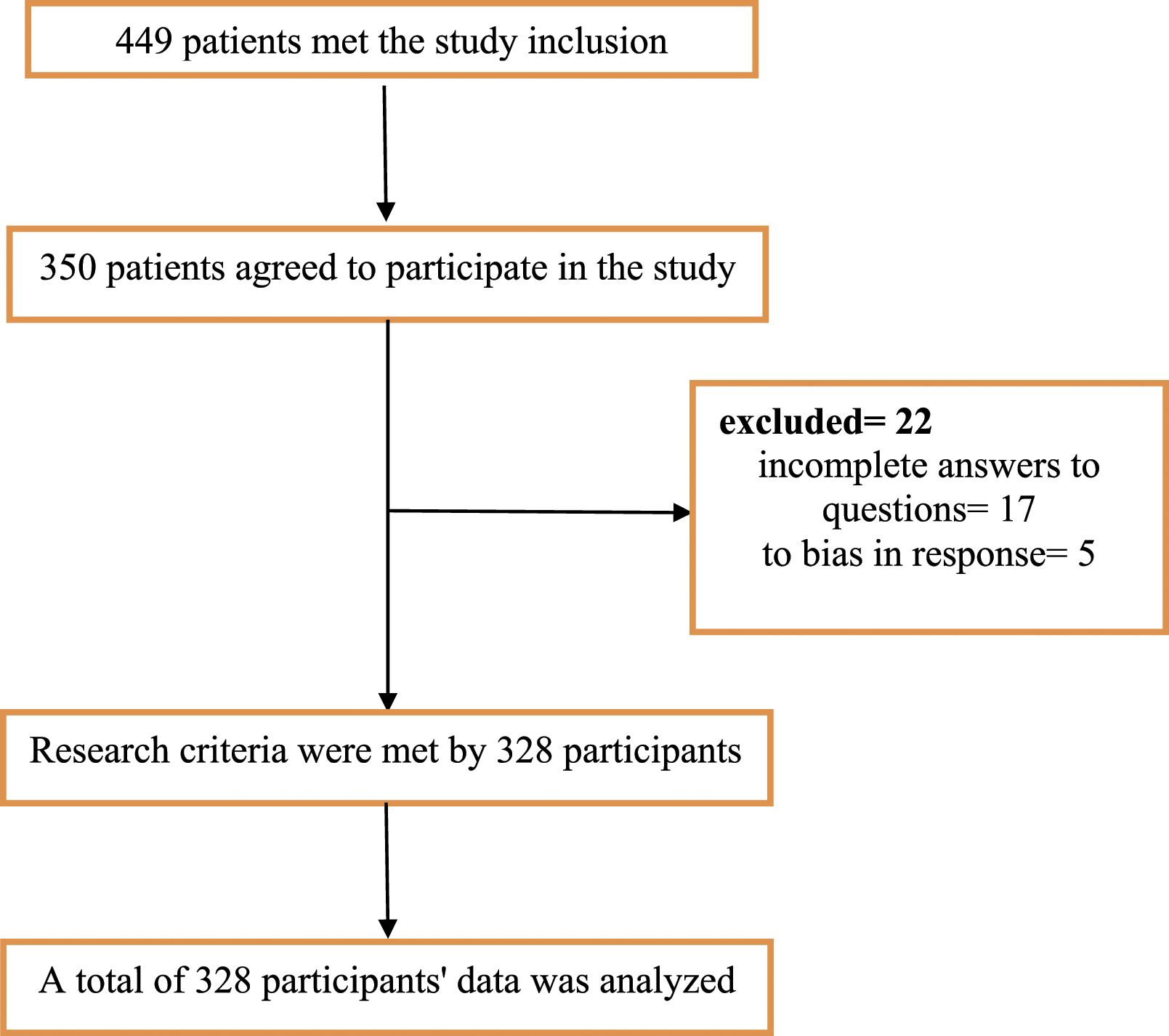
Procedure
After receiving an introduction letter from the Vice-Chancellor for Research and Technology of Kermanshah University of Medical Sciences, the researchers were referred to the dental clinics in Kermanshah. Moreover, after coordination with the clinics, the patients were asked to complete the questionnaires according to the inclusion criteria.
Measures
Revised McGill Pain Questionnaire (SF-MPQ-2)
2009 Dworkin et al. revised the McGill Pain Questionnaire. They added neuropathic and non-neuropathic pain symptoms to 22 items by modifying the response framework to this questionnaire. All subscales in the Likert scale ranged from not feeling pain = 0 to severe pain = 10. In this questionnaire, the range of scores ranges from 0–220. Cronbach’s alpha coefficient for subscales of continuous pain (0.87), varied pain 0.87, neuropathic pain 0.83, and emotional pain 0.86 was reported. 48 Besides, Tanhaee et al. (2012) said Cronbach's alpha coefficients for the whole questionnaire 0.92, the subscales of sensory pain 0.87, emotional pain 0.87, and neuropathic pain 0.78. 49
Dental Anxiety Inventory
The questionnaire was developed by Stouthard, Mellenbergh, and Hoogstraten (1993), including 36 items to assess frightening statements about dental conditions. All items in the Likert scale ranged from completely false = 1 to completely true = 5. In this questionnaire, the range of scores varies between 36–180. These researchers reported Cronbach's alpha coefficients of this questionnaire between 0.96 and 0.98 and its reliability between 0.84 and 0.87. 50 Furthermore, Yousefi and Piri (2017) said Cronbach's alpha coefficient of 0.94. 51
Orbach & Mikulincer Mental Pain Scale
This scale was created by Orbach et al. (2003), including 44 items in 9 subscales. The subscales had irreversibility, loss of control, narcissistic wounds, emotional flooding, freezing, self-estrangement, confusion, social distancing, and emptiness. All items in this questionnaire were graded on a Likert scale, ranging from strongly disagree = 1 to strongly agree = 5. In this scale, the range of scores varies between 44–220. They reported the test coefficients of the retest of this questionnaire between 0.79 and 0.94 after three weeks. In addition, Cronbach’s alpha coefficient reported the subscales of this questionnaire between 0.75 and 0.95.33,52 They said a Cronbach’s alpha coefficient of 0.97 for the whole questionnaire and between 0.62 and 0.95 for the subscales. In a study by Karami et al. (2018), the 6-factor model (emptiness, emotional flooding, loss of control, irreversibility, social distancing, and self-estrangement) was confirmed. 51
Pain Anxiety Symptoms Scale (PASS-20)
This scale was developed by McCracken et al. (2002) that includes 20 items and four subscales (cognitive anxiety, avoidance behavior, fear of pain, and the physiological symptoms of anxiety). All items in the Likert scale are scored from never = 0 to always = 5. In this scale, the range of scores varies between 1–100. 20 In a study by Kreddig et al. (2015), Cronbach's alpha was reported as 0.90 for the whole scale and between 0.66 and 0.84 for the subscales. 53 Paknejad et al. (2014) reported the reliability coefficient of the quarterly subscale retest, ranging from 0.48 to 0.57, and the internal consistency coefficients of the subscales between 0.81 and 0.91. 54
Statistical Analysis
SPSS-24 was used to analyze the research results. The descriptive results were evaluated using the mean, standard deviation, frequency, and percentage indicators. Kurtosis and skewness indices were run to assess the normality of the data. Further, the Pearson correlation coefficient and Multiple Linear Regression analysis were used to evaluate the study's main findings.
Results
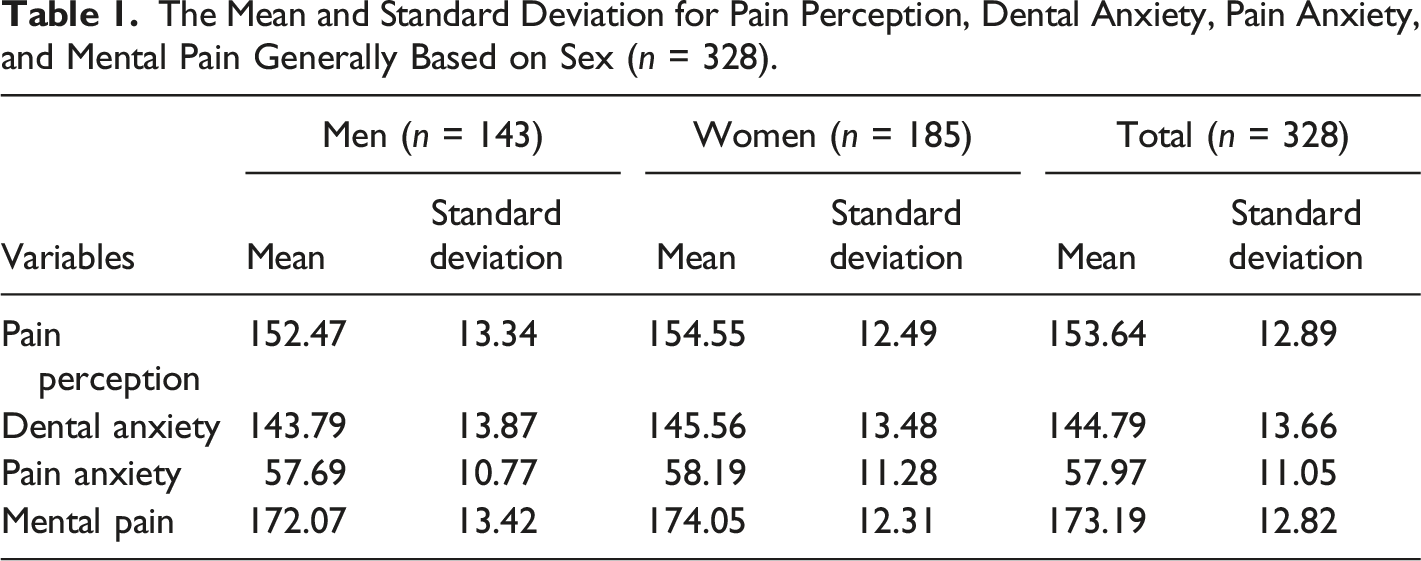
The Mean and Standard Deviation for Pain Perception, Dental Anxiety, Pain Anxiety, and Mental Pain Generally Based on Sex (n = 328).
The Correlation Coefficient Matrix for Pain Perception, Dental Anxiety, Pain Anxiety, and Mental Pain (n = 328).
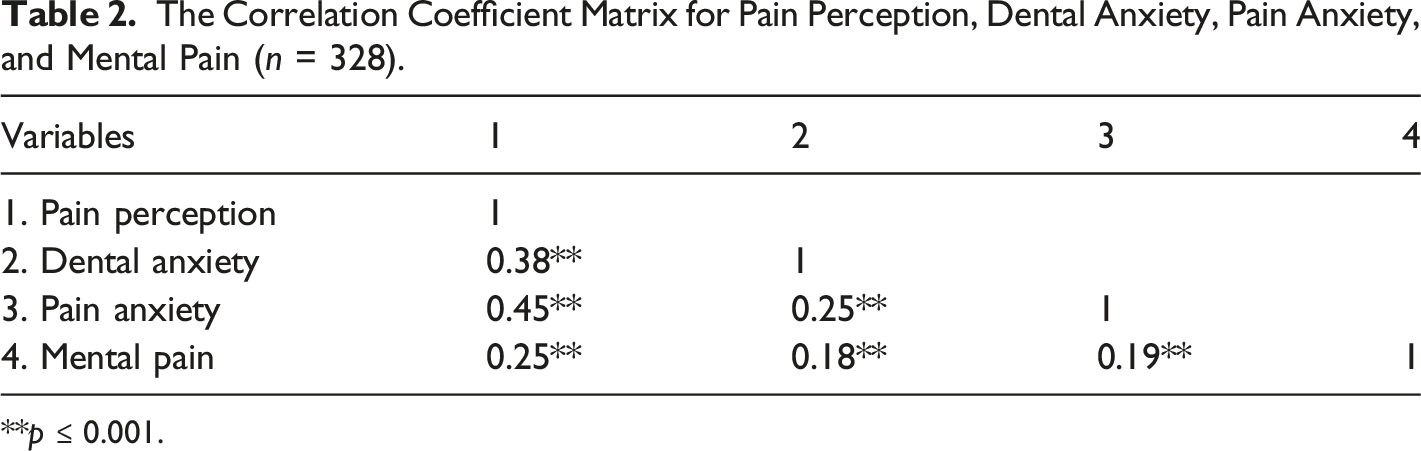
**p ≤ 0.001.
Presents the Results of Multiple Regression Analysis (Enter) to Predict Pain Perception Based on Predictor Variables (Dental Anxiety, Pain Anxiety, Mental Pain, Age, sex, Marital Status, and Education Level) (n = 328).
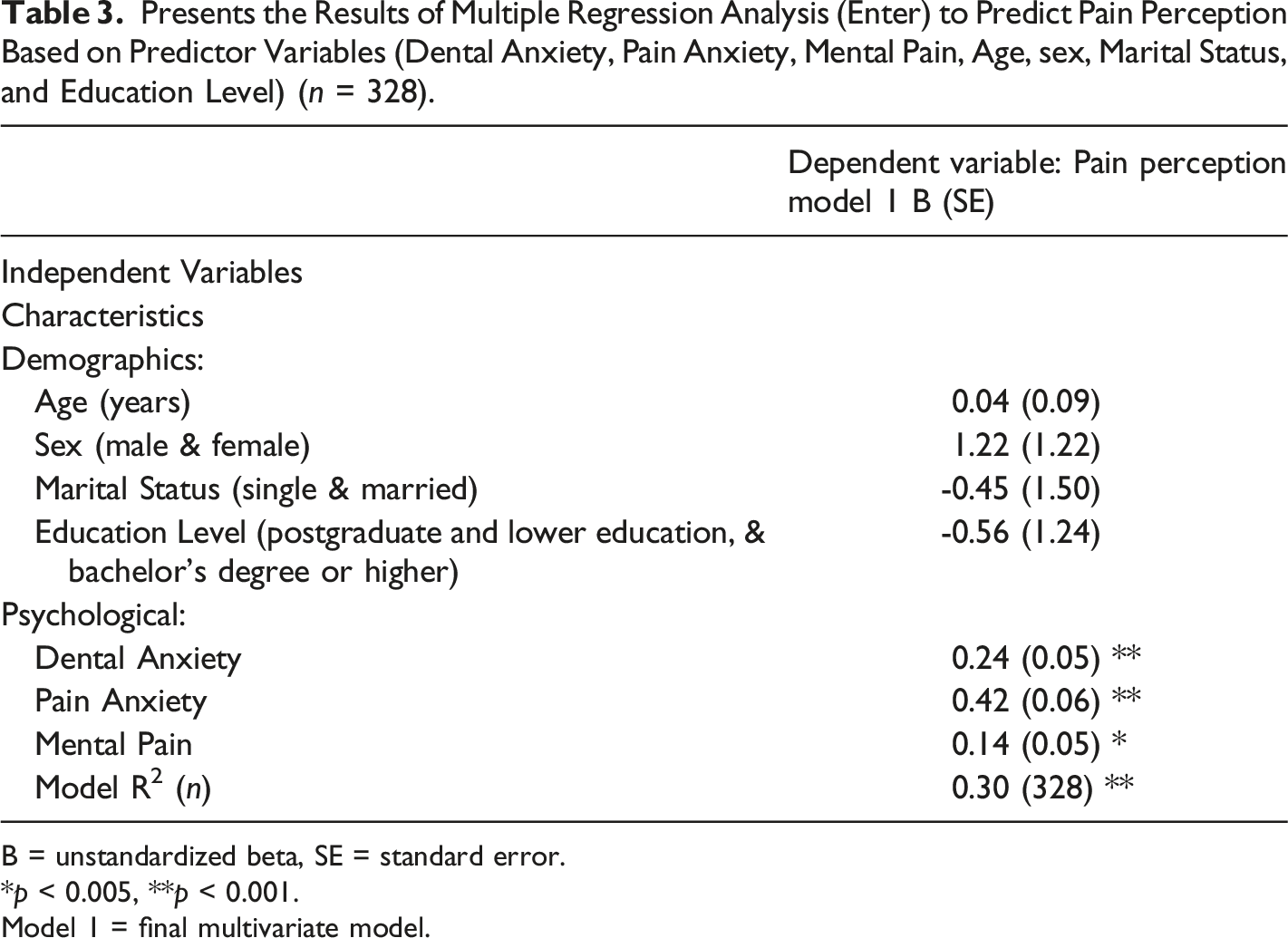
B = unstandardized beta, SE = standard error.
*p < 0.005, **p < 0.001.
Model 1 = final multivariate model.
As shown in Table 3, the Predictor variables of the study predict 30% of the variance of pain perception among patients referred to dental clinics.
Discussion
This study analyzed the relationship between the perception of dental pain and pain anxiety, mental pain, and dental anxiety in the Iranian sample. The statistical analysis revealed psychological factors correlated with pain perception, including pain anxiety, mental pain, and dental anxiety. In this study, pain anxiety showed the highest correlation with pain perception.
Various researchers have reported a relationship between psychological factors and dental pain.55,56,57 Similarly, Lamarca (2018) investigated stress, anxiety in perception, and expecting dental pain among children. The results were provided before receiving the intervention, immediately after receiving the intervention, and six months after that. These results stated that stress and anxiety do not directly affect pain perception while receiving the intervention. However, patients' anticipation of attending dental settings influences their pain perception. This result was repeated among older people as well. 58 Thus, it can be concluded that mental moods and people's attitudes toward dental intervention affect pain perception.
This research shows a relationship between pain anxiety and pain perception. In explaining the findings of this research, we can refer to a study by Carlton et al. (2009). This study examined the relationship between pain fear and anxiety sensitivity. The results showed anxiety disorders, including general and social anxiety, specific phobia disorder, panic disorder, and depressive disorder in people with chronic musculoskeletal pain. 59 It can also be considered anxiety sensitivity, fear of negative evaluation, and disease sensitivity as common elements between pain fear and other fears. 59 Predicting pain is also another important factor in anxiety and perception.
When predicting pain, a person imagines himself in a fearful situation through thoughts and mental images and makes it catastrophic.60,61 The patient becomes anxious about his pain and its aggravation in the future. This ه can be due to pain fear and overestimating the consequences of pain. Maladaptive interpretation of pain internalizes it intolerably in the patient's mind. 62 In such a situation, the patient finds a fusion with his pain. Therefore, prediction can be called an essential factor in pain anxiety. 63
Positive and negative emotions play a vital role in the experience of anxiety and depression. Studies show that people with positive emotions are less vulnerable to pain perception in anxiety-provoking situations. Therefore, it can be concluded that emotion regulation is one of the factors to adjust with pain anxiety. 64
Also, the role of mood and mental pain confirms the findings of this research. Our study showed a relationship between mental pain and pain perception, as we can refer to a study by e Raiisi et al. (2022). According to the results, mental pain plays a mediator role between pain anxiety and perception. 36 Other studies have revealed that people who suffer from depression have more complaints about pain. Regarding the vital role of emotion and mood in the perception of dental pain, the significant role of psychological factors should be considered. The part of maladaptive thoughts and interpretations can be mentioned in explaining the research findings.65,66 Patients with high mental pain and intensive anxiety see everything through the lens of pain and find themselves suffering much pain. In other words, all aspects of their life will be influenced by pain, regardless of their different personality traits.67,68 Also, patients become identified with their suffering and cannot imagine themselves without pain. In this situation, psychological interventions such as Acceptance and Commitment Therapy help people differentiate between their whole selves and their pain and do not consider the pain their entire existence.69,70
The present study’s results showed a relationship between pain anxiety and pain perception of this research. We can refer to a study by Eli et al. (2004) which examined the psychological model of patients who suffered from dental anxiety. 71 The results showed that the negative and painful experiences in a dental setting during childhood and the existence of pathological personality traits in terms of attachment styles are effective in perceiving pain. Those who reported unpleasant experiences in dental settings in childhood complained of having more anxiety in adulthood. In this study, the kind of child-parent attachment style was an essential predictor of a patient's pain in dental environments. 71 The patients with a safe attachment style reported less anxiety concerning their parents having a safer relationship with the dentist.71,72
On the other hand, the people with insecure attachment styles and feelings of ambivalence had an uneasy relationship with their dentist and suffered from more anxiety. 71 In the same conditions, the people with a safe schema in a child-parent relationship reported less anxiety than those with an insecure schema. In line with the findings of this study, it can be concluded that formed personality factors of the patient during the growing period can cause pain anxiety as a psychological pattern.71,72
Other psychological concepts related to pain perception and psychological traits, such as catastrophic pain, pain sensitivity, and low resiliency, can be mentioned.64,73 Also, the patient's interpretation of pain influences the type of pain perception. People who exaggerate the slightest pain in their teeth, and are sensitive to pain symptoms, overestimate the pain and overbear it. 17 Another critical factor in managing pain is resiliency. People with low resilience have low toleration and identify the pain as insufferable.64,74,75
According to the theoretical background of pain and psychological characteristics, it can be concluded that dental pain and pain perception do not occur only through neural pathways. Still, the psychological interpretation is effective in the intensity of pain experienced.73,76
This research helps to consider the psychological factors of the patients who avoid going to dental clinics due to pain fear, reducing patients' anxiety in dental clinics and finally perceiving less pain among them. Also, based on this research, complementary psychological interventions can be designed before and after dental services. 72
Ultimately, the results indicated the associations between the perception of dental pain and pain anxiety, mental pain, and dental anxiety. Considering the role of anxiety in dentistry, it is suggested to investigate whether dental anxiety manifests as health anxiety or refers to a specific phobia. Designing and evaluating psychoeducational packages to deal with anxiety and pain was also recommended.
The most important limitation of the current study was the lack of assessment of participants after receiving dental treatment. The researchers could not compare patients' perceptions and pain intensity before and after dental treatment. Finally, further research is proposed to study the patients’ attitudes toward receiving services and their perception of the pain after dental services.
Conclusion
Psychological factors are influential in the perception of dental pain. Therefore, psychological education about dental pain and awareness of the consequences of avoiding visiting the dentist is a priority. Further, there is a need to seriously identify people with a fear of dentistry and intervene in their psychological symptoms.
Footnotes
Acknowledgments
The authors of this article sincerely thank the Vice-Chancellor for Research and Technology of Kermanshah University of Medical Sciences and all those who participated in this research.
Author Contributions
All authors participated in the drafting of the present manuscript and its final approval. AAT: Ideation of the research subject and writing an article, AAP: corresponding authors and English edit, SR: data analyses and draft design, MJ: collecting data, YM: draft design and editing, KH: collecting data, AAF: Edit the discussion, ME, & MG: Edit the introduction.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The Vice-Chancellor for Research and Technology of Kermanshah University of Medical Sciences has financially supported this research. This article is from the approved plan with code "980,630" in Kermanshah University of Medical Sciences.
Ethical Approval
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2000. This investigation has been approved by the ethics committee of Kermanshah University of Medical Sciences (IR.KUMS.REC.1398.385).
Informed Consent
All participants completed a written informed consent form to enter the study.
Data Availability
It is possible to access the data after coordination with the corresponding author by email.