
Abstract
Objectives
High rates of post-traumatic stress disorder (PTSD) have been observed in earthquake survivors many years after the event. However, its prevalence among patients with schizophrenia is largely unknown. This study, which was conducted two years after the 2020 Elazığ earthquake, sought to identify risk factors for earthquake-related PTSD among patients with schizophrenia and healthy subjects.
Methods
Adult patients with schizophrenia (N = 103) and healthy subjects (N = 103) who had survived the earthquake were recruited from affected areas in the Eastern Anatolian Region of Turkey, Elazığ. A detailed questionnaire of earthquake-related risk factors, the Brief Coping Orientation to Problems Experienced (Brief COPE), the Multidimensional Scale of Perceived Social Support (MSPSS), and the Clinician-Administered PTSD scale for DSM-V (CAPS-5) scale were administered to participants.
Results
Twelve percent of the patients with schizophrenia and 25% of the healthy subjects had earthquake-related PTSD diagnoses two years after the 2020 Elazığ earthquake. Healthy subjects had a significantly higher rate of earthquake-related PTSD when compared to patients with schizophrenia. Religious coping, self-blaming, less emotional support seeking, and going to a safer place on the night of the earthquake were found to be associated with PTSD in patients with schizophrenia. History of traumatic events, self-blaming, and less social support from family were found to be associated with a PTSD diagnosis in healthy subjects.
Conclusions
The earthquake in Turkey created a situation such that significant symptoms of PTSD remained present at two years following the event in both patients diagnosed with schizophrenia and healthy subjects. Patients with schizophrenia have different risk factors for the development of PTSD when compared with healthy subjects. Clinical interventions should consider risk factors, coping strategies, and perceived social support when seeking to prevent earthquake-related PTSD.
Keywords
Introduction
Earthquakes are highly uncontrolled and unpredictable disasters that can cause widespread devastation. Turkey is located on the Alpine-Himalayan seismic zone, which is one of the most active seismic zones in the world, and the East Anatolian Fault Zone (EAFZ), which is one of the most important fault systems in and around Turkey. 1 An earthquake with a magnitude of 6.8 Mw and a depth of 8.6 km, reported by the Turkey Disaster and Emergency Management Presidency, occurred on January 24, 2020, at 20:55 local time in the Sivrice district of Elazığ province (latitude: 38.36 and longitude: 39.06), located in the EAFZ (according to the European-Mediterranean Seismological Center-France, it had a magnitude of 6.8 Mw, and a depth of 15.0 km). 2 Elazığ province is located in the Eastern Anatolia Region of Turkey. The epicenter of the earthquake, the village of Çevrimtaş, is located approximately 35 km southwest of the city center of Elazığ. After the first earthquake in Elazığ, on 24 January, 4322 aftershocks with magnitudes ranging from 0.8 to 5.4 Mw occurred. 30 of the aftershocks were of magnitude 4 and above. The earthquake lasted for 22 seconds. This earthquake, in which 41 people died, and 1466 people were injured, affected a wide geographical area and was felt in many surrounding cities. 3
Disasters cause short and long-term impacts on social, economic, political, physical, and psychological conditions. 4 While other problems are addressed subsequently, many of the psychological problems remain undetected. 5 Sleep disorders, anxiety, depression, and post-traumatic stress disorder (PTSD) are among the most common psychiatric disorders in earthquake survivors. PTSD can develop following exposure to actual or threatened death, serious injury, or sexual violation and is characterized by symptoms such as re-experiencing, avoidance, emotional and cognitive distortions, and hyperarousal. 6 The prevalence of PTSD following exposure to earthquakes varies in the literature. The prevalence of PTSD in survivors was found to be 49.6% two years after the Spitak earthquake in Armenia. 7 In a study conducted 20 months after the 1999 Marmara earthquake in Turkey, the prevalence of PTSD was found to be 39%. 8 Two years after the earthquake in Central Italy, the prevalence of PTSD was 21.7%. 9 This variability may be caused by the time elapsed since the disaster, the population considered, and the study design. Very little research examining the psychological impacts of earthquakes in patients with schizophrenia has been carried out compared to research on the general population. Several studies found increasing acute exacerbation rates in patients with schizophrenia after the earthquakes.10,11 There is, however, a research gap on earthquake-related PTSD in patients with schizophrenia. Despite the well-known association between PTSD and schizophrenia, to our knowledge, there has been no research on the long-term psychological effects of earthquakes in patients with schizophrenia.
Responses to disasters show striking individual variation, which may be shaped by coping strategies. Maladaptive coping strategies are associated with a greater likelihood of PTSD.12,13 Cofini et al. 14 found that individuals with PTSD scored more on religious coping, self-distraction, self-blaming, denial, venting, and behavioral disengagement after the year 2009 L’Aquila earthquake. The lower level of perceived social support is one of the most important risk factors for the onset and maintenance of PTSD symptoms. 15 In a meta-analysis of longitudinal studies, Wang et al. 16 showed that higher social support provides a buffer against the development of PTSD. In the wake of the disaster, evaluating social support and intervening to improve it could help to prevent PTSD among patients with schizophrenia. 17
Immense emotional suffering and physical devastation due to the earthquake caused a lingering effect on the mental health of the whole population. 18 Inadequate investigation of the earthquake-related PTSD symptoms in patients with schizophrenia may cause untreated PTSD and more resistant psychotic symptoms. Our aim in this study is to assess the prevalence of PTSD and its association with perceived social support, and coping strategies in patients with schizophrenia and healthy subjects two years after experiencing the 2020 Elazığ earthquake.
Methods
Participants and procedure
A descriptive, cross-sectional research design was used to evaluate the PTSD diagnosis, coping strategies, and perceived social support among the survivors of the 2020 Elazığ earthquake. In total, 103 patients diagnosed with schizophrenia and 103 adult respondents without any psychiatric diagnosis were assessed two years after the earthquake. The clinical diagnosis of schizophrenia was made by experienced psychiatrists through clinical interviews following the DSM-V criteria. 19 Patients were recruited from the outpatient clinic of Elazığ Mental Health and Disease Hospital. All of the patients with schizophrenia were in antipsychotic treatment. Data were collected from symptomatically remitted patients with schizophrenia, which were determined to comply with Andreasen's remission criteria. 20 According to this remission criteria, four core positive and four core negative symptoms on the Positive and Negative Syndrome Scale ( PANSS ) have to be no more than mild at least for 6 months.20,21 In addition, 103 adult respondents, without any psychiatric diagnosis before the interview date, who experienced the earthquake at the Elazığ city center, matched by age and sex, were recruited at the same time. Inclusion criteria were as follows: 1) 18–65 years of age; and 2) being mentally competent to answer the face-to-face interview questions. Exclusion criteria were as follows: 1) patients with dementia, mental retardation, or substance abuse; 2) history of severe head trauma, epilepsy or other neurological disorder; and 3) comorbid psychiatric disorder.
The respondents were interviewed about the 2020 Elazığ earthquake in detail. Sociodemographic characteristics and earthquake-related characteristics were assessed by clinicians using a standard interview questionnaire, which was developed by the research team specifically for this study after an extensive literature review on the earthquake, other natural disasters, and PTSD. We ascertained the respondents’ reactions immediately after the earthquake and the middle and long-term effects of the earthquake. We investigated the traumatic event history of respondents by using the Life Events Checklist for DSM-5 (LEC-5) and determined traumatic events which had been experienced personally. 22 Earthquake-related PTSD was measured using the Clinician-Administered PTSD Scale for DSM-5 (CAPS-5), a version of which was developed in Turkish.23,24
Informed verbal and written consent was obtained from respondents before the interview. The average time taken for the interview was about 90–120 min. Data were collected from January 1, 2022, to February 1, 2022. The respondents were assured of the confidentiality of their data and responses. The study was approved by the Non-Invasive Clinical Research Ethics Committee of the Faculty of Medicine, Fırat University, Elazığ, Turkey (2021/09–35).
Measurements
Information from the day of the earthquake, earthquake-related events, clinical, and sociodemographic data were collected with a detailed clinical interview. The clinical interviews were conducted by licensed psychiatrists with extensive training and experience in diagnosing and treating psychiatric disorders. During the interviews, the psychiatrists used open-ended questions and follow-up probes to elicit information about the patient’s symptoms, history, and the earthquake day. The Clinician-Administered PTSD Scale for DSM-5 (CAPS-5), Brief COPE scale, and Multidimensional Scale of Perceived Social Support (MSPSS) were used for clinical assessments.
Brief coping orientation to problems experienced
The “Coping Orientation to Problems Experienced (COPE)” scale, developed by Carver et al., 25 measures the different coping strategies that individuals exhibit for stress. Carver et al. 26 arranged a short version of the COPE scale named “Brief COPE Scale”, which is made up of 28 items, and 14 subscales. This self-report scale consists of four Likert-type questions. The Turkish validity and reliability study of the scale was conducted by Bacanlı et al. 27 Coping strategies could be analyzed under two main groups: adaptive (active coping, planning, positive reframing, use of instrumental support, use of emotional support, acceptance, religious coping, and humor) and maladaptive strategies (denial, behavioral disengagement, self-distraction, venting, substance use, and self-blame). 28
Multidimensional scale of perceived social support
The MSPSS was developed by Zimet et al., 29 and assesses three sources of perceived social support: family, friends, and significant others. This scale consists of 12 items and contains seven Likert-type questions. It contains four items for each support group. The Turkish validity and reliability study of the scale was conducted by Eker and Arkar. 30
Clinician-administered PTSD scale for DSM-5
CAPS was developed in 1989 at the National Center for PTSD. 31 CAPS was revised to correspond with PTSD criteria in the DSM-5 by Weathers et al. 24 The CAPS-5 is a 30-item structured interview that corresponds to the DSM-5 criteria for PTSD. The CAPS-5 items are evaluated in terms of intensity and frequency of symptoms and provide a single severity rating. The total symptom severity score is calculated by summing severity scores for items 1-20. Items were rated on five Likert-type questions with rating scale descriptors as “0 = absent”, “1 = mild/subthreshold”, “2 = moderate/threshold”, “3 = severe/markedly elevated”, and “4 = extreme/incapacitating”. A symptom is considered present only if the corresponding item severity score is rated 2 = moderate/threshold or higher. Criterion B (Intrusions) (items 1–5), Criterion C (avoidance) (items 6–7), Criterion D (negative alterations in mood and cognitions) (items 8–14), and Criterion E (arousal/ reactivity) (items 15–20) clusters were evaluated. A diagnosis of PTSD was made with the presence of at least one of five re-experiencing symptoms, one of two avoidance symptoms, two of seven symptoms of negative alterations in cognition, and mood, and two of six arousal symptoms for more than one month. Additionally, DSM-5 Criterion G should be met for PTSD diagnosis. Criterion G requires that the disturbance causes either clinically significant distress or functional impairment, as indicated by a rating of 2 = moderate or higher on items 23-25.32,33 The Turkish validity and reliability study of the scale was conducted by Boysan et al. 23
Statistical analysis
All statistical analyses were conducted with the IBM Statistical Package for the Social Sciences (SPSS) for Windows, version 21.0. The Kolmogorov-Smirnov test was used to determine whether the data were normally distributed. The Chi-square test was used to compare the categorical data between the two groups. The Student t-test or Mann-Whitney U test was performed to analyze the relationship between PTSD diagnosis and the sociodemographic, earthquake-related variables, social support, and coping strategies. A binominal logistic regression analysis was performed to examine the association between clinical and earthquake-related factors, and the diagnosis of PTSD. Clinical and earthquake-related factors, which were those with statistical significance in univariate analyses for both groups, were used as independent variables. The Hosmer-Lemeshow test was used for model fit. For all statistical analyses, a statistical significance level of P < .05 was used.
Results
Sociodemographic and clinical characteristics of participants
Sociodemographic and clinical characteristics of participants.
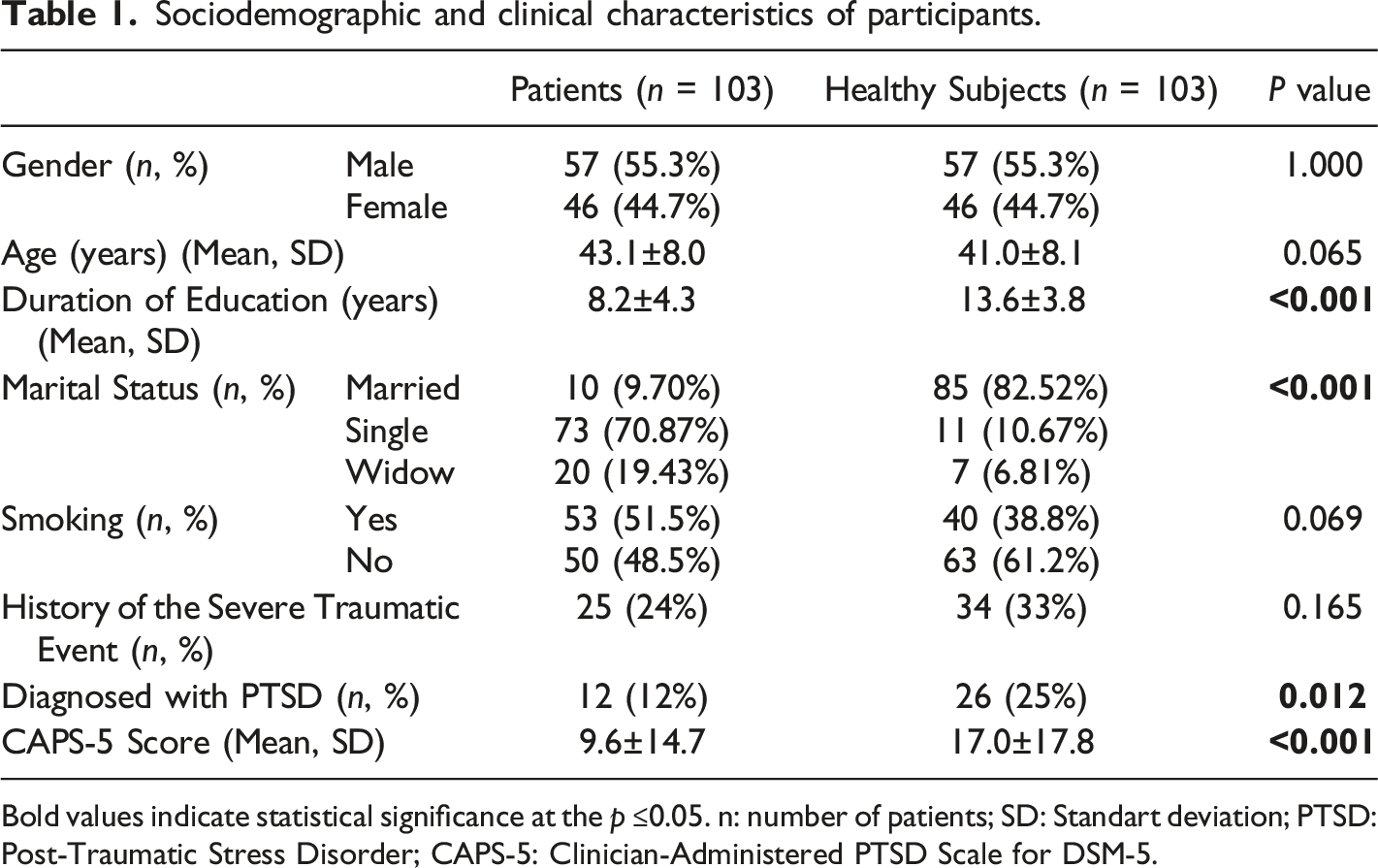
Bold values indicate statistical significance at the p ≤0.05. n: number of patients; SD: Standart deviation; PTSD:Post-Traumatic Stress Disorder; CAPS-5: Clinician-Administered PTSD Scale for DSM-5.
Earthquake-related characteristics of participants
Assessment of earthquake-related characteristics of the participants.
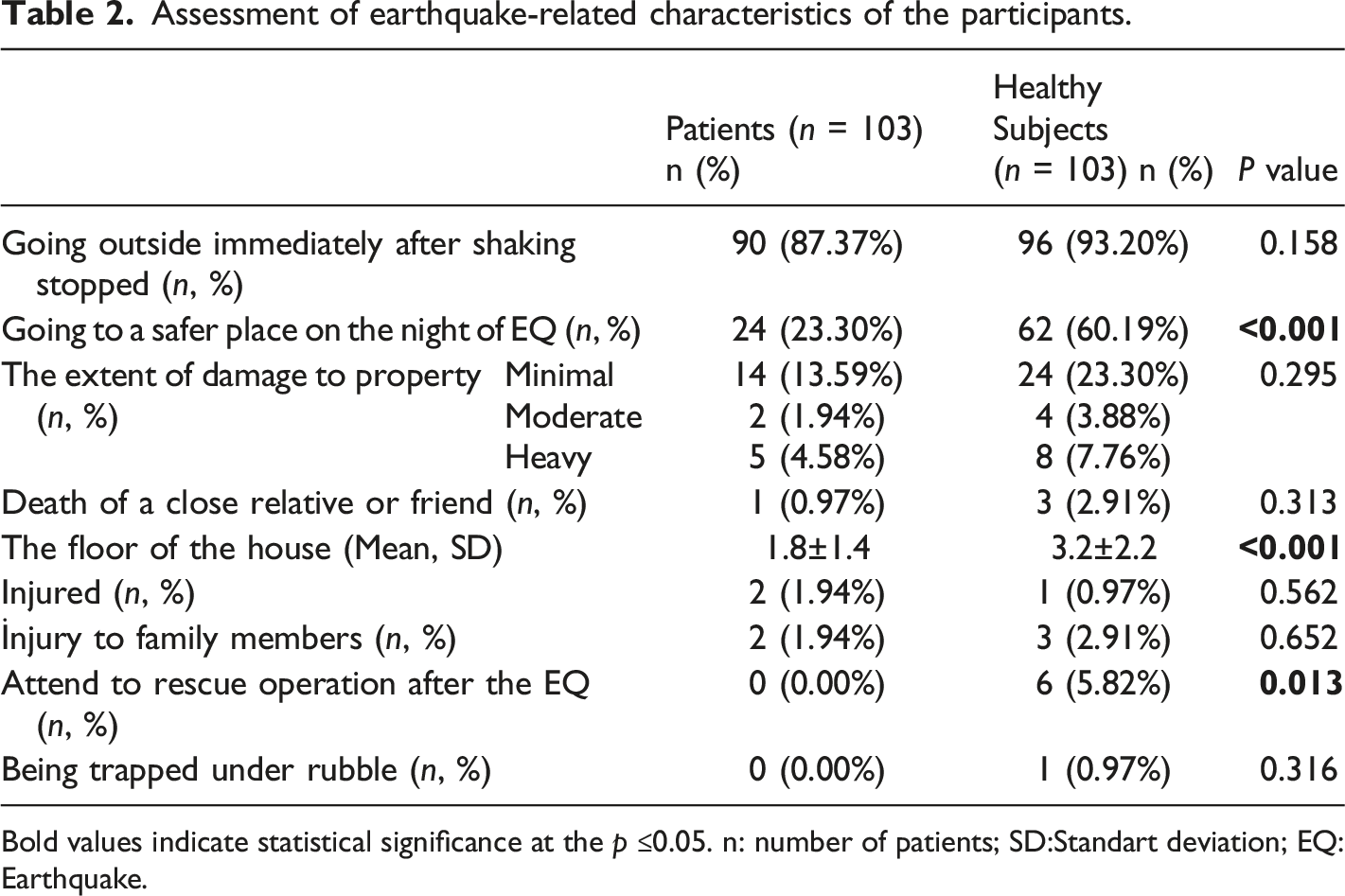
Bold values indicate statistical significance at the p ≤0.05. n: number of patients; SD:Standart deviation; EQ: Earthquake.
Assessment of coping strategies, and perceived social support of the participants
Adaptive coping styles such as active coping, planning, positive reframing, acceptance, and humor were significantly more common in healthy subjects (p < 0.001). As regards maladaptive coping styles, while disengagement was significantly more common in patients with schizophrenia, self-blaming, and venting were significantly more common in healthy subjects (P < .001). Perceived social support from family, friends, and significant others were significantly lower in patients with schizophrenia (p < 0.001).
The association of social supports and coping strategies with PTSD diagnosis
Association of PTSD with adaptive coping strategies.
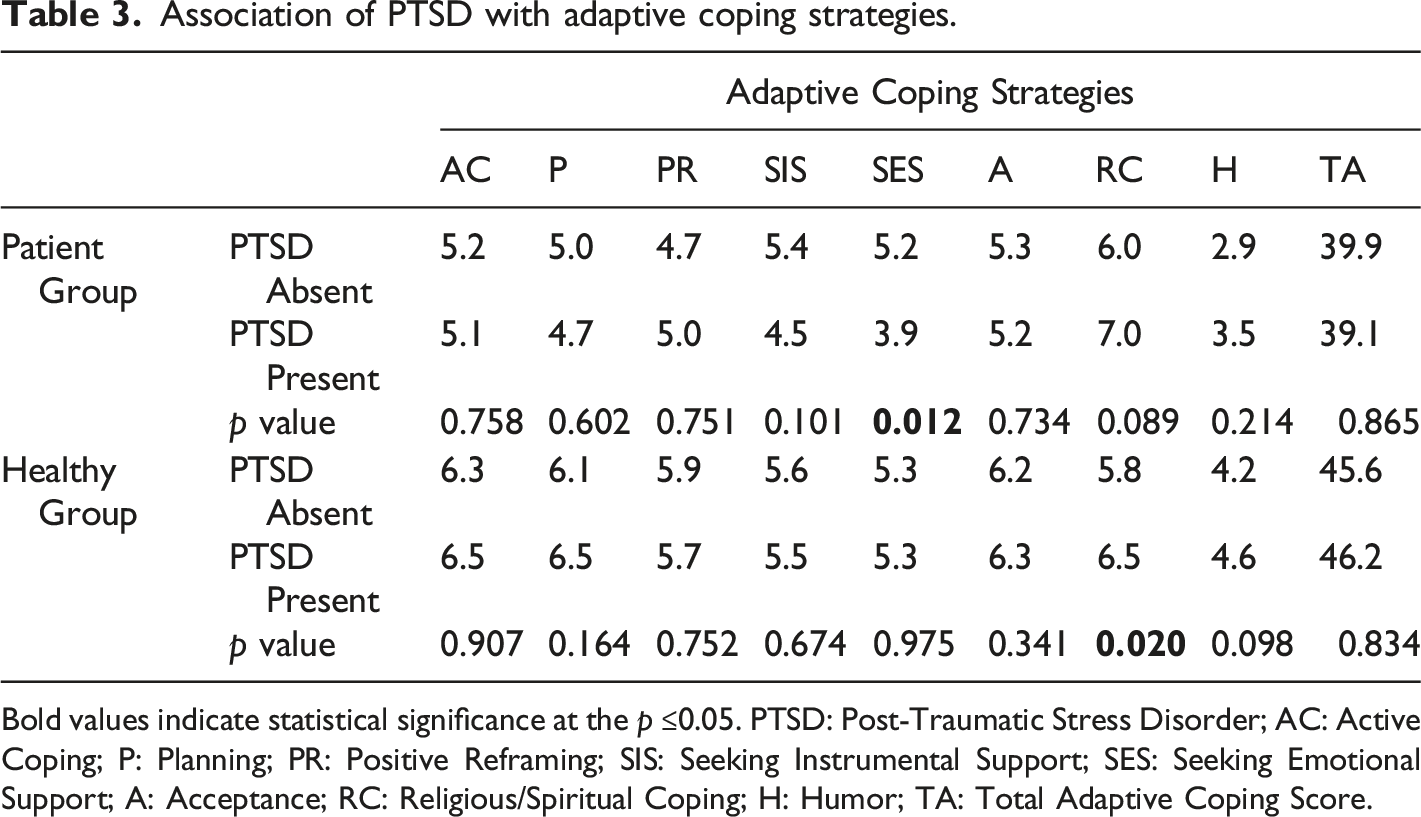
Bold values indicate statistical significance at the p ≤0.05. PTSD: Post-Traumatic Stress Disorder; AC: Active Coping; P: Planning; PR: Positive Reframing; SIS: Seeking Instrumental Support; SES: Seeking Emotional Support; A: Acceptance; RC: Religious/Spiritual Coping; H: Humor; TA: Total Adaptive Coping Score.
Association of PTSD with maladaptive coping strategies.
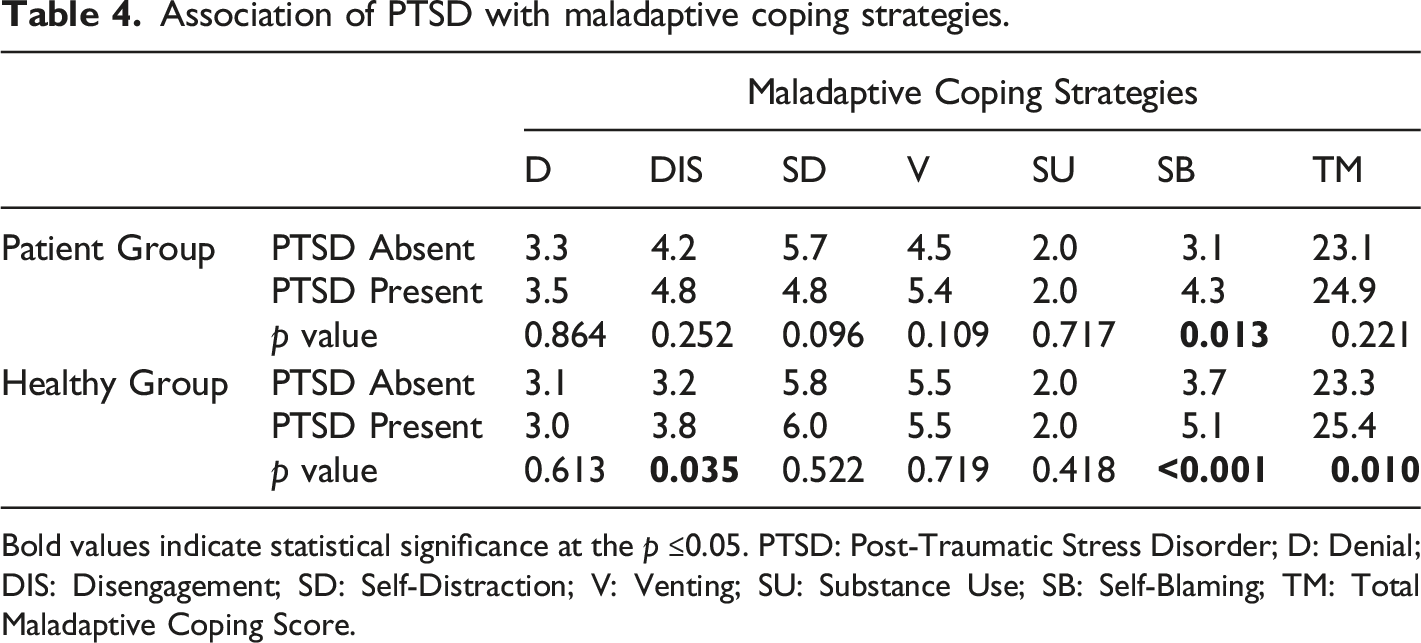
Bold values indicate statistical significance at the p ≤0.05. PTSD: Post-Traumatic Stress Disorder; D: Denial; DIS: Disengagement; SD: Self-Distraction; V: Venting; SU: Substance Use; SB: Self-Blaming; TM: Total Maladaptive Coping Score.
Association of PTSD with social support.
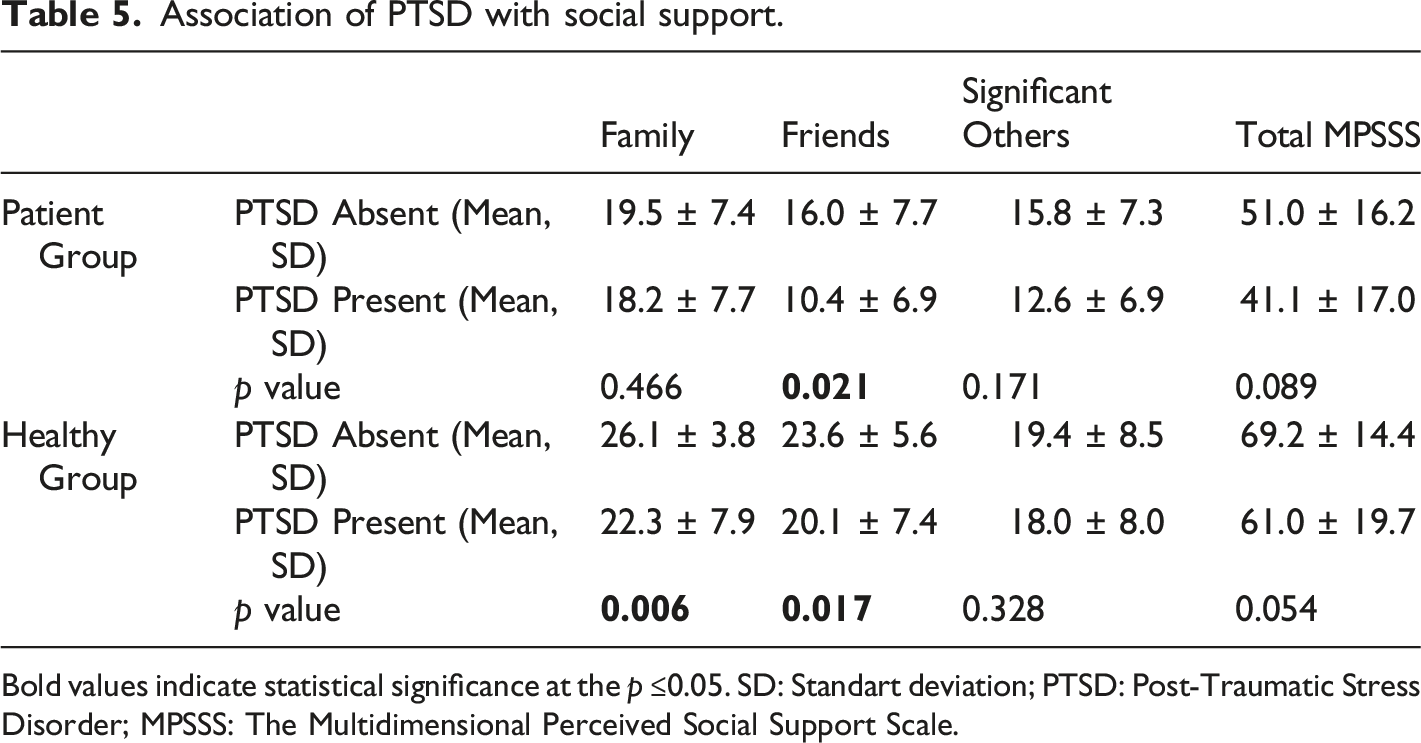
Bold values indicate statistical significance at the p ≤0.05. SD: Standart deviation; PTSD: Post-Traumatic Stress Disorder; MPSSS: The Multidimensional Perceived Social Support Scale.
The association of PTSD with sociodemographic factors and earthquake-related factors
The association of PTSD with gender, history of traumatic events, the floor of the house, going to a safer place on the night of the earthquake, going outside immediately after the shaking stopped, and the extent of damage to property within both groups were evaluated. Being female and having a history of traumatic events were significantly higher in the PTSD-present group among healthy subjects (P = .045, P < .001). Going to a safer place on the night after the earthquake and getting caught on the higher floors of a building were significantly higher in the PTSD-present group among patients with schizophrenia (P = .009, P = .002). There was no difference regarding PTSD diagnosis between male patients with schizophrenia and male healthy subjects (P = .281). Female healthy subjects have a significantly higher PTSD risk when compared with female patients with schizophrenia (P = .015).
The association between clinical variables and diagnosis of PTSD with logistic regression analysis
Determination of variables associated with a PTSD diagnosis in patients with schizophrenia using logistic regression analysis.
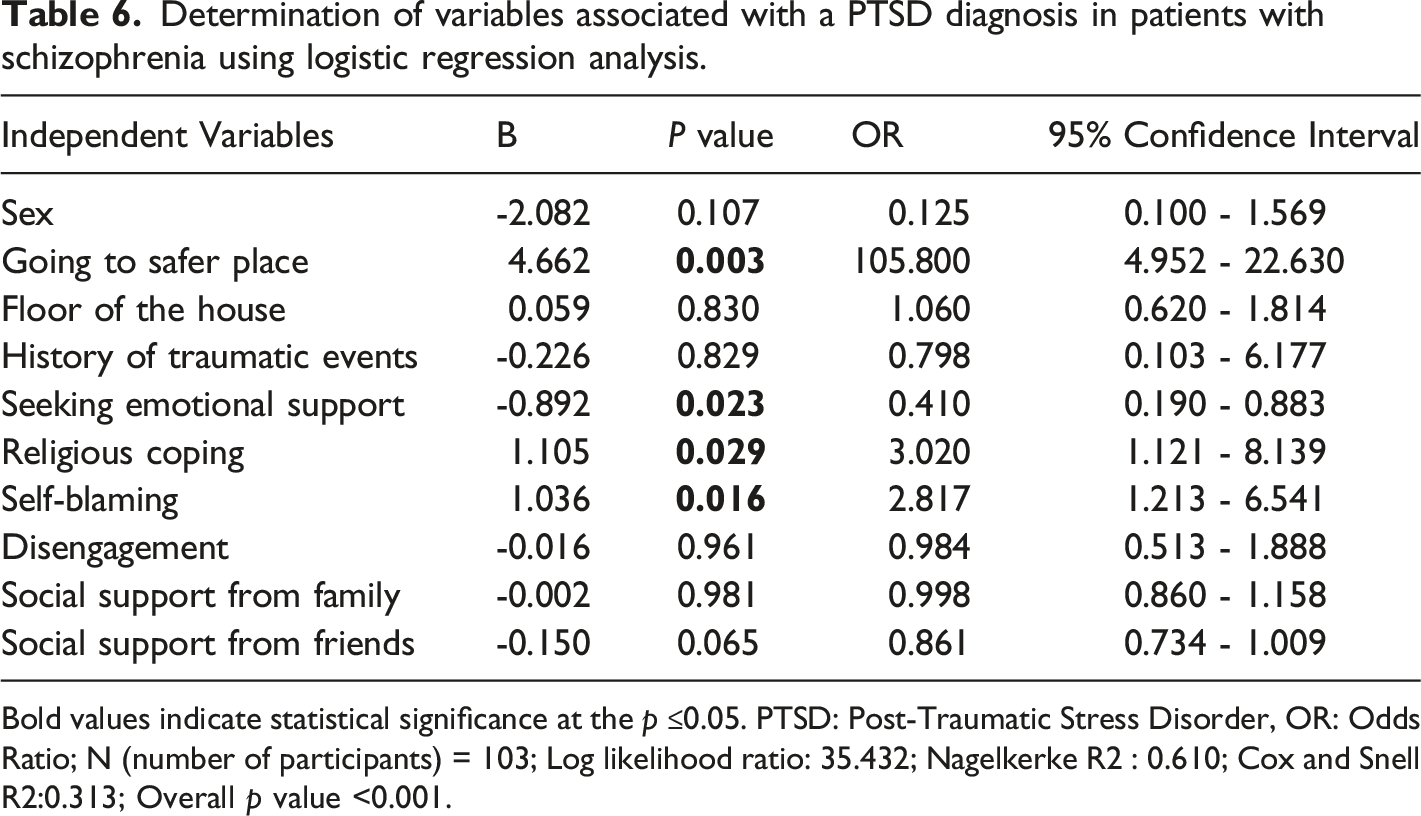
Bold values indicate statistical significance at the p ≤0.05. PTSD: Post-Traumatic Stress Disorder, OR: Odds Ratio; N (number of participants) = 103; Log likelihood ratio: 35.432; Nagelkerke R2 : 0.610; Cox and Snell R2:0.313; Overall p value <0.001.
Determination of variables associated with a PTSD diagnosis in healthy subjects using logistic regression analysis.
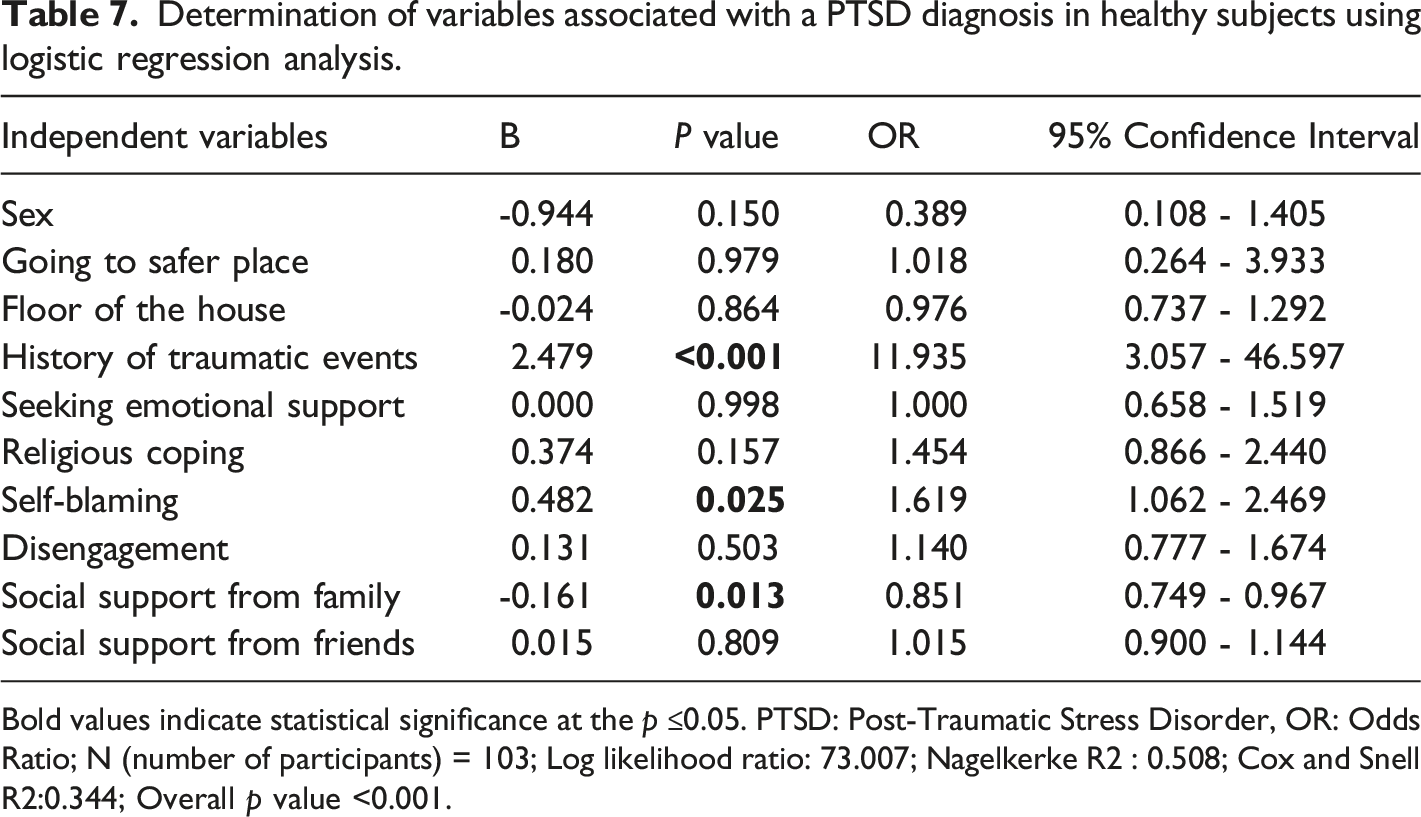
Bold values indicate statistical significance at the p ≤0.05. PTSD: Post-Traumatic Stress Disorder, OR: Odds Ratio; N (number of participants) = 103; Log likelihood ratio: 73.007; Nagelkerke R2 : 0.508; Cox and Snell R2:0.344; Overall p value <0.001.
Discussion
This study examined the prevalence of PTSD and the risk factors related to PTSD two years after the 2020 Elazığ earthquake in patients with schizophrenia and healthy subjects. One of the primary findings of this study was that PTSD symptoms experienced by survivors may persist even two years after the earthquake. We found that 25% of the healthy subjects and 12% of the patients with schizophrenia had earthquake-related PTSD diagnoses two years after the 2020 Elazığ earthquake. Healthy subjects had a significantly higher rate of earthquake-related PTSD diagnosis when compared with patients with schizophrenia. In literature, studies conducted after two years since the earthquake found a 21%-65% PTSD prevalence among healthy adults.7,34,35 The PTSD prevalence rate and CAPS-5 score were significantly lower in patients with schizophrenia when compared with healthy subjects. These findings could be attributed to the fact that we only included patients with schizophrenia who had been in remission for at least six months. Pollice et al. 36 found 17% earthquake-related PTSD prevalence among 54 patients with schizophrenia, who were hospitalized within the eight months after the 2009 L'aquila earthquake. We designed a study with patients with schizophrenia who had been in this six-month period of remission to avoid confounding effects of psychotic episodes, which might occur if they had been hospitalized soon afterward. In a systematic review, PTSD comorbidity was found to be associated with higher levels of positive symptoms, general psychopathology, and worse functioning. 37 Tseng et al. showed a 21.6% increase in hospitalization incidence for schizophrenia two years after the earthquake. 38 Taking into consideration the increased risk of hospitalization after the earthquake and higher symptomatology related to PTSD comorbidity, we discounted some patients with schizophrenia, who did not meet our remission criteria. Thus, we suggest that clinicians should investigate earthquake-related PTSD symptoms for at least two years after the earthquake in patients with schizophrenia.
Healthy subjects had a significantly higher rate of going to a safer place on the night of the earthquake. It was winter at the time of the 2020 Elazığ earthquake and the temperature was about minus 4 centigrade on the night that it happened. There were 4322 aftershocks with magnitudes ranging from 0.8 to 5.4 occurred and 30 of them were of magnitude 4 and above. People generally preferred to spend the night of the earthquake in their cars and in safer cities far from the earthquake epicenter. However, 77% of patients with schizophrenia were not able to find an alternative solution and spent the night in their homes. In the first 24 hours after the main shock, large aftershocks that cause secondary disasters and more casualties are highly probable in and around the focal area. 39 Going to a safer place on the night of an earthquake may be critical for survival due to the risk of a building collapsing with aftershocks. Patients with schizophrenia have disadvantages such as lower social support, a lower economic situation, and lower active coping and planning skills in terms of understanding how best to act during and immediately after the earthquake. Drills and training programs should be organized to raise awareness of the risks and how to stay safe, especially in high-risk seismic zones. 40 Besides that, earthquake assembly areas should be designated where people can gather to be better protected from secondary disasters. 41 Disadvantageous groups of society, such as patients with schizophrenia, should receive more frequent and specific training to give them the individual skills they need to react appropriately during and immediately after an earthquake.
We found that higher self-blaming scores were associated with a PTSD diagnosis in healthy subjects, while higher self-blaming and religious coping, and lower seeking for emotional support scores were associated with a PTSD diagnosis for patients with schizophrenia. These results are more consistent with prior research conducted among the general population, among which religious coping, self-distraction, self-blaming, substance use, denial, and venting were more common in earthquake-related PTSD compared with those who did not have PTSD.14,42 According to our results, providing emotional support may have a protective effect on earthquake-related PTSD for patients with schizophrenia. Mattson et al. 43 showed that coping-oriented clinical intervention has the potential to reduce PTSD symptoms. Taken together, as coping strategies can be modified, coping-oriented interventions may prevent chronic PTSD.
Lower social support from family was associated with PTSD diagnosis for healthy subjects. Within the schizophrenia group, individuals with PTSD had lower scores in social support from friends when compared with those who did not have PTSD. A higher perception of social support protects against the development of PTSD after the earthquake.44-46 In accordance with the literature, our study showed greater social support reduces the risk of the development of PTSD after the earthquake. Although social support is such a strong negative correlate of earthquake-related PTSD, the prevalence of earthquake-related PTSD was lower in those with schizophrenia. This may be attributed to the fact that we only included patients with schizophrenia who had been remitted for at least six months and patients with schizophrenia who were on antipsychotic treatment, which may have a protective effect against PTSD development. 47 More research would be needed to fully understand the complex relationships between social support, individual characteristics, and the development of PTSD in patients with schizophrenia.
Being female was a significantly higher factor in the PTSD-present group among healthy subjects. Although a significant result was obtained in univariate analysis, no relationship was found in the regression analysis. Being female has been shown as a risk factor for earthquake-related PTSD.48-50 There was no difference in PTSD diagnosis in terms of gender among patients with schizophrenia. We could not show a relationship between gender and PTSD diagnosis for both groups. However, when the current limitations of this study and the results of other studies are evaluated together, gender differences in terms of PTSD diagnosis in patients with schizophrenia and healthy subjects should be investigated in further research. The existence of traumatic event history was significantly higher in the PTSD-present group among healthy subjects and was associated with PTSD diagnosis in healthy subjects. Breslau et al. 51 showed that previous exposure to trauma signals a greater risk for the development of PTSD. Lowe et al. 52 showed that a history of traumatic events related to a higher risk for PTSD. Our findings suggest that the existence of traumatic event history causes no significant change in terms of PTSD diagnosis in patients with schizophrenia while increasing the risk of developing PTSD in healthy subjects. Going to a safer place on the night after the earthquake and getting caught on the higher floors of a building were significantly higher in the PTSD-present group among patients with schizophrenia. Going to a safer place on the night of the earthquake was found associated with PTSD diagnosis in the schizophrenia group. Going to a safer place on the night of the earthquake protects survivors from secondary disasters due to aftershocks, but it also seems related to the increased risk of the development of PTSD in patients with schizophrenia. This may be attributed to an increased fear response during the earthquake, which was shown as a predictor of earthquake-related PTSD. 48 We have thoroughly studied the literature and have not found research on earthquake-related PTSD in patients with schizophrenia. Trauma and PTSD are underreported among patients with schizophrenia. 53 PTSD may be underdiagnosed in patients with schizophrenia due to negative symptoms, cognitive impairment, and diminished capacity for self-expression. Clinicians should rigorously investigate PTSD symptoms among patients with schizophrenia, especially in high seismic risk zones.
Study limitations
This was a cross-sectional study, in a convenience sample, and with a limited number of participants. We only included patients with schizophrenia who had been clinically remitted for at least six months. Therefore, our sample does not represent all survivors with schizophrenia of the 2020 Elazığ earthquake. All of the patients with schizophrenia were on pharmacological treatment at the time of the interview. Atypical antipsychotics are effective in PTSD treatment, especially in terms of adjunctive utilization. 54 The NICE guideline pointed out the potential role of atypical antipsychotics in the treatment of PTSD. 47 Psychotropic medications may be a potential confounding factor, and the results may have been influenced by it. This study was conducted in the Elazığ city center, which is 35 km away from the epicenter, and data collection only lasted for four weeks, therefore it did not take into account survivors from other areas, nor data could have been obtained over a longer period.
Conclusion
In conclusion, the psychological impact of an earthquake may persist even years afterward, both in patients with schizophrenia and healthy subjects. Patients with schizophrenia may have different risk factors for the development of PTSD when compared with healthy subjects. Religious coping, self-blaming, less emotional support seeking, and going to a safer place on the night of the earthquake were found to be associated with a PTSD diagnosis in patients with schizophrenia. History of traumatic events, self-blaming, and less social support from family were found to be associated with a PTSD diagnosis in healthy subjects. The results of this study underscore the long-term psychological impact of earthquakes in patients with schizophrenia and suggest the need for interventions by taking into account coping strategies, social support, and other possible risk factors.
Footnotes
Acknowledgements
We would like to thank and acknowledge the contribution of the research participants, treatment centre and staff.
Author contributions
The authors of this study, ABT, MHÖ, HK, and SA, have all made substantial contributions that justify their inclusion as co-authors. ABT contributed to the conception and design of the work, as well as the acquisition, analysis, and interpretation of data. MHÖ played a crucial role in the study's conception and design, as well as the acquisition, analysis, and interpretation of data. HK contributed to the conception and design of the study, as well as the acquisition of data. SA made substantial contributions to the study's conception and design, as well as the acquisition of data. They also contributed to the drafting and critical revision of the manuscript. All authors have given their final approval for publication and agreed to be accountable for the work's integrity.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by the Non-Invasive Clinical Research Ethics Committee of the Faculty of Medicine, Fırat University, Elazığ, Turkey (2021/09–35).