
Abstract
Objective
The aim of this study was to compare the effects of transdiagnostic therapy compared to progressive muscle relaxation (PMR) on emotion regulation strategies, self-compassion, maternal role adaptation, and social and work adjustment in mothers of premature infants.
Materials and methods
This was a randomized controlled trial with two groups and pre-test, post-test, and a two-month follow-up assessment. Included were 27 mothers randomly assigned to either the transdiagnostic therapy group or the PMR group (13 in the transdiagnostic group and 14 in the PMR group). The experimental group received eight sessions of transdiagnostic therapy while the control group received eight sessions of PMR. The participants completed the following scales: Emotion Regulation Questionnaire, Self-Compassion Scale, Maternal Role Adaptation Scale, and Work and Social Adjustment Scale.
Results
Transdiagnostic therapy was significantly more effective than PMR in improving emotion regulation strategies, self-compassion, maternal role adaptation, and social and work adjustment based on the between-group comparison conducted at post-test and follow-up (p < 0.01).
Conclusion
Transdiagnostic therapy was shown to be effective in improving the emotional health of mothers with premature infants and was more effective than PMR techniques.
Keywords
Introduction
A premature or pre-term infant is one born before the 37th week of pregnancy. 1 Every year, 15 million premature infants are given birth. 2 The prevalence of pre-term birth in Iran ranges between 5.6% to 39.4%. 3 Premature newborns are hospitalized in Neonatal Intensive Care Units (NICU),4,5 whose atmosphere could affect the family 6 and the main caregiver (the mother). 7 Hospitalization of the infant in NICU is a stressful situation for the parents of premature infants; the members undergo negative emotions such as sadness and anxiety which can disrupt their emotion regulation strategies. 8 Emotion regulation moderates the response to emotion in a variety of ways. 9
On the other hand, the birth of a premature infant can interrupt maternal roles and increase mothers’ self-criticism in terms of caregiving. 10 Women who fail to adapt themselves with their role as a mother, experience reductions in functions. 11 Breines and Chen (2012) concluded that self-compassion can improve functionality through motivation. 12 In addition, according to Mercer’s theory, a mother whose newborn is hospitalized in NICU, would have a limited time to interact with the infants. 13
At the beginning of hospitalization, the parents of premature infants are forced to manage the obstacles by which their emotional experiences are affected. 14 The significant factors regarding the effects of NICU on the parents of premature infant's adjustment include low education and previous stressful experiences.15,16 Moreover, the unavailability of sufficient facilities could hinder adaptation and participation. 17 In this regard, time management problems, organizing caregiving to the infants, and financial matters of the family, could challenge the parents of premature infants. 18
According to what has been mentioned, it seems essential to conduct suitable interventions to improve mental health and adaptability for parents of premature infants. The interventions whose effectiveness on improving the psychological symptoms of parents of premature infants have been assessed include supportive interventions and various psychological treatments such as problem-solving-approach-based Counselling, 19 mindfulness, 20 Cognitive Behavioral Therapy (CBT) and Acceptance and Commitment Therapy (ACT), 21 stress management using relaxation techniques 22 all of which have focused on specific aspects of the psychological problems.
However, recently, considerable attention has been drawn to the transdiagnostic approach in various populations, in which mutual components in the development and continuation of psychological disorders are emphasized. 23 The unified transdiagnostic protocol is an intervention derived from CBT that focuses on emotions, targeting negative emotions and reacting to them. In this treatment, the clients become educated about adaptive emotion regulation strategies. 24 In transdiagnostic treatment, emotion regulation is known as a mutual factor linked with psychological pathology.25,26 Barlow et al. (2011) designed an integrative protocol for the transdiagnostic therapy of emotional disorders. 27 This therapeutic method emphasizes the adaptable and functional nature of emotions and increases awareness of the role of cognitions, emotions, bodily sensations, and behaviors. 28
In addition, according to Bastable (2003), relaxation is another non-medical intervention that may have potentially reduced effects on anxiety. 29 Therefore, the current study aims to determine and compare the effectiveness of transdiagnostic therapy with PMR techniques on emotion regulation strategies, self-compassion, maternal role adaptation, and social and work adjustment in mothers of premature infants.
There is a significant difference between the effectiveness of transdiagnostic therapy with PMR techniques on emotion regulation strategies, self-compassion, maternal role adaptation, and social and work adjustment in mothers of premature infants.
Methods
Study Design
The current study is a randomized controlled clinical trial with two groups and pre-test, post-test, and a two-month follow-up assessment.
Research Population
All mothers whose infants were hospitalized in NICU of all hospitals affiliated with Shiraz University of Medical Sciences during the first six months of the year 2021.
Sampling Method and Sample size
The sample size in the present study was obtained based on the mean and standard deviation of negative emotion in Hooman et al. 30 research and according to β = 0.20 and α = 0.05. Then, a minimum sample size of 14 people was obtained for each group.
Using available sampling, 83 individuals were selected out of all mothers who had been referred to the hospitals affiliated with Shiraz University of Medical Sciences within the first half of the year 2021. Of these, 53 participants were excluded from the study (Not meeting inclusion criteria (n = 29), Declined to participate (n = 11), and other reasons (n = 16)). Afterward, 27 participants (13 people in the transdiagnostic group and 14 people in the PMR techniques group) entered the research process according to the research criteria. Finally, the participants were assigned to transdiagnostic treatment groups and PMR techniques based on the random block method (Figure 1). The participants completed the questionnaires and scales before the interventions, at the end of the interventions, and two months after the termination of the sessions (follow-up). Sampling flowchart in research (n = 27).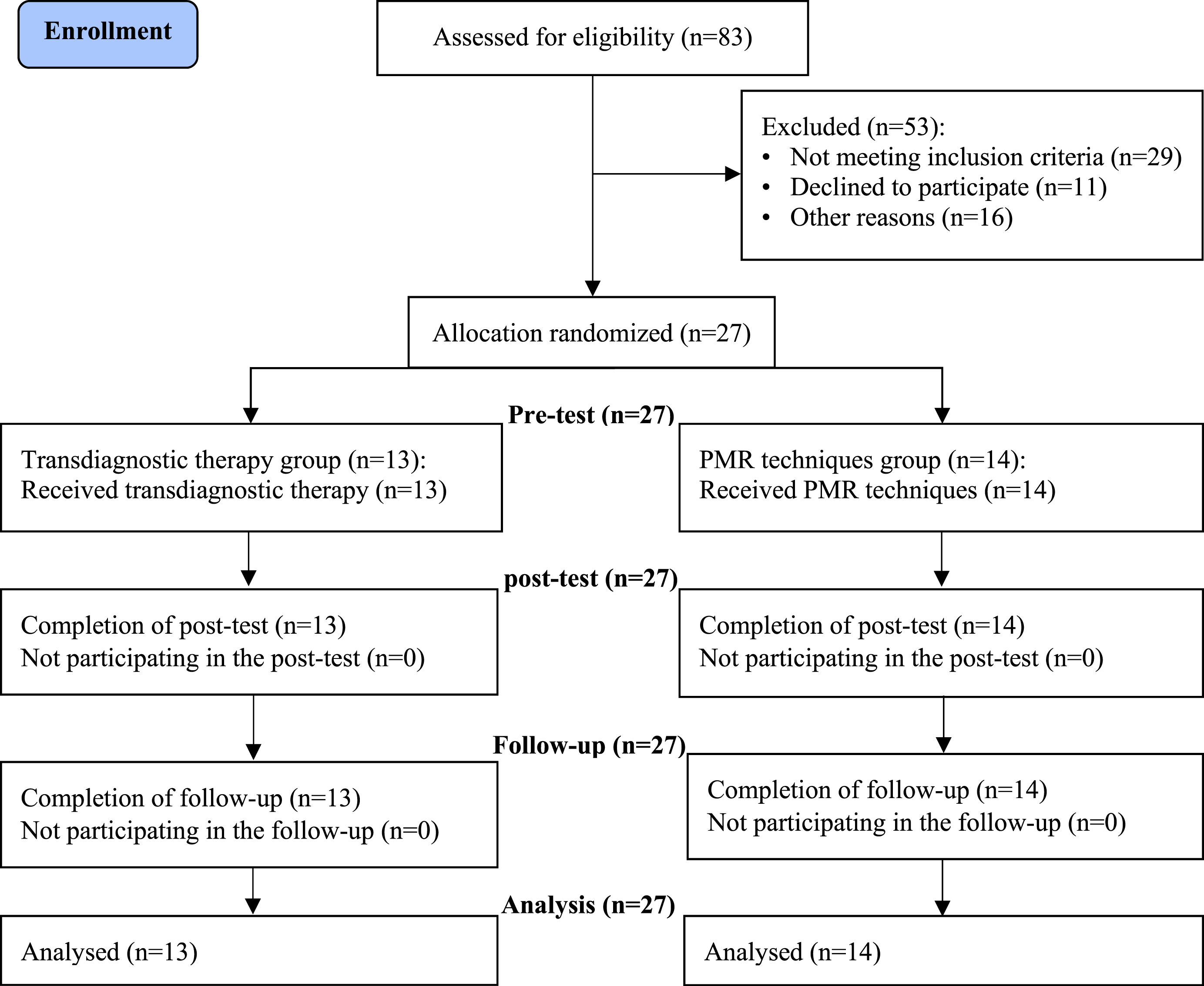
Inclusion Criteria for the Mothers
Giving informed consent for participating in the investigation; mother of a live, premature infant who has been admitted to the NICU for more than one week; not being simultaneously hospitalized; no history of drug, alcohol, or psychedelics abuse, not being diagnosed with chronic psychological or personality disorders; being able to read and write; not receiving concurrent psychological services; No cognitive problems (memory, concentration, etc.).
Exclusion Criteria
Not completing the questionnaires properly; having strong thoughts of suicide or attempting to commit it; and lack of interest in continuing the research process.
Procedure
First, the necessary permits were obtained. Afterward, mothers with newborns hospitalized in NICUs were informed of the study aims and the primary assessments regarding the inclusion criteria were carried out by an independent evaluator (a Master’s student of clinical psychology). The mothers who met the inclusion criteria and gave written informed consent were employed in the research. The participants in the experimental and control groups received transdiagnostic therapy (individual) and Compact Disks (CD) of PMR techniques (individual) respectively. The participants in the experimental group received the intended treatment in person. But the participants in the control group communicated with the therapists if needed after receiving the desired CD and completing each session. The interventions used in the present study were performed by two clinical psychologists (Ph.D).
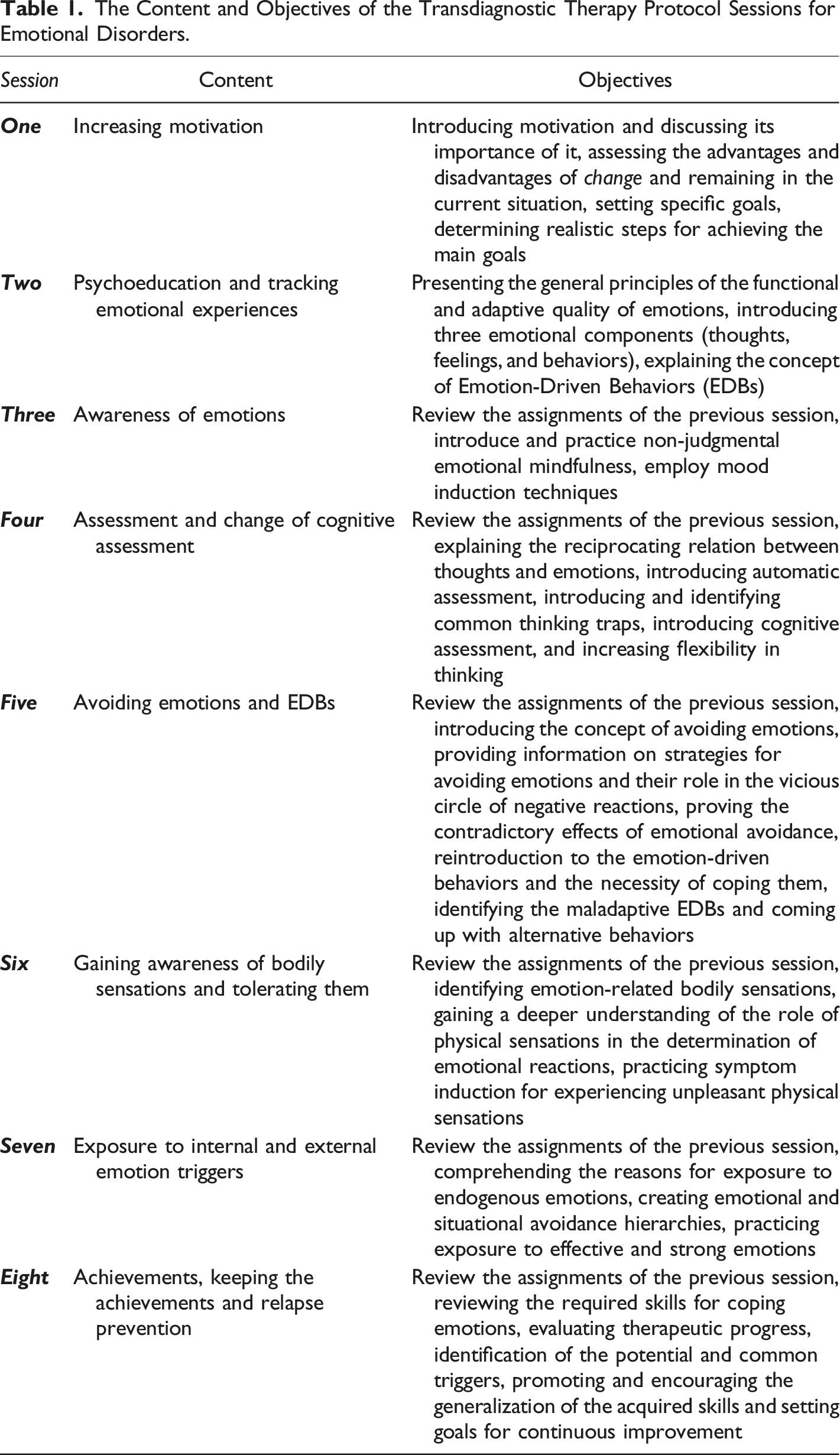
The Unified Protocol for Transdiagnostic Therapy of Emotional Disorders (UP)
The Content and Objectives of the Transdiagnostic Therapy Protocol Sessions for Emotional Disorders.
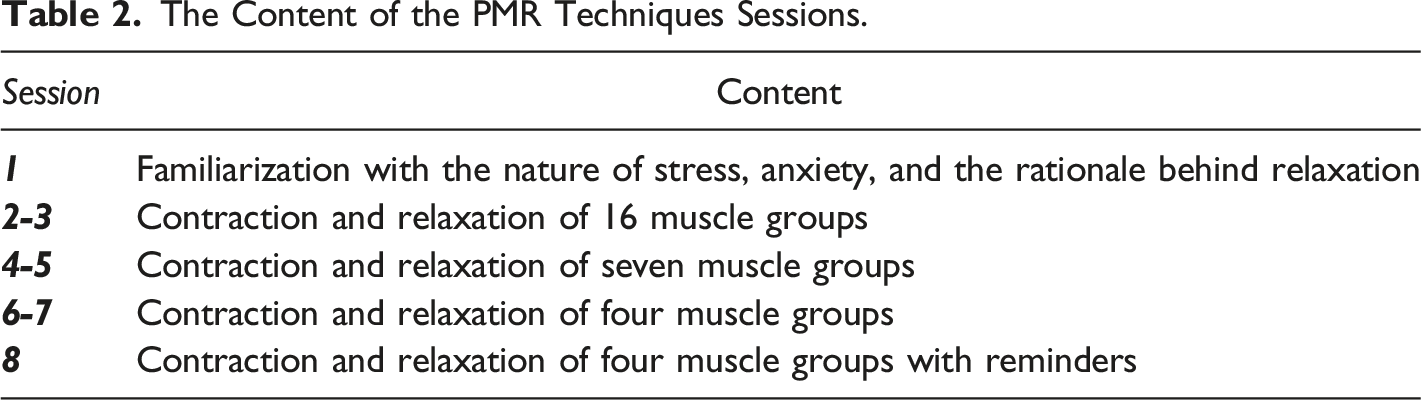
Guidance on PMR Techniques
Measurement Tools
Demographic Information Form
This researcher-made questionnaire item is regarding the age, education, and socio-economic status of the mothers and the duration of hospitalization for the newborns.
Emotion Regulation Questionnaire (ERQ)
Designed by Gross and John (2003), this scale consists of 10 items that examine emotion regulation strategies namely cognitive reappraisal (six items) and suppression (four items). All items are scored on a seven-point Likert scale from 1 = strongly disagree to 7 = strongly agree. 33 The psychometric properties of this instrument have been studied and confirmed in previous investigations.33,34
Self-Compassion Scale (SCS)
Developed by Neff (2003), this 26-item instrument is scored on a Likert scale of five points (from 1 = almost never to 5 = almost always). This scale evaluates three dual components. 35 The psychometric properties of this scale have been studied and confirmed in previous investigations.35,36
Maternal Role Adaptation Questionnaire
Consisting of 32 items, this scale was compiled by Heydarpour et al. (2016). The scores for all items are determined on a five-point Likert scale (1 = strongly disagree to 5 = strongly agree). the intra-cluster correlation of 0.81 and Cronbach’s alpha for this questionnaire is 0.77 in the population of mothers with premature infants. 37
Work and Social Adjustment Scale (WSAS)
The work and Social Adjustment Scale was created by Mundt et al. (2002). This scale includes five items and aims to examine functional impairments. The items are scored on a nine-point Likert scale from 0 = no impairment to 8 = severe impairment. A lower score indicates a more appropriate adaptation. 38 The psychometric properties of this scale have been studied and confirmed in previous investigations.30,38
Data Analysis
SPSS-25 was utilized in order to analyze the collected data. To examine the descriptive and demographic data in the current investigation, descriptive indexes, the Chi-square test, Fisher’s exact test, and independent T-test were performed. Moreover, to evaluate the hypothesis research, multivariate analysis of covariance (MANCOVA), and univariate analysis of covariance (ANCOVA) were used. The results were analyzed at a significance level of 0.95.
Results
Baseline Characteristics of Intervention and Active Control Group (n = 27).
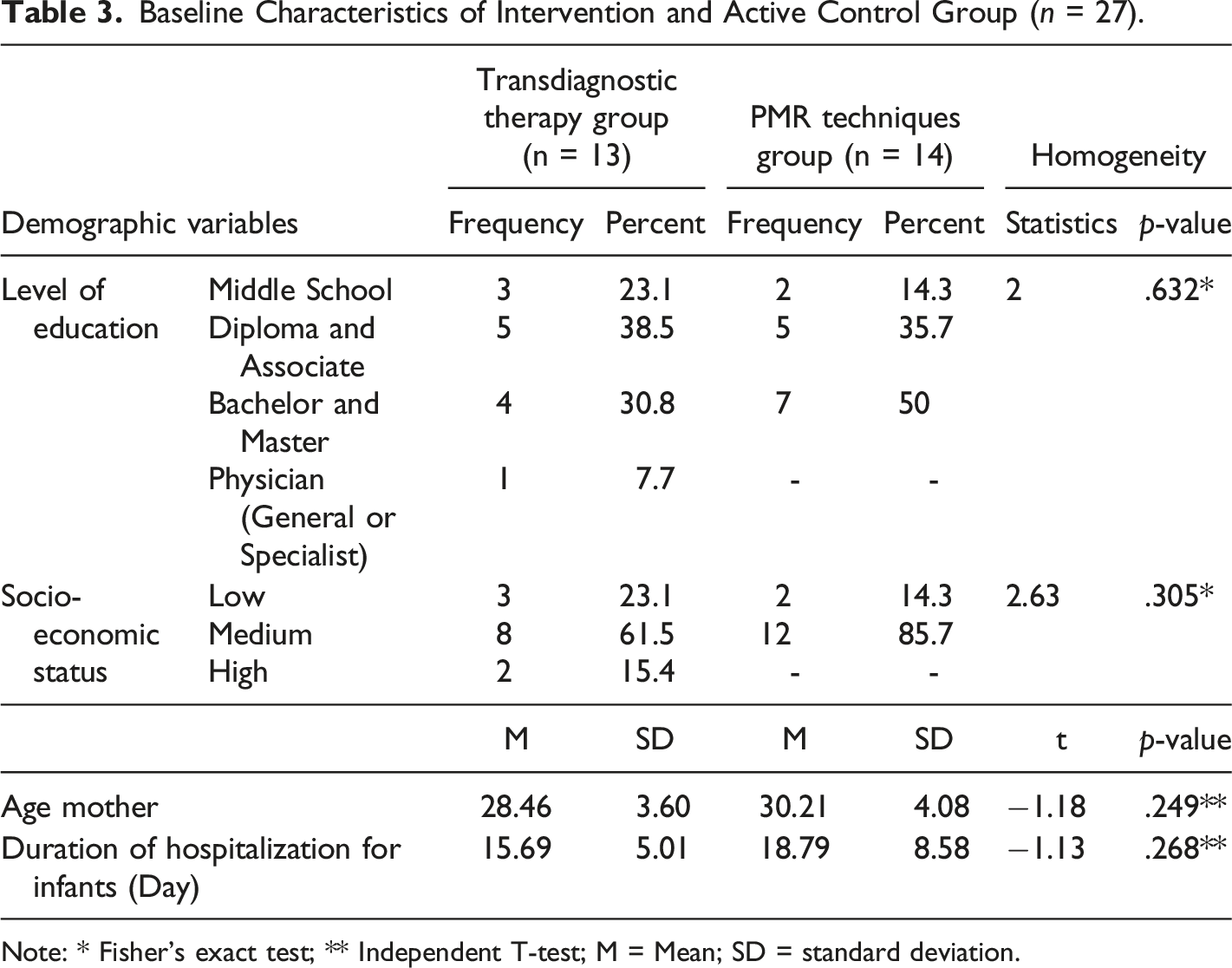
Note: * Fisher's exact test; ** Independent T-test; M = Mean; SD = standard deviation.
The Descriptive Indexes and the Results of the Independent T-Test of Both Groups for Emotion Regulation Strategies, Self-Compassion, Maternal Role Adaptation, and Social and Work Adjustment (n = 27).
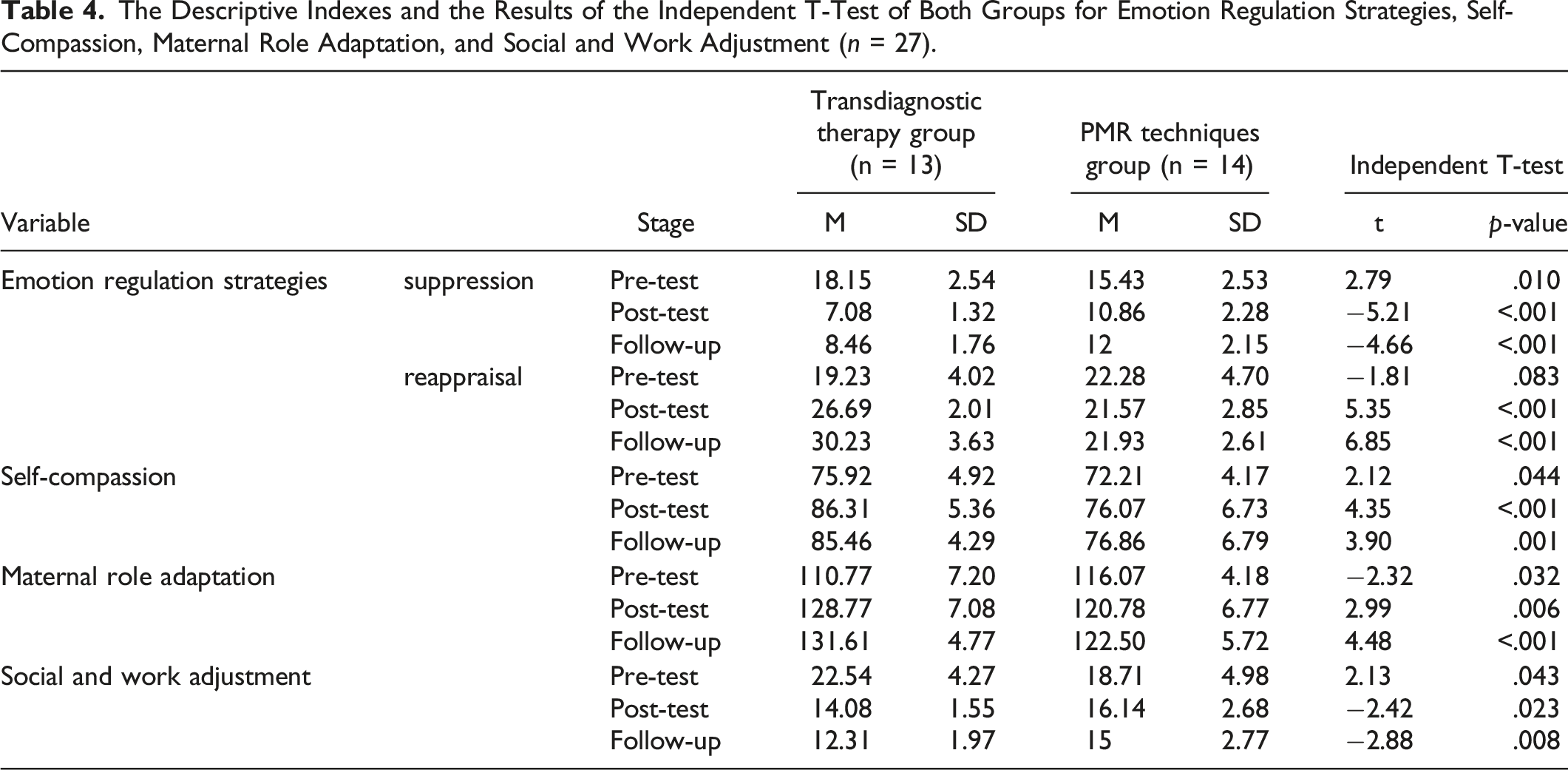
As it is presented in Table 4, and according to the independent t-test results in the pre-test assessments, there is a significant difference between the transdiagnostic and PMR techniques groups in terms of emotion regulation strategies (suppression component), self-compassion, maternal role adaptation, and social and work adjustment (p < 0.05). Therefore, to control between-group differences in the pre-test, MANCOVA and ANCOVA tests were performed. All the relevant pre-assumptions were considered and confirmed (p > 0.05). In order to compare the emotion regulation strategies in the transdiagnostic therapy intervention group and the PMR techniques control group in the post-test and follow-up phases, MANCOVA analysis was used. Since both components (suppression and reappraisal) are taken from the same instrument and ultimately show the regulation of the individual's emotion, MANCOVA was used to investigate their multivariate effect.
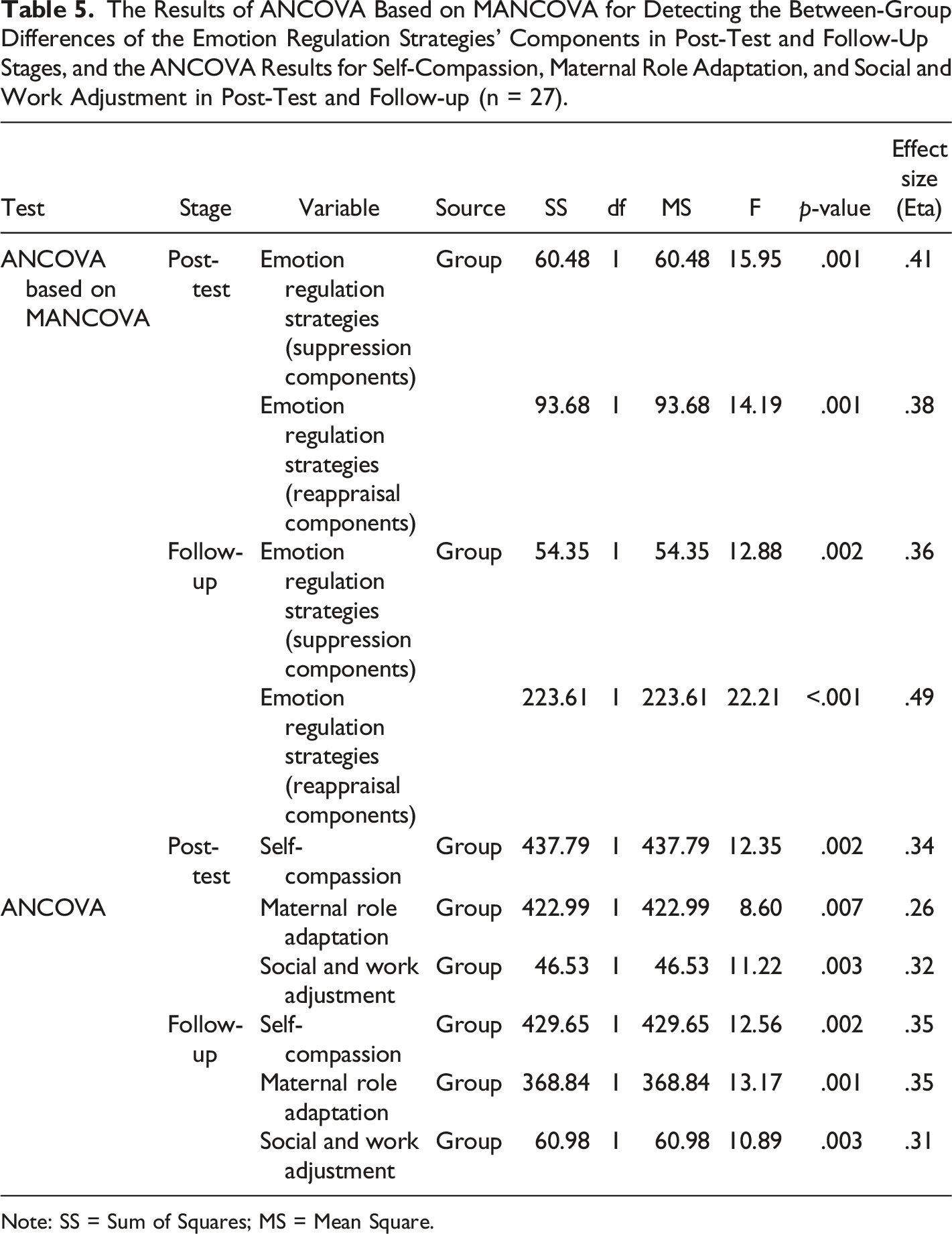
The Results of ANCOVA Based on MANCOVA for Detecting the Between-Group Differences of the Emotion Regulation Strategies’ Components in Post-Test and Follow-Up Stages, and the ANCOVA Results for Self-Compassion, Maternal Role Adaptation, and Social and Work Adjustment in Post-Test and Follow-up (n = 27).
Note: SS = Sum of Squares; MS = Mean Square.
According to Table 5, the between-group differences in the post-test for suppression and reappraisal components are significant. Furthermore, the between-group differences in follow-up are significant for the same components. According to the effect sizes (Eta), the transdiagnostic therapy can respectively explain 0.41% (post-test) and 0.36% (follow-up) of the variance in between-group differences of suppression, and also explain 0.38% (post-test) and 0.49% (follow-up) of the variance in between-group differences of reappraisal.
Furthermore, as Table 5, indicates according to the ANCOVA results in the post-test, there is a significant difference between the study groups in terms of self-compassion, maternal role adaptation, and social and work adjustment. According to the effect sizes (Eta), the transdiagnostic therapy can respectively explain 0.34%, 0.26%, and 0.32% of the variances in between-group differences of self-compassion, maternal role adaptation, and social and work adjustment in post-test. In addition, with respect to the ANCOVA results in follow-up, there has been a significant difference between the study groups in terms of self-compassion, maternal role adaptation, and social and work adjustment. As the effect sizes (Eta) show, it can be concluded that the transdiagnostic therapy can respectively explain 0.35%, 0.35%, and 0.31% of the variances in between-group differences of self-compassion, maternal role adaptation, and social and work adjustment in the follow-up.
Discussion
The current research aimed to determine and compare the effectiveness of the transdiagnostic therapy and PMR techniques on emotion regulation strategies, self-compassion, maternal role adaptation, and social and work adjustment in mothers of premature infants. The results of the current research indicate that compared to PMR techniques, the effectiveness of transdiagnostic therapy on emotion regulation strategies is significant. To the best of our knowledge, research has not examined the effect of transdiagnostic therapy on emotion regulation strategies for mothers of premature infants. However, in studies with different samples from the sample of the present study, it has been shown that transdiagnostic therapy is effective on emotion regulation strategies. for example, Research results done by Fernández-Martínez et al., 39 Corpas et al., 40 Soleymani et al., 41 Zemestani and Imani, 42 and Hooman et al., 30 are considered consistent with our findings. The unified transdiagnostic protocol is an intervention derived from CBT that focuses on emotions, targeting negative emotions and reacting to them. In this treatment, the clients become educated about adaptive emotion regulation strategies. 24 Due to their negative emotional experiences, parents of newborns hospitalized in NICUs tend to employ maladaptive emotion regulation strategies. 8 Therefore, not only does transdiagnostic therapy emphasize positive and negative emotions, it also leads to emotion regulation and reductions in thinking traps by concentrating on emotions. For this reason, the following techniques were utilized in the current study: emotion component identification, monitoring EDBs and changing them, emotion and mood induction, nonjudgmental mindfulness, alteration of cognitive appraisals, and emotional exposure. However, what is emphasized in PMR techniques, is limited to contracting and loosening the muscles.
The results of the current research indicate that compared to PMR techniques, the effectiveness of transdiagnostic therapy on self-compassion is significant. To the best of our knowledge, no previous investigation has shown similar results. Self-compassion requires adopting a positive attitude towards emotions in stressful situations. 43 Self-compassion consists of self-kindness, common humanity, and mindfulness.44-46 Therefore, rather than self-blame, self-compassionate individuals prefer expressing kindness towards themselves when faced with unpleasant emotional situations. 47 Therapeutic mechanisms that result in improved self-compassion, rely on decreases in self-blame and reduced fear from compassion. 48 Transdiagnostic therapy focuses on emotionally proper responses in unpleasant situations. 49 For this reason, in the present study, transdiagnostic therapy could plummet the intensity of unpleasant emotions (such as Self-criticism) and pave the way for improvements in self-compassion by provoking adaptive responses to the stressful experience of infant hospitalization in NICUs. In addition, this therapeutic method included education on functions of emotions, comprehending procedures behind maladaptive appraisals, facilitation of nonjudgmental awareness, and increases in flexibility; all of which could lead to rises in self-compassion. 43 Rather than improving emotion regulation strategies, relaxation relies highly on bodily sensations that play a role in experiencing anxiety.50,51 Contrarily, self-compassion requires not only reductions in the negative aspects of emotions (self-blame), but also increases in nonjudgmental mindfulness. 43 Thus, transdiagnostic therapy emphasizes the importance of identifying and modifying maladaptive emotional strategies and soaring positive emotional strategies in stressful situations; while PMR techniques focus solely on reducing negative emotional symptoms and mindfulness.
The results of the current study indicated that in comparison with PMR techniques, transdiagnostic therapy affected maternal role adaptation significantly. According to our knowledge, there was no previous investigation on the effectiveness of transdiagnostic therapy on maternal role adaptation. However, in their research, Rajabi et al. (2021) reported that maternal role adaptation could be affected by a problem-solving-based intervention. 19 Sohrabi et al. (2021) indicated that utilizing an educational program could affect maternal role adaptation. 52 According to Pouyan et al. (2019), interpersonal psychotherapy could considerably affect the adaptation of mothers with premature infants to their maternal role. 53 Mendelson et al. (2018) indicated that a mindfulness intervention can reduce the levels of distress in mothers in NICUs. 20 Even though the applied interventions in these investigations differ from ours, the results demonstrated that education and psychological programs are effective on maternal role adaptation. In this regard, mothers are the main caregivers of their infants and motherhood is the most important role they take during their lives. Hospitalization of newborns in NICUs can affect the levels of maternal role adaptation of their mothers; 54 and as a result, impairments could increase in the parent-infant relationship and their attachment. Therefore, by providing these mothers with education and psychological interventions, they could gain the required skills in terms of accepting their maternal roles. 52 Transdiagnostic therapy puts emphasis on comorbid symptoms which are expected to improve adaptation to maternal roles in stress-provoking experiences. In this respect, the following techniques were performed in the current investigation: the three-component model of emotions, identification, and modification of EDBs, nonjudgmental awareness, and identifying negative automatic thoughts using the downward arrow. However, what is emphasized in PMR techniques, is limited to contracting and loosening the muscles and reducing stress.
The results of the current study indicated that in comparison with PMR techniques, transdiagnostic therapy on social and work adjustment significantly. Based upon our knowledge, no prior studies had assessed the effectiveness of transdiagnostic therapy on social and work adjustment of parents of premature infants directly. But, Mohammadpour et al. (2018) however, concluded that the combination of transdiagnostic therapy and medication could significantly affect the general functions of individuals with generalized anxiety disorder. 55 To explain this finding, it could be stated that stress-provoking situations can reduce adaptability, and individuals with higher levels of adaptability experience fewer psychological problems. 56 Hospitalization of newborns in NICUs leads to changes in the work state of the parents. 57 After being admitted to the NICUs, the infants can affect the lifestyle of the family and the interactions between family members and consequently, the parents undergo functional problems. This issue can place heavy financial burdens on families. 58 To target such problems, the following techniques were applied in the transdiagnostic therapy: not avoiding unpleasant emotions, identifying negative automatic thoughts, cognitive reappraisal, the three-component model of emotions, and nonjudgmental mindfulness. It is noteworthy that the techniques utilized in PMR techniques were contracting and loosening the muscles in addition to mindfulness.
Limitations
Some of the limitations in the current research were: a lack of cooperation by some mothers and high caution in generalizing the findings to the populations of cities other than Shiraz. Also, due to the low participation of fathers in the early stages of the research, they were left out of the study in general. In addition, caution should be exercised in generalizing the results to other mothers based on their mental health. Another limitation was that the participants in the experimental group had human contact with the therapists, but the participants in the control group made this contact when needed. Therefore, it is suggested that these mothers are provided with more educational programs and psychological interventions during pregnancy or after having their infants discharged from hospitals. Also, it is suggested that the researchers carry out similar investigations in other cities of the country so that the results could be compared for higher generalizability. In addition, it is suggested that researchers investigate the effectiveness of psychological interventions on the fathers of these babies in future studies.
Conclusion
The hospitalization of infants in NICUs is considered a stress-provoking experience for mothers of premature infants. It seems vital to use educational-psychological programs and interventions that can improve the mental health and positive emotional experiences of mothers of premature infants and their adaptation to stressful conditions. Therefore, based on the results generated in the current investigation, if the findings from this study are verified in larger randomized controlled trials it is suggested that hospitals with NICUs and mental-health-related clinics use the findings of this study as a practical guide to improving the psychological health of the mothers of premature infants in NICUs.
Footnotes
Acknowledgement
The authors of the current study would like to express their deep appreciation of the staff of the Vice-Chancellor for Research and Technology of Kermanshah University of Medical Sciences and Shiraz University of Medical Sciences. In addition, we would like to thank all the parents who participated in this study and supported us in conducting this project.
Author Contributions
SR. SMA. AAF. AAP. Study Conception and/or Design; SR. SMA. AAF. RB. AAP. Data Processing, Collection, Perform Experiment; SR. SMA. AAP. Analysis and Interpretation of Results; SR. SMA. AAP. AAF. RB. Draft Manuscript Preparation, Visualization; SR. SMA. AAP. AAF. RB. Critical Revision or Editing of the Article; SR. SMA. AAP. AAF. RB. Final Approval of the Version to be Published; AAP. AAF. SMA. Supervision, Funding Acquisition.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The present research is derived from a master’s clinical psychology thesis (990821) which was financially supported by the Vice-Chancellor for Research and Technology of Kermanshah University of Medical Sciences.
Ethical Approval
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2000. This investigation has been approved by the ethics committee of Kermanshah University of Medical Sciences (IR.KUMS.REC.1399.809).
Informed Consent
All participants completed a written informed consent form to enter the study.
Data Availability
It is possible to access the data after coordination with the corresponding author by email.