
Abstract
Objective
This study examined whether antihypertensive medications and other patient characteristics are associated with severe depressive symptoms in patients with hypertension.
Methods
Patients with a diagnosis of hypertension were recruited from the internal medicine outpatient clinics of a hospital in Amman, Jordan, into this cross-sectional study. Depression severity was assessed using the Patient Health Questionnaire-9 (PHQ-9); anxiety by the General Anxiety Disorder-7; sleep quality by the Insomnia Severity Index; and psychological stress by the Perceived Stress Scale. Multivariable binary logistic regression was used to examine the association between the different classes of antihypertensive medication and depressive symptoms.
Results
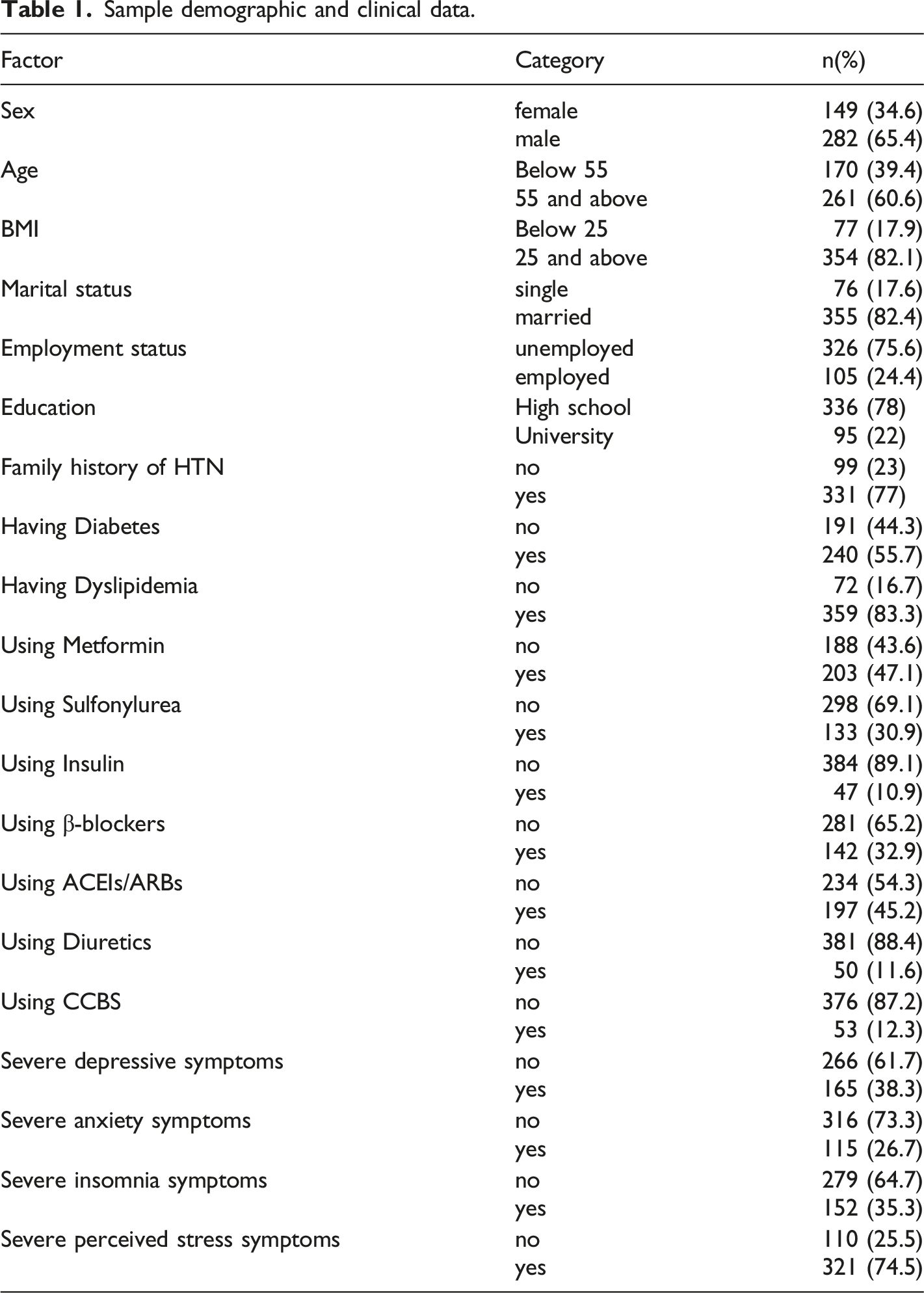
Of the 431 participants, 282 (65.4%) were men; 240 (55.7%) reported having type 2 diabetes; 359 (83.3%) had dyslipidemia; 142 (32.9%) were on beta-blockers; 197 (45.2%) were on ACE inhibitors or angiotensin receptor blockers; 203 (47.1%) were on metformin; and 133 (30.9%) were taking sulfonylurea. Severe depressive symptoms, indicated by scoring above the cut-off of 14 on the PHQ-9, were present in 165 (38.3%) patients. Severe depression was associated with younger age (<55 years) (OR = 3.15, 95% CI = 1.83-5.41, P < 0.001), unemployment (OR = 2.15, 95% CI = 1.15-4.00, P = 0.01), diabetes (OR = 1.81, 95% CI = 1.09-3.02, P = 0.02), severe anxiety (OR = 6.40, 95% CI = 3.64-11.28, P < 0.001), and severe insomnia (OR = 4.73, 95% CI = 2.85-7.82, P < 0.001).
Conclusion
Severe depressive symptoms were not associated with antihypertensive medications or other drugs used by hypertensive patients. Younger age, diabetes, anxiety, and insomnia were the primary correlates of depression.
Introduction
Hypertension is a widespread disease that is considered a major risk factor for cardiovascular diseases such as type 2 diabetes and dyslipidemia, and is a leading cause of death worldwide.1,2 Around 10.4 million deaths worldwide are attributed to hypertension each year. 3 In the Middle East, the estimated prevalence of hypertension is around 33%. 4
The association between hypertension and mental health is bi-directional. 5 Depression is associated with negative behaviours and habits, such as lack of physical exercise, smoking, and lack of medication adherence thus exacerbating hypertension and cardiovascular diseases.6,7 On the other hand, inflammation associated with hypertension could exacerbate depression 8 For example, one in every five patients with coronary artery disease or heart failure is depressed. Additionally. nearly one in every three is depressed post-stroke. 9
Anxiety is a state of uncertainty and fear of the future. 10 Anxiety could contribute to depression through negative behaviour patterns, such as cigarette smoking, lack of physical exercise, and excessive alcohol intake.
Biologically, chronic and uncontrolled anxiety activates the sympathetic system and the hypothalamus-pituitary axis, thus enhancing catecholamines and endothelial dysfunction. 11
Insomnia is a prevalent sleep disorder characterized by a lack of quality sleep and sleep latency. 12 The relationship between insomnia and depression is well-established. Insomnia increases the risk for depression through disrupted emotion; on the other hand, insomnia is a manifestation of depression symptoms. 13
Antihypertensive drugs are the mainstay treatment for hypertension. Evidence about the effect of antihypertensive drugs on mental health is emerging. 9 The use of angiotensin converting enzyme inhibitors (ACEIs) and angiotensin receptor blockers (ARBs) has been associated with improved mental health domains.9,14 Additionally, several studies have reported that calcium channel blockers (CCBs) have been associated with decreased risk of developing depression, perhaps as a result of the calcium regulatory mechanism.15,16 The effect of β-blockers and diuretics on mood disorders is, as yet, controversial.17,18 Depression is one of the main side effects that is reported in patients on beta-blocker medications.19,20 In patients with coronary artery disease, beta-blockers were associated with a higher risk of depression. 21 Furthermore, in an elderly population with hypertension living in Australia and the United States, a cross-sectional study found a positive association between depressive symptoms and the use of beta-blockers, this relationship was stronger in lipophilic and non-selective beta-blockers. 14
In addition to the antihypertensive agents, patients could receive other chronic medications for the associated comorbidities such as type II diabetes and dyslipidemia. It is estimated that 30% of diabetic patients experience clinically significant depressive symptoms. 22 Preclinical and clinical data suggest a potential role of metformin in improving depressive symptoms: however, the data is, as yet, inconclusive. 23 Dyslipidemia patients are at higher risk of developing cardiovascular diseases (CVD), and patients with CVD are at higher risk for depression. 24
Therefore, the current study objective is to investigate whether chronic medications and other patient-related factors are associated with severe depressive symptoms in a cohort of patients with hypertension.
Methods
Study design and participants
This cross-sectional study was approved by the Institutional Review Board of Yarmouk University, IRB project number (2/2023). Participants for their study were recruited from the internal medicine outpatient clinics at Prince Hamza Hospital, Amman, Jordan. All participants signed an electronic consent form prior to participating in the study.
Inclusion criteria
Patients with hypertension visiting the outpatient clinic were approached, and eligible participants were selected using the following inclusion criteria: 1. Diagnosed with hypertension according to the JNC8 guidelines 25 for at least one year, 2. Adhering to their current antihypertensive regimen for the past year according to the Morisky scale.
Exclusion criteria
Patients with established psychological disturbances, such as schizophrenia and other disorders that impair the patient’s ability and competency to fill in the study questionnaire and scales.
Data collection
After the orientation step at the clinics, an electronic link on Google forms was sent to the participants on the same day to ensure privacy. All the participants signed an electronic consent form before participation and had the right to withdraw from the study at any moment. The research team assisted illiterate participants and those unfamiliar with the online questionnaire, by reading out the study questionnaire over the phone for the participants.
The study instrument
Covariates
A self-administered structured online questionnaire was employed to cover the participants’ demographical and clinical data, including sex, age, body mass index, educational level, employment status, family history of hypertension, presence of comorbidities, and adherence. To evaluate adherence to the antihypertensive therapy, the Arabic-validated version of the Morisky scale was used.26,27 The scale is comprised of four items, which are behaviours associated with medication non-adherence, e.g., “do you forget to take your medication?” with simple scoring options as yes and no. The Arabic translation was demonstrated to be reliable with a Cronbach’s alpha score of 0.82. 27 A score of three or less out of four reflects moderate adherence.
Chronic medications
To record chronic medications used by the patients, the approved list of antihypertensive medications, diabetes medications, and dyslipidemia medications dispensed by Prince Hamza’s internal medicine pharmacy was included in a checklist on the online questionnaire. To ensure the accuracy of data collection, both the generic name, the brand name, and the picture of the medication pack were all presented and checked out by the patients. The antihypertensive classes used were β-blockers (bisoprolol, atenolol), diuretics (hydrochlorothiazide), CCBs (amlodipine), ACEIs (enalapril) and ARBs (valsartan). Diabetes medications included metformin, sulfonylurea, and insulin, and dyslipidemia comprised atorvastatin only.
Anxiety assessment
The General Anxiety Disorder-7 (GAD-7) is a short, self-administered scale. It measures anxiety for the last two weeks with a score range from 0 to 21 with a cut-off score of >14 for severe anxiety symptoms. 28 GAD-7 has a sensitivity of 89% and specificity of 82% for diagnosing generalized anxiety disorder 29 and was previously used in Arab-speaking patients. 28
Insomnia assessment
The insomnia severity index -Arabic version ISI-A was used to evaluate sleep quality. Developed by Morin et al., 30 the ISI consists of seven questions with Likert-type answers and a score range between 0-28 with a cut-off score of >14 for severe insomnia symptoms. The ISI is validated to be used in the Arabic language. 31
Perceived stress assessment
Participants were assessed for psychological stress for the past month according to the Arabic version of the Perceived Stress Scale (PSS). The PSS was developed by Cohen and Williamson. 32 It includes 14 items that are designed to measure individual stress for the last 30 days with a cut-off value of 14, reflecting clinically significant stress. The Arabic version was previously used for Arab-speaking patients. 33
Outcome variable: Depression
To assess depression severity, the Patient Health Questionnaire-9 (PHQ-9) Arabic-validated version was used. The PHQ-9 is a short, self-administered scale based on the nine Diagnostic and Statistical Manual of Mental Disorders-IV criteria for diagnosing depressive symptoms. 34 The PHQ-9 has a sensitivity of 88% and specificity of 88% for severe depression and was previously used in Arab-speaking patients. It measures depression for the last two weeks, and it has a score range between 0 to 27 with a cut-off score of > 14 for severe depression.35–37
Statistical analysis
Descriptive statistics were used, including frequencies and percentages to describe the sample characteristics. To investigate the association between the different patients’ factors and the dependent variable (depression severity), a Chi-square analysis was performed. Candidate variables below the cut-off value of P < .10 were included in the multivariate regression. To identify independent associations between the potential factors and dependent variable, a multivariate binary logistic analysis was performed, adjusted for age, employment status, diabetes, anxiety, and insomnia with depression severity as the dependent variable. Statistical significance was set at 2-sided P < .05 and estimates were set at 95% CI.
Results
Response rate
Out of the 516 eligible patients approached, 53 declined participation, 19 did meet inclusion criteria and 13 were excluded because of incomplete data. Therefore, a total of 431 participants were included for analysis, with a response rate of 83.5%.
Characteristics of the participants
Sample demographic and clinical data.
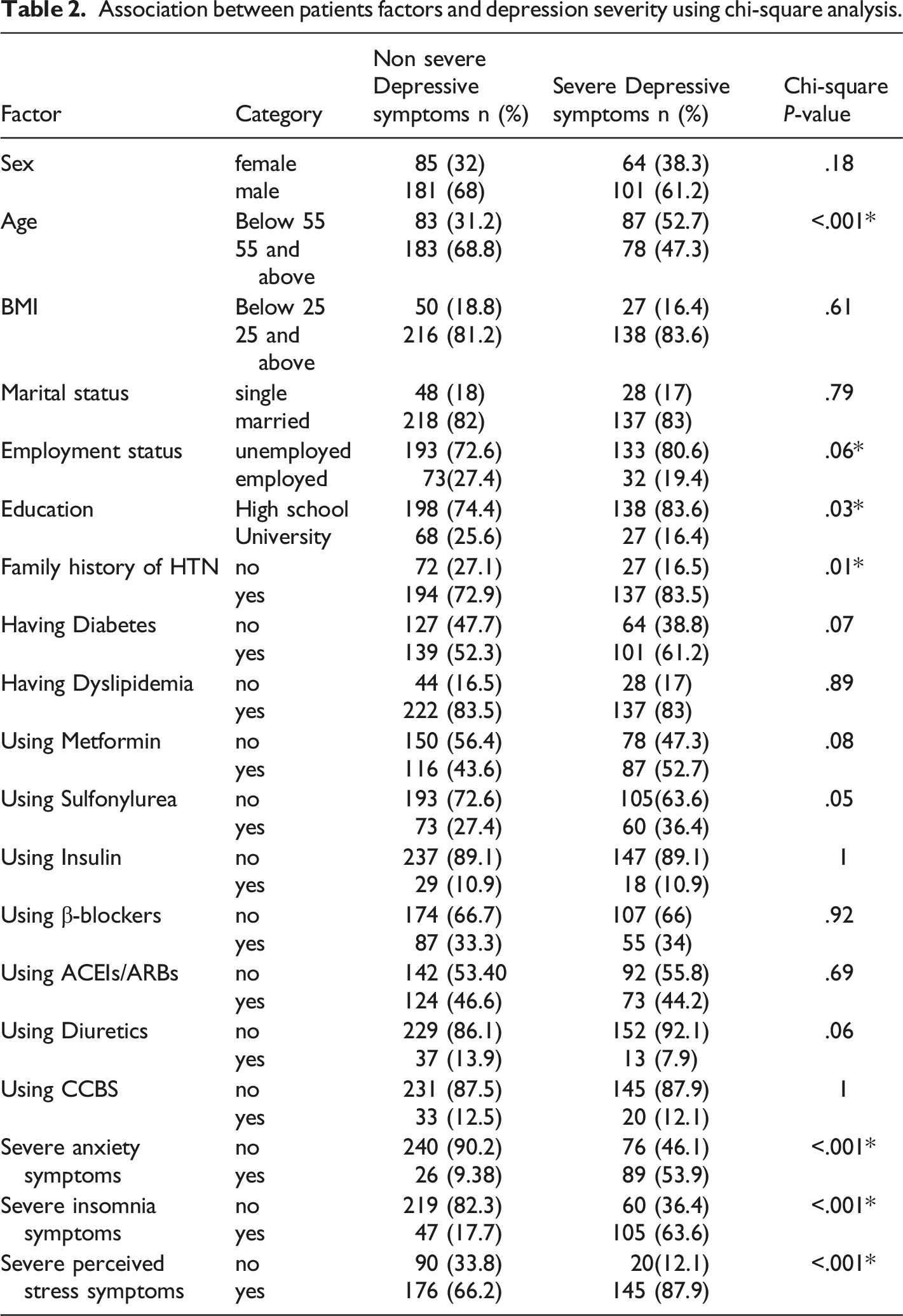
Factors associated with severe depressive symptoms
Association between patients factors and depression severity using chi-square analysis.
Predictors for severe depressive symptoms
Independent correlates of severe depression based on logistic regression analysis.
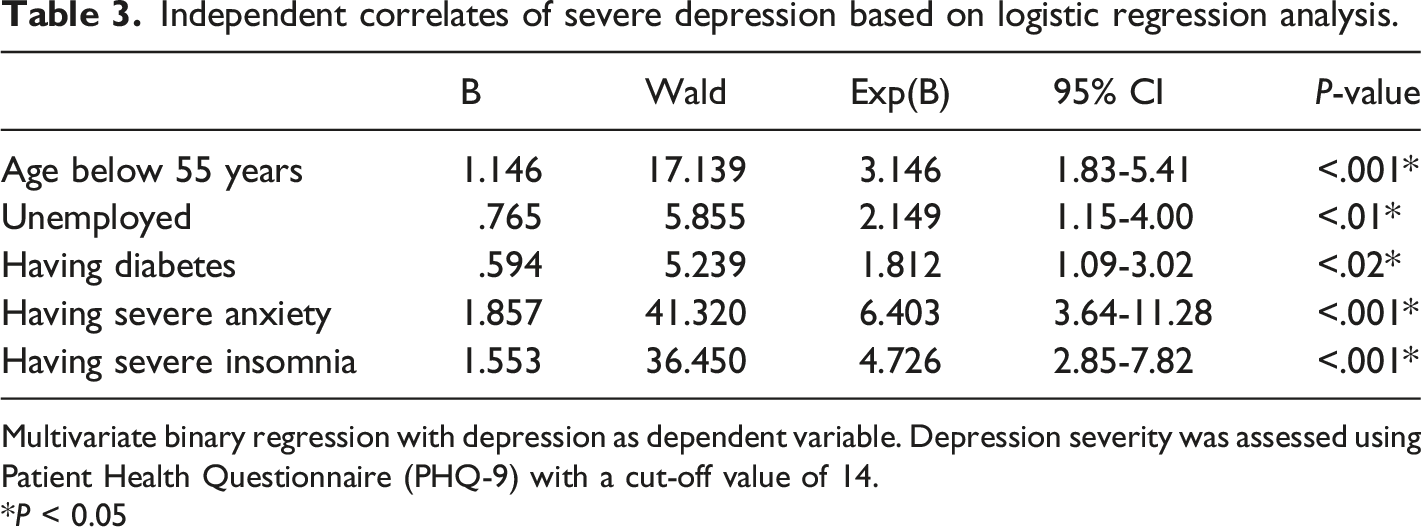
Multivariate binary regression with depression as dependent variable. Depression severity was assessed using Patient Health Questionnaire (PHQ-9) with a cut-off value of 14.
*P < 0.05
Discussion
The present study aimed at investigating whether chronic medications and other patient-related factors are associated with severe depressive symptoms. We report that chronic medications are not associated with severe depressive symptoms: however, we report that younger age (<55 years), unemployment, having diabetes, having severe anxiety, and severe insomnia were associated with severe depressive symptoms.
There are a number of underlying mechanisms suggesting the potential role of antihypertensives in depression. This could include mechanisms involving inflammation, 38 neurotransmission 39 and others. 40
The association between antihypertensive use and mental health outcomes is emerging and controversial.40,41 In our study, no association was found between antihypertensive medications and depression. Several studies focused on the association of β-blockers with depression yielded inconsistent results. For instance, some observational studies demonstrated a positive association between the use of β-blockers and depression.42,43 Similar to our study, other observational studies did not report such an association. In one multicentre prospective study extending for 12 months, there was no difference in depression scores between β-blocker users and non-users. 44 In addition, a recent large population-based study did not report any positive association between β-blockers and depression. 9
This controversy is not only related to β-blockers, as some studies reported that calcium channel blockers (CCB) may be associated with depression and anxiety. 45 This is supported by clinical assessment from a large hospital database with a follow-up for five years that concluded that the use of CCB is associated with increased risk of mood disorders. 46 On the other hand, a recent study on elderly patients treated for hypertension found that the use of CCB along with selective serotonin reuptake inhibitor improves depression and cognitive decline seen in elderly patients. 47
In the present study, antihypertensive medications were not associated with depression. This can be explained based on the cross-sectional study design that did not allow measuring of longitudinal changes of depression i.e., the depression scores in the current study were not measured before and after the antihypertensive therapy. Additionally, the study sample recruited herein was different, depressive symptoms reported by the patients are an outcome of a complex interplay between their underlying medical conditions, environmental exposures and stressors and ethnicity.48,49 Our sample comprised Jordanian patients with diabetes and dyslipidemia who are receiving different chronic medications such as metformin and statins that could have overlapping effects on depression.40,50
Another possible explanation of the results is the antihypertensive medication subtype, for example, depression has been related to propranolol, a lipophilic β-blocker, while other β-blockers were not associated with depression.42,44 Furthermore, the diagnosis or screening of depression across the different studies could yield differences in the results, as while some studies used validated and reliable screening tools, 41 others entirely relied on the use of antidepressants as a proxy for a depression diagnosis.42,44
Chronic depression can also affect the medication use in hypertension; for example, chronic depression could lead to a chronic activation of the hypothalamus-pituitary-adrenal axis, thus counteracting the effects of antihypertensives. 51
Our findings revealed that having diabetes, having severe anxiety, and having severe insomnia were associated with severe depressive symptoms. The risk of major depression is doubled in people with type 2 diabetes mellitus (T2DM), compared with the general population. 52 Depressive symptoms are associated with negative behaviours that could predispose to diabetes; inversely, diabetes is associated with depression based on the hormonal and inflammatory basis. 53
Our findings demonstrated that severe anxiety and insomnia are independently associated with severe depressive symptoms.
Patients with hypertension are at higher risk of developing mental health challenges, compared to their healthy peers. 54 Although the relationship between insomnia, anxiety, and depression is strong, nevertheless, the complete underlying mechanisms are not established yet. Existing literature points to the role of interacting social, psychological, and biological factors. 55
Study limitations
Although the current research has several strengths, such as the sample size; the inclusion criteria and the validated scales, nevertheless, some limitations should be considered. The study subjects were not assessed for psychiatric diagnoses; however, the study used reliable and validated scales to measure all the psychiatric outcomes. However, the cross-sectional design did not allow for measuring longitudinal changes prior and after medication use. Moreover, the sample size per each antihypertensive class was inconsistent.
Conclusions
In this study conducted in Jordan, severe depressive symptoms were not associated with antihypertensive medications or other drugs used by hypertensive patients. Instead, age, diabetes, anxiety, and insomnia were the primary correlates of depression in this patient population.
Footnotes
Acknowledgements
The authors would like to thank Nour, Yasmina, and Suzi for their support.
Authors contribution
Inclusion as a co-author, as required by the International Committee of Medical Journal Editors: have made substantial contributions to the conception or design of the work (Omar Salem Gammoh, Abdelrahim Alqudah, Hanan Abu shaikh) ; or the acquisition, analysis, or interpretation of data for the work (Hanan Abu shaikh , Abdel-Ellah Al-Shudifat, Omar Salem Gammoh) ; AND the drafting the work(Omar Salem Gammoh, Abdelrahim Alqudah) or revising it critically for important intellectual content (Omar Salem Gammoh, Abdel-Ellah Al-Shudifat); AND give their final approval of the version to be published (Omar Salem Gammoh, Abdelrahim Alqudah , Hanan Abu shaikh , Abdel-Ellah Al-Shudifat); AND agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved (Omar Salem Gammoh).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by Yarmouk University (Grant number 2/2023).