
Abstract
Introduction
Balint Groups provide physicians with a forum to develop their capacity to empathically engage with patients, through exploring patient-provider relationships. The Dalhousie University Department of Psychiatry implemented a mandatory Balint Group as part of the junior resident curriculum. The purpose of this study is to explore how residents describe their experience of participating in this Balint Group.
Methods
Psychiatry residents in their first year of training participated in a focus group to discuss their experiences of the Balint Group. Data was analyzed using content analysis.
Results
Three main categories were identified: the purpose of, the process of, and participation in the Balint Group. Process was subdivided into Balint Frame and Institutional Factors. Participation was further subdivided into vulnerability, reflection, fellowship, and validation.
Conclusion
Residents attributed fellowship with their peers, self-efficacy and hope in their work to their participation in the Balint Group. While there was an adjustment period, residents grew to accept, and even appreciate the group. Lack of problem-solving became accepted as part of the purpose of the group and this acceptance was attributed to having other avenues within the program to address problems raised in the discussion. Feeling disconnected when the session ended was described and was related to the abrupt termination of the virtual session or having to exit the group early to return to clinical duties. While the virtual nature of the group was not explicitly identified as a challenge, having to leave early was. While these institutional factors can be mitigated through programmatic implementation, they are not a deal breaker to implementing a Balint Group in a residency training program. Even in a lunch hour or virtual environment our data suggests that the juice is worth the squeeze.
Introduction
Balint Groups are closed groups of physicians who meet regularly to explore thoughts and feelings of their patients and themselves in the context of a patient-provider relationship. 1 These groups serve as an opportunity for physicians to develop their capacity to empathically engage with patients. 2 They also serve as a safe and supportive forum for physicians to explore their own emotions and reactions to difficult cases 2 . While Balint Groups were initially introduced with General Practitioners, 3 with the aim to incorporate psychiatry into general practice, 4 they have also been introduced into medical education programs, where they have been found to guide trainees in becoming more patient-centric as they improve communication, levels of empathy, and reduce personal feelings of burnout. 5 Balint Groups have been a part of residency training for decades but are now more commonly requiring mandatory attendance with continued investigation into the ideal size and frequency of Balint Group sessions. 6 The literature suggests that residents initially report Balint Groups to be stressful as it can invoke a fear of being judged upon expressing personal feelings in a group setting, particularly with respected staff as facilitators. 4 However, the benefits of undergoing this stress are developing feelings of trust, connectedness, and empathy early in physician careers. 4 Although attempts are being made to investigate the efficacy of Balint Groups and its impact on physician behavior 1 there remains limited research in this area particularly from the participant viewpoints. The purpose of this study was to assess how psychiatry residents experience Balint Groups.
Methods
This project has received Research Ethics Board approval through Dalhousie University. All eight psychiatry residents in their first year of residency (PGY-1) at Dalhousie University were invited to participate in a focus group held virtually on MS Teams, where discussion was stimulated in a semi-structured manner to better understand their experience within a program-sanctioned mandatory Balint Group. Three PGY-1 residents participated in the focus group which was held at the end of the academic year. Responses were recorded using a handheld recorder. De-identified transcripts were analyzed by both researchers using qualitative content analysis. 3 Discrepancies were identified and discussed until consensus was achieved.
Results & Analysis
Residents’ experiences of participating in the Balint Group were categorized into three broad categories: experiences related to the purpose of the Balint Group, experiences related to the process of Balint Group and experiences related to participation in Balint Group. Each of these broad categories were further subdivided to produce the coding frame (Figure 1). Coding Frame.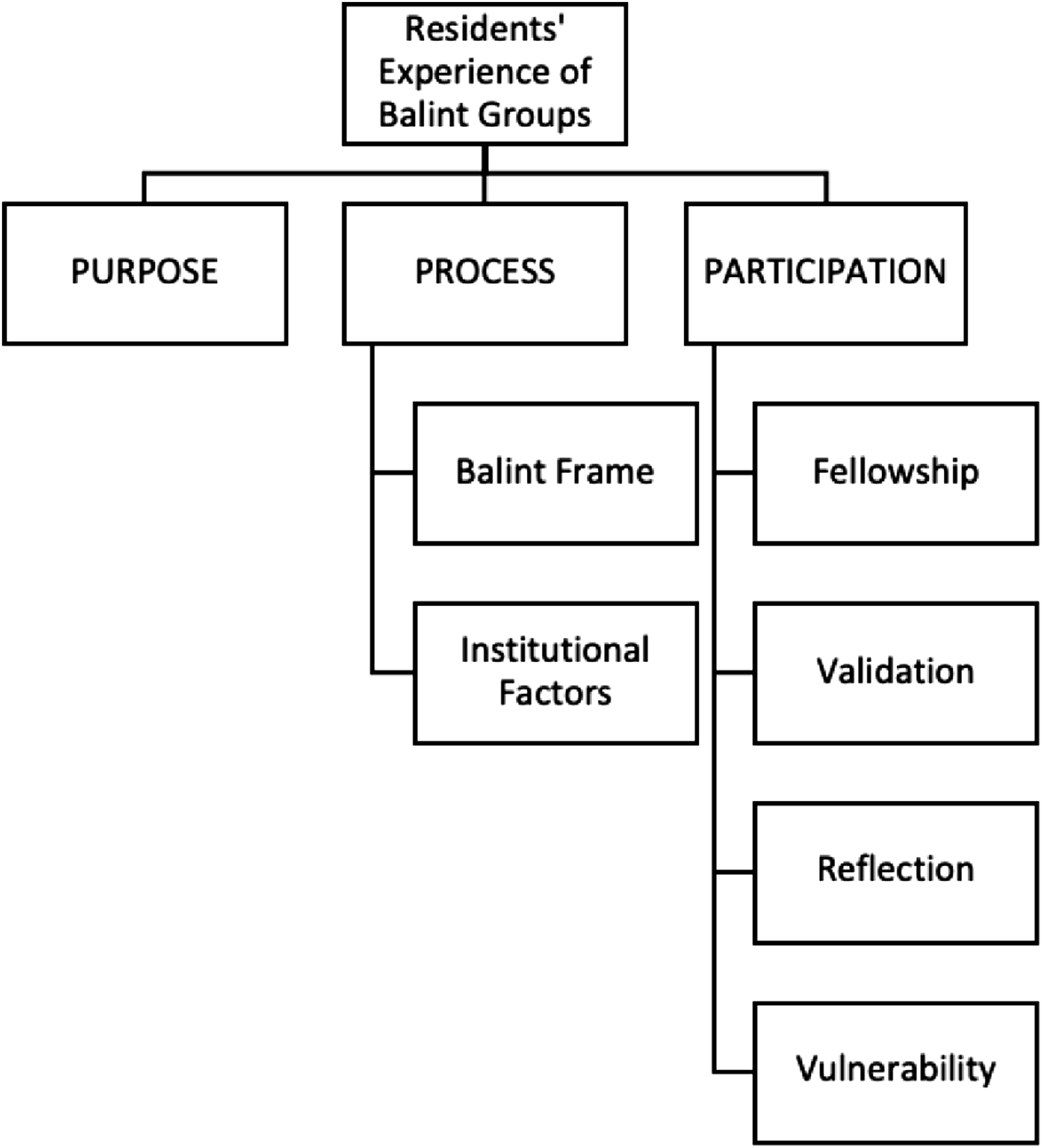
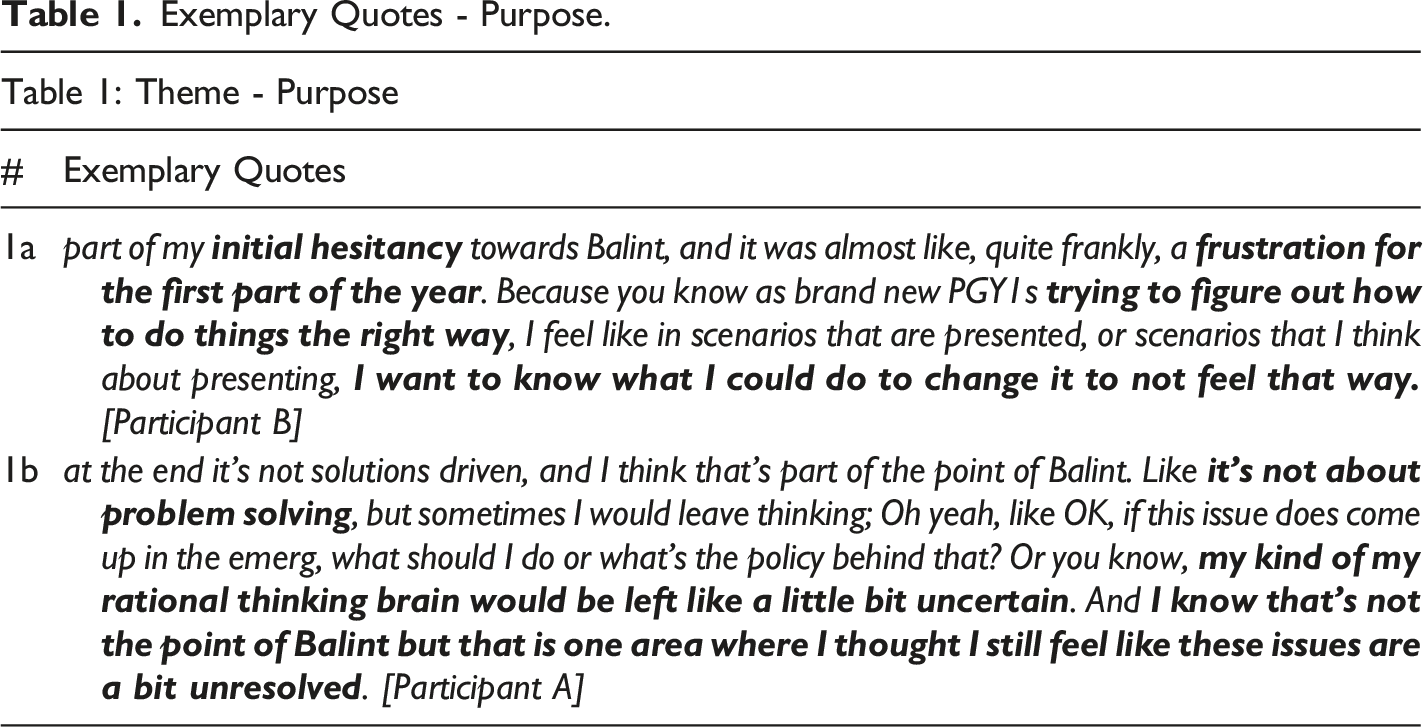
Purpose
Exemplary Quotes - Purpose.
Process
The process of the Balint Group was divided into two sub-categories, Balint Frame, which were structural components that are core features of Balint Groups regardless of the institutional setting, and Institutional Factors which were program-driven decisions related to the implementation of the program within the Dalhousie University Department of Psychiatry.
Exemplary Quotes - Process.
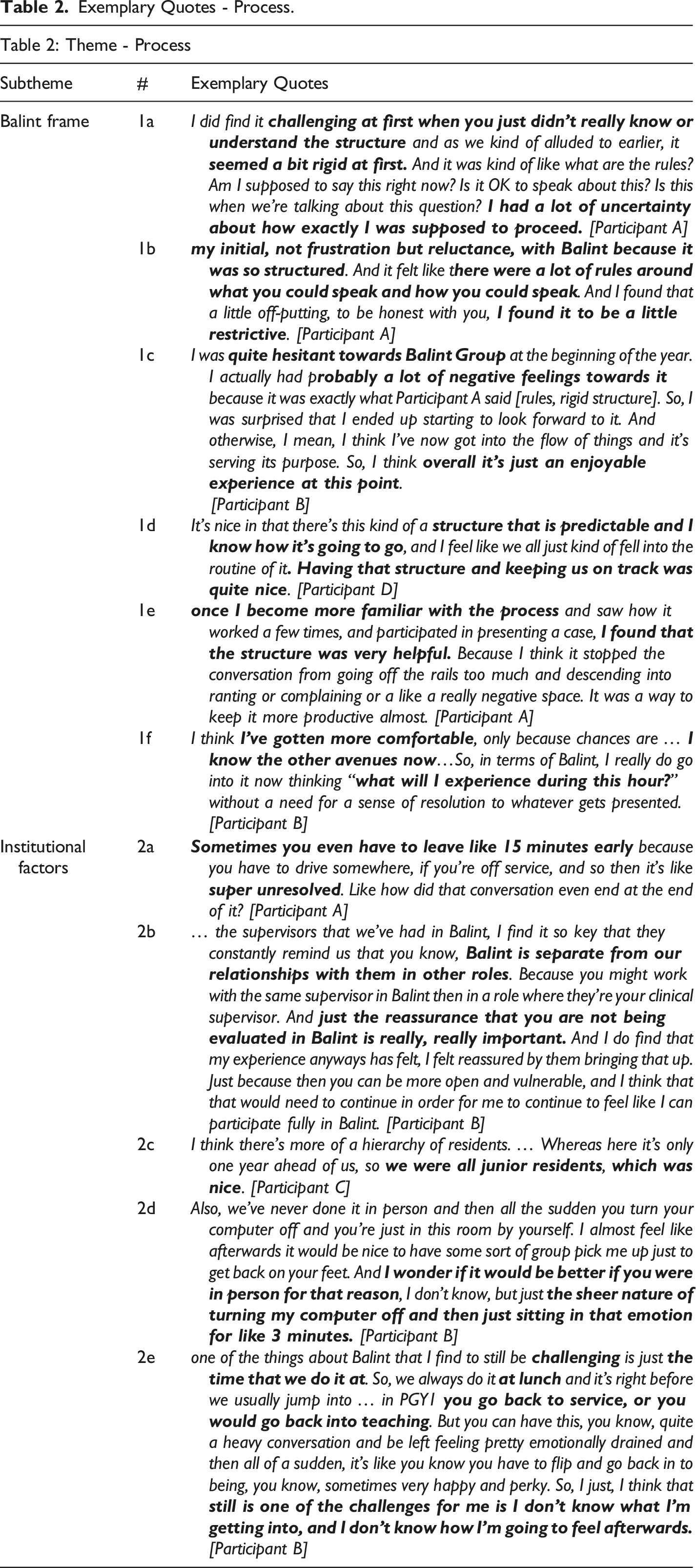
Institutional Factors related to the scheduling of the group (during the lunch hour session), the format of the group (virtual), the stance of the facilitator (non-evaluative), the co-participants (junior residents), and the fact that it was mandatory. The scheduling of the group was described as a challenging factor as some residents, depending on their training rotation, would have to leave the group early to report for clinical duties. Even when the session did end on time, the virtual nature of the group led to feelings of an abrupt ending to the session. The Balint Group was not evaluated beyond attendance. This was experienced as ‘really important’ [Table 2 - 2b] and allowed for authentic participation. It was perceived as unproblematic for facilitators to have dual relationships, where they may assume a supervisory (and thus evaluator) role in other areas of training; but it was important to distinguish these two roles and reassure residents their participation in the Balint group would not impact their clinical rotation evaluation. Participants described it was ‘nice’ [Table 2 - 2c] that the group was composed of members in a similar stage of training and not in a senior stage of training.
Participation
Participation in the Balint Group was further divided into four sub-categories. The most discussed was fellowship, followed by validation, reflection, and vulnerability.
Exemplary Quotes - Participation.
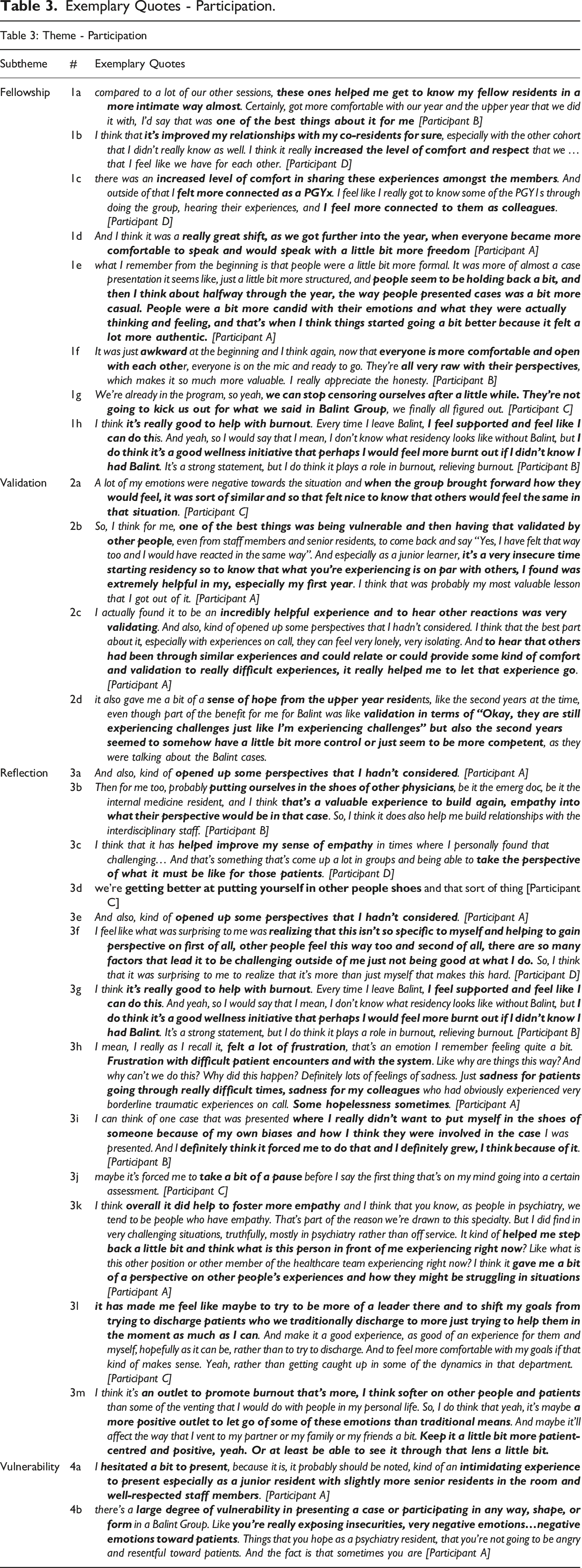
Validation was another prominent theme discussed by residents. Residents felt validated when talking about experiences in both case presentations and discussions. In listening to others, they learned ‘others would feel similar’ [Table 3 - 2a]. One resident commented that ‘one of the best things was being vulnerable and then having that validated by other people’ [Table 3 - 2b]. It was under the process of feeling validated by their peers that residents also commented about ‘finally’ being able to ‘let that [case] go’ [Table 3 - 2c].
Reflection was characterized by residents imagining the thoughts and feelings of themselves and others within the presented case. This was described as ‘perspective taking’ [Table 3 - 3a] and ‘putting themselves in the shoes’ [Table 3 - 3b] of others. Residents perceived themselves as ‘improving’ [Table 3 - 3c] and ‘getting better’ [Table 3 - 3d] at this. They described ‘opening up’ [Table 3 - 3e] to new ways of thinking about challenging encounters, which could lead to ‘feelings of self-sufficiency; ‘realizing there’s more than just themselves that make this hard’ [Table 3 - 3f] and that ‘[they]’ve got this’ [Table 3 - 3g]. It was not always perceived as a comfortable experience. Residents described feelings of ‘sadness’, ‘hopelessness’ and ‘frustration’ [Table 3 - 3h]. One resident described an experience where reflecting on another’s perspective ‘forced’ them out of their ‘comfort zone’ [Table 3 - 3i] Despite the feeling of discomfort, they reported they ‘grew’ [Table 3 - 3i] from the experience. Residents described this as ‘a pause’ [Table 3 - 3j] to ‘step back’ [Table 3 - 3k] and consider what others may be experiencing, which allowed residents to reflect on their own role in the clinical encounter and to reframe the encounter as a ‘leader’ [Table 3 - 3l] in a way that prioritized patient care and separated interpersonal dynamics between health-care teams and systemic pressures.
Vulnerability included a general sense of ‘hesitancy’ [Table 3 - 4a] that preceded participation. Participating ‘in any way, shape or form’ [Table 3 - 4b] was experienced as ‘exposing’ [Table 3 - 4b] insecurities and perceived weaknesses.
Discussion
Residents described a variety of experiences in their participation in a program sanctioned Balint Group. There was a definite adjustment period as residents came to accept and appreciate the Balint Group’s purpose and processes. Residents described an initial ‘reluctance’ [Table 2 - 1b] to engage in Balint Group and described it as being ‘awkward’ [Table 3 - 1f]. These experiences were often described as being problematic in the first half of the academic year which suggests that some of this may be explained by normative reactions of adjusting to new expectations, such as negotiating participation in a new group and engaging in new ways of thinking about, and talking about, challenging clinical encounters. While it is tempting to try and mitigate this adjustment period by directly addressing the why and how of Balint, some residents described that despite being informed of this, it was something that they just had to ‘experience’ [Table 2 - 1f].
As residents came to appreciate the Balint Group, they described the group as enjoyable [Table 2 - 1c] and experienced an increased sense of cohesiveness between co-participants and universality in shared experience.7,8 The group was perceived to be supportive and generated both a sense of hope and increased self-efficacy [Table 3 - 2d]. One resident spontaneously suggested that Balint Group was ‘a sort of wellness thing [the program] brought in’ [Table 3 - 1h]. Another participant later offered that they ‘believed [the Balint Group] helped to mitigate against burnout’ [Table 3 - 1h] as it provided an opportunity to share challenging patient encounters and speak authentically about thoughts and emotional reactions to clinical encounters.
Residents described that through participation in the Balint Group they gained a sense of hope and self-efficacy. This is supported by research associating Balint Groups with improved empathy, supporting professional development and decreased rates of burnout. 9 They have also been associated with self-efficacy. 10 Burnout is a clinical syndrome characterized by three domains: depersonalization, 11 emotional exhaustion and low personal accomplishment. 12 Residents described a shift in how they understood perceived negative patient encounters as not solely a reflection of their competence; ‘it’s more than just myself that makes this hard’ [Table 3 - 3f]. This suggests that Balint Groups may act as a wellness intervention in promoting self-efficacy in their role as physicians by creating a sense of emotional readiness to engage in their work and a willingness to engage in discussions related to challenging patient encounters in a ‘softer’ [Table 3 - 3m] way. With increased attention on reports of burnout in medical professionals, 10 including medical trainees, 13 this is an important consideration. Training programs have an increasing responsibility to support residents in the professional development of the competencies required to effectively care for patients - including maintaining their own well-being. 14 These findings offer support for the inclusion of Balint Groups in the post-graduate medical education curriculum.
Residents described feeling disconnected when Balint Group sessions ended [Table 2 - 2d]. While disconnection from the group discussion can be considered part and parcel of any Balint Group session, the experiences described by residents highlight the abruptness of the virtual session being terminated as the technology switches off. Leaving the group early also contributed to a sense of being disconnected from the group discussion. It was not uncommon for residents to have to ‘leave 15 minutes early’ [Table 2 - 2a] and resume clinical duties with others who had not participated in the Balint Group [Table 2 - 2e]. This challenge was solely attributed to the scheduling of the Balint Group - during the lunch hour session and was the only feature of the Balint Group that was consistently described as challenging. While these feelings of disconnection and isolation were clearly mentioned in our data, it is not talked about in the literature. This may relate to the Balint Group being virtual. In a virtual Balint Group, there is a loss of informal interpersonal interactions that bookend the group work. While this raises important considerations for implementing a virtual Balint Group, our data also suggests that the Balint purpose and process can be maintained in virtual groups. They offer an acceptable and feasible pivot to overcome factors that may otherwise be considered a barrier to implementation. For example, in the context of the COVID-19 global health pandemic, they offered a safe gathering venue. They also have the potential to overcome challenges associated with ensuring equitable training opportunities across distributed medical education training sites. As such, ongoing research in this area will be of interest.
While disconnection from the abrupt or early termination of the group was felt to be challenging throughout the academic year, coming to terms with case discussions being unresolved came to be accepted. One resident described it as ‘if it does feel unresolved now, it doesn’t bother me as much as in the beginning, because I have the expectation that Balint Group is not for problem-solving, it's for processing’. While this shift in expectation was largely felt to be secondary to having other avenues to raise concerns within the program, our data suggests that there is a shift in tolerating sitting with uncomfortable emotion and unfinished business.
There are limitations to this study. It was conducted with a small sample of PGY-1 residents from one residency program which limits generalizability. It is possible that some of this cohesiveness may be attributed to other activities in the residency program, these were not part of the focus group discussion. Ongoing research in the qualitative experiences of residents’ participation in Balint Groups may provide further insight into the benefits and limitations of this curriculum intervention.
Conclusion
Residents in the Balint Group clearly developed a sense of fellowship and trust in the group and the experience became enjoyable and valued over the course of the academic year. Residents described increased hope and self-efficacy in participating in case discussions and themselves suggested that the Balint Group may help to mitigate burnout. While there was an adjustment period as residents became accustomed to participating in the Balint Group, over time they grew to accept, and even appreciate the group. Lack of problem-solving became accepted, rather than appreciated, and this acceptance was attributed to having other avenues within the program to address problems raised in the Balint Group discussion; however, our data suggests that there may also be an increased tolerance to sitting with unresolved problems as they arise in clinical encounters. Residents described a sense of feeling disconnected from the group following the Balint Group session, which seemed to be attributed to the abrupt shut-down of the technology or having to leave the group early to return to service. While the virtual nature of the group was not explicitly identified as a challenge, having to leave early was. In fact, the only feature that remained an ongoing challenge throughout the year was the scheduling of the group which conflicted with clinical duties that trumped participation in the Balint Group. While these institutional factors can be mitigated through programmatic implementation, they are not a deal breaker to implementing a Balint Group in a residency training program. Even in a lunch hour or virtual environment our data suggests that the juice is worth the squeeze.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Mach-Gaensslen Foundation of Canada ($5000).