
Abstract
In spite of scientific developments, paranormal beliefs remain widespread, especially in South Asian societies. Numerous disorders connected to possession and trance have been theorized in recent years. In this study, three community samples were used to develop a comprehensive scale of Belief in Jinn Possession Scale (BJPS) and to examine its consistency and relevance. The BJPS scale was proposed to be multidimensional with four factors displaying satisfactory internal consistency reliability estimated by the exploratory factor analysis (EFA) (n = 300). However, confirmatory factor analyses (n = 300) reduced the number of factors to two. The BJPS demonstrated excellent reliability and statistically significant positive correlations among its factors of beliefs about signs of possession and beliefs about vulnerability and preventive measures. Convergent and discriminant validity (n = 316) was supported by a high correlation between BJPS, Revised Paranormal Belief Scale (RPBS), and Paranormal and Supernatural Belief Scale (PSBS) and a low correlation between BJPS, Narcissistic Personality Inventory 16 (NPI-16), and Moral Identity Measure (MIM). These results suggest that the BJPS is a well-grounded and sound tool for evaluating one’s irrational beliefs about possession states in Pakistani culture, and it may be the first attempt to conceptualize possession.
Introduction
When the father of modern psychiatry Krapelin visited Asia, he suggested incorporating cultural differences into psychopathology as his patients failed to express their illness in the typical mannerism (Braakman, 2021). It is said that medical symptoms, diagnoses, and practices reflect social, cultural, and moral concerns (Kirmayer et al., 2021). In addition to defining what constitutes an illness, culture also determines how that ailment will be treated, and culture tailoring can enhance treatment outcomes (Huey & Tilley, 2018). Over the previous two decades, significant medical investigations and conceptual inquiries were conducted to examine the intricate interaction between psychiatric illness, race, and culture and they were successful in creating a completely new field of research called cross-cultural psychiatry, often referred to as ethnopsychiatry, transcultural, or, more recently, cultural psychiatry (see Grau et al., 2020; Mendenhall et al., 2019). Because the human brain is primarily a social brain and mental health issues can manifest themselves in learning deficiencies in families and communities, cross-cultural psychiatry is now more important than ever. This importance of culture for diagnosis, assessment, and treatment is also expressed by the DSM 5 (American Psychiatric Association [APA], 2013) through the inclusion of a section on culture-bound disorders. One of the most crucial jobs for academics and therapists working in cross-cultural studies may be the identification and comprehension of “Cultural Bound Syndromes.” It may enable a better insight into individuals’ behavior in a particular culture, encouraging a tolerant interpersonal connection and an effective therapeutic setting (Asnaani et al., 2022).
Among Muslims, societal and theological genesis, attribution, and conceptualization are significant factors in determining a person’s psychological or mental health issues and the choice of appropriate services. An overview of the literature specified that Muslims tended to put off getting professional mental health services owing to numerous possibly treatable factors such as possibly due to negative attitudes and beliefs toward these facilities and their providers, their belief in supernatural explanatory models, and subsequently their magico-religious practices (Lim et al., 2018; Ventriglio et al., 2018). Several experts emphasize individuals’ beliefs should be interpreted within the backdrop in which they appear they will impact both clinical manifestations and individuals’ explanatory theories (Pietkiewicz et al., 2021). Muslim communities incline to attribute psychiatric illness to possession mostly by paranormal entities such as the demon or jinns (McCrae et al., 2019). However, among clinical practices, possession states are perhaps the most vivid, conspicuous, and exotic but least understood as there is a gap in research exploring the experiences and explanatory models of people labeled in local communities as possessed (Pietkiewicz et al., 2022a). Possession states are defined as the substitution of the established sense of personal identity by a novel self, ascribe to the effect of a spirit or Supreme Being, and are intentionally sought or occur unintentionally and can be classified as either normal or pathological depending on whether it adheres to societal norms and expectations (Sapkota et al., 2014). Possession states are linked with stereotyped “involuntary” actions or amnesia, speaking foreign languages or speaking in spirit’s voice, changes in articulation or inflection, speechlessness, paracusias, impulsivity, inappropriate giggling and sobs, and aberrant bodily experiences including aches, tingling, and paralysis of limbs, paraplegia, changes of personality, rapid mood shifts, uncontrollable laughing or crying, depression, preference for solitude, and other detrimental impacts on behavior or overall health, or enhanced powers and classified as socio-culturally shaped dissociative phenomena (Guthrie et al., 2016; Hanwella et al., 2012; Sapkota et al., 2014; Van Duijl, et al., 2010).
This phenomenon is prevalent in several developing countries, particularly in Asia and Africa as a component of religious and healing rituals and as a form of affliction (Pietkiewicz et al., 2020, 2021). However, it is not only common in Asian cultures but also in European-American cultures (Koc & Hocaoglu, 2020; Van Duijl et al., 2010). As a matter of fact, in a worldwide survey of 488 societies, 437 (90%) had at least 1 altered state of consciousness in their culturally structured form, and in 252 societies, such incidents were ascribed to possession (Bourguignon as cited in Al-Adawi et al., 2019). However, in the European and North American cultures where the bio-medical and psychological models dominate, such states are most likely to be observed among people from Nepal, the Middle East, Africa, or Pakistan (Acharya, 2019; Ahmad et al., 2023; Rashed, 2020; Zaretsky & Shambaugh, 2019). Subsequently, it is demand that healthcare professionals should handle these experiences using a culturally appropriate framework (Gunson et al., 2019).
Possession is listed in the DSM-5 as a potential sign of dissociative identity disorder (DID; APA, 2013). Thus, DSM-5 emphasizes people with DID may experience abrupt changes in behavior and identity that are ascribed to possession and is a transition between dissociative personality states (Somer et al., 2015). However, such studies do exist that identified no link between DID diagnosis and accounts of being possessed by spirits. On the contrary, having a belief in possession is directly linked with auditory hallucinations, visual hallucinations, impairment of consciousness, loss of speech (Bakhshani et al., 2013), haptic and olfactory hallucinations, affective disorders, suicidal activity (Kopeyko et al., 2018), borderline personality disorders (Martins et al., 2022), locus of control (Sagone & De Caroli, 2014), cognitive ability (Andrews & Tyson, 2019), and ability to deal with adversity and stress (Betsch et al., 2021). Possession is also used as an explanation by individuals to describe certain other psychiatric conditions (Khan & Sanober, 2016). In an analysis of 47 case reports of jinn possession, 66% of the subjects had a psychiatric condition, and 45.2% of them had schizophrenia (Lim et al., 2015). In another study on psychiatric patients with possession symptoms, 73% had schizophrenia diagnoses, 10% had dissociative disorders, 13% had somatoform disorders, and 3% had affective disorders (Somasundaram et al., 2008). The extant body of literature demonstrates that clinical manifestations associated with schizophrenia, such as delusions and hallucinations, bear a resemblance to the phenomenological presentation observed in cases of purported possession. In certain instances, possession phenomena have been colloquially referred to as a form of delusion of possession (Pietkiewicz et al., 2021). Possession has also been substantially considered in the literature in association with culture-specific syndrome (Zulfiqar et al., 2019), conversion disorder (Irmak, 2014), post-traumatic stress disorder (PTSD) and trauma (Herath & Perera, 2020), panic disorder (Bragazzi & Del Puente, 2012), depression (Marshal, 2017), capgras syndrome (Koc & Hocaoglu, 2020), mania (Khan & Sanober, 2016), somatoform disorders (Pietkiewicz et al., 2022b), and suicidal ideations (Scripcaru et al., 2017). Because of the existing link between mental health and possession, it is critical to investigate all aspects of possession. The current research is an attempt in this regard.
Rationale
Additional research is required to investigate the connection between explanatory models and the usage of health care (McKay & Ross, 2021). The variety of religious beliefs among the global population presents difficulties for healthcare providers and healthcare systems in providing medical care that is culturally sensitive and appropriate (Swihart et al., 2018). Nevertheless, incorporating traditional indigenous cultural wisdom into the understanding of mental illness provides extremely valuable perspectives for a more meaningful contextualization of mental well-being (Verginer & Juen, 2019). Cultural diversity is present in understanding mental health and the issues related to it globally, but, unfortunately, the dangers of applying Western explanatory models to the experiences of different cultural groups, without an acknowledgment of cultural differences, are obvious (Apers et al., 2023). One of the most commonly encountered cultural explanatory frameworks comprises of faith-driven supernatural explanatory models (Jacobi et al., 2022; Pan et al., 2020; Rathod et al., 2023) that are more resilient one in society than other models. Understanding these indigenous knowledge systems is important because culturally specific notions about mental health may determine how people seek out medical care (Martinez et al., 2020), respond to disease, and the implementation of effective approaches to mental health care (Arundell et al., 2020). The fact that we currently live in a globalizing society where individuals of all cultures and religions frequently interact with one another in both the real world and the virtual world is another reason why a cultural psychology approach is necessary (Jensen, 2021). Consequently, it is critical to incorporate religion into clinical practice when appropriate and take a patient’s cultural and religious views into account when choosing a specific clinical intervention (Ventriglio et al., 2018).
In the realm of individualized treatment, it is crucial to remember that Muslims are diversified people (Lim et al., 2018) yet psychiatric illness among them is frequently underreported and undiagnosed due to apprehension about mental health practitioners misinterpreting them (Tanhan & Young, 2022). Tanhan (2019) shows that most Muslims were interested in seeking help from a therapist who was a Muslim and were not willing to take part in therapy with a therapist who was not Muslim. This may be because situational attribution such as evil eye or jinn possession exists in certain Muslim psychiatric populations and since Western medical experts are generally unfamiliar with such attribution styles; consequently, diagnosis may prove challenging, particularly when language barriers and cultural differences are already present during the patient–physician consultation (Tanhan & Francisco, 2019). Due to these reasons, DSM 5 recently acknowledged the importance of integrating various worldviews in psychology practices to transcend Eurocentric focus and to recognize the psychological diversity present in cultures around the world (Sersch, 2019).
The sphere of spirit possession is extensive, and multifaceted, different accounts are present from various fields of study and with varying degrees of analysis (Rashed, 2020) which demands further study. However, it is not given much attention by mental health care systems, partly because diagnosing and treating pathological trance syndromes are culturally challenging. There also exists relatively little information on the mental health of people who often encounter possession states in a spiritual context (Moreira-Almeida & Cardeña, 2011). Some experts further believe that the association between DID and possession states has to be investigated further as it is common for health professionals to misdiagnose for DID and also that possession and trance disorder is not a culture-bound syndrome (Rassool, 2018). Therefore, there is a more urgent need for healthcare professionals to have some level of cultural competency or understanding, awareness, and respect for diverse worldviews (Rice & Harris, 2021). However, achieving a comprehensive understanding and cultural competence regarding the concept of possession requires a deep exploration of how possession is perceived and defined within various cultural contexts. This research marks the initial phase of this endeavor by providing an extensive analysis of how possession is conceptualized, especially within the Pakistani culture. This conceptual insight equips us with specific information that can assist in understanding instances of possession in clinical settings, although it is important to note that further research is essential in this area. This assessment tool can prove valuable in screening individuals who hold beliefs related to possession, rather than hastily categorizing them as DID patients. It emphasizes the importance of considering their cultural beliefs as an integral part of the assessment process.
Method
Study 1. Initial development of the BJPS
This study was approved by the National Institute of Psychology, Islamabad, Pakistan. The scale development in this study draws upon the conceptualization of jinn possession in Pakistani culture. Items for this indigenous scale and domains were specified and formulated after scrutinizing interviews with 21 adults who were believers of possession and available literature (see DeVellis, 2016). Responses of the interviewers were analyzed in a way that ensured that the content of the items reflected the construct of jinn possession. This process resulted in the articulation of 39 items that were written as declarative statements followed by response options that indicated several levels of agreement or disagreement with the statement on a 5-point Likert-type scale. These items and domains correspond to symptoms, indications, vulnerable states, and means of prevention of jinn possession by locals. Each item’s face validity was graded, and comments were made on each item as well as the scale as a whole by three experts (n = 3) on scale development in indigenous contexts and two bilingual experts (n = 2). For each item, they were given three options; retain, delete, and amend. Items were reduced to 34 when experts’ suggestions were added and problematic or items with low face validity ratings were edited or removed. To further maximize the face validity of the items, a total of 30 believers of jinn possession were given the scale to assess the items for relevancy, clarity, language appropriateness dimensionality, and redundancy. In addition, each of these believers participated in in-person discussions where they expanded on their remarks and evaluations of the scale. However, some redundancy was kept in the final item pool as a necessary component of internal consistency (DeVellis & Thorpe, 2021). After this process, The Belief in Jinn Possession Scale (BJPS) items were reduced to 31 items that indicate the extent of belief in jinn possession on a 5-point Likert-type scale with 1 being strongly disagreed and 5 strongly agree.
Initial administration
Sample
In this study, we recruited adults from various regions, specifically from Khyber Pakhtunkhwa (KPK), Punjab, and Islamabad in Pakistan. These regions were deliberately chosen due to their diverse cultures, which were expected to have a significant impact on the beliefs we were investigating. Our participants represented a broad spectrum of backgrounds within the local community, including different religious denominations. The largest proportion of respondents belonged to the Ahle Sunnat sect (25.4%), followed by the Ahle Hadith sect of Islam (24.7%), and the Ahle Sunnat Barelv sect (24.1%), with smaller percentages belonging to the Ahle Tasheeh sect (13.0%) and the Ahle Sunnat Deobandi sect (10.7%). Furthermore, our sample predominantly consisted of individuals with higher levels of education, with a significant portion having completed either graduate (35.8%) or postgraduate (35.1%) degrees, while fewer had undergraduate qualifications (28.7%). It is important to note that our sample was primarily drawn from relatively developed areas of Pakistan rather than urban areas, and this factor should be taken into consideration when interpreting our study’s findings. In terms of demographics, our participants had an average age of 27.32 years, with a standard deviation of 9.51 years. Finally, we maintained an equal gender balance within our overall sample, with 150 men and 150 women.
At the outset, our study began with a total sample size of N = 347 individuals who participated in the survey. These participants were initially recruited using a convenient sampling method. Subsequently, we implemented a rigorous screening procedure to ensure the validity and reliability of the data collected. During this screening process, we identified and removed questionnaires with a significant percentage of missing data or those exhibiting low levels of participation. In total, 47 such cases were excluded from the dataset, further enhancing the overall data quality.
It is worth noting that Comrey and Lee (as cited in Pearson & Mundform, 2010) suggested that a sample size of 300 individuals is adequate for conducting exploratory factor analysis. Consequently, for this study, we made the deliberate decision to work with a final sample of precisely 300 individuals. This sample size was sufficient to meet the recommended criteria for conducting an exploratory factor analysis.
Results
A variety of data analytics is used to demonstrate the validity and reliability of this instrument. Following the standards of research, the 5-point Likert-type scale was handled as interval-scaled data (Norman, 2010). Analysis was carried out using IBM SPSS® version 21. Exploratory factor analysis was performed using principal axis factoring with promax rotation (see Table 1) because of their advantage over other extraction and rotation methods such as simpler statistical structure and realistic results (see Finch, 2006). KMO was 0.93 and Bartlett’s test of sphericity was 4046.62 (df = 465, p < .000) indicating the adequacy of this sample for factor analysis. This initial analysis produced five factors with the first factor accounting for 35.21% of the variance, and each subsequent factor explaining 6%, 3%, 2%, and 1% of the variance, respectively. Two frequently used criteria were taken into consideration when deciding which factors to keep. One of these was Kaiser’s (1960) renowned rule of the eigenvalue greater than one and in our case, five factors demonstrated this. Another was Cattell’s (1966) scree plot, which provided a graphical representation of the factors, and in this case, it showed a substantial drop after the fourth factor. These four factors were kept in scale after further examining the meaningfulness and significance of each one, and one was eliminated since it is incomprehensible and simply represents cross-loadings. To improve the validity of the resulting scale, only items with 0.3 or more loadings were retained (see Costello & Osborne, 2005). This process resulted in a 25-item scale with four subscales. These four factors were labeled based on their conceptual resemblance with domains identified from the interview. Four dimensions of jinn possession emerged: beliefs about signs of possession, beliefs about vulnerability and prevention from possession, beliefs about the conceptualization of possession, and non-believers constituting reverse-coded items. This final factor exhibits a negative correlation with the other factors and was included to identify individuals who do not hold beliefs in jinn possession. After this structural finalization, we proceeded to evaluate the internal consistency of BJPS using Cronbach’s alpha and omega total. The scale’s Cronbach’s alpha and McDonald’s omega coefficients were .92. Cronbach’s alpha was found as .90 for beliefs about signs of possession, .80 for vulnerability and preventive measures, .71 for beliefs about nature, and .74 for non-believers. Item total correlation for this scale was also computed for this scale which indicates very good discriminatory power of the items added to this scale and can be seen as evidence for the validity of the items of the scale.
Final items of the scale along with their factor loadings based on a principal axis factoring with promax rotation and psychometric properties for Belief in Jinn Possession Scale (BJPS; N = 300).
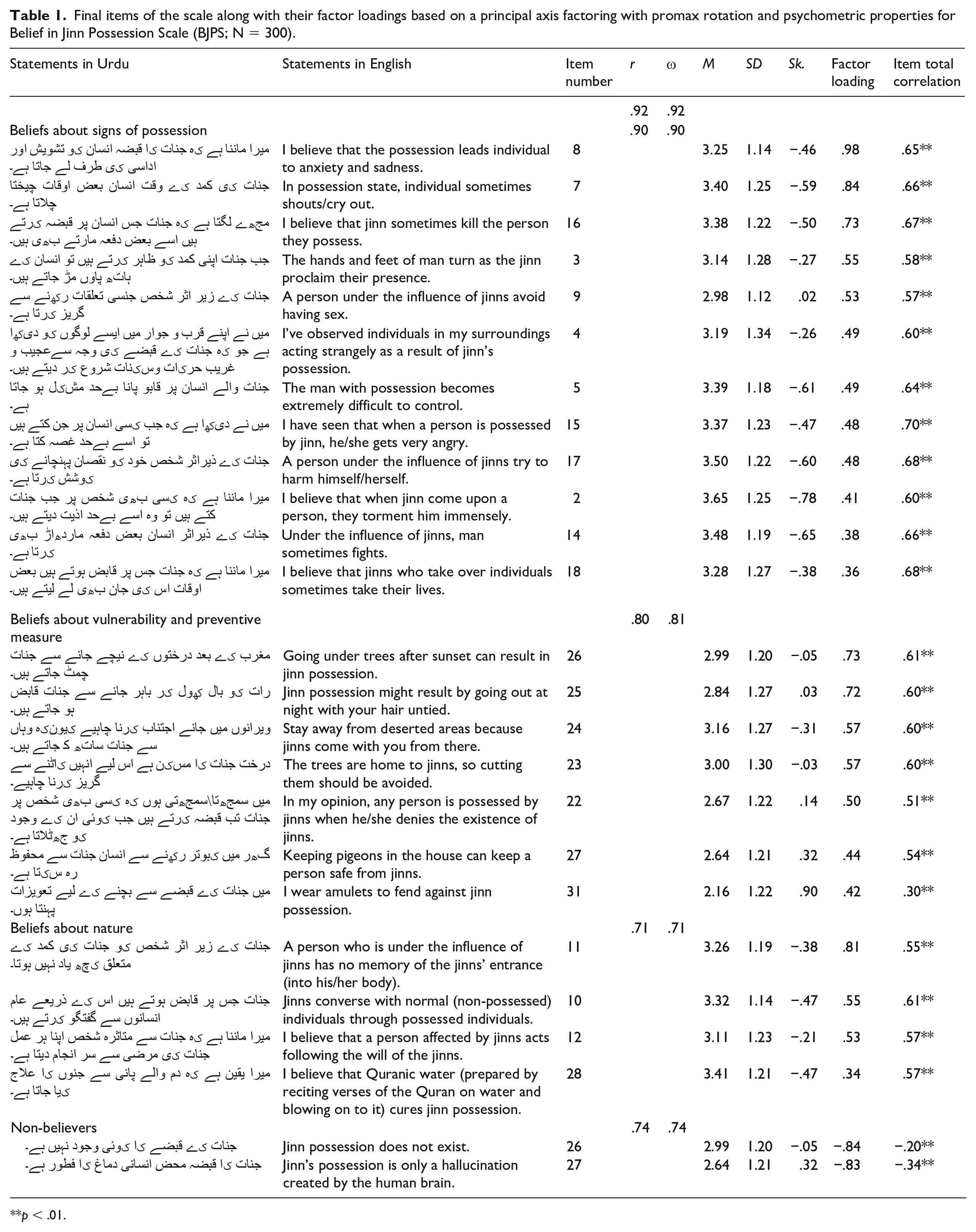
p < .01.
Study 2. Validation
Method
To provide the validity of the proposed model of jinn possession and to confirm the four-factor solution derived from exploratory factor analysis (EFA), confirmatory factor analysis (CFA) was performed on a new sample using Amos as it is user-friendly (Shek & Yu, 2014). It was anticipated that Study 2 would confirm the relationships between the items and factors that were explored. The data were normally distributed because the skewness and kurtosis values were less than 2 and 3, respectively; hence, a maximum likelihood estimate was performed (Chou & Bentler, 1995). We looked at the chi-square fit index to assess the fit of various models. We also included the Tucker–Lewis index (TLI), the root-mean-square error of approximation (RMSEA), and the standardized root-mean-square (SRMR) residual because the latter relies on sample size.
Sample
The sample encompasses N = 300 adult participants representing the community sample. 63.7% of the respondents identified as female and 36.3% as male. Most respondents identified (75.7%) their sect as Ahle Sunnat, followed by Deobandi and Barelvi (6%) and 3% Ahle Hadith and Ahle Tasheeh. The most commonly held education was postgraduate (38.8%). Others are either Graduates (37.5%) or the remaining respondents (23.4%). Participants reported an average age of 27.90 years (SD = 8.43 years).
Results
The results of the CFA with the hypothesized four-factor solution revealed that the model did not fit adequately (IFI = 0.88, TLI = 0.87, CFI = 0.88, and RMSEA = 0.74; see Hu & Bentler, 1999). Examination of the output resulted in the deletion of factor four from the scale and model modification. Factor 4 represents non-believers and contains reversed polarity items (see Table 2). Particularly, the reason that reverse items may be slightly more difficult to understand or comprehend (Swain et al., 2008) and contaminate the data’s covariance structure (Savalei & Falk, 2014) leads to the weakening of the overall psychometric properties of the scale. We once again used CFA to determine whether the three-factor model was preferable to the four-factor model. After the removal of the problematic factor, this time model was logically substantially better than the full four-factor model (IFI = 0.90, TLI = 0.88, CFI = 0.90, and RMSEA = 0.74). Yet, model fit indices are still below the specified threshold range recommended by the literature. To improve the model, the third factor was deleted as it was discovered that if any item of this scale was removed, the factor’s variance would turn negative which may be the representation of the Heywood case (see McDonald, 1985). Therefore, for this dataset, a two-factor solution is preferable over a three-factor structure (IFI = 0.91, TLI = 0.90, CFI = 0.91, and RMSEA = 0.07); nonetheless, the fit of Model 2 was still insufficient. Model 2 was further modified in accordance with the indices of the greatest values to provide a better fit for the data. These modification indices suggested that permitting error covariance between some of the items would improve the model’s fit to the data and items may covary because of the similarity between those items. Results indicated that after implementing this modification, Model 2a fits our data significantly better than Model 2 (IFI = 0.95, TLI = 0.94, CFI = 0.95, and RMSEA = 0.05). Moreover, the factor loadings obtained in Model 2a on all items are above 0.06. After the model fit was achieved, reliability analysis was conducted, and the Reliability value of the total scale and subscales ranged from 0.87 to 0.93, which again shows the soundness of this scale as a measurement tool. As presented in Table 3, the inter-factor correlations between the two factors are 0.68 (p < .01), suggesting that the factors are related to each other but do not overlap. In general, the moderate inters factor correlations, and the strong alpha values indicate that the scales’ items consistently measure the same latent construct. After establishing the validity of this scale, gender differences in belief in jinn possession were looked into. Women had a higher mean score than men regarding beliefs about jinn possession indicating that gender is strongly linked to paranormal beliefs and fears. These findings correspond with past studies on supernatural beliefs, which demonstrated that women are more inclined to hold such ideas (Irwin, 2009; Utinans et al., 2015).
Confirmatory factor analysis of BJPS (N = 300).
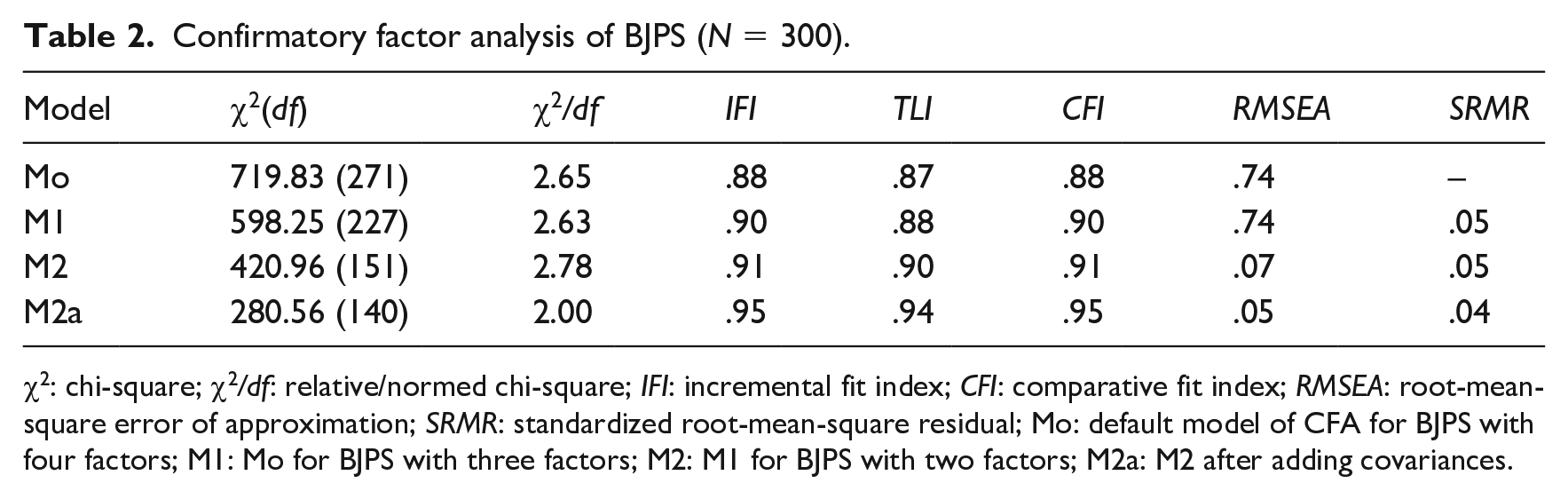
χ2: chi-square; χ2/df: relative/normed chi-square; IFI: incremental fit index; CFI: comparative fit index; RMSEA: root-mean-square error of approximation; SRMR: standardized root-mean-square residual; Mo: default model of CFA for BJPS with four factors; M1: Mo for BJPS with three factors; M2: M1 for BJPS with two factors; M2a: M2 after adding covariances.
Mean and standard deviations (SD), reliability, and inter-factor correlation on BJPS by gender (N = 300).
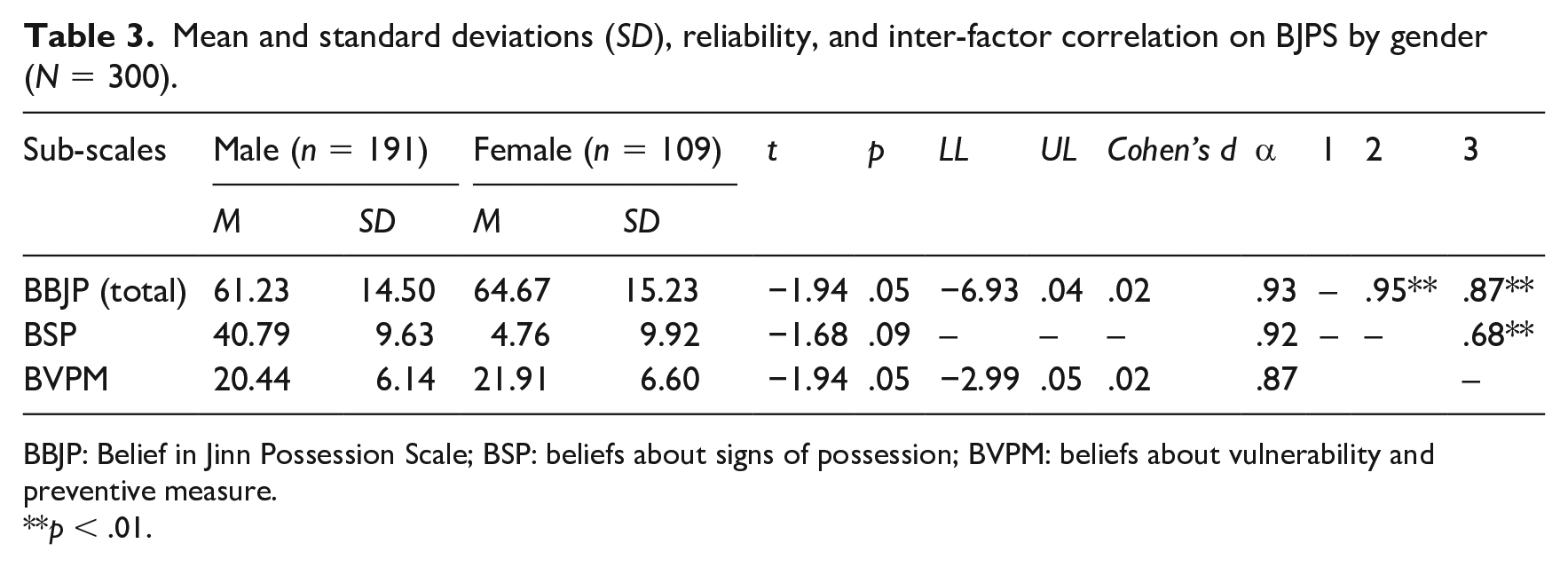
BBJP: Belief in Jinn Possession Scale; BSP: beliefs about signs of possession; BVPM: beliefs about vulnerability and preventive measure.
p < .01.
Study 3. Convergent validity and discriminant validity
Method
In this study, the convergent and discriminant validity of the BJPS were examined to make sure that the factor structure observed in previous studies was not a result of the survey’s design, the sample’s characteristics, or the way the data were collected (Johnson et al., 2011). Convergent validity is the way employed to evaluate how closely elements in the same construct correlate with one another (Campbell & Fiske, 1959). To provide convergent validity evidence of the BJPS, we examined its association with instruments measuring similar constructs among adults. Initially, we looked at the relationship between the BJPS and Paranormal and Supernatural Belief Scale (PSBS) (Dean et al., 2021) that assesses belief in paranormal phenomena. We also examined the association between BJPS and the Revised Paranormal Belief Scale (RPBS) (Tobacyk, 2004), and we anticipated that BJPS would be positively correlated with the PSBS and RPBS. For discriminant validity of BJPS, we run a correlation among BJPS with a Narcissistic Personality Inventory 16 (NPI-16) (Ames et al., 2006) and a Moral Identity Measure (MIM) (Aquino & Reed, 2002). Discriminant validity demonstrates that the scale for a particular concept does not correlate with other constructs (Malhotra, 2005).
Sample
Using a paper pencil-based self-report survey conducted, data from Pakistan were gathered. The data collection protocol was approved by the National Institute of Psychology, Islamabad, Pakistan, and all respondents provided consent before beginning the survey. The total sample size was 316 adults. The ages of respondents ranged from 18 to 68 (M = 34.22 years, SD = 11.79). Notably, 50% of the participants were male, and 50% were female. The majority (34.8%) had completed matriculation, 26.6% had barely finished intermediate, and 30% had completed 16 years of education or more.
Measures
The following questionnaires were distributed:
Belief in Jinn Possession Scale
See prior studies.
Revised Paranormal Belief Scale
An RPBS was developed by Tobacyk (2004) which measures the degree of paranormal belief in seven dimensions: traditional religious belief, extraordinary life forms, precognition, psi, superstition, spiritualism, and witchcraft. It constitutes 26 items with a 7-point Likert-type scale and from these, item number 23 is reverse-coded. This study had a reliability value of α = .95 which is acceptable.
Paranormal and Supernatural Belief Scale
The PSBS (Dean et al., 2021) has 13 items with a 4-point Likert-type scale. Items 7, 8, and 12 were reverse-coded. The alpha coefficient (α = .95) of the scale is acceptable in the original study. In this study, the reliability of this scale is α = .85.
Narcissistic Personality Inventory 16
Developed by Ames et al. (2006), it contains 16 items that were drawn from Raskin and Terry’s (1988) 40-item measure. The NPI-16 score was computed as the mean across the items with narcissism-consistent responses coded as 1 and narcissism-inconsistent responses coded as 0. The reliability of this scale in the original study was α = .78 and is α = .77. in this study.
Moral Identity Measure
The MIM was developed by Aquino and Reed (2002), and it contains 10 items with a 5-point Likert-type Scale. It measures two dimensions of moral identity, that is, internalization and symbolization. Cronbach’s alpha reliability of this scale in the original study was .85 (Aquino & Reed, 2002). In this study, the alpha coefficient of this scale is α = .71.
Results
Regarding the single scales included in Table 4, BJPS had a positive correlation (r = .66, p = .01) with RPBS and PSBS (r = .52, p = .01), indicating an overlap between the three scales. This supports the idea that independent measures of the same trait are associated, which gives evidence for convergent validity (Raedeke et al., 2013). Similarly, Table 4 represents no correlation between NPI-16 (r = .00, p = .01) and MIM (r = .66, p = .01).
Bivariate correlation and alpha coefficients on study variables.
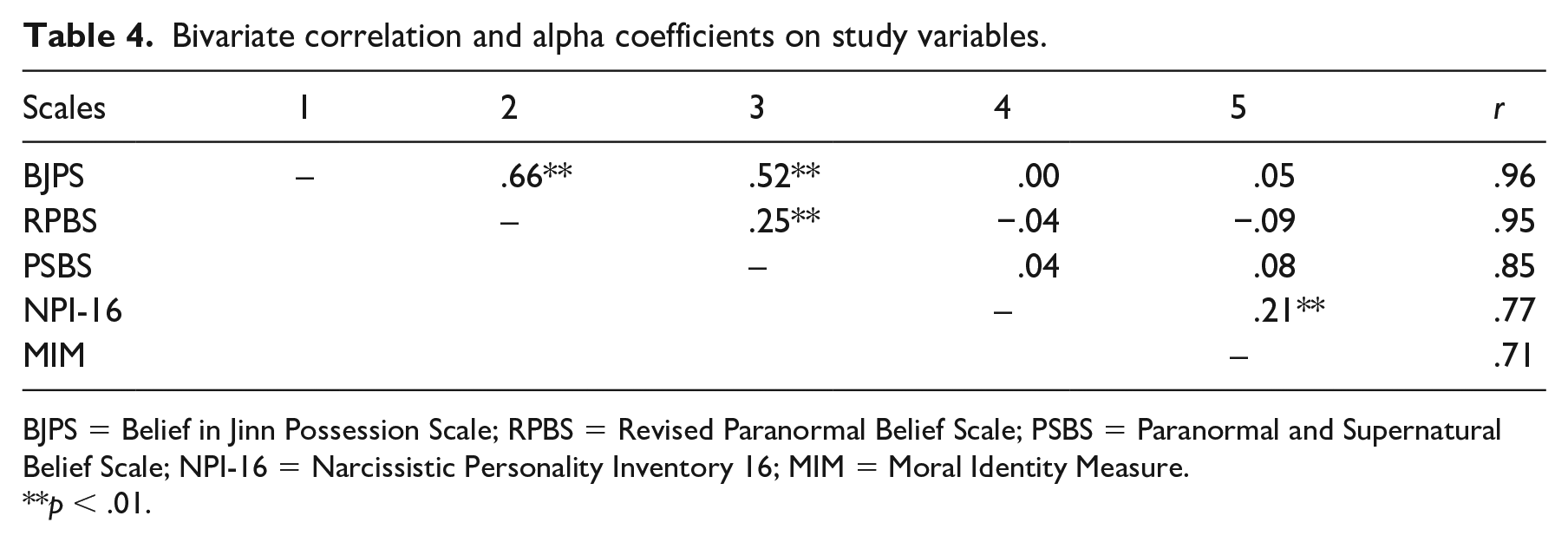
BJPS = Belief in Jinn Possession Scale; RPBS = Revised Paranormal Belief Scale; PSBS = Paranormal and Supernatural Belief Scale; NPI-16 = Narcissistic Personality Inventory 16; MIM = Moral Identity Measure.
p < .01.
Therefore, with these results, it was concluded that the discriminant validity issue did not exist in this study.
Discussion
The need for cultural awareness among clinicians working with patients from many cultures has increased because of rising globalization and migration (Hecker et al., 2016). There is no doubt that some diagnoses are easy to understand across cultures, whereas others need culturally and religiously relativist understanding of factors and beliefs such as paranormal beliefs that might influence the presentation, manifestation of symptoms, and help-seeking among individuals (Bakhshani et al., 2013; Bhavsar et al., 2016). Belief in jinn possession is one of the paranormal beliefs and as a construct is still in its infancy as there is not much empirical evidence available in the literature and particularly little has been written on its phenomenology in Pakistan. This study has reported the construction and validation of a measure of adult belief in the jinn possession scale to explore the local features, and explanations and to verify the local classification of spirit possession and is intended to fill in the gaps of existing knowledge. The study helps to understand the impact of culture on the presentation of clinically relevant symptoms that are essential to culturally sensitive treatment.
A set of studies on paranormal beliefs suggests that such beliefs are complex, multidimensional, and influenced by human experiences and understandings (see Sen & Yesilyurt, 2014). In this study, jinn possession is conceptualized as a multidimensional concept that encompasses a variety of beliefs, including beliefs about the symptoms of jinn possession, beliefs about how to prevent someone from becoming possessed, and beliefs about states that make a person susceptible to jinn possession. In the current study, the most common beliefs associated with possession as described by adults were collected and transformed into a 5-point rating scale given the name of the BJPS. In the first study, the exploratory analysis also confirmed that belief in jinn possession is also a multidimensional construct and yielded four factors. The first factor donates the indications and manifestations of states of possession. This factor constitutes the range of symptoms possession is often accompanied by such as anxiety, sadness, crying out, turning off the hands and feet, avoiding sex, acting strangely, rage, aggressive impulses, losing control, and suicidal tendencies. These states that can prompt a person to consider himself\herself possessed are linked with a variety of mental diseases as many disorders generally share these symptoms and studies confirm that possession states involve mental trauma for those affected and are linked to poor mental health (Berkowski & MacDonald, 2014). This might be the case because, in that cultural setting, having a diagnosis of the condition is more stigmatizing than being possessed (Ventriglio et al., 2018). They are thus given a discourse that enables them to give meaning to their distress and obtain assistance within the regionally accessible explanatory models and resources by attributing their psychological distress to possession.
The second factor consists of beliefs that indicate behaviors such as avoiding deserted regions and ceasing to speculate about the existence of jinns, all of which should be avoided to protect oneself against possession. This element essentially expresses believers’ unreasonable concerns and irrational fears associated with possession that may arise due to errors in reasoning caused by an emotional appeal (Irwin et al., 2012). Two items on this factor represent behaviors such as wearing amulets and keeping a pigeon as a pet are two actions that should be taken to obtain protection from supernatural beings. Exorcism, Dhikr, the use of natural remedies, consuming water laced with Quranic writing, and numerous other approaches are reported in earlier studies as therapy procedures for the supernatural (Saged et al., 2020) and the expulsion of jinn from the human being. Belief in such preventive or therapeutic approaches also discourages or postpones receiving psychotherapy and medical care for mental health issues.
The third factor constitutes beliefs about the general conceptualization of possession in local culture. It entails items portraying amnesia, loss of self-control, identity substitution, and treatment choices as a fundamental component of the possession construct. This idea of possession is fairly similar to the DSM-5 model of dissociative disorders in that it emphasizes amnesia and identity replacement (APA, 2013). Negatively phrased items that show a lack of belief in possession states make up the fourth factor. Because prior measures evaluating paranormal beliefs were criticized for lacking negatively worded items, this study intended to deal with this problem by constructing a scale that merges both positively and negatively phrased items (Dean et al., 2021). These four factors represent believers of jinn possession ranging from informed believers (whose views reflect a profound knowledge of paranormal events) to quasi-believers (whose opinions reflect a naive grasp of paranormal occurrences) (see Dean et al., 2021). In addition, this scale also considers the emotional and behavioral dimensions of beliefs in addition to the cognitive ones (see Marks, 2021). The findings also demonstrate the instrument’s satisfactory psychometric properties in terms of Cronbach’s alpha and McDonald’s omega (.80–.90). There is a general lack of multidimensional theoretical conceptualization or instrumentation for measuring belief in possession. By defining jinn possession as having multiple dimensions and by empirically validating this theoretical premise, the current work has made a theoretical contribution.
In the second study, CFA was further performed to validate the scale. In this process, two factors were deleted because the model did not reach a reasonable fit in their presence. The two-factor model shows that the data were consistent with the model and that the items had standardized loadings on the proposed latent factors. Therefore, the 19-item scores can be added together to reflect a person’s belief in possession, or each factor’s score can be calculated separately, with higher scores indicating a stronger belief. In the third study, the convergent and discriminant validity of this scale was established. The moderate correlation between the BJPS, the RPBS, and the PSBS reflects the shared constructs’ underlying commonality and provides evidence for their convergent validity. Moreover, no correlation of BJPS with NPI-16 and MIM suggests a substantial distinction between these constructs which provides us with discriminant validity of the scale. The results imply that the use of the BJPS Scale as a standard measurement would be especially helpful in evaluating a person’s explanatory model of illness to fully comprehend the diagnosis and develop tailored treatment regimens.
Implications and limitations
Due to the unique context in Pakistan and the idiosyncrasy of our sample, the generalizability of this study is restricted. Cross-cultural evaluation and validation for a broader population must be confirmed. Experts should collect additional data from clinical populations as well. Other studies are required to examine other psychometric features of this instrument, such as the test–retest reliability of BJPS scores. Despite several limitations, provides more evidence in favor of the idea that improving our comprehension of pathological spirit possession in different cultural contexts is crucial for providing mental health treatment (Van Duijl et al., 2014). Clinician who wants their patients to entrust them and to help them feel more understood could use the BJPS Scale to gain a better understanding of their patient concerning how they react to their illness, and this would help the clinician to better fulfill their clinician’s needs by using more efficient methods multiple-component treatment strategies. Moving forward, these results provide practical guidance for professionals supporting Muslim communities. However, further investigation is required to look into how such an interpretation might be acknowledged and handled in psychological practices in Western societies to optimally assist Muslim people. In conclusion, this research adds to the growing body of knowledge and awareness of the concept of possession in non-Western societies.