
Abstract
This study explored the nature of mental health stigma within communities and its impact on mothers of children diagnosed with attention-deficit/hyperactivity disorder. A qualitative research design was employed, using purposive and snowball sampling to recruit ten mothers of children with attention-deficit/hyperactivity disorder. Data were collected through semi-structured, face-to-face interviews and analysed using thematic analysis. Findings revealed that mothers frequently encountered judgement and stigma from both community members and within their own families. These negative experiences significantly influenced their attitudes towards treatment and, in some cases, contributed to the decision to discontinue their child’s pharmacological intervention. The study highlights the role of social stigma in shaping treatment decisions and underscores the need for greater mental health awareness and support for caregivers.
Introduction
Stigma related to mental illness and the use of both pharmacological and psychological treatment is universal (Abolfotouh et al., 2019; Vaishnav et al., 2023). Stigma can be societal, organisational, or individual (Zhang et al., 2021). Stigma is more likely to affect vulnerable groups, such as children, adolescents, the elderly, and gender minorities (Murthy, 2022). Sociocultural elements, whether macro or micro, determine the extent of stigma and the detrimental effects thereof. Stigma around mental health is linked to more severe psychological issues in the individuals, less access to mental health services and poor treatment compliance (Vaishnav et al., 2023). This study will unpack and provide evidence as to how stigma in low-socioeconomic communities can have an effect on children with attention-deficit/hyperactivity disorder (ADHD) and their caregivers.
Despite the increasing prevalence of mental disorders (Monnapula-Mazabane & Petersen, 2021; World Health Organization, 2022) and improved public attitudes, mental health still receives limited attention in health care services, and ignorance and stigma persist (Angermeyer et al., 2017; Karaffa & Koch, 2016). Community attitudes significantly impact treatment success, social reintegration, help-seeking behaviours, and knowledge of drug treatment (Mckenna et al., 2024). Compliance with medication can be negatively affected by community beliefs about mental illness, such as ADHD (Furnham & Swami, 2018). Poor symptom recognition and preference for self-help over professional mental health care treatment influence help-seeking, particularly in parents and children (Furnham & Swami, 2018). Disparities between public and professional views on therapy also affect treatment adherence (Furnham & Swami, 2018).
The stigma attached to mental illness causes more distress for individuals, as individuals with mental illness face stigma related to mental health and illness in addition to the negative effects of their psychiatric illness (Vaishnav et al., 2023; Zhang et al., 2021). In addition, the emergence, maintenance, and negative consequences of stigma are also significantly influenced by cultural factors (Zhang et al., 2021). Research indicates that beliefs about mental illness differ between countries and cultures (Ahmad & Koncsol, 2022; Fekih-Romdhane et al., 2023; Zhang et al., 2021).
Stigma towards mental illness
‘Associate stigma’ refers to prejudice and discrimination towards those without mental illness due to their connections with individuals diagnosed with a mental illness (Quinn et al., 2015). When family members internalise this stigma, it becomes ‘affiliate stigma’ (Mak & Cheung, 2012). Nxumalo and Mchunu (2017) found that families of individuals with mental illness often experience stigma, poor self-esteem, and anger. Internalised stigma and self-stigma are two other types of stigma that cause people to feel guilty about their mental illness and place the responsibility on themselves (Africa–Elizabeth & Njararuhi, 2024). Self-stigmatised individuals may have a reduced sense of self-worth and self-acceptance and believe they are not important (Chan et al., 2022). In addition, they could see their identities more negatively and feel ashamed, humiliated, and dissatisfied in themselves for having a mental illness (Chan et al., 2022). Specifically, they might avoid social situations and show signs of social disengagement to keep their mental health diagnosis and symptoms from being revealed (Chan et al., 2022).
Cultural backgrounds significantly shape the stigma associated with ADHD (Mueller et al., 2012). While the grassroots campaigns in Ghana and Kenya have aimed to reduce stigma (Potts & Henderson, 2021), few global interventions focus on stigma reduction for family carers (Morgan et al., 2018). Only 3% of stigma interventions in low-income countries address mental health, with most focusing on HIV/AIDS (Kemp et al., 2019). Research suggests Africans hold more stigmatising views towards mental illness (Abdullah & Brown, 2011). This stigma impacts help-seeking behaviours, particularly in South Africa, where cultural diversity influences perceptions of ADHD (Gómez-Benito et al., 2019; Truter et al., 2018). Many South Africans are reluctant to discuss mental illnesses, leading to misunderstandings, such as labelling a child’s behaviour as ‘naughty’ without considering conditions like ADHD (Dosreis et al., 2010; Voges, 2021).
Attention-deficit/hyperactivity disorder as a mental illness
Attention-deficit/hyperactivity disorder (ADHD) is a neurodevelopmental disorder marked by inattention, hyperactivity, and impulsivity (Rivas-Vazquez et al., 2023). Globally, the prevalence of Attention-Deficit/Hyperactivity Disorder (ADHD) varies, with most studies estimating that it affects approximately 5%–7% of children and 2.5%–4% of adults (World Health Organization, 2024). ADHD is more prevalent in males than females (American Psychiatric Association, 2022), and the disorder often coexists with other conditions (Boland, 2021).
Metzger and Hamilton (2021) highlight the prevalence, stigma, and impact of ADHD diagnoses in schools, particularly regarding teacher perceptions and biases. Students diagnosed with ADHD often faced negative stereotypes and social rejection (Metzger and Hamilton, 2021). While an ADHD diagnosis provides access to additional support in high income countries, it may also lead to stigma and lower teacher expectations. Even when there is little evidence to support these preconceptions, teachers may view ADHD pupils as disruptive or uninterested, potentially due to implicit biases, including cultural prejudices (Metzger and Hamilton, 2021). This is a response that aligns with modified labelling theory, which emphasises how stigma after a diagnosis can lead to disadvantages in social environments, work, and education (Voges, 2021).
Research on ADHD in South Africa is limited compared with other countries. However, some studies suggest that the prevalence in South African children is similar to global estimates, falling between 5% and 10% (World Health Organization, 2024). It is important to note that differences in health care access, cultural perceptions, and diagnostic practices can influence the reported prevalence rates in various regions within the country (Boland, 2021; World Health Organization, 2024). In South Africa, apartheid has contributed to disparities in public and private health care, leading to a 75% treatment gap for mental illnesses (Egbe et al., 2014). Stigma from medical professionals may worsen this gap (Egbe et al., 2014). While pharmaceuticals are commonly used, medication alone is not fully effective; combining stimulant medication with behavioural therapy can reduce ADHD symptoms (Sprich et al., 2015; Toomey et al., 2012).
The present study is based on Bowen’s (1979/1985) family systems theory, which views the family as an interconnected emotional unit. The theory emphasises studying individuals within the family context rather than in isolation, focusing on how children’s health impacts sibling behaviour, caregiver stress, and family functioning (Wilson, 2021). Bowen’s theory has been applied to cultural differences, relevant to South Africa’s diverse family structures, which often extend beyond the nuclear family. This study used Bowen’s theory to explore mental health stigma in low-socioeconomic communities and its effects on children with ADHD and their caregivers.
Methods
Research design
This study employed a qualitative descriptive design, appropriate for capturing participants’ experiences in a clear and comprehensive manner (Colorafi & Evans, 2016). This approach aligned with the study’s aim of exploring the nature of mental health stigma within communities and its impact on mothers of children diagnosed with ADHD.
Sampling
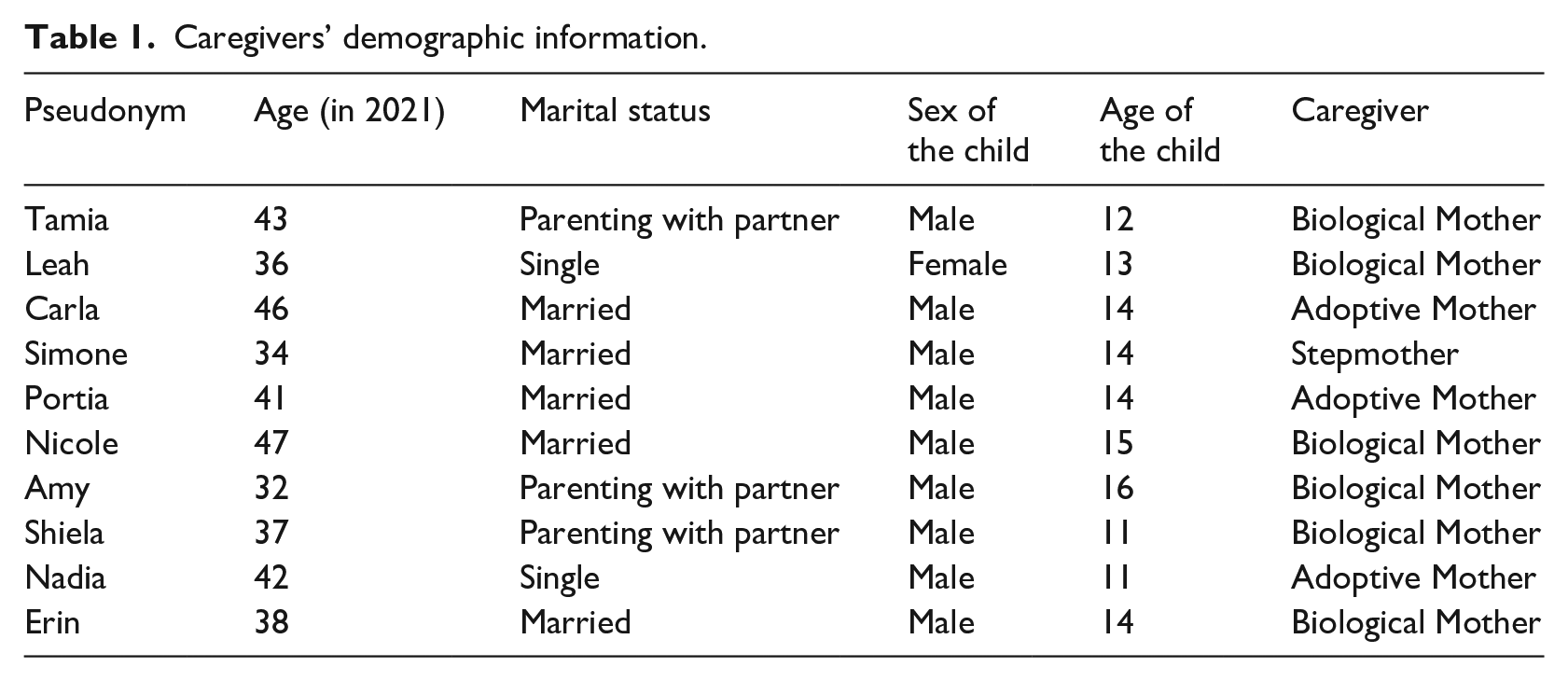
This study used a qualitative methodological approach with a total of 10 participants who were purposively selected from various communities across Cape Town. Participants were eligible for inclusion in the study if they were the primary caregiver (biological mother, stepmother, adoptive mother) of a child diagnosed with ADHD. The snowball sampling technique was used to recruit participants, where the initial participants were asked to recommend another potential participant who also met the inclusion criteria (Babbie, 2013). Due to the difficulty of recruiting participants who were open to and willing to participate in the study, the snowball sampling technique assisted in gaining participants, as caregivers recommended relatives and friends when asked if they were familiar with any additional person who fit the inclusion criteria of the study. Participants in this study were the primary caregivers (biological, adoptive, and stepmothers) of children diagnosed with ADHD, as shown in Table 1. The females were aged between 32 and 47 years. The children were mostly males aged between 11 and 16 years.
Caregivers’ demographic information.
Procedure and data collection
Participants were recruited using the snowball method. All data were collected by the first author who at the time of data collection, was a registered research psychology student with the Health Professions Council of South Africa (HPCSA). All interviews were once-off, however the researcher kept maintaining contact with the participants to share updates about the research study. Data were collected through semi-structured interviews which were conducted through online video platforms, such as WhatsApp video calls and Google Meet. The data were collected between the period of July 2021 and October 2021. Prior to the interview, an information sheet and consent form were sent to participants via WhatsApp or email. The information sheet detailed the research topic, the aim of the study, the research design, the data collection method, and the participant’s ethical rights. The consent form when signed, limited permission for the use of shared information. Interested participants were contacted to arrange a phone call for further discussion and to answer any questions. Consent was obtained, and participants were informed of their right to withdraw at any time. The interview guide covered questions related to the mother’s experience since learning their child’s diagnosis, the family history, the family dynamics, and their support system. The interviews were audio-recorded, transcribed manually by the researcher and stored on a password-protected computer. All interviews were conducted in English. Although participants were given the option to be interviewed in Afrikaans or isiXhosa, none requested it. The researcher ensured the information was relevant and unbiased, focusing on four key aspects of trustworthiness: credibility, dependability, confirmability, and transferability (Haq et al., 2023). Credibility was achieved by confirming participants’ responses during and after the interviews to ensure accuracy (Pandey & Patnaik, 2014). Dependability was maintained through regular meetings with research supervisors and quality evaluations of data collection. Confirmability involved an audit trail to ensure the results reflected participants’ responses, not the researcher’s biases. Finally, transferability was ensured by providing a detailed description of the final results (Pandey & Patnaik, 2014).
Reflexivity statement
As the lead researcher, the first author recognised their position as a young woman without children or direct experience with ADHD might make the first author appear as an ‘outsider’ to participants. To minimise bias and misinterpretations, the first author employed regular personal reflection throughout the research process, focusing on their attitudes towards ADHD, medication, parenting, and sociocultural decision-making.
Data analysis
The data were analysed using reflexive thematic analysis, as outlined by Braun and Clarke (2006, 2019), which involves an iterative, researcher-driven process of coding and theme development. This approach was appropriate as it allowed for inductive generation of codes and construction of themes through deep engagement with the data, acknowledging the active role of the researcher in meaning-making. The ATLAS.ti software was used for data management through the data analysis process. The researcher began by transcribing the interviews and reading each transcript while taking notes. In steps two and three, codes were identified, and potential themes were explored using the ATLAS.ti software. As analysis continued, codes were adjusted based on data elements. In step four, themes were reviewed to ensure they accurately reflected the data, with any overlooked themes added. Step five involved naming and defining themes in alignment with the research questions. Finally, step six involved producing the report, using extracts from ATLAS.ti software.
Ethical considerations
Ethics approval (HS21/5/22) was obtained from the Humanities and Social Sciences Research Ethics Committee (HSSREC) at the University of the Western Cape (UWC). All participants provided informed consent. Participants were informed of their rights during the research process. Data were kept private and processed according to the Protection of Personal Information Act (Staunton et al., 2020).
Results
Information regarding stigma towards mental health, particularly mothers of children with ADHD, was revealed through the analysis of the semi-structured interview transcripts. Based on the participants’ responses, three major themes were developed: disapproval of pharmaceutical usage for ADHD, stigma towards mental illness in the low socio-economic communities and support systems. Notably, the mothers in this study had completely discontinued medication, were in the process of discontinuation, while others have implemented periods of non-medication. Seven mothers had completely discontinued their child’s medication and three mothers were in the weaning off process at the time of data collection (Botha, 2022).
Disapproval of pharmaceutical usage for mental illnesses
Judgements that parents and children frequently felt resulted in the discontinuation of the child’s ADHD medication. Participants’ children received a professional diagnosis of ADHD between the ages of 4 and 7 years old. Mothers shared their struggles in dealing with relatives who were wary of their child’s oral medication consumption. The concern here was regarding medication used to treat ADHD and that a child would become dependent on the medication, and consequently be unable to cope without it. Since addictive behaviours were fairly common in their families, one caregiver recalled that her family was wary. Consequently, out of concern that the child may become drug dependent, parents chose to discontinue treatment:
My family was very against me, putting him on meds in the first place because addiction runs in my family, and they would say that I am giving him cocaine . . . so it was hectic, so I had a lot to deal with. (Shiela)
Since addictive behaviours were prevalent in Shiela’s family history, the family viewed medication as a threat and feared that the child may grow reliant on it. Another parent described a similar situation, in which family members stigmatised the child for taking medication as they were hesitant about the medication use:
I have seen many people who are so against the use of medication, and even with family members, I had so many arguments with them that I do not bring it up now because there is like this huge stigma attached to taking medication. (Tamia)
Tamia felt that her family and close friends had developed a stigma against medication use to treat her child’s ADHD symptoms. Caregivers stopped treatment owing to the stigmatisation from family and community members. Meanwhile, another mother shared her own beliefs regarding the treatment of her child:
My husband and I do not want him to be on this stuff [medication] for the rest of his life. He must try to get used to being his own self, we want to see how he is gonna be his own self. (Nicole)
Nicole’s pre-conceived belief regarding medication use reflected her past experiences with medication as a treatment choice for her child. This could indicate negative experiences with the side effects, or the family’s stigma towards the treatment. Consequently, parents sought alternative treatment types or methods to avoid medication use, and, ultimately, ostracism from their family and friends:
We started an exercise regime. I live close to a sports field so we could go every evening. Where he could go run to his heart’s content. We make sure that he exercises daily, we will make sure that he is involved in sports at school, in a lot of activities. (Tamia)
Alternative interventions, such as sports and extracurricular activities, were common replacements for many mothers. They believed that exercising was a more natural method for the child to cope with the different symptoms associated with ADHD. This resulted in a happier child and mother, and consequently, lesser judgement from outsiders. Most parents mentioned that their child was stigmatised by their own relatives and called ‘naughty’ or ‘lazy’ while in reality they exhibited symptoms of ADHD. An initial sentiment of denial of ADHD as a legitimate disorder was typical within the family and cultural systems, as shown by the demographics:
Coming from a colored household they always used to say he is just naughty, or he is lazy. And I thought there was something wrong and a doctor supported me a lot and then I realised that this is all very normal [within ADHD]. (Nadia)
Family members assumed that since ADHD was not a legitimate diagnosis, no medication was required. Consequently, family members were wary of medication use, since some did not see it as a treatment for ADHD symptoms, rather as a way to control the child’s disruptive behaviour. The behaviour of one caregiver’s child was perceived as typical boy behaviour based on her cultural background, although this was not how she felt. With the help of a doctor, she realised that the behaviour her son displayed was typical of a child of his age who exhibited indications of ADHD, rather than being labelled as lazy and misbehaving.
The mothers reported having encounters with peers, community members, and family members who were highly vocal and hostile towards their views on ADHD as a mental illness. These individuals criticised the mother’s choices for their children’s pharmacological treatment, accusing them of over-medicating and passing judgement on their treatment choices. It was noted that the participants’ families were apprehensive about the pharmacological treatment prescribed to the children, creating internal conflict for the mothers about whether to continue or discontinue the pharmacological treatment.
Stigma towards mental illness
Parents and their children endured judgement and critique from their families and friends. Children themselves were stigmatised and bullied at schools for playing and working differently than their peers. They were uninvited to family gatherings as they were seen as disruptive in social settings. This often led to mothers being seen as not being in control of their children’s behaviour:
And they [the family] would say they do not want to be rude but do not bring him again [to family gatherings]. (Nadia) At the beginning of the year, he was bullied by a boy in his class, but he immediately came to tell us. (Carla)
A distinction must be made between the stigma directed towards children diagnosed with ADHD and the stigma experienced by their mothers in relation to their parenting. While children may be labelled, excluded, or misunderstood due to their diagnosis and associated behaviours, mothers often face a parallel form of stigma rooted in societal judgements about their parenting competence. This maternal stigma is shaped by perceptions that behavioural difficulties in the child reflect poor parenting, leading to blame, scrutiny, and social isolation. In this study, both forms of stigma were evident: children were subjected to peer rejection and negative stereotyping, while mothers reported feeling judged or dismissed by educators, family members, and the broader community. These intersecting experiences of stigma reinforce one another and contribute to the emotional and relational burden carried by both the child and the mother.
Support systems
The mothers interviewed in this study all had different ways of managing their experiences. The mothers mentioned they had their families as support systems to help them cope with pressures and take charge when they needed to take a step back. Their support systems varied from husbands, sisters and direct family members, who helped them manage the criticism, judgement, and stigmatisation. These mothers were able to talk to their support systems and ask for advice, help to carry the load of motherhood, and all the responsibilities that came with it:
My support system include my sisters. With him it is not parents alone raising him it is a village. He must be watched closely. (Shiela) I come from a very supportive family, I come from a family of teachers. My sister is a social care manager, so she works with patients with autism, and she has quite a lot of knowledge, so I had a lot of really strong support. (Tamia) I have a very hands-on husband, very supportive. (Erin)
Although the mothers experienced stigmatisation from their families and surrounding community members as their children did not behave in the conventional way expected in society, their support systems helped them persevere and prioritise their child’s health and well-being over others’ judgement and expectations.
Discussion
This study highlights the emotionally complex and socially charged experiences of mothers navigating ADHD diagnoses and treatment decisions for their children. While mothers held the primary responsibility for initiating and maintaining treatment, these decisions were often influenced by social pressures and family judgements, particularly regarding the use of medication. In line with previous research (Dosreis et al., 2010; Leitch et al., 2019), participants reported experiencing high levels of stress resulting from external criticisms about their parenting, their child’s behaviour, and their decision to pursue pharmacological treatment. These experiences were deeply personal, often evoking feelings of shame, anxiety, and isolation.
Emotional impact on mothers and parenting
The emotional burden carried by mothers was compounded by the stigma surrounding both mental health and ADHD. Participants described being scrutinised by extended family, friends, school staff, and even health care professionals. These perceived and actual judgements contributed to chronic self-doubt and, in some cases, led to mothers discontinuing or delaying medical treatment. This mirrors findings from Shahwan et al. (2022) and Singh (2004), who documented how caregiver decisions are shaped by social stigma and contested notions of ‘good mothering’ in the context of mental health care.
Mothers in this study often felt compelled to ‘defend’ their child’s diagnosis and treatment needs, particularly in households where there were fears of overmedicalisation or a family history of substance use. These anxieties sometimes led to a reluctance to use stimulant medication, even when it proved effective, echoing Bussing et al.’s (2003) and Gough and Novikova’s (2020) observations on families preferring informal, non-pharmacological strategies due to mistrust of medical advice or fear of social judgement. This reluctance was not simply a matter of individual choice but a reflection of broader societal narratives about medicalisation, childhood behaviour, and parenting responsibility.
These pressures, compounded by inadequate support systems, had a clear toll on mothers’ emotional well-being. Many reported persistent guilt, emotional fatigue, and feelings of helplessness. Such experiences align with the concept of ‘caregiver burden’ widely discussed in the literature (Harborne et al., 2004; Mueller et al., 2012) and raise concerns about long-term maternal mental health. This emotional exhaustion can affect caregiving quality, disrupt attachment, and reduce the consistency of support provided to children.
Distinct but intersecting stigmas
A key finding of this study is the dual stigma operating at different levels: stigma directed at the child due to the ADHD diagnosis and behaviours, and stigma directed at the mother for perceived parenting failures. While previous studies have often focused on either child or caregiver experiences in isolation, the current findings underscore how these stigmas are interlinked and mutually reinforcing. Children may experience exclusion or stereotyping, while mothers are blamed for their child’s perceived lack of discipline or behavioural issues (Kendall et al., 2003; Norvilitis et al., 2002). This distinction is important for intervention, as each form of stigma requires a different point of entry: public education for child-focused stigma, and targeted parent support and professional sensitivity for caregiver-related stigma.
Impact on childrearing and family dynamics
The study also showed that stigma and familial disapproval directly impacted parenting strategies and family dynamics. Although mothers attempted to support their children through positive coping mechanisms such as engagement in sports, social activities, and alternative therapies these efforts were frequently met with criticism from extended family members or school personnel. As noted by Klassen et al. (2006), such interference can undermine parental confidence and disrupt family cohesion.
When treatment decisions are shaped more by social perceptions than by clinical indicators, children may not receive the consistent care they need. Research has long indicated that parental ambivalence can negatively affect treatment adherence and child outcomes (Barkley & Murphy, 2006; Brinkman et al., 2009). In this context, children may internalise stigma, perceive themselves as ‘problems’, or resist intervention efforts. The compounding effect of inconsistent support and emotional tension at home could worsen symptoms related to emotional regulation, academic performance, and social relationships (Sciberras et al., 2011).
Community awareness and the role of stigma
A consistent theme in participant narratives was the limited understanding of ADHD within their communities. Misattributions of ADHD symptoms to poor discipline or bad parenting were common, reinforcing stigma and deterring help-seeking. This aligns with Renwick et al. (2024) and other work showing that lack of mental health literacy contributes to underdiagnosis, delayed intervention, and greater caregiver burden (Sayal et al., 2006).
These findings reinforce the importance of community-based mental health literacy campaigns aimed at improving awareness and reducing stigma. In addition, professional training is essential to equip teachers and health care workers with the skills to support rather than judge families navigating ADHD care. As this study illustrates, improving the broader social environment can reduce the psychosocial load on families and create more enabling conditions for effective intervention.
The growing literature on caregiver experiences of ADHD by drawing attention to the dual stigma experienced by both mothers and their children. It deepens our understanding of how social judgement not only affects health care decisions but also shapes family dynamics and emotional well-being. Importantly, it highlights the need for systemic responses, including education, training, and support systems, that attend to both the clinical and relational dimensions of ADHD care.
This study was limited to the perspectives of mothers, as no fathers volunteered to participate. While the focus on maternal experiences offers valuable insight, future studies should seek to explore the perspectives of fathers and other caregivers to better understand the broader family dynamics at play. In addition, given the small sample size, these findings cannot be generalised to all parents of children with ADHD. Nonetheless, the study provides important qualitative insights into the lived realities of caregiving under conditions of stigma and uncertainty. Notably, participants expressed gratitude for the support of partners, sisters, and direct family members, underscoring the protective value of social support. Future research could further explore how positive support networks buffer against the negative impacts of stigma and judgement.
Conclusion
The study underscores the far-reaching impact of stigma on the emotional well-being of mothers caring for children with ADHD. Stigma influenced not only how mothers felt about themselves and their children but also the choices they made around treatment and parenting. These decisions, in turn, affected their children’s development and access to support. A more informed and compassionate public discourse around ADHD grounded in accurate knowledge and cultural sensitivity is urgently needed. Creating community environments that empower rather than shame parents may significantly improve both parental well-being and child outcomes.
Footnotes
Acknowledgements
The authors would like to acknowledge the participants who shared their stories and experiences with us.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded through the National Research Foundation (NRF).