
Abstract
Technologically assisted interventions offer significant opportunities for treating various psychological and neurological symptoms and disorders. This may improve learning experiences, social interactions, and assist patient rehabilitation. This study explored primary research on these interventions in South Africa from 2006 to 2021. Using specific inclusion and exclusion criteria and the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews search strategy, 14 databases were searched, resulting in 13 studies reviewed. Five trends (geographic location, year of publication, sample size, modality of technologically assisted intervention, medium of mHealth intervention, and treatment support) and five themes (technological efficacy, adoption, accessibility, and barriers, ethical considerations in digital interventions, community support, emotional connection, and psychological meaning, and gratitude hope) emerged following a thematic analysis of the reviewed studies. The importance of understanding healthcare system limitations is underscored by the national focus on the Fourth Industrial Revolution, the burden of disease, and health inequalities in rural or smaller urban areas that lack specialists. This study provides an overview of the South African landscape of technologically assisted interventions in psychological and neurological applied areas, and highlights the trends and themes that have emerged. It also provides a foundation for further research on the potential of technologically assisted interventions to enhance South Africa’s healthcare outcomes.
Keywords
Technologically assisted interventions are evolving tools in healthcare, encompassing a range of digital modalities that deliver evidence-based care for psychological and neurological conditions (Holmes et al., 2019; Wiederhold & Bouchard, 2014). These interventions include mobile health (mHealth), telemonitoring platforms, robotics, virtual environments, brain–computer interfaces (BCIs), neurofeedback, virtual reality (VR), and deep brain stimulation (DBS). Importantly, technologies are defined not only by their format, but also by how they facilitate therapeutic engagement, monitoring, and communication.
The origins of technology in healthcare trace back to the 1920s, when the term eHealth was coined to describe cost-effective and efficient healthcare delivery supported by innovation (Rooij & Marsh, 2016). Telemedicine, a term often used interchangeably with eHealth, mHealth, and digital medicine, specifically refers to delivering care remotely, particularly to underserved or rural communities (Rooij & Marsh, 2016). Notable early uses include consultations via Morse code in Australia (1929) and medication support in Canadian remote areas (1942) (Kuzel et al., 2012; Terry et al., 2014). The digitalisation of healthcare continued with the introduction of electronic health records in the early 1990s (Sjöström et al., 2014).
Telemedicine software, or virtual health platforms, now incorporate video conferencing tools like Zoom, Microsoft Teams, and Google Duo to deliver care remotely (Kaminski, 2020). These platforms improved patient access, reduced assessment times, and enhanced public health communication, while cutting sanitation and facility costs (Vidal-Alaball et al., 2020). Usability-focused interventions, such as the iterative design of eating disorder programmes, have demonstrated improved adherence and patient motivation (Nitsch et al., 2016). This review pays particular attention to telemonitoring – where patients manage health conditions from home with digital support – as well as mHealth tools delivered via mobile applications and integrated computer sciences. For clarity, this review defines: Telemedicine as remote clinical care using digital platforms; mHealth as mobile health tools delivered via mobile devices (e.g., applications, SMS); Mobile applications as software installed on mobile devices for healthcare use; Multimedia technology as platforms integrating audio-visual content to support care or education.
Beyond clinical delivery, these technologies have been incorporated into remote education and patient training programmes. Though widely used in response to COVID-19 (Bokolo, 2021; Carrillo & Flores, 2020; Tadesse & Muluye, 2020), digital education platforms are not the focus of this review. Instead, the review concentrates on how these technologies are applied in clinical and rehabilitative contexts to support individuals with psychological and neurological challenges.
There has been growing global integration of these interventions to complement pharmacological and therapeutic approaches and support rehabilitation (Howard, 2017; Thurner et al., 2020). For instance, robotics and brain stimulation offer personalised care in neurorehabilitation (Masiero et al., 2014; Mehrholz et al., 2020; Morone et al., 2017; Semprini et al., 2018). Similarly, BCI, neurofeedback and VR have improved outcomes in conditions such as attention-deficit/hyperactivity disorder (ADHD) and depression (Botella et al., 2017). While DBS is a well-established for movement disorders, its psychiatric applications remain limited (Anderson et al., 2017; Denys et al., 2010).
Barriers to conventional healthcare, including geographic and financial constraints, have prompted interest in these accessible, flexible, and often cost-effective interventions (Franz et al., 2017; Opriş et al., 2012). These technologies offer ongoing advantages such as scalability, continuity of care in remote areas, as well as the capacity to deliver personalised interventions with limited physical infrastructure. Contexts such as South Africa’s dual burden of disease and resource scarcity underscore the need for such scalable, evidence-based digital interventions (Hofman & Madhi, 2020). Nonetheless, utilisation remains low due to insufficient training, limited funding, and a lack of comprehensive mental health policies (Patel et al., 2018; Pillay, 2019).
With the Fourth Industrial Revolution (4IR) driving technological innovation, there is increased interest in applying advanced tools like VR and neurotechnology in clinical settings (Olaitan et al., 2021; Schwab, 2017). Despite this momentum, South African literature on the implementation and effectiveness of such tools remains sparse (Liebenberg, 2021). In response, this scoping review seeks to systematically map existing evidence on technologically assisted interventions in South Africa and highlight directions for future research.
Method
This study’s methodology follows the Joanna Briggs Institute (JBI) guidelines for scoping reviews and the framework by Arksey and O’Malley (2005). Reporting adheres to the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) checklist and the four-phase flow diagram for scoping reviews (Levac et al., 2010; Tricco et al., 2018). To enhance rigour, a peer rater was involved throughout the appraisal and inclusion process. The guiding research question was: What technologically assisted interventions have been utilised in South Africa for neurological and psychological outcomes?
Ethical considerations
The researcher gathered data ethically by refraining from plagiarism, using any illegal sites and pirated articles, and following scoping review protocols in a transparent manner, enhancing replicability. According to Peters et al. (2020), it is not required for scoping review protocols to be registered; however, ethical clearance (HUM008/0721) was obtained from the Faculty of Humanities Postgraduate Research Ethics Committee at the University of Pretoria.
Data collection
Inclusion and exclusion criteria were based on existing literature covering healthcare services and sciences, neurosciences, clinical neurology, psychology, and neurorehabilitation. A broad range of academic sources was considered, irrespective of publication status. These included qualitative, quantitative, and mixed-methods studies, as well as editorials, case studies, guidelines, research agendas, and letters. Grey literature, including both published and unpublished studies and conference abstracts, was also included to minimise bias and enhance comprehensiveness (Haddaway et al., 2020).
Search strategy
The search followed JBIMES’ three-step strategy. An initial MEDLINE and Scopus search based on the PCC mnemonic guided refinement of search terms by analysing titles and abstracts. PRESS guidelines (McGowan et al., 2016) informed search design, and inter-rater reliability between the researcher and reviewer was ensured through independent reviews and consensus discussions. A second search used refined terms across 16 databases and 9 grey literature sources and Boolean logic and wildcards captured variations of core terms (Cherry & Dickson, 2017). Reference lists were reviewed, and searches were updated in August 2022.
Screening process
Following the PRISMA-ScR protocol (Arksey & O’Malley, 2005; Levac et al., 2010), the researcher and reviewer conducted independent screenings at each stage. Discrepancies were resolved through consensus meetings. Inter-rater reliability was maintained through calibration exercises and regular discussions to ensure consistency in applying inclusion criteria. Thirteen studies were selected for inclusion. The data extraction process is summarised in the PRISMA-ScR flow diagram (Figure 1).
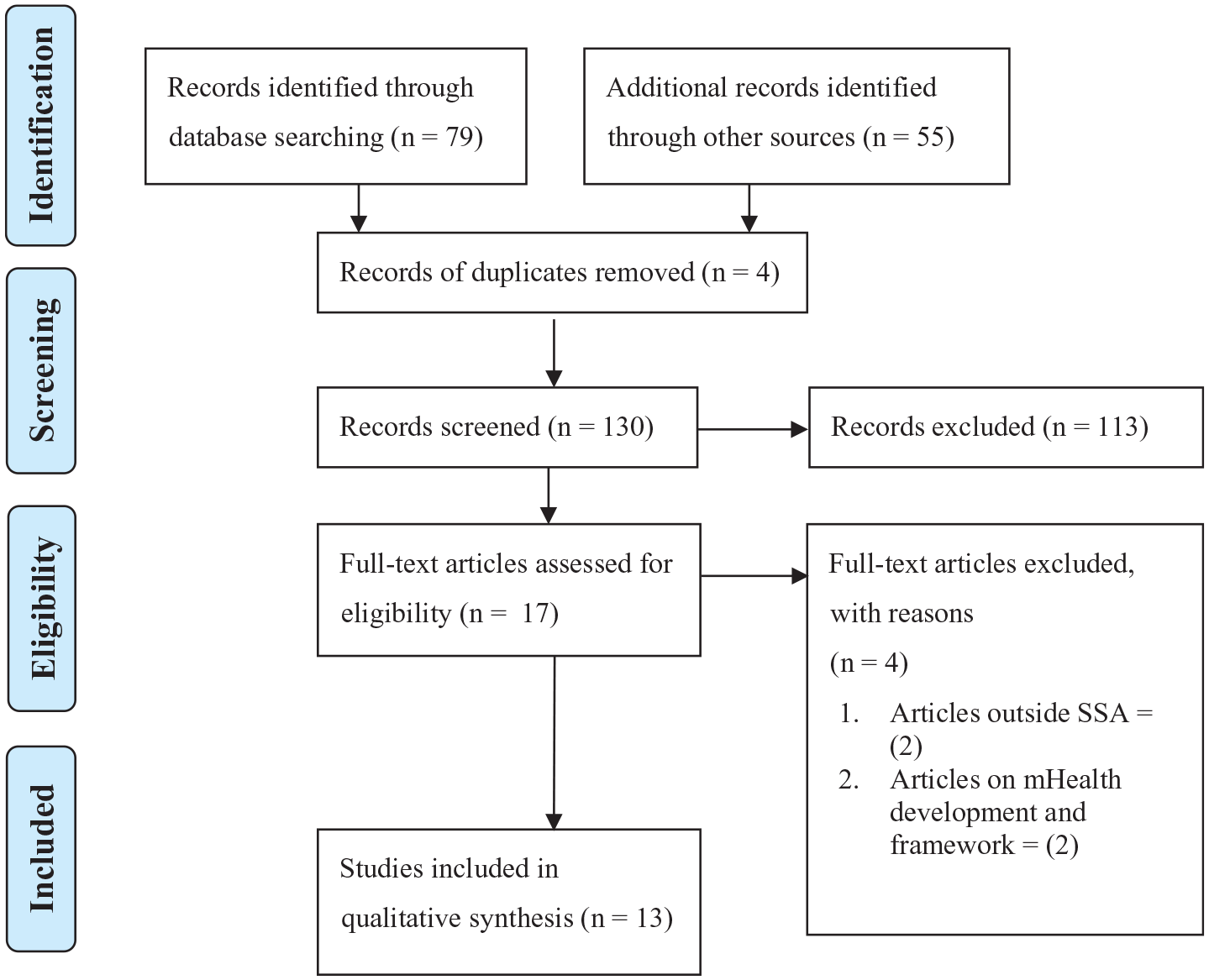
PRISMA-ScR flow diagram.
Data synthesis
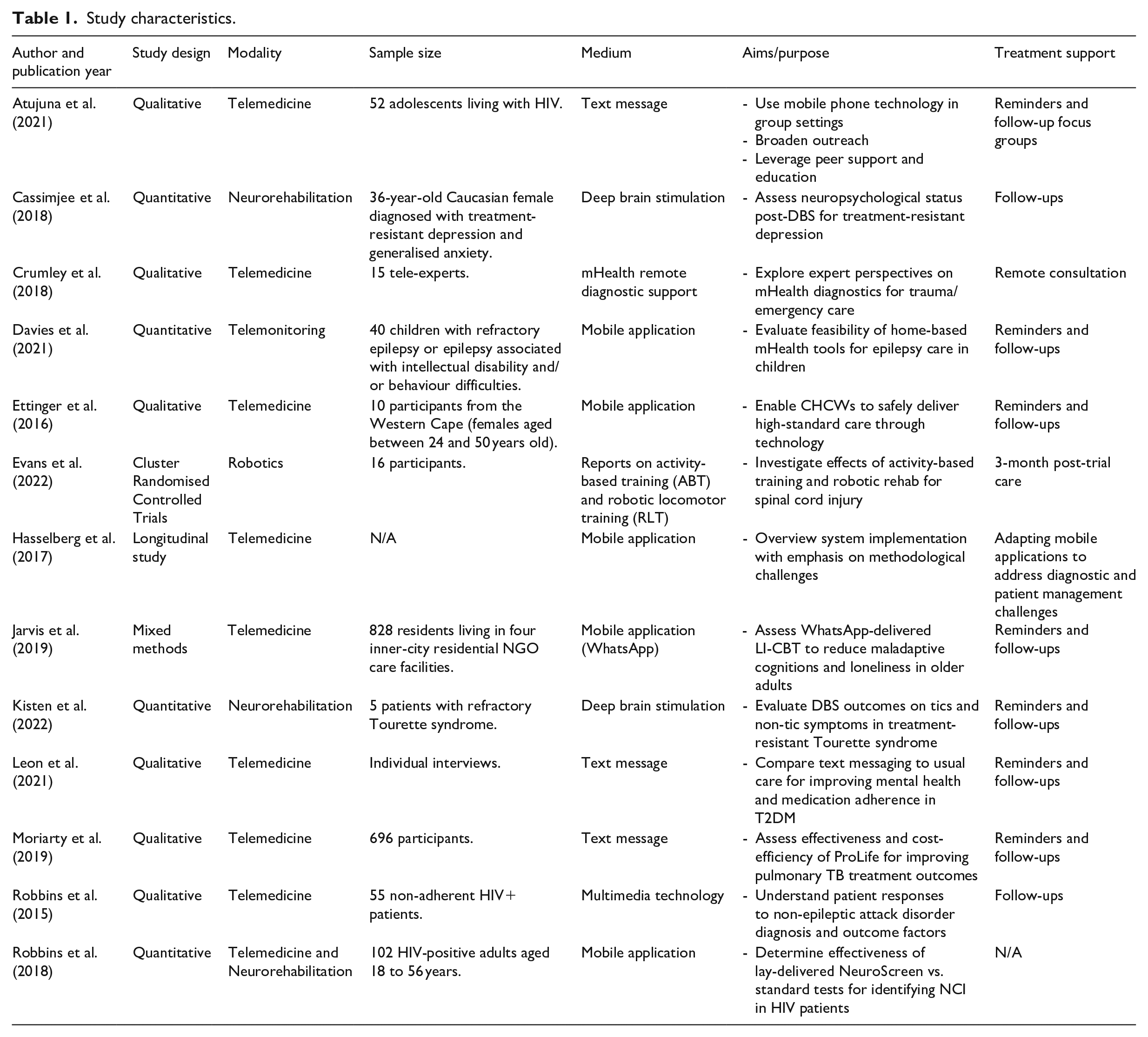
A master table was used to organise the key schema of each study (Peters et al., 2020). Table 1 provides a collation of information on study design, modality of intervention, sample size, medium of intervention, aims/purpose of study, as well as treatment support. In line with Arksey and O’Malley’s (2005) guidelines, a thematic analysis was conducted, wherein a data-charting table was used to identify, organise and categorise common and distinct themes.
Study characteristics.
Results
Characteristics of studies
Table 1 presents the characteristics of the reviewed studies. These include six qualitative studies (Atujuna et al., 2021; Crumley et al., 2018; Ettinger et al., 2016; Leon et al., 2021; Moriarty et al., 2019; Robbins et al., 2015), one cluster randomised controlled trial (Evans et al., 2022), four quantitative studies (Cassimjee et al., 2018; Davies et al., 2021; Kisten et al., 2022; Robbins et al., 2018), one mixed-methods study (Jarvis et al., 2019), and one longitudinal study (Hasselberg et al., 2017).
Trends in technologically assisted intervention studies
Geographic location
The geographic distribution of the 13 studies indicates a concentration in specific South African provinces. Nine studies were conducted in the Western Cape (Crumley et al., 2018; Davies et al., 2021; Ettinger et al., 2016; Evans et al., 2022; Hasselberg et al., 2017; Jarvis et al., 2019; Leon et al., 2021; Robbins et al., 2015, 2018), two in Gauteng (Cassimjee et al., 2018; Kisten et al., 2022), one in both Gauteng and Western Cape (Atujuna et al., 2021), and one spanning Gauteng, Free State, and North–West provinces (Moriarty et al., 2019). This distribution suggests a trend towards regions with better resources and infrastructure, underscoring the need to consider socioeconomics and context to ensure equitable resource allocation. The predominance of studies in the Western Cape likely reflects greater research infrastructure, healthcare resources, and digital access in that province. This geographic concentration limits generalisability to rural or underserved regions, highlighting the need for expanded research across diverse contexts.
Year of publication
Over 76% of the studies were published in the past 5 years (Atujuna et al., 2021; Cassimjee et al., 2018; Crumley et al., 2018; Davies et al., 2021; Evans et al., 2022; Jarvis et al., 2019; Kisten et al., 2022; Leon et al., 2021; Moriarty et al., 2019; Robbins et al., 2018). This recent trend reflects a growing focus on technologically assisted interventions in South Africa. These are influenced by policies promoting evidence-based practice (Patel et al., 2018) and increased use of mobile technology in developing countries (Norris et al., 2013). The COVID-19 pandemic further accelerated this trend (Bokolo, 2021; Madigan et al., 2021).
Sample size
Sample sizes across the reviewed studies varied greatly. While Jarvis et al. (2019) and Moriarty et al. (2019) included 828 and 696 participants respectively, most other studies had fewer than 60 participants. Larger samples were more common in quantitative designs, reflecting the methodological variation across the field.
Modality of technologically assisted intervention
Telemedicine was the primary modality in the majority of the studies (Atujuna et al., 2021; Crumley et al., 2018; Ettinger et al., 2016; Hasselberg et al., 2017; Jarvis et al., 2019; Leon et al., 2021; Moriarty et al., 2019; Robbins et al., 2015). The prominence of telemedicine over neurorehabilitation likely reflects its accessibility and the challenges of implementing more complex interventions in resource-constrained settings.
Medium of mHealth intervention and treatment support
Mobile applications were the most frequently used mHealth interventions. Eight studies required mobile devices for interventions, while text messaging was used in seven studies for treatment support, including follow-ups (Atujuna et al., 2021; Davies et al., 2021; Ettinger et al., 2016; Jarvis et al., 2019; Kisten et al., 2022; Leon et al., 2021; Moriarty et al., 2019). This trend highlights the reach of mobile technology in delivering healthcare interventions, especially in regions with limited access to traditional healthcare.
Thematic analysis
The studies show five distinct yet interconnected overarching themes. These are outlined below.
Theme 1: technological efficacy
The evidence underscores substantial benefits associated with technologically assisted interventions in improving health outcomes across diverse contexts. Jarvis et al. (2019) found that low-intensity cognitive behavioural therapy (CBT), delivered through mobile instant messaging, significantly reduced loneliness and improved cognitive function in elderly populations. Ettinger et al. (2016) demonstrated how the ClinicalGuide application, integrating World Health Organization (WHO) guidelines into a mobile platform, elevated the quality of primary care in rural South Africa. DBS, as shown in studies by Cassimjee et al. (2018) and Kisten et al. (2022), not only offered immediate clinical efficacy in conditions like Tourette syndrome and treatment-resistant depression, but also sustained improvements in quality of life.
Several studies further explored how assistive and augmentative communication (AAC) devices – ranging from speech-generating tools to mobile applications – facilitated language acquisition and interpersonal communication. Training caregivers and educators in AAC usage fostered deeper engagement for children with limited speech capabilities, with positive ripple effects on learning and psychosocial well-being (Naidoo & Bhigjee, 2021). These findings reiterate the interrelation between functional improvements and broader psychological and educational outcomes.
Technological usability and cultural relevance emerged as critical factors contributing to both the success and psychological resonance of interventions. The Masivukeni platform, for example, used multimedia tools to empower lay counsellors in delivering adherence counselling (Robbins et al., 2015), while the Khuluma project aligned its digital format with the literacy levels and context of its users (Atujuna et al., 2021). Such alignment with user capabilities improved health outcomes, enhanced user satisfaction, and increased engagement.
Theme 2: adoption, accessibility, and barriers
The effectiveness of technologically assisted interventions hinges on accessibility and seamless integration into healthcare routines, particularly in low- and middle-income countries (LMICs) like South Africa. Initiatives targeting rural healthcare providers emphasised simplicity and the presence of strong support systems. Human-centred design (HCD) approaches were key to fostering adoption, as demonstrated by the ClinicalGuide applications, which simplified complex clinical guidelines for easier use in under-resourced contexts (Ettinger et al., 2016).
Mobile phone ubiquity across LMICs creates opportunities for scalable health technologies. Studies on trauma care, community health delivery and burn injury assessment reveal the versatility of these digital tools in improving treatment outcomes (Crumley et al., 2018; Hasselberg et al., 2017). However, variability in device ownership and familiarity with mobile technologies can impact user engagement. For instance, differences in smartphone literacy influenced interaction with health applications, despite widespread device ownership (Ettinger et al., 2016).
Adoption rates were closely tied to user-centred design and infrastructure readiness. Interventions that prioritised simplicity, affordability and integration into daily routines saw higher uptake, particularly among rural healthcare workers and patients with limited digital literacy (Ettinger et al., 2016; Hasselberg et al., 2017). Disparities in connectivity, data affordability and device access remained persistent challenges. Nonetheless, when interventions were supported by comprehensive training and technical infrastructure, user satisfaction and effectiveness improved – linking this theme closely with the efficacy of interventions (Theme 1).
Barriers to adoption also include economic and infrastructural limitations – such as unreliable access to electricity and internet – which impede both implementation and sustainability (Ettinger et al., 2016; Jarvis et al., 2019). Concerns around device security, data protection and network reliability contribute to user mistrust in mobile health interventions. Psychological and cultural readiness influenced receptiveness to digital tools. Futhermore, concerns regarding privacy, unfamiliarity, and distrust of mobile health applications contributed to resistance (Crumley et al., 2018).
Digital interventions played a pivotal role in inclusive education by enabling access to curriculum content for learners with developmental delays. Tools like computer-based literacy programmes and virtual learning environments, grounded in universal design principles, enhanced learner confidence and participation. Effective communication technologies, such as those detailed under the Technological Efficacy theme, further supported these educational outcomes.
Theme 3: ethical considerations in digital interventions
While barriers to use technologically assisted interventions are often practical or psychological, ethical concerns represent a more pervasive challenge in the implementation of these interventions. mHealth technologies can empower community healthcare workers (CHCWs) by expanding their roles, but this shift introduces ethical complexities. Issues such as consent, confidentiality, and data security must be carefully managed. Informal practices – like image sharing through messaging platforms – raise additional legal and ethical questions, especially in emergency contexts.
Ethical considerations emerged as central to the responsible implementation of digital interventions. Ettinger et al. (2016) and Hasselberg et al. (2017) highlighted the need for structured ethical guidance and bioethics consultations in applications development, to navigate dilemmas surrounding autonomy and clinical decision-making. Developing clear protocols that secure patient data and ensure informed consent is essential to maintaining public trust and legal compliance.
Innovative technologies such as VR and robotics also face ethical deployment challenges. Programmes like Armeo® Spring and virtual rehabilitation platforms demonstrated positive outcomes in post-stroke and injury rehabilitation (Mehrholz et al., 2020), yet their integration remained contingent on ethical strategies that safeguard both users and providers. These interventions contributed not only to physical recovery, but also to psychological well-being – emphasising the need for holistic, ethically grounded implementation.
Theme 4: community support, emotional connection, and psychological meaning
Technologically assisted interventions, including mHealth applications, telemedicine platforms, and multimedia technologies, have played a critical role in bridging gaps in social support and enhancing emotional well-being – particularly for individuals living with chronic health or mental health challenges. These digital tools enable peer interaction, community involvement, and psychosocial connection, helping to reduce isolation and foster a sense of belonging. By linking users with others who share similar experiences, such platforms promote social inclusion and psychological safety, especially among individuals managing complex or stigmatised conditions.
For example, mHealth interventions have facilitated peer support groups and the sharing of motivational and supportive messages among individuals with HIV or diabetes, contributing to lower psychological distress and improved social cognition (Jarvis et al., 2019). Participants across several studies expressed profound gratitude for the relational connections nurtured through these platforms, which were perceived not merely as sources of information, but as tangible expressions of care, empathy, and community (Ettinger et al., 2016; Leon et al., 2021; Robbins et al., 2015).
The Khuluma project, a peer-led mHealth intervention, exemplifies how mobile technologies can create effective support networks among adolescents living with HIV, fostering self-esteem, emotional resilience and expanded social engagement (Atujuna et al., 2021). Importantly, educational components embedded within these digital platforms have provided not only practical knowledge but also psychological meaning, empowering individuals to better manage their health with confidence and agency (Moriarty et al., 2019; Robbins et al., 2018).
Emerging research also demonstrates how digital tools, such as text messaging and social media platforms, enable motivational exchanges that transcend geographic boundaries, offering participants a renewed sense of hope, belonging and connection. These platforms have been perceived as vehicles for emotional expression, social inclusion and care, particularly in contexts where in-person support is limited (Kisten et al., 2022; Leon et al., 2021).
Collectively, these findings illustrate how technologically assisted interventions – including telemedicine, mHealth applications, and multimedia technologies – not only foster community support and emotional connection, but also provide critical psychological meaning for users. When thoughtfully adapted to the realities of lower-resource settings, these tools represent a scalable, sustainable pathway towards inclusive and socially just healthcare delivery in South Africa.
Theme 5: gratitude and hope
Beyond clinical and therapeutic outcomes, participants across several studies expressed a profound sense of gratitude for the care received through technologically assisted interventions (Atujuna et al., 2021; Ettinger et al., 2016; Leon et al., 2021; Moriarty et al., 2019; Robbins et al., 2015). This appreciation often extended beyond the therapeutic modalities themselves to include broader aspects such as access to healthcare services that might otherwise have been inaccessible. For instance, in the context of spinal cord injury rehabilitation, gratitude was directed not only toward the technology used, but also for the opportunity to engage with healthcare systems that were previously out of reach (Evans et al., 2022).
Interventions such as Khuluma, a mobile application psychosocial support programme for individuals living with HIV, exemplified how digital methodologies can create meaningful psychosocial spaces. These platforms enabled participants to openly share their experiences and emotions, contributing to a sense of belonging and community – a factor often cited as central to managing chronic illness (Atujuna et al., 2021). The perceived emotional safety and peer support offered through such programmes emerged as critical components in fostering psychological resilience and well-being.
Importantly, the educational aspects embedded within these multimedia technologies interventions were consistently highlighted as valuable by participants (Robbins et al., 2015, 2018). These components provided not only practical knowledge, but also psychological meaning, empowering individuals to understand and manage their conditions with greater confidence. Such insights demonstrate that the impact of technologically assisted interventions transcends traditional health metrics; they nurture emotional support, facilitate social connection, and enhance both access to and engagement with care systems.
Studies consistently reported that improved healthcare access, particularly in underserved areas, was met with gratitude (Evans et al., 2022; Jarvis et al., 2019), while renewed hope emerged as a powerful byproduct of interventions targeting chronic or stigmatised conditions (Leon et al., 2021). Far from being incidental, these affective responses were often correlated with improved adherence, greater satisfaction, and sustained engagement in care. In particular, the inclusion of educational elements – such as those in the ProLife messaging applications – was noted to enrich participants’ sense of psychological purpose and agency (Moriarty et al., 2019). Collectively, these findings suggest that emotional responses such as gratitude and hope play a significant role in intervention success, contributing to enhanced therapeutic alliance, increased motivation and overall quality of life (Kisten et al., 2022).
Ultimately, although presented as discrete categories, the themes discussed are intrinsically linked. Technological efficacy is contingent upon accessibility (Themes 1 and 2), while ethical clarity (Theme 3) fosters trust and enables broader uptake. Community and peer networks (Theme 4) not only strengthen psychological resilience but also reinforce engagement and long-term adherence, which are deeply intertwined with the emotional responses explored in Theme 5. Together, these findings offer a holistic view of technologically assisted interventions, situating clinical, emotional, and systemic outcomes within an integrated framework of digital health innovation.
Discussion
South Africa has emerged as a global leader in mobile-phone-based eHealth interventions for HIV care, especially in rural contexts (de Tolly et al., 2009). However, the application of technologically assisted psychological and neurorehabilitation interventions remains limited in comparison, both nationally and globally (Hák et al., 2016; Patel et al., 2018). This review identified a range of interventions – such as those targeting epilepsy, psychosocial support, neurorehabilitation, trauma response and maladaptive cognition, which have potential for use in the South African context (Atujuna et al., 2021; Davies et al., 2021; Evans et al., 2022; Jarvis et al., 2019).
Globally, technological modalities such as VR, artificial intelligence, and BCIs are gaining traction in psychological and neurological care, particularly in high-income settings. Compared to these developments, the South African literature remains less focused on emerging tools like BCIs and neurofeedback, with only limited investigation into neural interfaces (Naidoo & Bhigjee, 2021). Robotics and DBS, while explored locally, would benefit from further applied research and contextual evaluation (Cassimjee et al., 2018; Kisten et al., 2022).
The review also found that mHealth and multimedia technologies are frequently used in primary healthcare, trauma and patient education (Crumley et al., 2018; Ettinger et al., 2016; Robbins et al., 2015). These interventions play an important role in reducing service fragmentation and improving patient engagement, particularly where access to care is constrained. However, most interventions were developed in high-resource contexts and few studies address the infrastructural and educational challenges of rural or underserved regions (Evans et al., 2022; Leon et al., 2021). These findings suggest a need for more targeted research and implementation in low-resource settings to ensure greater equity in health outcomes.
Successful scale-up of technologically assisted interventions, including telemedicine, mHealth, and advanced tools like BCIs, is contingent on addressing persistent barriers such as unreliable internet access, limited device availability and varying levels of digital literacy – particularly in rural and underserved communities. Without careful attention to these infrastructural challenges, such interventions risk exacerbating existing health inequities. In this context, South Africa’s healthcare system stands to benefit from structured, policy-driven implementation of scalable digital interventions. Policies that promote digital literacy, subsidise mobile access and support community-based training are essential to mitigate barriers and enhance equitable adoption, especially in resource-limited settings. Alignment with national 4IR objectives and integration into public health strategies may further facilitate sustainable deployment (Schwab, 2017). Interventions such as telemedicine and neurorehabilitative robotics, if supported by infrastructure investment and professional development, may offer viable, cost-effective solutions in both urban and rural contexts (Crumley et al., 2018; Robbins et al., 2018).
Future research should focus on underrepresented modalities such as neurofeedback, BCI, AI-driven diagnostics, as well as long-term outcomes of robotic rehabilitation. There is also a need to explore the integration of these technologies with community health systems and their cost-effectiveness in diverse socioeconomic settings. As this was a scoping review, findings should be viewed as a descriptive map of current evidence rather than evaluative conclusions about intervention efficacy. Further primary studies and systematic evaluations are necessary to substantiate these early trends and guide policy formulation.
Conclusion
This review mapped the current use of technologically assisted interventions for psychological and neurological care in South Africa. The findings underscore the potential of these tools to expand healthcare access and support. While telemedicine and mHealth emerged as dominant, the generalisability of these positive outcomes is limited by a focus on higher-resourced contexts. Emerging technologies such as BCIs, neurofeedback and AI-driven diagnostic tools hold significant promise for enhancing neurological and psychological care, particularly in addressing gaps in specialist access within underserved communities. To ensure these innovations translate into equitable healthcare benefits, future research must prioritise evaluating the feasibility, cost-effectiveness, and long-term outcomes of such tools in resource-constrained environments. Crucially, broader implementation must also address persistent infrastructural gaps, digital literacy challenges and inequitable access to devices and connectivity. When adapted to the realities of lower-resource settings, technologically assisted interventions – including telemedicine, mHealth, mobile applications, and multimedia tools – offer a sustainable, scalable pathway towards advancing social justice and inclusive healthcare delivery in South Africa.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.