
Abstract
Recent evidence on the lasting psychological impacts of COVID-19, including threats from new variants, highlights the need to examine factors driving psychological distress during the pandemic. We have identified the unique contributions of COVID-19 infodemics to psychological distress among the general population of New Zealand and Ghana. We sampled 936 (New Zealand: n = 413, Ghana: n = 523) respondents to participate in an online cross-sectional study. After accounting for the country of residence, the belief in punishment from God and the perception that COVID-19 is not dangerous were positively associated with psychological distress, while the belief in the lab origin of COVID-19 was negatively linked to psychological distress. In New Zealand, the belief that COVID-19 is a ‘Whiteman’s disease’ uniquely accounted for the highest variance in psychological distress (8%, β = .17, p = .003), while in Ghana, the belief that COVID-19 is a punishment from God independently explained 5% of the variance (β = .19, p < .001). The belief that COVID-19 is not dangerous remained a significant predictor in both Ghana (β = .30, p = .010) and New Zealand (β = .13, p = .010), uniquely contributing 2% each to distress variation. The apocalyptic belief in New Zealand (β = .14, p = .011) and concerns about COVID-19 vaccination causing infertility in Ghana (β = .09, p = .037) had the lowest unique contribution each explaining 1% of the variance. Acknowledging the influences of infodemics can guide the development of more effective and culturally sensitive interventions to promote mental health and well-being within various communities during pandemics, epidemics, and Pathogen X.
Introduction
Five years since the onset of the COVID-19 pandemic, widespread vaccinations have effectively managed its impact on society but have not completely halted the transmission of COVID-19 and other viral infectious diseases (Vasileiou et al., 2021). While the COVID-19 pandemic may seem to be transitioning towards an endemic phase, concerns persist regarding the emergence of new variants of COVID-19. These variants continue to pose a threat to the prospect of returning to a fully functional and normal way of life (Fernandes et al., 2022). Recent evidence has documented the profound negative psychological impacts of the COVID-19 pandemic, implying that the pandemic continues to influence individuals’ mental states (Anteneh et al., 2023). These challenges underscore the need for continuous research and the development of avenues, including the exploration of the psychological impacts of COVID-19, encompassing COVID-19 infodemics to inform mental health interventions amid COVID-19 and other evolving viruses.
Infodemics related to pandemics have endured for centuries. Some of the most impactful and unexpected pandemics, such as Ebola, HIV/AIDS, and COVID-19, have captured global attention, and public health campaigns surrounding these pandemics to combat infodemics persist (van Der Linden et al., 2020). Infodemics encompass false or misleading information in digital and physical environments during disease outbreaks (World Health Organization [WHO], 2023). For instance, during the Ebola outbreak, false beliefs emerged, such as the notion that taking a daily hot water bath with salt could prevent the disease. In addition, there was the perception that the vaccine intended to combat Ebola could cause the disease instead of curing it (Xu, 2023). The belief that HIV emerged because of an experiment that went wrong, and it was deliberately created to kill poor people in the world was found to be common among African Americans (Bohnert & Latkin, 2009).
The infodemics observed with COVID-19, including Ebola, and HIV/AIDS are likely applied to many pandemics the world has faced or will face. These include the widespread tendency to downplay the existence of deadly diseases at the beginning or throughout their duration, persistent scepticism and mistrust towards governments, scientific institutions, and pharmaceutical companies, including associated fears (Ball, 2016; Schmidt et al., 2020). Therefore, the resurgence of infodemics during epidemics and pandemics is not merely due to ignorance, naivety, or extreme beliefs (Joseph & Joseph, 2020). Infodemics surrounding pandemics and epidemics not only impede disease containment efforts (Lohiniva et al., 2022) but also significantly impact individuals’ mental health during disease outbreaks.
Perhaps more concerning is the recent impact of the COVID-19 pandemic on mental health in Ghana and New Zealand, the context of the current study. Found out that psychological distress increased with high levels of fear of COVID-19 among university students in Ghana. Victims of COVID-19 in Ghana were found to experience distress stemming from stigmatization (Adom et al., 2021). Researchers also reported that the social isolation protocols during the pandemic led to psychological distress across cities in Ghana, including Tamale, Accra, and Kumasi (Asiamah et al., 2021). On the other hand, in New Zealand during the first 10 weeks of COVID-19, depression and anxiety levels exceeded population norms (Gasteiger et al., 2021). Individuals were also found to be at greater risk for anxiety and well-being within this same context during the pandemic (Bell et al., 2021), with an observed increase in updates of mental health services (Johnstone et al., 2021; Mahoney et al., 2021). Furthermore, evidence from other countries shows similar trends. For instance, Molenda et al. (2023) found that such infodemics are associated with poorer health outcomes, including emotional regulation difficulties among British, American, and Polish samples. Religion-related infodemics were found to be associated with anxiety, paranoid ideation, and depression in the Czech Republic (Kosarkova et al., 2023). Likewise, the belief that COVID-19 was deliberately developed in the laboratory related to heighten levels of psychological distress, including anxiety among healthcare workers in Ecuador (Chen et al., 2020).
Literature gaps and current study
We observed that existing studies have not comprehensively addressed the specific impact of infodemics on psychological distress during the pandemic. For example, the impact of the belief in Africa that COVID-19 signifies the end-times remains largely unexplored in terms of its influence on distress, especially in highly religious regions like Sub-Saharan Africa and potentially other Western countries. While the literature has examined the impact of COVID-19 on mental health, researchers emphasized prevalence rates of mental health among diverse populations and the impact of factors such as the emergence of the pandemic and stigma, indicating that the influence of infodemics in the literature is largely neglected. Meanwhile, the trends observed in the above literature syntheses demonstrated that various aspects of the pandemic had a negative impact on individuals’ mental health, warranting the exploration of the impact of COVID-19 infodemics on mental health.
Additionally, most available research has also been conducted within Western, Educated, Industrialized, Rich, and Democratic (WEIRD; Henrich et al., 2010) societies, which raises challenges in generalizing findings to less developed countries, including Ghana. Ghana, part of the Sub-Saharan Africa-West African region, has a culturally diverse population of about 31 million, including ethnic groups such as the Akan, Mole-Dagbani, Ewe, and Ga-Dangme, each with distinct languages and cultural practices (Ghana Statistical Service, 2021). This culture’s beliefs and practices are dominated by the notion that signs and wonders, miracles and other supernatural occurrences are normal parts of human life (Fosu-Ankrah & Amoako-Gyampah, 2021). As a result, the highly religious Ghanaian society is known for attributing life events like disease outbreaks to spiritual causes (Read & Doku, 2012). This implies that individuals in this context could be more inclined to endorse and be impacted by COVID-19 religion-related infodemics. For example, the majority of Africans, including Ghana, believe that the COVID-19 pandemic is a punishment for sinful acts committed by humanity (Fosu-Ankrah & Amoako-Gyampah, 2021).
New Zealand, on the other hand, is an island nation in the southwestern Pacific Ocean, with a population of approximately 5 million people, it is ethnically diverse, comprising Europeans, Maori, Pacific Islanders, and Asians. Culturally, New Zealand blends Maori heritage, colonial history, and modern multicultural influences. Although public health systems in this country are widely accessible, New Zealand can still be impacted by common COVID-19 infodemics, such as the belief that COVID-19 is a bioweapon. Similarly, other developed countries, such as the United States, have also been negatively affected by such infodemics (Cardenas, 2022). The current study adapted infodemics related to COVID-19 and religion, the COVID-19 vaccine, and the origin of COVID-19. The selection of these infodemics is important for the study because they represent key themes of infodemics that have been widely discussed and circulated during the COVID-19 pandemic. In addition, they tend to capture the diverse range of infodemics prevalent across different regions of the world. This approach allows for a comprehensive examination of how various types of infodemics have impacted distress (Adu, et al., 2023b).
While diverse cultural comparisons, such as the current study, could be beneficial for global health and well-being, studies have predominantly focused on single populations and sub-groups, resulting in a segmented understanding of the impact of infodemics on the COVID-19 pandemic across countries. Such cross-cultural study is also essential as research has indicated that cultures and sociodemographic factors influence beliefs differently, including infodemics (Fu et al., 2004; Loomba et al., 2021). Furthermore, a key methodological limitation in the existing literature is the absence of ranking the magnitude of the impact of COVID-19 infodemics on psychological distress.
Most previous studies employed regression models where all predictors were included in a single step, potentially obscuring the unique contributions of individual factors. For instance, Xu and Liu (2021) reported that their infodemic factors collectively accounted for 0.05% of the variance in anxiety, limiting the ability to identify the distinct effects of each factor. To address such issues, we utilized stepwise regression, which systematically selects the most significant predictors and reduces model complexity, thereby complementing similar regression findings. Notably, some variables may hold greater explanatory power than others, highlighting the potential for optimized health interventions when understanding the distinct variances each variable explains.
Therefore, the present study aimed to examine the unique contribution of infodemic beliefs to psychological distress among individuals living in Ghana and New Zealand. Specifically, we sought to identify which of these beliefs are most strongly associated with distress, considering both cross-national patterns and context-specific dynamics. By exploring these associations, the study contributed to a deeper understanding of how misinformation influences mental health outcomes in diverse sociocultural settings.
Method
Participants and procedure
This research utilized data gathered from the general population of New Zealand and Ghana. Ethical approval was first obtained from the authors’ institutional ethics committee (#0000029770). We used convenience sampling technique to collect data from Ghana using SelectSurvey.net data collection software. We initially recruited participants based on accessibility and then encouraged them to share the survey link with others in their networks. Different online platforms such as WhatsApp, email, Instagram, and Facebook were used for the data collection. The survey was open online from June to July 2022. The Global Positioning System (GPS) coordinates and Internet Protocol (IP) address functions were disabled to protect participants’ identities and ensure compliance with ethical guidelines. No incentives were provided to the Ghanaian participants for their participation in the study, as the social networks of researchers were used for the data collection in Ghana. We engaged the services of Qualtrics, a data collection company, for collecting the data in New Zealand. Participants received a minor monetary compensation (e.g., NZ$5 or the opportunity to enter a draw). Data collection companies may lack a complete understanding of the research context, but they possess expertise in efficient data collection and handling, which helps save time and resources for researchers (Wright, 2005). Participation in this study was voluntary, and individuals aged 18 and above were eligible to participate.
Furthermore, our choice to use the current study design was primarily driven by the COVID-19 safety protocols in place during our data collection period. Online data collection methods are also found to be cost-effective and provide access to a broader segment of the population across diverse geographic locations (Lefever et al., 2007). Participation in the survey was voluntary. Before proceeding to the main measures, participants provided demographic information. On average, participants took about 15min to complete the entire questionnaire. Participants first responded to basic demographic information before proceeding to the main measures, which included distress and COVID-19 infodemics.
Power analysis
A priori power analysis using G*Power 3.1 was conducted to determine the required sample size for regression analysis with 13 predictors: an effect size of .15, an α error probability of .05, and an anticipated power of .95 yielded a required sample size of n = 189 for these parameters (Faul et al., 2007). Hence, the current sample is greater, contributing to more statistical power.
Measures
The commonly used Depression Anxiety Stress Scale (DASS-21; Lovibond & Lovibond, 1995) was used to measure psychological distress. This scale has about 18,000+ citations on Google Scholar currently. The scale comprises 21 items and uses a 4-point Likert-type scale ranging from 0 = ‘Did not apply to me at all’ to 3 = ‘Applied to me very much’. Participants were asked to indicate how much each statement in the scale applied to them over the past weeks. Sample items on the scale include depression (‘I couldn’t seem to experience any positive feeling at all’); anxiety (‘I was aware of dryness of my mouth’); and stress (‘I found it hard to wind down’). This scale was treated as a unidimensional measure, combining the scores of all three subscales into a single score. The internal consistency coefficient of the scale in the current study was excellent for both New Zealand (Cronbach’s alpha (α) = .97, McDonald’s omega (ω) = .97; M = 25.19, SD = 19.70) and Ghana (α = .95, ω = .95; M = 35.01, SD = 12.83).
Thirteen COVID-19-related infodemics were assessed in the current study. These infodemics were adapted for the current study based on their common usage in previous COVID-19 literature (Adu, et al., 2023a; DiGregorio et al., 2022)). Each infodemic was assessed with a single item using a 5-point Likert-type scale ranging from 1 = ‘strongly disagree’ to 5 = ‘strongly agree’, as was done in previous literature (Lohiniva et al., 2022). Items included: ‘I believe that the COVID-19 pandemic is a punishment from God as a result of humanity’s sinful acts’, ‘I believe that the presence of COVID-19 is one of the signs that the end-time is near’, ‘I believe that God can protect me from COVID-19 even if I don’t take the vaccine’, ‘I believe that COVID-19 crisis was deliberately created to keep people at home while 5G engineers install the technology everywhere’, ‘I believe that COVID-19 is a Whiteman’s disease’, ‘I believe that the COVID-19 was created in a Chinese laboratory, as the pandemic originated from Wuhan in China’, ‘I believe that the COVID-19 was designed as a bioweapon (to reduce the world population)’, ‘I believe that COVID-19 originated as a result of Chinese eating bat meat and the virus passed from bats to humans’, ‘I believe that COVID-19 vaccine can cause infertility’, ‘I believe that COVID-19 vaccination will change my genetic’, ‘I believe that COVID-19 vaccination will cause heritable damage to my health/my body’, ‘I believe that COVID-19 is not dangerous and therefore COVID-19 vaccination is not necessary’, and ‘I believe that COVID-19 has been deliberately spread by the elite and the rich families of the world’.
Of note, while these beliefs included conspiracy, misinformation, and disinformation, the current study refrained from disentangling the distinct differences between the terms. Instead, we treated all these terms as forms of informational distortions, collectively termed infodemics, acknowledging their shared profound consequences on psychological distress during the COVID-19 pandemic.
Statistical analysis
Data analyses was conducted using Statistical Package for the Social Sciences (IBM SPSS; version 28) and Jeffreys’ Amazing Statistics Program (JASP Team, 2022). The New Zealand data had no missing values, while the Expectation Maximization algorithm in SPSS was used to handle the few missing data points in the Ghanaian dataset (Nelwamondo et al., 2007). The main analysis was carried out in JASP. Descriptive analysis summarized demographic variables. For the primary analysis, total scores of non-binary scales were computed. The normality of these variables was confirmed through Q-Q plots and skewness and kurtosis, which were within the acceptable range of −2 to +2 (George, 2011). The assumption of homoscedasticity was met, as indicated by the casewise diagnoses revealing that all predicted values fell within a narrow range. This suggests a non-significant difference in the spread of residuals across the entire range of predicted values. In addition, the P-P plots and scatterplot showed a random distribution of variables along the horizontal axis. The Variance Inflation Factor (VIF) of all variables was below 5, suggesting the absence of multicollinearity (Marcoulides & Raykov, 2019). To mitigate multicollinearity risks, regression analyses were conducted for the combined distress scale as a dependent variable.
Pearson’s correlation coefficients were first calculated to examine the associations among all study variables. While some variables were binary, they were dummy coded, making the use of Pearson’s correlation appropriate (Cohen et al., 2003). This was followed by stepwise linear regression and hierarchical regression. While the stepwise regression was used within each country, hierarchical regression controlled for country-level differences in a pooled analysis. The stepwise regression used the forward and backward entry method. This analysis was employed to demonstrate the unique contributions of the predictors to psychological distress among the samples. The modelling process began with the inclusion of the strongest predictor with a substantial explained variance. The variance of this predictor was then controlled, and subsequently, additional significant predictors that independently contribute to the outcome’s variance were sequentially incorporated, all these were done to identify and eliminate redundant predictors. The statistical criteria for predictor variables’ inclusion was p < .05, and for removal of a predictor variable was p ⩾ .10 (Roemer et al., 2021). We meticulously controlled for the influence of each variable and subsequently introduced all predictor variables for psychological distress. This systematic procedure was executed independently for each of the countries under examination.
We used hierarchical regression to account for country differences. In this analysis, we first introduced country as a control variable before entering the 13 COVID-19 infodemic beliefs, without imposing a strict theoretical hierarchy, as the selection of infodemic beliefs was data-driven, similar to previous literature (Andrade, 2019; Medvedev et al., 2018). In sum, we used stepwise regression to identify key infodemic beliefs predicting distress, while pooled hierarchical regression controlled for country differences to assess their overall impact.
Results
Descriptive statistics
The final sample size consisted of 936 participants who actively completed the survey (New Zealand: n = 413, Ghana: n = 523). The ages of participants ranged from: New Zealand 18 to 89 years (Mage = 46.35; SDage = 18.07); and Ghana 18 to 63 years (Mage = 29.48; SDage = 5.69). In Ghana, 338 participants (65%) were males, while 185 (35%) were females. In New Zealand, 179 (43%) were males, and 234 (57%) were females. Furthermore, in New Zealand, 275 participants (67%) identified as Europeans, 36(9.2%) as Asians, 64(16%) as Maori and Pacific, and 4(1%) as Middle Eastern, Latin American, and African. All participants from Ghana identified themselves as belonging to their heritage. In terms of religiosity, 468 (89.52%) identified as being religious and 55 (10.48%) did not belong to any religious group. In New Zealand, 223 (54.01%) were not religious but 190 (45.99%) identified as being religious.
Pearson’s correlation results
Results from the Pearson’s correlation coefficient analysis revealed that beliefs such as viewing the COVID-19 pandemic as a punishment from God, not dangerous, a sign of the end-time, a creation to install 5G technology, and the notion that the COVID-19 vaccine can cause infertility, heritable damage, and alter genes, as well as the belief in divine protection from COVID-19 without vaccination, were positively correlated with psychological distress (Table 1). These correlations were observed in Ghana and New Zealand, with correlation coefficients (r) ranging from .11 to .27 (p < .001; Table 1). However, beliefs such as the notion that COVID-19 was designed as a bioweapon, that it is a ‘Whiteman’s disease’, that it originated due to Chinese consumption of bat meat, and that it was deliberately spread by the elite and rich families of the world were positively associated with psychological distress. in New Zealand only, with correlation coefficients (r) ranging from .11 to .29 (p < .001; Table 1).
Summary of the Pearson’s correlation coefficients of COVID-19 infodemics and psychological distress in Ghana (n = 523) and New Zealand (n = 413).
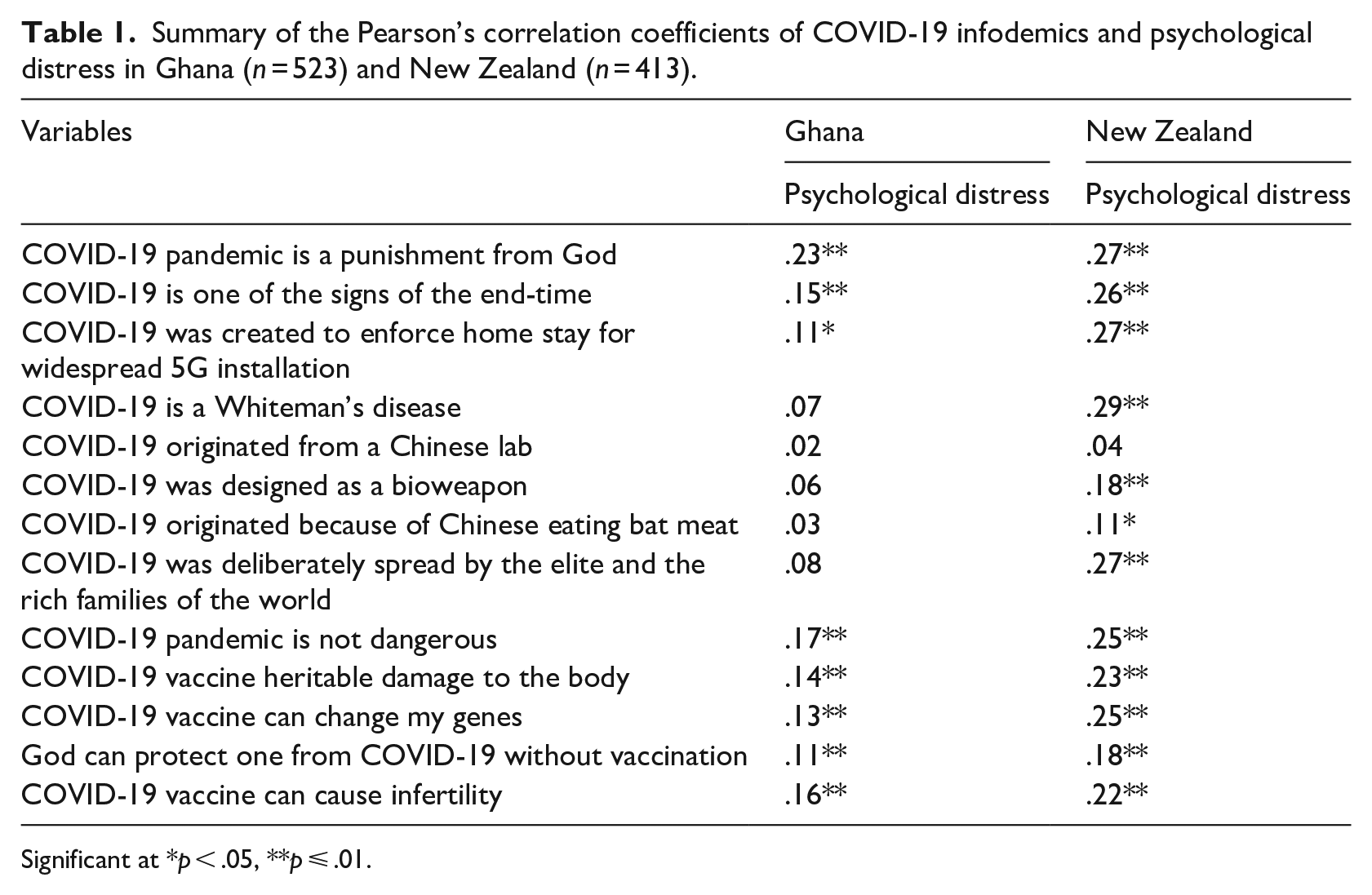
Significant at *p < .05, **p ⩽ .01.
Hierarchical multiple regression results
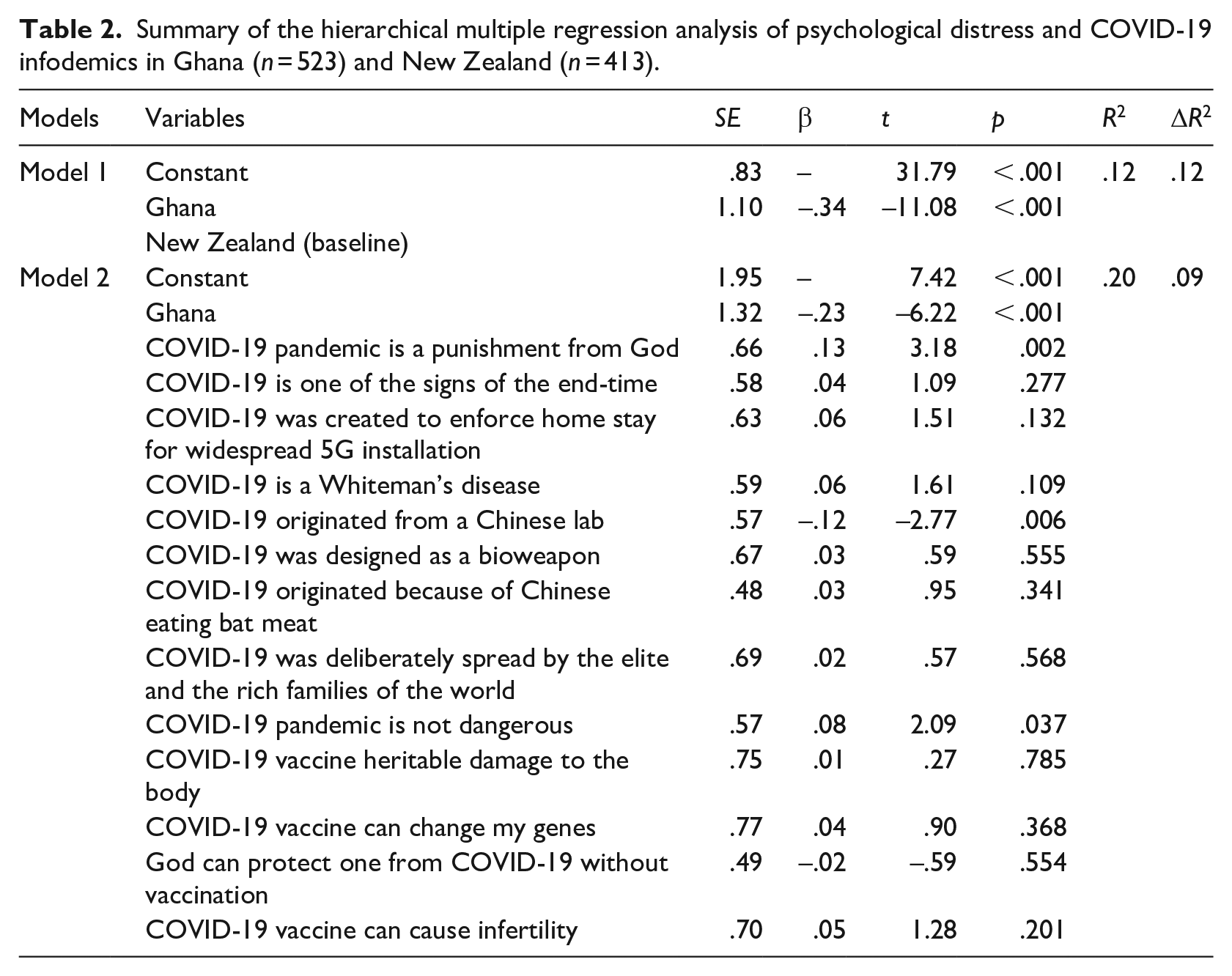
The findings of the hierarchical multiple regression analysis revealed that, at the first step, country of residence significantly contributed to the regression model, F(934) = 122.74, p < .001, explaining 12% of the variance in psychological distress (Table 2). Subsequently, introducing all the infodemic variables in the second step accounted for an additional 9% of the variance in psychological distress beyond the country effects. This change in R2 was statistically significant, F(921) = 17.22, p < .001. Furthermore, our results showed significant differences in psychological distress among residents in the countries. Compared to residents in New Zealand (baseline category), individuals in Ghana reported significantly less psychological distress (β = −.34, t(921) = −11.08, p < .001; Table 2) in Model 1, and remained significant in Model 2 (β = −.23, t(921) = −6.22, p < .001; Table 2). After controlling for country of residence, three infodemic beliefs emerged as significant predictors of psychological distress. The belief that the COVID-19 pandemic is a punishment from God was positively associated with distress (β = .13, t = 3.18, p = .002; Table 2), as was the belief that COVID-19 is not dangerous (β = .08, t = 2.09, p = .037; Table 2). Conversely, belief in the lab-origin theory of COVID-19 was negatively associated with distress (β = −.12, t = −2.77, p = .006; Table 2). Together, the model explained 20% of the variance in psychological distress (R2 = .20; Table 2), with infodemic beliefs accounting for an additional 9% beyond country-level effects (ΔR2 = .09; Table 2).
Summary of the hierarchical multiple regression analysis of psychological distress and COVID-19 infodemics in Ghana (n = 523) and New Zealand (n = 413).
Stepwise linear regression results
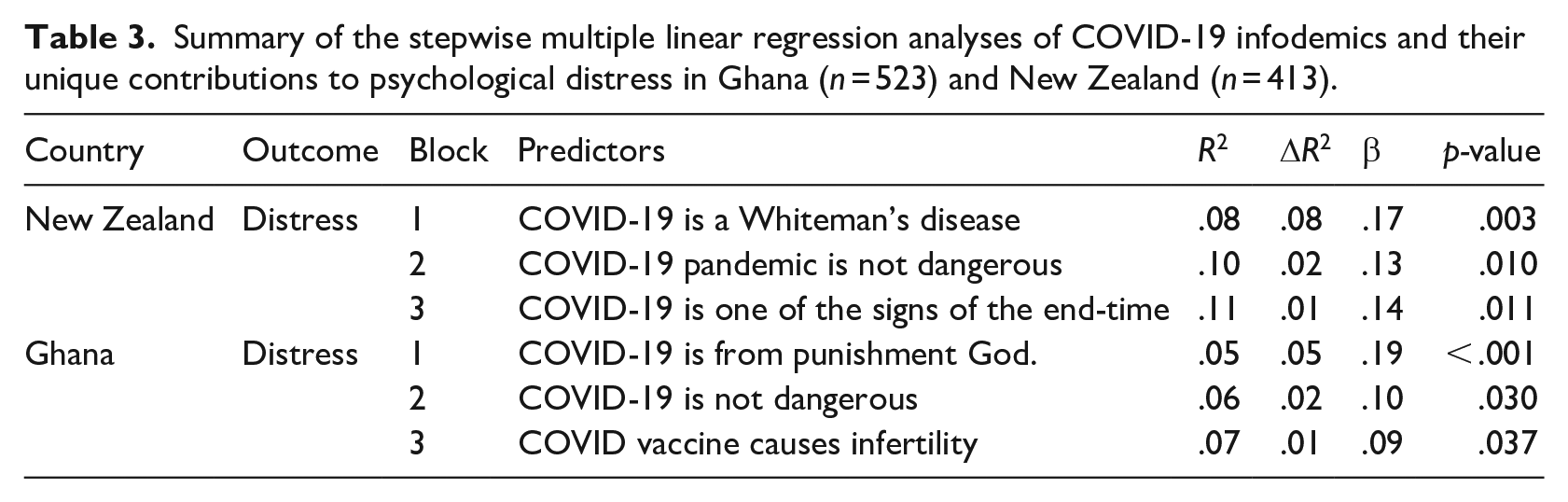
Table 3 presents stepwise linear regression results illustrating the unique contributions of infodemic beliefs to psychological distress. In New Zealand, the belief that COVID-19 is a ‘Whiteman’s disease’ independently accounted for the highest explained variance (8%) in psychological distress (β = .17, p = .003). Similarly, in Ghana, the belief that COVID-19 is a punishment from God uniquely predicted psychological distress, explaining 5% of the variance (β = .19, p ⩽ .001). After adjusting for the most dominant predictors in each country through a stepwise approach, the belief that COVID-19 is not dangerous emerged as the second strongest independent predictor of distress in both Ghana (β = .30, p = .010) and New Zealand (β = .13, p = .010), contributing 2% to the variation. Conversely, the apocalyptic belief in New Zealand and concerns about COVID-19 vaccination causing infertility in Ghana exhibited the lowest yet statistically significant contributions, each uniquely accounting for 1% of the variance (β = .14, p = .011; β = .09, p = .037, respectively). These findings underscore the uniquely psychological impact of infodemic beliefs beyond mere associations, highlighting their role as distinct and independent factors influencing psychological distress.
Summary of the stepwise multiple linear regression analyses of COVID-19 infodemics and their unique contributions to psychological distress in Ghana (n = 523) and New Zealand (n = 413).
Discussion
We used a community sample from Ghana and New Zealand to investigate the independent contributions of COVID-19 infodemics to psychological distress. We used stepwise regression to identify key infodemic beliefs predicting distress, while pooled hierarchical regression controlled for country differences to assess their overall impact. After accounting for the country of residence, the belief in punishment from God, and the perception that COVID-19 is not harmful were positively associated with psychological distress, while the belief in the lab origin of COVID-19 was negatively linked to distress. In New Zealand, perceiving COVID-19 as a Whiteman’s disease uniquely accounted for the highest variance in psychological distress followed by the notion that COVID-19 is not harmful and the apocalyptic belief. Notwithstanding, among the Ghanaian sample, divine punishment independently explained the highest variance in psychological distress, which was then followed by the notion that COVID-19 is not harmful and the infertility belief of COVID-19 vaccination.
The interplay between generalizable predictors and context-specific influences highlights the complexity of psychological distress in response to infodemic beliefs. While generalizable predictors reflect consistent psychological associations across countries, context-specific influences reveal how cultural, religious, historical factors, as well as the circumstances surrounding the COVID-19 pandemic, shape distress differently. Addressing infodemics during health crises requires both global strategies targeting widely distressing beliefs and localized approaches that consider societal narratives. Generalizable predictors suggest that some infodemic beliefs have a cross-national psychological impact, making them key targets for large-scale misinformation interventions, while their local variations in strength and meaning underscore the need for culturally adaptive public health messaging.
These variations highlight the complex dynamic system of health-related variables (Fonseca-Pedrero, 2018). Particularly, psychological distress tends to be common in most populations worldwide (Adu et al., 2021a). Research has indicated that depression and anxiety levels exceeded population norms during the COVID-19 pandemic in New Zealand, with about 30% of respondents reporting moderate to severe levels of depression (Every-Palmer et al., 2020; Gasteiger et al., 2021). Ghana reported prevalence rates of 12.3% depression among the adult population (Adu et al., 2021a). Perhaps the differences in reported cases of COVID-19, which tended to be higher in Western countries, including New Zealand compared to African countries, fuelled such differences (WHO, 2024).
Moreover, our results imply that in New Zealand, psychological distress increased with the belief that COVID-19 is a Whiteman disease. Such a belief can worsen internalized stigma and negative feelings about the pandemic (Kulkarni et al., 2020), possibly resulting in increased psychological distress. Infodemics and conspiracy theories have been found to amplify fear and anxiety surrounding pandemics (Kulkarni et al., 2020). While such findings were infrequently reported in the Western literature, Schmidt et al. (2020) documented similar findings in their qualitative study among Nigerians, similar to Manda’s (2021) study in Malawi. A possible reason for this finding could be that Western countries reported higher cases of COVID-19 compared to the African continents (WHO, 2024). The differences in methodologies between studies may have contributed to the limited findings in Western countries regarding this particular result. Many quantitative COVID-19 infodemic studies presented participants with a restricted number of items, excluding consideration of this belief (Gallotti et al., 2020). Perhaps our finding extent the existing literature by providing evidence in a Western country in relation to the belief that COVID-19 is a Whiteman disease and its impact on distress. Such detrimental stigmatizing attitudes are not uncommon in the extant literature and are found to impede efforts towards better health outcomes (Link et al., 2001). Our finding also reflects the need for qualitative data documenting the reason behind the current finding (Spratt et al., 2004).
In addition, the belief in apocalyptic scenarios observed in the data may be influenced by specific cultural views on the causes of health issues and religious interpretations. Religious beliefs often shape how individuals interpret events and their emotional reactions to them (Adu et al., 2021b; 2023a. For example, some cultures attribute certain health conditions to spiritual causes (Adu et al., 2023a; Dein, 2021). People who hold these beliefs may perceive the end of the world as inevitable, leading to a fatalistic view that events are predetermined and efforts to control the pandemic are futile (Kügler & Gies, 2023; Mamani-Benito et al., 2023). This fatalistic attitude can result in a sense of helplessness and its associated distress. For instance, it has also been stated in the Christian bible that one of the signs of the end-time is that humanity will be afflicted with famines and diseases without cure (New International Bible; Matthew 24:6-8), aligning with the perceptions about the COVID-19 pandemic. Kanozia and Arya (2021) also reported religion-related misinformation about the pandemic, likewise Schmidt et al. (2020) and Adu et al. (2023b).
Furthermore, among the Ghanaian sample, the belief that COVID-19 is a punishment from God explaining the highest variance in psychological distress suggests that individuals’ levels of psychological distress increased with belief in this infodemic about the pandemic. This evidence is not surprising as there is a strong belief in the supernatural within the African context, including Ghana, where signs, wonders, miracles, and other extraordinary occurrences are seen as a natural part of everyday life (Fosu-Ankrah & Amoako-Gyampah, 2021; Jones, 2018). This deeply religious society often interprets various life events, including disease outbreaks, through a spiritual lens, attributing them to supernatural causes (Adu et al., 2023a; Read & Doku, 2012). Hence, the belief that COVID-19 is a punishment from a higher power may lead to a fate-control outlook on life events, where individuals feel powerless to control the course of the disease, potentially resulting in hopelessness, anxiousness, and psychological distress (Kügler & Gies, 2023; Mamani-Benito et al., 2023). This observation underscores the significance of acknowledging possible cultural influences on health and well-being within populations worldwide (American Psychiatric Association [APA], 2022) In relation to literature, similar religion-related COVID-19 infodemics have been reported to be linked to anxiety and paranoia ideations, including COVID vaccination hesitancy (Kosarkova et al., 2023; Samal, 2021), highlighting the possible detrimental impact of falsehood on the well-being of individuals, especially during the outbreak of diseases.
We also observed a link between the belief that the COVID-19 vaccine causes infertility and the likelihood of experiencing heightened psychological distress in our data. Notably, this misconception gained attention during the initial phases of the COVID-19 vaccination programme (Zaçe et al., 2022). In the United States, an internet search unveiled a significant surge in the dissemination of misinformation suggesting a link between the COVID-19 vaccine and infertility (Sajjadi et al., 2021). This association can be attributed to several factors. Individuals holding this belief may experience increased anxiety, driven by fears of potential harm to their reproductive health, resulting in distress. Such infodemic narratives could adversely impact the perceived safety and effectiveness of the COVID-19 vaccine, which could lead to COVID-19 vaccine hesitancy (Sajjadi et al., 2021). Samal (2021) also indicated that such COVID-19 infodemics negatively impacted the psychological well-being and COVID-19 vaccination among participants, demonstrating the unfavourable double-edged sword nature of infodemics for health outcomes.
Our findings suggest that infodemics, particularly about health crises not only hinder the fight against pandemics and epidemics but can amplify psychological distress, especially during these challenging times. Results also reflected the impact of informational distortions on mental health outcomes during pandemics and epidemics among the general population. Essentially, the resurgence of infodemics amid epidemics and pandemics is a result of a multifaceted interplay involving historical, cultural, and socio-political factors, as well as informational and mythological influences. Hence, the integral aspects of individuals’ identity and experience intersect in intricate ways with psychological well-being (Joseph & Joseph, 2020). Recognizing this complex interplay is essential for comprehending the diverse ways individuals navigate challenges and distress. Furthermore, acknowledging these influences can guide the development of more effective and sensitive interventions, for example, targeting informational distortions, to promote mental health and mental well-being within various communities during pandemics and epidemics. Whereas the current trends in psychology emphasize the cultural underpinnings of psychological distress, the present findings highlighted the necessity of considering infodemics, and social informational distortion, and its impact during pandemics and epidemics (APA, 2022).
Strengths and limitations
The present study presented several strengths. This study is one of the first studies in the era of the pandemic to investigate the above-mentioned variables in relation to psychological distress among the two countries in a single study. Our study highlights the impact of infodemic on psychological well-being during pandemics and epidemics, providing evidence that can inform tailored interventions for psychological distress during these periods. It also contributes to the limited literature in sub-Saharan Africa and other countries in the region. The use of the stepwise regression analysis implies that variables were examined simultaneously, which provided a comprehensive understanding of the relative and unique importance of each variable in contributing to psychological distress. Such information can inform tailored intervention towards reducing psychological distress among the sample.
Nevertheless, the following limitations are worth mentioning. First, the sample used does not represent the larger population of Ghana and New Zealand, limiting the generalization of the findings. Second, the use of convenient sampling method in recruiting study participants could introduce selection bias as researchers relied on the part of the population that was available. The use of online data collection suggests that the results may reflect this segment of the population. We used cross-sectional design, which did not allow for cause-and-effect inferences. Self-report measures stand the risk of introducing bias, such as social desirability in the data; participants can guess possible relations when using such measures (Grimm, 2010). Regression methods, especially stepwise, can lead to overfitting when the number of predictors is large relative to the sample size, causing the model to perform poorly on new data. In addition, meeting all the underlying assumptions of regression analysis (e.g., linearity, independence, homoscedasticity, normality) could be challenging, which can result in biased or invalid results (Kamer-Ainur & Marioara, 2007; Olusegun et al., 2015).
Implications and future direction
Results emphasize the need for targeted public health communication to address and counteract misinformation surrounding pandemics, epidemics and Pathogen X by recognizing the interplay between cultural nuances and infodemics impact to foster resilience, correct misinformation, and support mental well-being within diverse cultural communities. Exposing individuals to a version of already known information, which they can refute (i.e., psychological inoculation), is found to help address infodemics (van Der Linden et al., 2020). Future research should employ longitudinal study design to establish the cause-and-effect relations between predictor variables to enable a sronger conclusion for the results. Findings also suggest avenues for further research into the intersection of cultural beliefs, health perceptions, and mental health outcomes.
Conclusion
We examined the unique contributions of COVID-19-related infodemics to psychological distress among Ghanaians and New Zealanders. We found out that after accounting for country of residence, the belief in punishment from God and the perception that COVID-19 is not harmful were positively associated with psychological distress, while the belief in the lab origin of COVID-19 was negatively linked to distress. In New Zealand, the belief that COVID-19 is a Whiteman’s disease explained the highest variance in psychological distress, followed by the belief that COVID-19 is not harmful and apocalyptic beliefs. However, in the Ghanaian sample, the belief in divine punishment explained the highest variance in psychological distress, followed by the belief that COVID-19 is not harmful and concerns about COVID-19 vaccination causing infertility. The results highlight the importance of culturally tailored public health communication to counter misinformation, promote resilience, and support mental well-being during pandemics like the COVID-19, epidemics and Pathogen X.
Footnotes
Author contributions
P.A. involved in the conception of the study; data collection of the manuscript, including analysis of data; P.A. led the writing of the manuscript. R.H.A. and J.M. commented on the paper to improve the manuscript; all authors contributed to the study design. All authors contributed to drafting the paper and revised the manuscript for important intellectual content. All authors gave final approval for this version to be published.
Data availability
Study participants did not consent to having their data shared publicly. The deidentified participant dataset generated during the current study can be made available to researchers with relevant permissions upon a reasonable request to the corresponding author. The current data is part of a larger international data on COVID-19.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This research was approved by the Human Research Ethics Committee board of Victoria University of Wellington, Wellington, New Zealand (#0000029770). The study was in line with the Declaration of Helsinki, which outlines fundamental ethical principles for health research involving the use of human participants (World Medical Association, 2001).
Consent to participate and for publication
Participants freely gave consent to participate in this study and for their results to be published or used for other academic purposes such as reports, presentations, and public documentation in aggregate form (i.e., a combined data analysed with those of others).