
Abstract
This exploratory study investigated the mental health status of first responders, specifically police officers and paramedics (n = 429), primarily from the Western Cape Province of South Africa. Participants completed an electronic questionnaire, including the Patient Health Questionnaire-9, Generalized Anxiety Disorder-7 scale, and the post-traumatic stress disorder Checklist for Diagnostic and Statistical Manual of Mental Disorders, fifth edition. Descriptive statistics, including means and standard deviations, were calculated. In addition, a one-sample t-test was performed to compare the means obtained in this study with those from other studies involving samples from the African continent and international contexts. The instruments demonstrated strong reliability, consistent with previous studies conducted in South Africa. Using established cutoff scores from the literature, the study found that 47.3% of the sample would qualify for a diagnosis of depression, 37.8% for generalized anxiety disorder, and 48.5% for post-traumatic stress disorder. These levels are notably high, underscoring the significant psychological burden carried by first responders. The findings underscore the urgent need for targeted mental health interventions tailored to the unique stressors faced by first responders, as well as the importance of addressing barriers to help-seeking within this population group.
Keywords
Introduction
The term “first responder” encompasses a heterogeneous grouping of professionals who are responsible for providing critical services in emergencies. Their main occupational task is first response (Haugen et al., 2012). First responders include police officers, sea rescue personnel, firefighters, and emergency medical services (EMS) personnel (McAlearney et al., 2022). They typically have specialized training that prepares them to safeguard individuals and communities while managing high work demands and routine exposure to physical and psychological stressors (McAlearney et al., 2022). First responders are some of the few occupations in which individuals are repeatedly and consistently placed in extremely stressful and high-risk situations (Syed et al., 2020). Therefore, first responders are disproportionally susceptible to adverse mental health outcomes. This study aims to investigate the mental health status of two categories of first responders in South Africa: police officers and paramedics. The study also examines the associations between mental health indicators and demographic and work-related factors among this sample.
A significant body of international literature has examined the rates of common mental health disorders among police officers (Regehr et al., 2021; Varker et al., 2023). Compared to the general population, police officers report higher rates of anxiety, depression, post-traumatic stress disorder (PTSD), suicidal ideation, and alcohol abuse (Brewin et al., 2022; Kyron et al., 2022). Syed and colleagues (2020), in a systematic review and meta-analysis of the global prevalence of and risk factors for mental health disorders among law enforcement personnel from 24 countries, reported elevated levels of depression (18.6%), PTSD (14.2%), generalized anxiety disorder (9.6%), suicidal ideation (8.5%), and alcohol dependence and hazardous drinking (25.7%). The strongest risk factor for depression, suicidal ideation, and PTSD was high occupational stress, including high levels of exposure to physical danger and threats to personal safety.
Existing studies of paramedics indicate that this group has lower levels of mental well-being, higher levels of psychological distress, and a three-fold higher prevalence of PTSD, compared to the general population (Reardon et al., 2020). Some studies have suggested that emergency service dispatchers have higher levels of traumatic distress than police officers (Smith et al., 2019). In a systematic review, Petrie and colleagues (2018) reported high prevalence rates for depression (15%) and anxiety (15%), as well as elevated general psychological distress (27%), among EMS personnel. Similarly, in a comprehensive synthesis of the extant literature on mental health outcomes among EMS personnel, Wagner and colleagues (2020) found prevalence rates for depression ranging from 6.4% to 42.9% and anxiety ranging from 6% to 33.9%.
There is a paucity of research on mental health outcomes among first responders in South Africa. Ward and colleagues (2006) investigated the prevalence of mental health disorders among emergency services personnel—including ambulance workers, fire fighters, and sea rescue service workers—and reported high rates of general psychopathology, PTSD, and problematic alcohol use. The study also found gendered differences, with women being more likely to experience internalizing disorders (i.e., anxiety and depression) and men more likely to report physical aggression and substance use. Ntatamala and Adams (2022) reported a PTSD prevalence rate of 30% among a sample of ambulance personnel in the Western Cape. Chronic exposure to work-related stress, traumatic incidents, and current treatment for a medical condition were associated with increased risk of traumatic stress reactions in this sample of ambulance personnel. Fjeldheim and colleagues (2014) reported that 16% of trainee paramedics from a university in the Western Cape met the criteria for PTSD. In addition, the sample reported a high prevalence of depression (28%), alcohol abuse (23%), and chronic perceived stress (7%). O’Neil and Kruger (2022) reported that 78% of a sample of first responders—including EMS, Search and Rescue, Fire and Rescue workers, and South African Police Services (SAPS)—reported experiencing moderate-to-high levels of work-related stress.
In a study of the occupational stress and mental health of South African crime scene investigators in Gauteng province, Steyn and Klopper (2020) reported that 20.5% of the sample had been diagnosed with a mental health problem. Most of the sample (60.7%) described their work as stressful, and 58.2% presented with trauma symptomology. The Employee Health and Wellness Services (EHWS) portfolio committee reported that 89% of SAPS officers had been diagnosed with depression and 22% had been diagnosed with PTSD (South African Police Service, 2016). Police officers have been found to ignore the impact of traumatic events, potentially due to the social stigma associated with mental health disorders and seeking help. Social stigma surrounding mental health remains a pervasive issue in South Africa and can inhibit help-seeking behavior. Ascribing to traditional masculine gender roles, which emphasize self-reliance and emotional suppression, can also discourage male first responders from acknowledging and addressing mental health struggles. This can increase their risk of suicidal ideation, anxiety, depression, PTSD, and resorting to problematic coping strategies such as aggression and substance use (Steyn and Klopper, 2020). Furthermore, access to mental health care in South Africa is limited, with services often concentrated in urban settings. The shortage of mental health professionals in the country can restrict the availability of effective support for first responders, particularly those working in rural communities (Booysen et al., 2021; Padmanabhanunni et al., 2022).
The Job-Demands Resource (JD-R) theory provides a conceptual framework for understanding the increased susceptibility for adverse mental health outcomes among first responders (Bakker & Demerouti, 2007). In terms of the theory, job demands refer to those aspects of the job that require sustained emotional, physical or mental effort and are associated with certain physical or psychological costs (e.g., emotional distress). Job resources entail aspects of the job that facilitate the achievement of work-related tasks, mitigate physical or psychological costs, and foster personal growth and development. This includes, for example, support from colleagues, clarity in work roles and tasks, and participation in decision-making. In terms of the model, the persistent exposure to high work demands—traumatic events, long working hours, and unpredictable events—can deplete the internal capacities and resources of first responders. In adequate job resources (e.g., limited organizational support or insufficient training) can aggravate the adverse effects of high job demands and lead to diminished wellbeing and increased risk of mental health challenges including PTSD, anxiety, depression, and substance use (Bonumwezi et al., 2022; Gryshchuk et al., 2022).
This study explored the levels of anxiety, depression, and PTSD among a sample of South African paramedics and police officers. The study also investigated the correlates of mental health outcomes emphasizing age, gender, work setting (urban or rural), relationship status, type of first responder, and length of service.
Method
Participants and procedure
Participants (n = 429) were police officers and paramedics, mainly from the Western Cape. We used Google Forms to construct an electronic version of the questionnaire described in the Instruments section of this article. We sought permission from the administrators of several Facebook groups consisting of first responders to post the electronic link on their Facebook page with an invitation to participate in the study. We also used research assistants to collect data in person by visiting police stations and hospitals to recruit participants and distribute the link.
The demographics of the sample are reported in Table 1.
Description of the sample.

Table 1 reflects that the majority of the sample were women (45%), worked in an urban area (92.3%), served in the police force (72.0%), and were married (51.5%). The mean age of the sample was 39 years (SD = 9.9), and the mean length of service was 13.2 years (SD = 9.7).
Instruments
Participants completed the following instruments: a brief demographic questionnaire, the Patient Health Questionnaire-9 (PHQ-9: Kroenke et al., 2001), the Generalized Anxiety Disorder-7 scale (GAD-7: Spitzer et al., 2006), and the PTSD Checklist for DSM-5 (PCL-5: Blevins et al., 2015).
The PHQ-9 is a nine-item self-administered questionnaire used to screen, diagnose, monitor, and measure the severity of depression. An example of an item of the PHQ-9 is: “Over the last two weeks, how often have you been bothered by little interest or pleasure in doing things?” Participants respond to the items of the PHQ-9 using a four-point scale ranging from not at all (0) to nearly every day (3). The authors of the PHQ-9 reported reliability coefficients of .89 and .86 in two separate studies and provided evidence for the construct validity of the instrument (Kroenke et al., 2001). Studies in South Africa have reported reliability coefficients of .76 among a sample of chronic care patients (Bhana et al., 2015) and .84 among a sample of students (Makhubela & Khumalo, 2023). The latter study also reported on the reliability of the PHQ-9 in student samples in Kenya (α = .82) and Uganda (α = .85). The authors of the PHQ-9 suggest the following classification of levels of depression based on PHQ-9 scores: less than 5 = no depression, 5–9 = mild depression, 10–14 = moderate depression, 15–19 = moderately severe depression, and 20–27 = severe depression. In addition, the authors suggest a cutoff score of 10 for diagnosing depression. In South Africa, some studies have used a similar cutoff score (Marlow et al., 2023; Mkhize et al., 2024). However, Bhana and colleagues (2015) conducted a receiver-operating curve (ROC) analysis and found an optimal cutoff score of 9 among a sample of chronic care patients in South Africa.
The GAD-7 is a seven-item questionnaire used to screen and measure the severity of generalized anxiety disorder. An example of an item of the GAD-7 is: “Over the last two weeks, how often have you been bothered by becoming easily annoyed or irritable?” The response format for the GAD-7 is a four-point Likert-type scale ranging from not at all (0) to nearly every day (3). In the original development study, the authors reported an internal consistency estimate of .92 and provided evidence for construct, criterion, and factorial validity. In South Africa, two different studies of university students (Tadi et al., 2022) and working adults (Henn & Morgan, 2019) reported reliability coefficients of .89 and .92, respectively. Spitzer and colleagues (2006) suggested the following classification of levels of anxiety based on GAD-7 scores: less than 5 = no anxiety, 5–9 = mild anxiety, 10–14 = moderate anxiety, 15–21 = severe anxiety. In addition, the authors suggest a cutoff score of 10 for diagnosing generalized anxiety disorder. In South Africa, studies have largely used the same cutoff score of 10 (e.g., Mkhwanazi & Gibbs, 2021). However, Marlow and colleagues (2023) reported a lower cutoff score of 6 for an isiXhosa version of the GAD-7 using a ROC analysis among a sample of adolescents in South Africa.
The PCL-5 is a 20-item measure that is used to assess the presence and severity of PTSD symptoms. An example of an item from the PCL-5 is: “In the past two years, how much were you bothered by trouble remembering important parts of the stressful experience?” The PCL-5 is scored on a five-point scale ranging from not at all (0) to extremely (4). In their study on the development and validation of the PCL-5, Blevins and colleagues (2015) reported an internal consistency estimate of .94 and provided evidence of convergent and discriminant validity. In South Africa, Padmanabhanunni and Pretorius (2024) reported an alpha coefficient of .94 and used a Mokken analysis to demonstrate that the PCL-5 is essentially unidimensional. It has been suggested that when using average PCL-5 scores (i.e., summed score/20), the following descriptors can apply: less than or equal to 1.23 = normal, 1.23–1.64 = mild, 1.64–2.455 = moderate, 2.455–3.265 = severe, and greater than 3.265 = extremely severe (NovoPsych, 2023). The National Center for PTSD (2023) in the United States suggests that a total PCL-5 cutoff score from 31 to 33 would indicate probable PTSD. Similarly, Kagee and colleagues (2022) used an ROC analysis and reported an optimal cutoff score of 32 to detect PTSD among HIV patients in South Africa, while Verhey and colleagues (2018) reported a cutoff score of 33 in a primary care population with high HIV prevalence.
Ethics
The study received ethical clearance from the Humanities and Social Sciences Ethics Committee of the University of XXXX (Reference Number: HS23/2/4, 18 October 2023) and was conducted in accordance with the guidelines of the Declaration of Helsinki. In addition, we received an ethics clearance from SAPS (Reference number: 3/34/2). We also received approvals from the Western Cape government to access healthcare facilities (Reference: WC_202307_041) and permission from a private emergency response company to approach their employees (Reference: 20231124). Participants provided informed consent on the landing page of the electronic instrument. Participation was entirely voluntary, and participants did not receive any compensation for participating. No personal information was collected during the research process.
Data analyses
All statistical analyses were conducted using IBM SPSS for Windows, version 29 (IBM Corp., Armonk, NY, USA). We examined the distribution of the data using indices of skewness and excess kurtosis. Data are considered to be approximately normally distributed if skewness values range from −2 to +2 (Hair et al., 2010) and kurtosis values from −1 to +1 (Illinois State University, 2023). We also obtained estimates of internal consistency (Cronbach’s alpha and McDonald’s omega) and descriptive statistics (means and SDs). We compared the means obtained in this study with those of other studies that included samples from the African continent and other international studies using a one-sample t-test.
We used the cutoff scores reported in the literature to determine the prevalence of depression, anxiety, and PTSD in terms of percentages. We also used the previously reported classification levels to describe levels of depression, anxiety, and PTSD in terms of percentages.
Finally, we used multiple linear regression to determine whether any of the demographic variables was a significant predictor of the indices of mental health disorders. In this regard, categorical variables with more than two categories (i.e., work setting and relationship status) were dummy coded.
Results
Reliabilities and descriptive statistics
Cronbach alpha values for the PHQ-9, the GAD-7, and the PCL-5 were .89, .92, and .95, respectively. McDonald’s omega values were the same as the Cronbach alpha values for the PHQ-9 and the GAD-7 but slightly lower for the PCL-5 (.94). The descriptive statistics and a comparison with national and international studies are reported in Table 2.
Descriptive statistics and comparison with previous studies.

p < .001.
First, Table 2 reflects that the skewness values were within the acceptable range of −2 to +2 (0.09 to 0.38), and excess kurtosis was within the range of −1 to +1 (−0.81 to −0.49). These findings indicate that the data for all the scales were approximately normally distributed. Furthermore, Table 2 indicates that there were significant differences between the means for this sample of first responders and an international sample in terms of depression, a South African study in terms of anxiety, and a South African and an international sample in terms of PTSD.
Prevalence of mental disorders
Using a cutoff score of 10, we found that almost half of the sample (47.3%) would qualify for a diagnosis of depression. The classification of the levels of depression in the current sample is shown in Figure 1 and indicates that 24.9% of the sample reported moderate levels of depression, 15.4% moderately severe depression, and 7% severe depression.
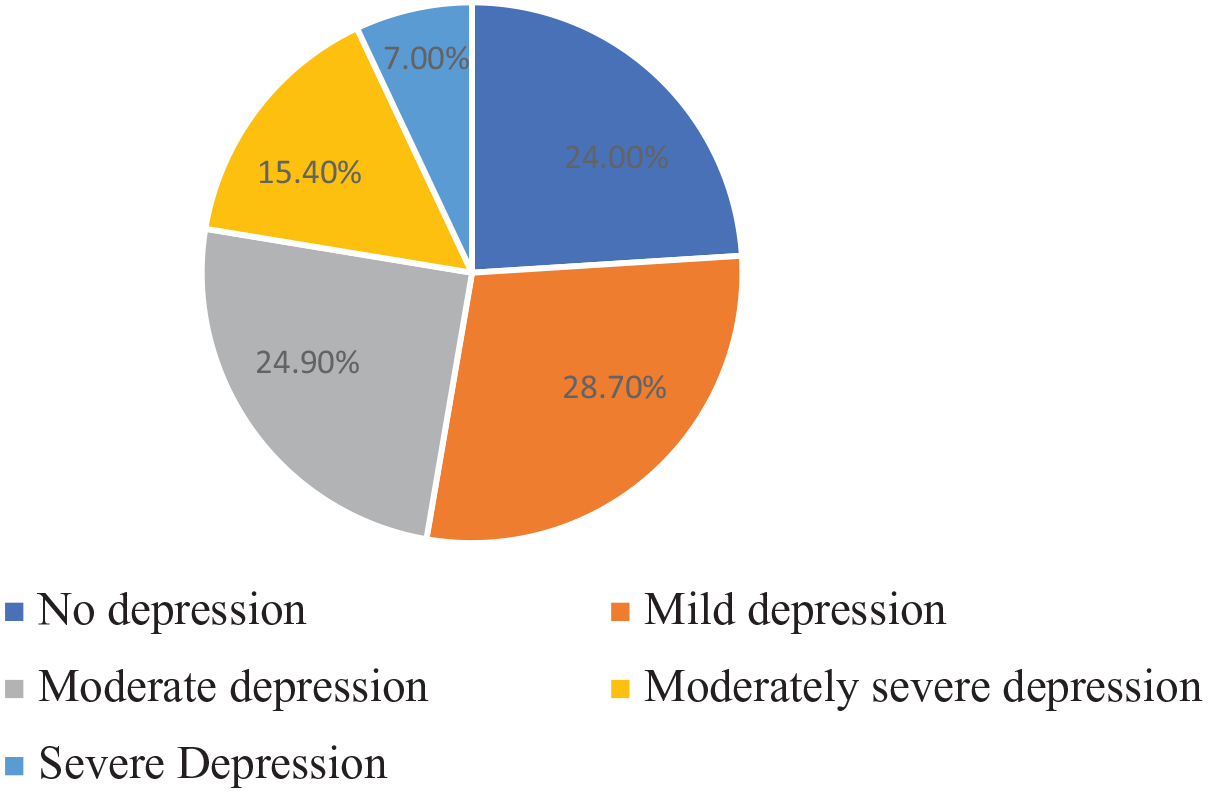
Classification of levels of depression.
A cutoff of 10 resulted in 37.8% of the sample being eligible for a diagnosis of generalized anxiety disorder. The classification of levels of anxiety is shown in Figure 2 and indicates that 24.7% of the sample reported moderate anxiety and 13.1% severe anxiety.
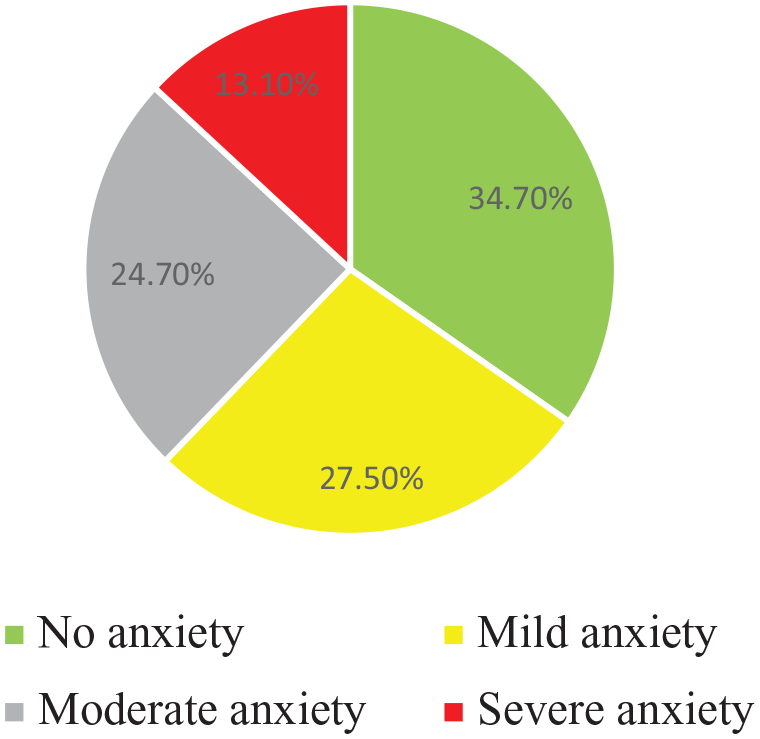
Classification of levels of anxiety.
For the PCL-5, we used a cutoff score of 33 and found that 48.5% of the sample would meet the criteria for a diagnosis of PTSD. The classification of levels of PTSD is shown in Figure 3 and reflects that 34.5% of the sample reported moderate PTSD, 11.4% severe PTSD, and 2.6% extremely severe PTSD.
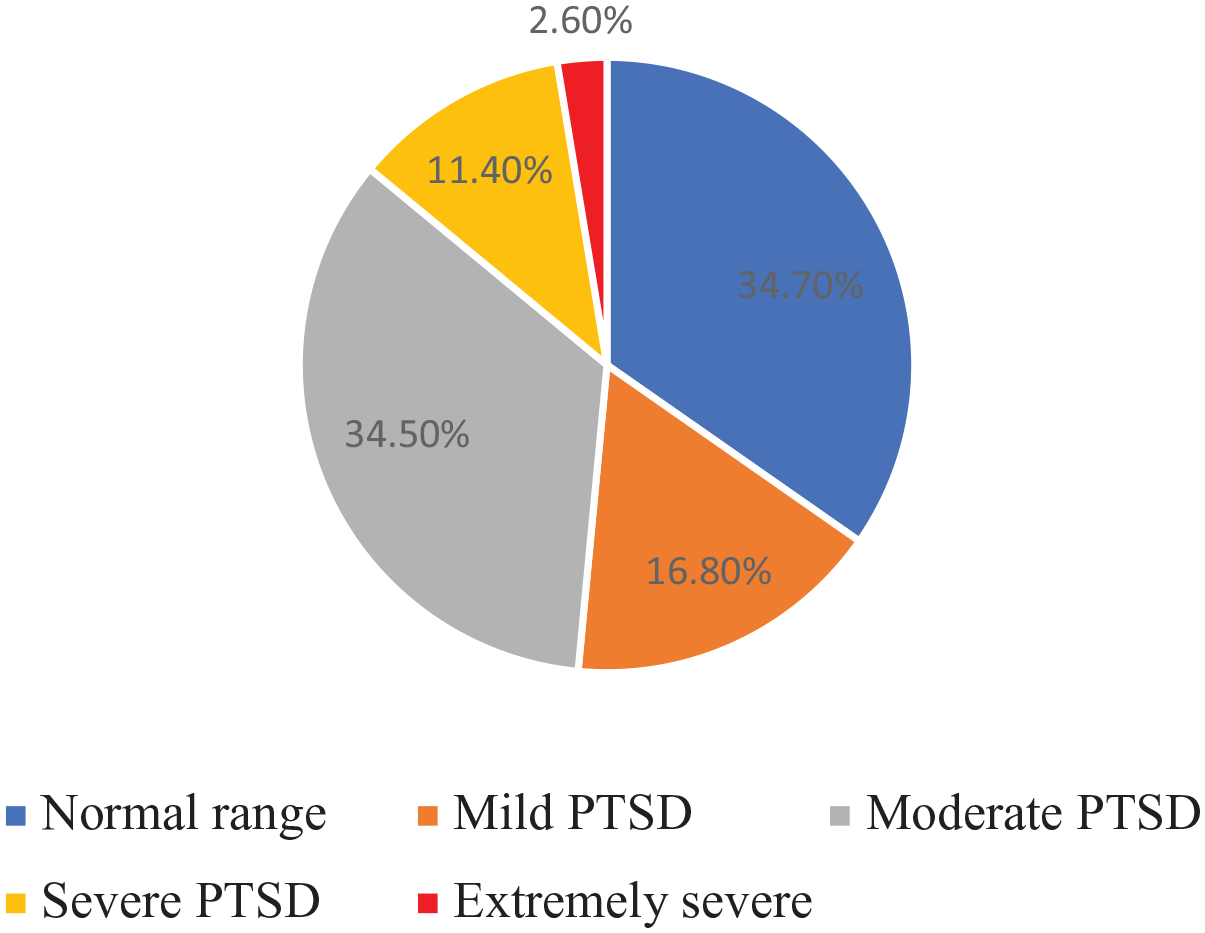
Classification of levels of PTSD.
Predicting mental health disorders
The results of linear regression with the indices of mental health as dependent variables and demographic variables as predictors are reported in Table 3.
Predictors of mental health outcomes.

PTSD: post-traumatic stress disorder.
Reference category is urban.
Reference category is single.
p < .05.
Table 3 indicates that there were no significant demographic predictors of anxiety or PTSD. The only significant predictor of depression was being divorced or separated. The positive beta coefficient indicates that those who were divorced or separated were more likely to be depressed than those who were single (the reference category).
Discussion
International research has established that first responders experience adverse mental health outcomes at a higher rate compared to the general population (Kyron et al., 2022; Vujanovic et al., 2021). However, research on first responders in South Africa is significantly lacking. This study provides the most current evidence on the mental health status of first responders in South Africa, a population group that is routinely exposed to high levels of occupational stress. The findings highlight alarmingly high levels of depression, anxiety, and PTSD, underscoring the pressing need for targeted interventions.
First, nearly half of the sample (47.3%) would qualify for a diagnosis of depression based on established cutoff scores. This rate is significantly higher than that found in the general population (Kocalevent et al., 2013), highlighting the substantial burden of depressive symptoms among first responders. The high prevalence also suggests that many first responders may be struggling with the demands of their roles without adequate coping mechanisms, which can lead to diminished job performance and increased risk of burnout (Haugen et al., 2017). Being divorced or separated was a significant predictor of depression and this further confirms the salient role of social support in mental health outcomes. The absence or loss of close social connections, as seen in those who are divorced or separated, may leave individuals more vulnerable to depressive symptoms (Proescher et al., 2022; Wang et al., 2018).
Second, 37.8% of the sample met the criteria for generalized anxiety disorder and reported higher levels of anxiety than an international sample of the general population (Kocalevent et al., 2013). This finding indicates that more than a third of the first responders are experiencing pervasive and excessive anxiety, which may be linked to the unpredictability and intensity of their work. The high rate of generalized anxiety among first responders suggests that the pressures of their responsibilities, combined with the constant exposure to potentially life-threatening situations, create a sustained level of psychological distress that can significantly impact their overall well-being.
Third, almost half the sample (48.5%) would meet the criteria for a diagnosis of PTSD. Although this level is lower than trauma survivors in South Africa (Joubert et al., 2022) and a sample of first responders in the United States (Morrison et al., 2021), it remains a significant health concern. The relatively lower level may reflect differences in the nature of exposure to traumatic events or variations in reporting of symptoms. Nevertheless, PTSD is associated with severe and potentially debilitating symptoms, including intrusive memories, hypervigilance, emotional numbing, and avoidance behaviors, all of which can significantly impair the ability of a first responder to function in both their personal and professional lives (Brewin et al., 2022).
These findings paint a stark picture of the mental health challenges faced by first responders in South Africa. The high prevalence rates of depression, anxiety, and PTSD in this study suggest that these individuals are at a substantial risk of experiencing long-term mental health problems. It also raises important questions about the accessibility and effectiveness of mental health support services for first responders. For instance, SAPS has implemented various services and programs under the EHWS including mental health care, interventions focusing on stress-management, and crisis intervention, and suicide prevention programs. However, there is evidence to suggest that these services are under-utilized (Mushwana et al., 2019).
Several factors may contribute to this situation. Limited awareness of mental health conditions can hinder recognition of when professional help is needed. In addition, stigma surrounding mental illness remains a pervasive barrier, often preventing first responders from seeking support due to fears of judgment, perceived weakness, or potential career repercussions. Furthermore, concerns about confidentiality and the potential for sensitive information to be disclosed within the workplace may further discourage help-seeking behavior. The culture of self-reliance, deeply ingrained in first responder communities, may contribute to pressure to manage their mental health on their own rather than seek external assistance (Haugen et al., 2017; Jones et al., 2020).
These challenges underscore the need for contextually relevant and culturally appropriate interventions aimed at addressing social stigma, challenging problematic gender roles that discourage help-seeking behavior and enhancing access to mental health resources. Existing studies have reported that increased mental health literacy, the use of online educational resources on mental health, and peer-led interventions can improve help-seeking attitudes, which is a precursor to help-seeking behavior (Ahorsu et al., 2021; Hofer & Savell, 2021). Furthermore, cognitive bias modification interventions that target underlying maladaptive appraisals of inadequacy or fears of judgment, can reduce barriers to accessing care (Trombka et al., 2021). Integrating these interventions into existing mental health support programs could potentially enhance their reach and effectiveness.
The study had several limitations. First, the cross-sectional design limits the ability to infer causality or understand the longitudinal progression of mental health disorders. Second, the study relied on self-reported data, which can be subject to social desirability bias, recall bias, or inaccuracies in reporting. Participants might underreport or overreport their symptoms due to stigma, fear of judgment, or misunderstanding of the questions. Third, while the study used validated cutoff scores to estimate the levels of mental health disorders, it did not include clinical interviews or diagnostic assessments by mental health professionals. This approach may result in either overestimation or underestimation of the true rates of these disorders. Finally, the study focused primarily on first responders from the Western Cape Province, which may limit the generalizability of the findings to other regions of South Africa.
Conclusion
This study highlights the significant mental health challenges faced by first responders in South Africa, revealing concerning levels of depression, anxiety, and PTSD within this critical workforce. The findings underscore the urgent need for targeted mental health services and interventions to address barriers to help-seeking among this population group.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.