
Abstract
Developmental Coordination Disorder (DCD) is a fairly common neurodevelopmental motor disorder resulting in challenges with the acquisition and execution of motor skills that impact academic productivity, leisure, and play. Although DCD is typically only diagnosed in one member of the family, the multi-domain and lifelong obstacles created by this disorder influence the entire family unit. However, families are seldom offered post-diagnostic support. Therefore, the objective of this study was to identify the support required by families journeying with DCD. To achieve this, a descriptive qualitative study was used to describe the experiences of families. Families (n = 44, from eight countries) completed an online questionnaire and participated in semi-structured interviews (n = 12). The families indicated three key areas of support which they believe would be beneficial. The sharing of information which is easily accessible, understandable, includes practical examples, and location-specific support services was crucial in supporting families. Families stressed the need for informative collaboration with healthcare and education sectors to promote greater awareness so that less parental advocacy on behalf of the patient is required. Since families frequently feel isolated, support in developing connections both online and with other families in similar geographical locations is crucial for sharing ideas and interacting, so that the journey with DCD is not walked alone. These findings indicate a broader and deeper understanding of the psycho-social support required by families with guidelines for psychologists working with DCD individuals.
Keywords
Introduction
Although Developmental Coordination Disorder (DCD) is a common neurodevelopmental disorder affecting 5% to 6% of school-aged children (American Psychiatric Association [APA], 2022), it is typically only diagnosed in one member of the family. The chronic obstacles characterising DCD influence the entire family unit, yet families are seldom offered sufficient support pre- and post-diagnosis. DCD is primarily a motor functioning disorder where individuals exhibit gross and fine motor skills that are substantially lower than age expectations, resulting in challenges with daily living and school activities (APA, 2022). These motor skills deficits often lead to further emotional, social, and behavioural challenges (Cairney et al., 2013). Since being identified in 1962 as ‘clumsy children’ (British Medical Journal), the last six decades have seen increasing focus on understanding the clinical symptoms and effects on academic and behavioral functioning (Farmer et al., 2016). Despite a greater understanding of the extent of the motor skills deficits, children with DCD are still overlooked both in the education and medical spheres and families encounter daily struggles in relation to obtaining tailored psycho-social support (Meachon et al., 2023).
Developmental coordination disorder
The symptoms displayed by children with DCD were first viewed primarily as a medical condition with ‘minimal brain dysfunction’ (Grant, 2017), ‘dyspraxia’, and ‘specific developmental disorder of motor function’ (Esser, 2012). In 1995, the term, developmental coordination disorder, was accepted as the official term (Polatajko et al., 1995). Despite clear criteria for diagnosing DCD (APA, 2022), the subtle, hidden symptoms are frequently overlooked (Missiuna et al., 2007) and often misdiagnosed (Klein, Licari, et al., 2024).
DCD is a chronic neurodevelopmental disorder with 50% to 70% of individuals continuing to experience challenges into adulthood (Sadock et al., 2015). DCD has a multi-domain impact (Meachon, 2023) as documented in the diagnostic criteria of the DSM-5-TR (APA, 2022). The diagnostic criteria note challenges with the acquisition and execution of motor skills that impact academic productivity, leisure, and play (APA, 2022). Specific effects of these motor skill deficits may include challenges with handwriting, and speech articulation (Winson & Fourie, 2020), which result in inaccurate written and verbal reflections of the individual’s cognitive capabilities (Prunty et al., 2016). Challenges with executive functioning may occur (Lachambre et al., 2021; Meachon et al., 2022) as well as difficulties with concentration (Farmer et al., 2016). DCD may be a primary stressor placing the individual at risk of interpersonal and intrapersonal difficulties (Blank et al., 2019; Meachon et al., 2022) and decrease self-confidence while elevating anxiety and depression (Saban & Kirby, 2019). Increased anxiety levels often exacerbate difficulties with motor planning (Harris et al., 2022). These physical and emotional struggles ripple through all domains of functioning and place a heavy burden on parents and carers (Klein, Licari, et al., 2024). DCD affects not only the individual diagnosed with the condition but also the entire family (Mancini et al., 2024).
Long before obtaining a DCD diagnosis, concerns may arise. Parents may begin to identify subtle differences between their child’s development and that of other children, resulting in uncertainty as to whether to consider the differences problematic or simply due to variations in development (Missiuna et al., 2006). Should these observations be shared with a healthcare professional, parents may find their concerns dismissed (Klein et al., 2023). On average, a DCD diagnosis is received after two-and-a-half years after the diagnostic process was initiated by families (Soriano et al., 2015).
After a diagnosis has been shared, families often find navigating the education and healthcare systems in search of support riddled with obstacles (Missiuna et al., 2006). Due to the time spent advocating for their child and attending supportive therapy sessions, mothers, in particular, may find that they are required to reduce work hours or change careers to have greater time available to assist their child (Cleaton et al., 2019). The time spent supporting an individual with DCD has been identified as a key stressor for mothers (Stephenson & Chesson, 2008). Mothers report elevated levels of worry, stress, anger, and frustration resulting in emotional fatigue and feeling drained (Cleaton et al., 2019). However, fathers and siblings also experience emotional strain (Stephenson & Chesson, 2008), and up to half of families report dissatisfaction with their family’s emotional well-being (Cleaton et al., 2019).
Families may find that DCD impacts their ability to participate in family activities, make holiday plans, and engage in social gatherings (Cleaton et al., 2019). A study in Australia reported that children’s motor difficulties influence their self-care, dressing, eating, and sporting activities, often resulting in home schooling and feelings of being unsupported (Reynolds et al., 2024). Although parents fear exposing their children to repeated failures resulting in reduced self-esteem, they are also concerned that a lack of participation and social interaction may hamper self-concept development (Missiuna et al., 2006). Parental fears of non-participation and social withdrawal were found in children with a single diagnosis of DCD and those with multiple co-occurring diagnoses that impact the whole family (Mancini et al., 2024). DCD influences the child throughout the lifespan, and particular care for adolescents in fostering social connections as they enter adulthood should be considered in standards of care (Khairati et al., 2024).
International clinical practice recommendations on the definition, diagnosis, assessment, intervention, and psychosocial aspects of DCD point to parental support as an important factor in the effective outcome of intervention, and list parental guidance as the 30th recommendation (Blank et al., 2019).
In South Africa, the Green Paper on Families: Promoting Family Life and Strengthening Families in South Africa (Department of Social Development, 2011) explains that focusing on supporting families rather than targeting individuals would have greater positive outcomes. In addition, the policy on Screening, Identification, Assessment and Support (SIAS) acknowledges the pivotal role that parents and caregivers play in the early identification of learning problems (Department of Basic Education [DoE], 2014). The SIAS policy advocates for family empowerment to have greater insight into the optimal development of the child (DoE, 2014). In families where parents and siblings understand the strengths and abilities of the individual with DCD, the daily journey with this condition tends to be easier, and there is greater participation in activities within the home and community and positive self-understanding (O’Dea et al., 2021). However, when the family unit is unsupportive of the child with DCD, there tends to be conflict in the home, negative self-perceptions, and reduced participation in activities (O’Dea et al., 2021).
Although it has been identified that pre- and post-diagnostic support for the family is crucial for effective treatment of the individual (Blank et al., 2019; Soriano et al., 2015), there is little understanding of the unique support required by families as they navigate the invisible and subtle difficulties presented by this condition. Since an individual’s well-being and ability to function optimally are interrelated with societal contextual factors (Froggett & Richards, 2002), this study explored the psychological and social support required by families journeying with DCD.
Method
This study used a descriptive qualitative design (Creswell & Creswell, 2022) to explore the experiences and support needs of families journeying with DCD. Ethical clearance for the study was granted by the University of Johannesburg, Faculty of Education Research Ethics Committee (Sem2-2020-019). Ethical considerations included maintaining the participants’ rights to privacy, withdrawal, anonymity, confidentiality, informed consent, and non-malevolence.
Participant sampling and recruitment
Since participants were purposively sampled, they met key criteria for participation in the study. Participants needed experience of DCD within the family context. This included parents raising children with DCD who were able to share their current support needs as well as adults with DCD who were able to reflect on their family’s journey with DCD. Participants were not excluded if the family structure did not conform to a traditional family structure nor were participants excluded on grounds of the presence of co-occurring disorders. Although different countries have varying educational and health policies, the focus of this study was on the general support required by families journeying with DCD. Families from different countries were thus allowed to participate in the study.
Recruitment of participants in South Africa proved challenging. Remedial schools, multidisciplinary practices, paediatricians, and healthcare practitioner associations were contacted. However, no participants were obtained through these means. Thus, the researcher turned to social media and an advertisement was posted on six Facebook groups which specified that they were related to DCD or dyspraxia. These sites were, ‘Dyspraxia – dyspraxic adults surviving in a non-dyspraxic world’, ‘Developmental coordination disorder’, ‘Dyspraxia/DCD and ADHD’, ‘Dyspraxia awareness’, ‘Dyspraxia support group’, and ‘Dyspraxia about’. In addition, the advertisement was posted on two Facebook groups which cater specifically for allied healthcare practitioners in South Africa, namely, the ‘SA Psychologists Resources and Discussion Group’ and ‘Allied health in South Africa (Professionals only)’.
To specifically target families, the advertisement detailed the background of the study and presented a live link to an online questionnaire. This was posted on the above six social media groups and two social media groups associated with the allied health profession in South Africa. The online participant recruitment and data collection methods used were due to this study being conducted during the COVID-19 pandemic, while restrictions on interpersonal interaction were in place.
Participant biographical details
This participant recruitment method resulted in the completion of 44 questionnaires, from eight countries. Demographic characteristics show that participants were mostly Caucasian, females, between the ages of 20 and 50 years old, with a tertiary qualification (Table 1). Parental levels of education were relevant as education generally gives access to sources of information, and empowers parental advocacy. Twenty-three participants had a biological son with DCD, 10 had a biological daughter with DCD, and 16 experienced DCD themselves. Each participant was assigned a participant number.
Demographic information of participants.

N = 44.
Data collection methods
This study used an online questionnaire consisting of forced-choice and open-ended questions, conducted via Google Forms between January and June 2021. Data saturation was reached when it was noted that newly completed questionnaires contributed towards already identified themes rather than producing new ideas.
The first page of the questionnaire contained detailed information regarding the study as well as participant requirements. It explained the rights of participants and requested their consent before the questionnaire was completed further. It also included an item requesting the participants’ names and signatures.
The forced-choice questions pertained to demographic information, the family member with DCD, whether the DCD had been formally diagnosed or is suspected, who made the DCD diagnosis, a rating for the healthcare and the family’s understanding of DCD, through whom support was provided, and the usefulness of the support provided. The open-ended questions included the opportunity to describe the challenges which lead to seeking a diagnosis of DCD, the diagnostic process itself, the impact of DCD on the family, support that has been offered, and skills that would have been useful to navigate the journey with DCD more successfully. This provided the families with the opportunity to share their lived experience of journeying with DCD.
Once a questionnaire had been completed, the participant was given the opportunity to provide their contact details should they have wished to participate in a follow-up semi-structured interview. Twelve participants agreed to participate in an interview which was conducted online. Again, before the interview was conducted, the researcher discussed the study with the participants, reminded them of their rights, and obtained informed written consent before the interview commenced.
Participants 1 to 12 completed the online questionnaire and participated in an online interview. Of these, 4 participants were living with DCD themselves. Participants 13 to 44 only completed the online questionnaire.
The researcher conducted the semi-structured interviews via Zoom. Interviews lasted a minimum of half an hour. The data from the questionnaires informed the specific questions asked during the interview giving the researcher the opportunity to consider which questions would elicit further relevant information before conducting the interview. Although the participants were all asked questions that were unique to their previously presented information, some questions were asked of all participants. These questions included: What support have you found most useful on this journey? What support do you wish you had obtained earlier in this process? What advice would you give to a family who is just starting out on this journey?
Data analysis
The thematic content analysis took place (Creswell & Creswell, 2022) where all data were collected and initially analysed by the first author. The data collected from the online questionnaires were stored in an Excel spreadsheet. Otter.ai was used for the verbatim transcription of interviews. The transcriptions were reviewed for accuracy by an independent transcriber. The open-ended questions from the questionnaires and the transcribed interviews were uploaded into Atlas.ti for coding. Code categories, such as ‘awareness’, ‘support desired’, and ‘support obtained’ were used to identify the patterns within the data. Raw data transcripts and coding were then verified by the second author, and consensus was reached regarding the final codes. The coded data units were then reassembled into themes, agreed on by both authors, so that the interpretation of the data could take place.
Credibility, trustworthiness, and dependability
The trustworthiness of the findings was ensured by means of various strategies as posited by Lincoln and Guba (1985). Credibility was established by triangulating qualitative data from questionnaires and interviews with a wide range of participants. Questionnaires were completed personally by the participants, and audio recordings of the interviews and accurate transcriptions aided dependability. Credibility was further achieved with a member-checking strategy (Creswell & Creswell, 2022), whereby participants were given the opportunity to review the analysed data, via an email sent, to confirm the accuracy of the findings. Only three participants responded to the email and confirmed that the themes resonated with their personal experiences.
Findings
The focus of this study was to identify the support required by families journeying with DCD. Three common themes emerged: the availability of accessible and practical information; increasing awareness and understanding of DCD, and building strong social connections.
Theme 1: availability of accessible and practical information
According to the questionnaire responses, 48% of families reported receiving no support thus far in their journey with DCD. Of the remaining 52% who had received support, this tended to have been self-sought. When asked what support families require, a range of areas were raised, as summarised in Figure 1.
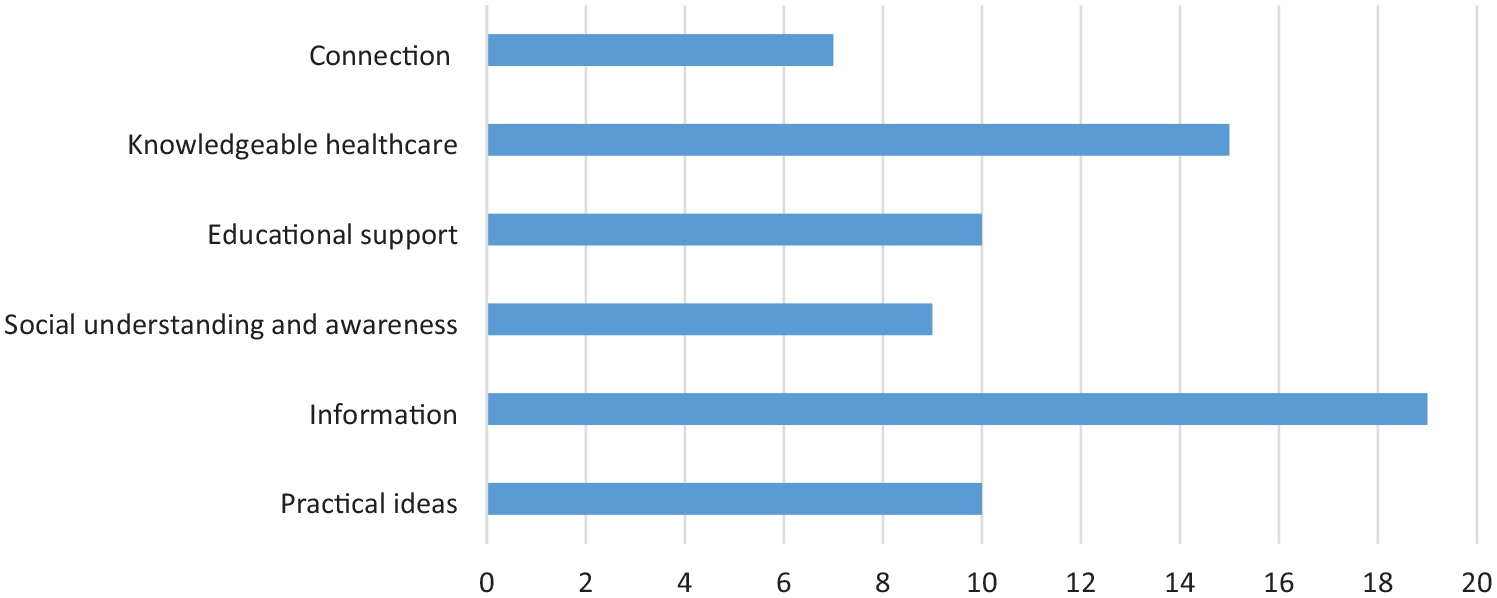
Support requested by participants.
The key areas identified as requiring support included, the provision of accurate information, knowledgeable healthcare providers, aware educators, greater connection with other families, and practical ideas.
A primary means through which families can be supported is through the provision of easily accessible, accurate information with practical strategies. One participant pointed out that
The greatest challenge is learning about DCD. (P27 USA)
Another participant stated,
It’s like you’re walking in a dark cave and the only thing you have to get around is the light on your phone. It’s like where do we go now? We’re getting these little snippets of information. (P1 USA)
Families are searching for information that is easy to read, understandable, current and from experts in the field:
We need information that is easy to understand because I don’t do well with all the scientific journals, they’re just boring as hell. (P2 AU)
While another participant desired,
Basic information, to make it as simple as possible for other people to understand. (P5 USA)
Another participant explained that
We need more practical layman’s knowledge on DCD. (P12 ZA)
A participant’s career allowed access to information:
I think the co-workers that I work with, because they’re all in the same disability type of community they have been my biggest resource. (P7 USA)
Another person explained that their friendship with an occupational therapist resulted in access to invaluable information. However, many families are not able to access information via friends or the workplace and rely on social media or the internet for information. For example,
Through Facebook groups and old Yahoo groups, I really educated myself on the condition. (P9 USA)
However, as a parent explained, this can result in information being obtained by chance:
I think it is important to include the other members of the family in understanding what the diagnosis is . . . because when you have multiple people believing in and supporting the child who is floundering, there is a much higher chance of that child succeeding and, it also makes everybody else feel better too . . . each member gets positive feedback from helping the others. (P11 CA)
Information needs to inform parents, siblings, and extended family members. The family will be able to support the various members to a greater extent when each family member has the information necessary to develop understanding.
Participants needed to know what specific support services were available. For example,
Knowing what supports are available to us as parents would have been good. I didn’t even know about occupational therapists until we were referred to one. (P2 AU)
Families may find it difficult to locate information that is relevant to their specific location. One participant pointed out that
Most of the information that I could find was all like UK-based research. I needed psychologists to help in my state. (P5 USA)
Families would like information pertaining to the multi-domain influence of DCD. One participant explained that
We need more info on all the related difficulties. When we first learned of the diagnosis it was mostly fine motor skills but now we know a lot of other motor planning and emotional regulation issues are related to DCD. (P5 USA)
Another participant added that she would like:
More information about the learning side, not just focus on balance and motor skills. Like help with his planning of studying, he gets anxious with large chunks to learn rote. (P14 UK)
Families are looking for information that is useful for everyday tasks and daily life as this condition is taxing.
A participant shared that
We need resources, training, education, and more material with suggestions on what to do with him. Even like a website that just explains the different activities that you can try. (P3 ZA) [Child with DCD] needs better organisational skills but I don’t know how to help him with this. (P6 USA)
Specific information pertaining to parenting a child with DCD would also be useful for families. This includes information that would respond to a question like:
How do we parent a child with DCD? He can’t do what other kids do easily and gets so frustrated with himself. (P11 CA)
Families are looking for information which they can share with the teachers:
We need reading material guiding how we can actively support him, similarly for his teachers, a quick brochure explaining what to do in class. (P32 ZA)
Another participant explained that parents and teachers have different needs when searching for information regarding DCD. She explained that
We want to understand what’s going on and what causes it, . . . (but) for the teachers, they just need to know how to help him. What pencils to use and how to pace learning, things like that. (P5 USA)
Parents are often required to provide information to teachers. Having practical strategies readily available will assist with alleviating the pressure of continually having to advocate for the child in the classroom.
Families were also interested in the real-life stories of other families journeying with the condition. One participant explained that
Stories of how other people have dealt with kids in similar situations and how they’ve come out the other side because, it can be terrifying to think, ‘Is this my life now, is it gonna get better?’ (P2 AU)
The stories of others navigating DCD can assist in bringing hope to those who are struggling on their journey. When parents feel informed, they can better understand the condition, access resources, and apply practical strategies. This, in turn, assists the other family members in approaching life’s challenges with confidence. For example,
If I’m informed and confident, then I can say to him, ‘It’ll be fine because we’ve got this and this and this’. (P10 UK)
While information on DCD has typically focused on the medical and physical aspects of the condition, families are interested in access to information that provides insight into the challenges associated with DCD. Families requested information that is easily understood, location-specific, practical in nature, and includes suggestions for teachers and professionals in healthcare.
Theme 2: awareness and understanding of DCD in society, healthcare and education
When considering the support required by families journeying with DCD, the second key area in which families feel support is required is of increased awareness and understanding of the condition and what the disorder entails. Awareness in society in general and specifically within the healthcare and education systems would result in the family unit as a whole feeling more supported. Poor understanding of DCD negatively impacts the willingness of families to participate in social events. A participant shared that
I would like to have more social awareness of this. Often in our social circles people expect my son to behave as typical children do, and when he gets frustrated they often perceive this as misbehaviour. (P32 ZA)
A participant pointed out that
Social awareness can definitely help to include the kids without having to fight for their rights all the time. (P31 EG)
Parents are often faced with having to explain DCD to their healthcare providers, incurring unnecessary consultation costs:
More education of physicians to know about the diagnosis, so it doesn’t take so long with so much expense. (P1 USA) I think, from a paediatrician point of view, it might be good if they knew what to look out for and what they could try so they don’t miss it. We spent a lot on wasted medical consultations. (P3 ZA)
Healthcare content on DCD should be included in the pre- and in-service training of healthcare professionals, especially doctors and psychologists, as these practitioners make diagnoses. Knowing that a family member is effectively supported by their healthcare team can assist the whole family and reduce stress. A participant explained that
Knowing that she has good therapies in place and good therapists where she’s making progress, that’s helpful to me because I feel like if she’s better, I’m better. (P2 AU)
Participants shared that
Just having that medical professional validate and say, ‘Yes, this is what he has’. (P6 USA) Validation that this is real . . . would be helpful, we would know how to help. (P16 ZA)
Healthcare professionals can guide the family with realistic expectations. A participant commented,
He gave me ideas for parenting, how to do it differently. He gave me different books to read. . . and another main thing was, he helped me to have more realistic expectations. (P6 USA)
Healthcare providers working as part of a multidisciplinary team provide cumulative support as participants commented,
She [the occupational therapist] confers and speaks to the paediatrician quite a lot . . . it’s a group effort. (P3 ZA) I’ll get advice from his occupational therapist because she is very, very positive and willing to liaise with teachers and other professionals. (P11 CA)
Healthcare professionals can assist in setting realistic goals and timeframes and navigating potential obstacles:
Having the expectation that they’re going to catch up and be where they’re supposed to be, you have to let go of that a little bit. He will learn it, but because it takes him longer, he’s not suddenly going to be cured. Like they let me know he will have serious difficulty driving a car, the complex mechanics of moving his hands and feet and the car, all this simultaneously he will battle with this. (P5 USA)
Families can be supported further when they encounter knowledgeable and empathic educators, as indicated by one of the participants:
I wish that teachers and early childhood teachers knew what DCD was, so they would just make small adjustments in school, like less written tasks. Then we’d all be less frustrated. (P20 AU)
When teachers understand DCD, they can make classroom modifications. Families shared their frustrations, stress and behind-the-scenes advocacy in relation to ensuring that the child was supported at school:
It’s frustrating, sometimes, as parents we feel like we’re constantly trying to start again, every year with a new teacher, explaining things. (P11 CA) It was always stressful meeting his new teacher and going through everything again about what DCD was. It’s just not something commonly known. (P20 AU)
When teachers display an understanding of DCD, parents are no longer required to continually explain the condition to every teacher. Families are not always aware of the procedures to be followed in the education system to obtain the required additional support. A parent stated,
I wish I’d understood how the education system works (or doesn’t) in terms of special educational needs earlier – having to fathom it out as I go along has been very hard, stressful and time consuming without particularly great results. (P35 UK)
Educators can actively guide families through the paperwork process required to obtain support, such as applying for additional time concessions. A participant explained,
There is an appreciation for having the IEP [Individual Education Plan] services that give us some grace so that we can relax a little bit and not worry that my child’s behind. He now gets additional time to do tests which helps a lot. (P5 USA)
Families can be supported to a greater extent when teachers display an understanding of DCD, and an availability to guide parents through the required support processes. This can reduce the amount of time required to advocate on behalf of the child, as well as assist with lowering family stress and frustration.
Theme 3: creating social connections
Following from the desire for awareness and understanding within society, healthcare and education, families journeying with DCD, also indicated the need for social connections with others who are encountering similar challenges. Families can be supported through connection with other similar families, to counter the feelings of isolation, as explained below:
I think connecting with other families would be super helpful. (P1 USA) I think it would be nice to have another parent to talk to. If there was someone we could talk to and relate to and see what they’re being challenged with and how they overcame the challenges. (P3 ZA)
Families who have engaged with other families, in person or online, described the experience as useful for sharing information and building social connections:
I keep looking online for different support groups . . . they have been really helpful, just ideas and knowing you are not the only parent out there. (P11 CA) I think a good thing about the Facebook group is I can ask questions, and I get instant feedback on what I’m looking for. Like I wanted to know about his totally disorganised room and school bag, and I got some good ideas to help him. (P9 USA)
This immediate feedback contrasts with the extended time periods families contend with when interacting with healthcare and education professionals. Although online connection was supportive for some families, others would prefer connection with families in closer proximity so that local resources and services can be shared. A participant shared,
We have a DCD society in New Zealand who sound great, but they are in the South Island and here is no local support nearby us in the North. We really can’t afford the shoe inserts and need advice with the weighted blanket for sleeping. (P28 NZ)
The development of community specific support networks would assist with alleviating the sense of isolation experienced while providing an opportunity for the sharing of information and resources, such as orthotics for devices, such as braces, splints, shoes, and weighted blankets.
Groups that foster connection between individuals with DCD would be helpful, as making friends is often a challenge, as explained by one of the participants:
We need more social groups for DCD kids. My son has a hard time making friends and interacting with his peers. I wish the therapist would give him some skills to make friends. (P5 USA)
Through an increased sense of connection, both the individual with DCD and the family unit can be supported to a greater extent. Support groups can be facilitated by those journeying with DCD themselves, healthcare professionals or educators, and social skills can be learnt in these groups.
Discussion
Participants identified three areas through which families journeying with DCD can be better supported. These were the provision of accurate information, greater awareness of DCD, and a sense of connection. Participants requested information that is easily accessible, includes both general information and practical ideas, is research-based, includes real-life stories, is relevant to the various members of the family, and is location-specific. Increasing awareness of DCD in society, healthcare and education is essential. Developing connections through both online and local support groups for all members of the family can mitigate the sense of isolation often experienced by families.
An understanding of DCD within healthcare could assist in alleviating the challenges experienced by families during the diagnostic process. Our study concurs with Missiuna et al. (2006) that parents experience the diagnostic process as one of ‘unravelling the mystery’ and negotiating a diagnostic ‘maze’. Since DCD is not a clearly visible disability, and manifests with subtle motor coordination difficulties, clumsiness and slowness of activities (Farmer et al., 2016), the diagnosis requires medical practitioners who are adept at identifying these nuances in patients. Although standardised diagnostic guidelines have been suggested for occupational therapists (Klein et al., 2023) in Canada, the diagnostic protocols are not streamlined in the general medical field to enable crucial early identification and intervention (Klein, Licari, et al., 2024). Parents in our study reported that generally the DCD diagnosis, frustratingly, was obtained two years after they started consulting with medical practitioners costing unnecessary time and funds. A similar result was found by Soriano et al. (2015), in their survey of UK parents who reported a confirmed diagnosis on average, ‘two and a half years after parents initially sought professional help’. Similarly, parents in a Canadian study reported long waitlists, delayed diagnostic services, and poor awareness among healthcare professionals (Klein, Licari, et al., 2024). Since our study included participants from eight countries, this long diagnostic process does need to be addressed globally.
Participants in this study indicated that awareness of DCD in healthcare and education would reduce the time that parents spend on advocating for their child with DCD. A similar finding was reported from a study of mothers in New Zealand, who continually advocated for their child’s needs to be understood and addressed (Hitchcock et al., 2020). Improved post-diagnostic support in these sectors has been advocated for in the UK (Soriano et al., 2015). Surveys of parents with a child diagnosed with DCD in the UK, report considerable stress levels for parents, as their work and family social life are impacted (Cleaton et al., 2019). In our study, parents wished they did not need to continually advocate for their child, and ask teachers to make adjustments, such a reducing the amount of written work given, sing soft pencils and jotter paper. Similarly parents in Stephenson and Chesson’s (2008) study reported that they spent time ‘fighting the system’ to access educational and classroom support. A large-scale study in Australia, similarly found that most children with DCD are not receiving adequate support to reach their academic potential (Reynolds et al., 2024).
Families in our study reported that facilitating a means of connecting with others experiencing a similar journey could assist with social participation and provide a space in which the individual with DCD can be accepted. For example, one mother in our study reported there is a support group in New Zealand south island, but no social support in the north island. Similar ‘lack of support’ and ‘feelings of isolation’ were reported by mothers in Stephenson and Chesson’s (2008) study.
Socially isolated children are at increased risk for internalised stress responses, such as depression and anxiety, which have been reported among individuals with DCD (Cairney et al., 2013). Participants in our study reported their children need help with emotional regulation, become anxious when large chunks of information require memorisation, and are frustrated when they struggle with motor skills, which others perceive as misbehaviours. Mental health challenges for parents are a risk associated with increased caregiver burdens (Klein, Cheung, et al., 2024). A parent in our study noted the ‘terrifying prospect’ that this condition meant for the future, as there was ‘no cure and no catch-up’. Psychologists can alleviate fears, and provide coping strategies to minimise stressful situations, when the child is frustrated and anxious. Parents can be assisted to set realistic expectations for their child, such as the serious difficulties associated with learning to drive a car.
Since these social and emotional areas are particularly challenging for families (Cleaton et al., 2019; Missiuna et al., 2006), psychological support should be incorporated into standards of care practices to alleviate stress and further mental health challenges (Missiuna et al., 2007).
An understanding of the influence that DCD may have on the diagnosed individual can be valuable in creating a positive journey for the family (O’Dea et al., 2021). This includes the provision of timely, practical information, which is relevant and accessible to all members of the family. A study by Jasmin et al. (2018) confirms that parents want information about the condition.
Supporting not only the individual diagnosed with DCD but also the family unit may result in further positive outcomes, as recommended in the South African Green Paper on supporting families with a child with any disability (Department of Social Development, 2011). The need for post-diagnostic support has been previously identified (Soriano et al., 2015) and the benefits of early support for individuals (Blank et al., 2019) with DCD through family-centred approaches guiding the physical motor and associated psychosocial impairments are clearly indicated (Klein, Cheung, et al., 2024).
Implications
Families frequently find themselves navigating the journey with DCD, which is riddled with obstacles, alone. To better support families, medical practitioners, psychologists, occupational therapists, and teachers can collaborate to increase societal awareness. Healthcare professionals are in the unique position to make accurate early diagnoses and reduce families’ frustrations with prolonged periods of searching for the cause of their child’s hidden difficulties. The provision of easily accessible, location specific, research-based, and practical information that is relevant to the various family members would be helpful. Finally, practitioners can facilitate connections via social media and local support groups, which will be valuable for each member of the family in reducing the sense of isolation often experienced by these families.
Limitations
The difficulties of recruiting suitable participants resulted in a small sample size with few people from each country participating in the study. Caution must be taken when generalising the findings across countries as service provisioning differs. Most participants were Caucasian females (mothers) who shared their experiences. Including more fathers and siblings would have provided a more nuanced understanding from each family member’s own perspective. The participants, especially those from South Africa, all made use of private healthcare and education. Thus, it may be difficult to generalise the findings to those who access public healthcare and education.
Recommendations for future research
Research on DCD has been conducted in Europe, America, Australia, and New Zealand. Specific diagnostic guidelines relating to the African context is an area in which further research can be conducted. Participants should include indigenous populations who may reflect an African collectivist (rather than Western) worldview, according to which communal activities and social participation is valued (Masolo, 2005). The lifelong impact of DCD is unclear and research into the difficulties of being a parent who lives with a DCD diagnosis is an under-researched area. The experiences of growing up with a sibling with DCD from the perspective of the sibling could also be studied.
Conclusion
Global healthcare practitioners and educators appear to be woefully unaware of the symptoms children with DCD exhibit. We recommend awareness training on the invisible, subtle presentation of DCD to accelerate the current protracted diagnostic process. A timely, accurate diagnosis would alleviate much family stress and anxiety, allowing healthcare professionals to provide early psychosocial support interventions for the child and their family. The agency of parents advocating for both healthcare and education interventions will continue as families navigate the daily struggles that accompany ‘invisible’ motor coordination deficits.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: N O’Kelly received a Merit bursary from the University of Johannesburg to conduct the research. Publication fees were supported by the Department of Educational Psychology, Centre for Neurodiversity, through a grant from the DHET and European Union.