
Abstract
Parenting a child with autism spectrum disorder (ASD) is known to be complex and challenging and likely to be exacerbated under conditions of stress and uncertainty. We aimed to explore how parents experienced parenting their child with ASD during the initial COVID-19 lockdown in 2020. We also aimed to identify the coping strategies and sources of support available to them during this time. Using an exploratory qualitative design within an interpretivist paradigm, we interviewed 23 parents of children with ASD between the ages of 6 and 12 years. Parents were recruited from an online support group for ASD in South Africa. Interviews were semi-structured and transcribed verbatim for thematic analysis, using ATLAS.ti. We identified five themes: (1) The experience of communicating lockdown rules and disease containment measures to children, (2) Consequences of disruption to routine, (3) Parenting and interpersonal relationships in conditions of confinement, (4) Help-seeking and sources of support, and (5) Finding ways to cope amid a crisis. The findings demonstrate that the initial COVID-19 lockdown placed parents of children with ASD under considerable stress. Disrupted routines and interrupted access to financial, psychological, social, and educational support during the initial lockdown period exacerbated parenting experiences. This study highlights the importance of providing parents of children with ASD strategies to communicate significant change and various forms of support to navigate the negative effects of routine disruptions during conditions of uncertainty and crisis.
In response to the rapid spread of COVID-19 globally, South Africa, like many other countries, declared a national state of disaster. This was done on 15 March 2020 in terms of Section 3 of the Disaster Management Act 57 of 2002 (Department of Co-operative Governance and Traditional Affairs, 2020). It entailed strict lockdown regulations, which meant the closure of businesses and schools, and shifts to remote working. Furthermore, individuals were asked to follow specific disease containment measures (DCMs), such as mask-wearing, hand sanitising, social distancing, quarantine, and home confinement (‘lockdown’). These DCMs and lockdown orders meant a disruption to the daily routine for all families, which made parenting more difficult, particularly among parents with children with autism spectrum disorder (ASD) (Alhuzimi, 2021; Gruszka et al., 2023; Kaba et al., 2023). Indeed, a large U.S.-based study conducted during the height of the pandemic showed that parents with a child with ASD (n = 3556) were significantly more likely to report psychological distress, defined in the study as symptoms of anxiety, depression, loneliness, and hyperarousal, than parents in general (n = 5506) (Kalb et al., 2021). However, it should be noted that even before the pandemic, it was well-established that parents of children with ASD were more likely to experience poorer quality of life (QoL) and higher levels of stress due to their child’s behavioural symptoms compared to parents of neurotypical children (Alhazmi et al., 2018; Benson & Karlof, 2009; Cohrs & Leslie, 2017; Crowell et al., 2019; Keenan et al., 2016; Lai et al., 2015; Schlebusch et al., 2017). For example, in the Western Cape, South Africa, Alhazmi et al. (2018) demonstrated that QoL among parents raising a child with ASD was significantly lower across all domains of functioning (physical, psychological, social, and environmental health) compared to those raising a neurotypical child.
ASD is a neurodevelopmental disorder that is evident from a young age and is estimated to occur in 1 in 100 children globally (World Health Organization, 2023). More recent estimates suggest that 1 in 36 children aged 8 have ASD (Maenner et al., 2023). ASD is also highly co-morbid with attention-deficit hyperactivity disorder (ADHD) in children, with estimates ranging between 37% and 78% (Salazar et al., 2015; Stevens et al., 2016). The prevalence of ASD in South Africa has not been established (Van Biljon et al., 2015).
ASD has two key features according to the American Psychological Association (APA), namely (1) deficits in social communication and social interaction across various settings and (2) patterns of behaviour, interests, or activities that are repetitive and restricted (American Psychiatric Association, 2022). These key features, given the spectrum nature of the disorder, can range in severity (between children with ASD) from mild, to moderate, to severe. We acknowledge, however, that these criteria are under much scrutiny in the research community (Fletcher-Watson, 2024). Furthermore, we also acknowledge that these criteria may be limited and that the broad umbrella term, ESSENCE (early symptomatic syndromes eliciting neurodevelopmental clinical examinations), perhaps better captures the broad range of symptoms (which can be identified early) and co-morbidities associated with many neurodevelopmental disorders, including ASD (Fernell & Gillberg, 2023).
Given the key features of the disorder, as described by the APA, compensation strategies such as clear communication about daily activities and strict adherence to daily routines, diets, and sleep schedules can help manage those emotional and behavioural problems in some individuals with ASD that arise from uncertainty and stressful situations. Even slight disruptions to these strategies are likely to cause marked distress among some children with ASD and will affect parenting (Alhuzimi, 2021; Lai et al., 2015).
In keeping with transactional theories, for example, Lazarus and Folkman’s transactional model of stress and coping (Lazarus & Folkman, 1984) and the bidirectional view of parenting stress (Benson, 2023; Rodriguez et al., 2019; Sameroff, 2009), both parent-driven and child-driven effects influence parenting stress. Indeed, parenting behaviour plays an important role in the development and everyday functioning of children living with ASD. Similarly, children’s symptoms and behaviours too affect parental stress and mental health (Crowell et al., 2019).
Studies show that the severity of children’s ASD symptoms worsened during the initial lockdown period (Adams et al., 2022; Colizzi et al., 2020; Cooke et al., 2020; Fontanesi et al., 2020; Narzisi, 2020; Pellicano & Stears, 2020). For example, in a study conducted by Narzisi (2020) in Italy, children with ASD experienced an increase in negative behaviours such as destruction, aggression, hyperactivity, emotional dysregulation, a decrease in social motivation, as well as an increase in ritualised behaviours. Moreover, children expressed feelings of anger, anxiety, sadness, frustration, and loneliness (Narzisi, 2020). In a South African study, 21 family members reported that their children struggled with changes to their routine, had an increase in emotional dysregulation, and lost previously acquired skills due to difficulties in accessing services during the lockdown (Adams et al., 2022).
Studies on parenting a child with ASD during COVID-19, particularly in high-income countries, have highlighted the diversity of experiences, both negative and positive (Alhuzimi, 2021; Chan & Fung, 2022; Colizzi et al., 2020; Lee et al., 2021; Tokatly Latzer et al., 2021). For example, in Tel-Aviv, 31 parents of 25 children with ASD (ages 4–6 years), recruited via the Child Development Institute database, described their negative and positive experiences of lockdown through anonymous telephone interviews. Some parents reported having to take the role of being both full-time educators and caregivers to their children, and they seldom had support (whether instrumental or financial) to juggle both of these roles. Other parents reported that their child with ASD not only overcame the challenges of the ever-changing conditions but even seemed to benefit from them (Tokatly Latzer et al., 2021).
Despite the increase in challenging experiences, parents reported varying access to professional, educational, financial, governmental, and social support during this time, which affected their ability and capacity to parent and cope (Adams et al., 2022; Tokatly Latzer et al., 2021). Studies report that parents faced considerable stress due to the lack of or limited access to special education services, having to support their children’s developmental and learning needs, the change in routine to family and work life, changes in food, sleep-related, and behavioural issues among their children with ASD, and limited physical space for children to expend their energy (Alhuzimi, 2021; Bruni et al., 2022; Colizzi et al., 2020; Tokatly Latzer et al., 2021). In the absence of support, and in keeping with Lazarus and Folkman’s transactional model of stress and coping (Lazarus & Folkman, 1984), parents seemed to engage in maladaptive coping (such as drinking alcohol and overeating) and avoidant coping strategies (such as emotional suppression) in response to many of these difficulties (Fatehi et al., 2023; Yılmaz et al., 2021). However, parents also used adaptive coping strategies such as reframing the situation in a positive way and problem-solving (Adams et al., 2022; Tokatly Latzer et al., 2021; Yılmaz et al., 2021).
Aims of the study
Taken together, the literature shows that parenting a child with ASD (especially during the initial COVID-19 lockdown) was complex and challenging not only due to a myriad of child and parent-related factors but also due to broader contextual factors (such as restrictions to public spaces and loss of employment) and limited access to support (Adams et al., 2022; Tokatly Latzer et al., 2021; Yılmaz et al., 2021). To our knowledge, only a handful of South African studies have documented COVID-19 experiences among children with ASD and their parents (see Adams et al., 2022). There is generally limited research on ASD among South African children with ASD and their parents. The available studies have mostly focused on children with ASD’s experiences of the pandemic from the perspectives of family members, whereas ours focused on parenting experiences predominantly with the mention of child experiences. In this study, using data collected in 2021, we sought to qualitatively explore how South African parents with a child diagnosed with ASD experienced, coped with, and sought support during the initial COVID-19 lockdown period in South Africa.
Methods
Study design
We undertook an exploratory qualitative research study, broadly nestled within the interpretivist/constructivist paradigm, to explore parents’ subjective experiences (Willig, 2013).
Setting
Our study took place online among South African parents with children with ASD who were part of a social media support group for parents. We approached the administrator of a South African autism support group on Facebook and obtained permission to make a post about the study on the support group page.
Research participants and sampling strategy
Our participants were 23 parents of children with ASD. We used purposive sampling (Creswell, 2013) to recruit eligible parent participants using an online approach. Participants had to be (1) members of the ASD social media support group, (2) parents (biological parents or a caregiver living in the same house as the child) of children with a confirmed diagnosis of ASD, and (3) parents of children between the ages 6 and 12 years. We chose parents of children between 6 and 12 years as these children fall within the developmental period of middle childhood and are typically in primary school.
Data collection methods
Interested participants who saw the study details on the online support group were able to contact M.K. directly via e-mail if they were interested in taking part. Participants were then sent an informational leaflet and consent form detailing the particulars of the study. Participants who were interested in taking part in the interview were then contacted to organise a convenient date and time for the interview to take place. Interviews took place via WhatsApp calls, or via online calls, using Zoom, Skype, or Microsoft Teams. Each interview lasted approximately 45 to 60 min. We made use of semi-structured interviews to collect data. Interviews were conducted from 7 to 26 June 2021. Our interview schedule was developed to address our research question and constructed based on previous literature related to the topic. We used probes such as ‘Can you tell me more?’ or ‘Can you provide me with an example?’ to elicit richer responses. The audio recordings of the interviews were transcribed verbatim for analysis. We used the notion of information power to guide data collection in our study (Malterud et al., 2016).
Data analysis
We analysed the data using reflexive thematic analysis (Braun & Clarke, 2021) and used ATLAS.ti version 9 software to code the data inductively. We used the six steps prescribed by Braun and Clarke (2021) to carry out the analysis in relation to the research question. These six steps were: (1) familiarising ourselves with the data through repeated reading; (2) generating initial codes guided by the interview questions and overall research question of the study; (3) identifying themes from the codes developed; (4) reviewing of themes to ensure consistency and coherence among the codes included; (5) defining and naming themes to reflect an overarching idea; and (6) producing the final report. The final report took the form of M.K.’s master’s thesis. B.C. was her supervisor. Both M.K. and B.C. read the transcripts of the interviews. The data were coded in full by M.K. During supervision meetings, M.K. and B.C. met to discuss the accuracy and the relevance of the codes and to identify suitable themes to show patterned responses to the data. To establish rigour and trustworthiness in this study, we used member checks during the interviews by paraphrasing questions to alleviate any ambiguity in understanding participants’ responses (Guba & Lincoln, 1985).
Ethics
The study was approved by the Stellenbosch University Social Behavioural and Education Research (SBER) committee (study number: 22174). All participants provided written informed consent prior to the start of the recording of the interviews. Participants received an airtime voucher from the supplier of their choice to the value of R50.00 (approximately USD 3.00) as a token of appreciation for their time and willingness to participate in the research study.
Findings
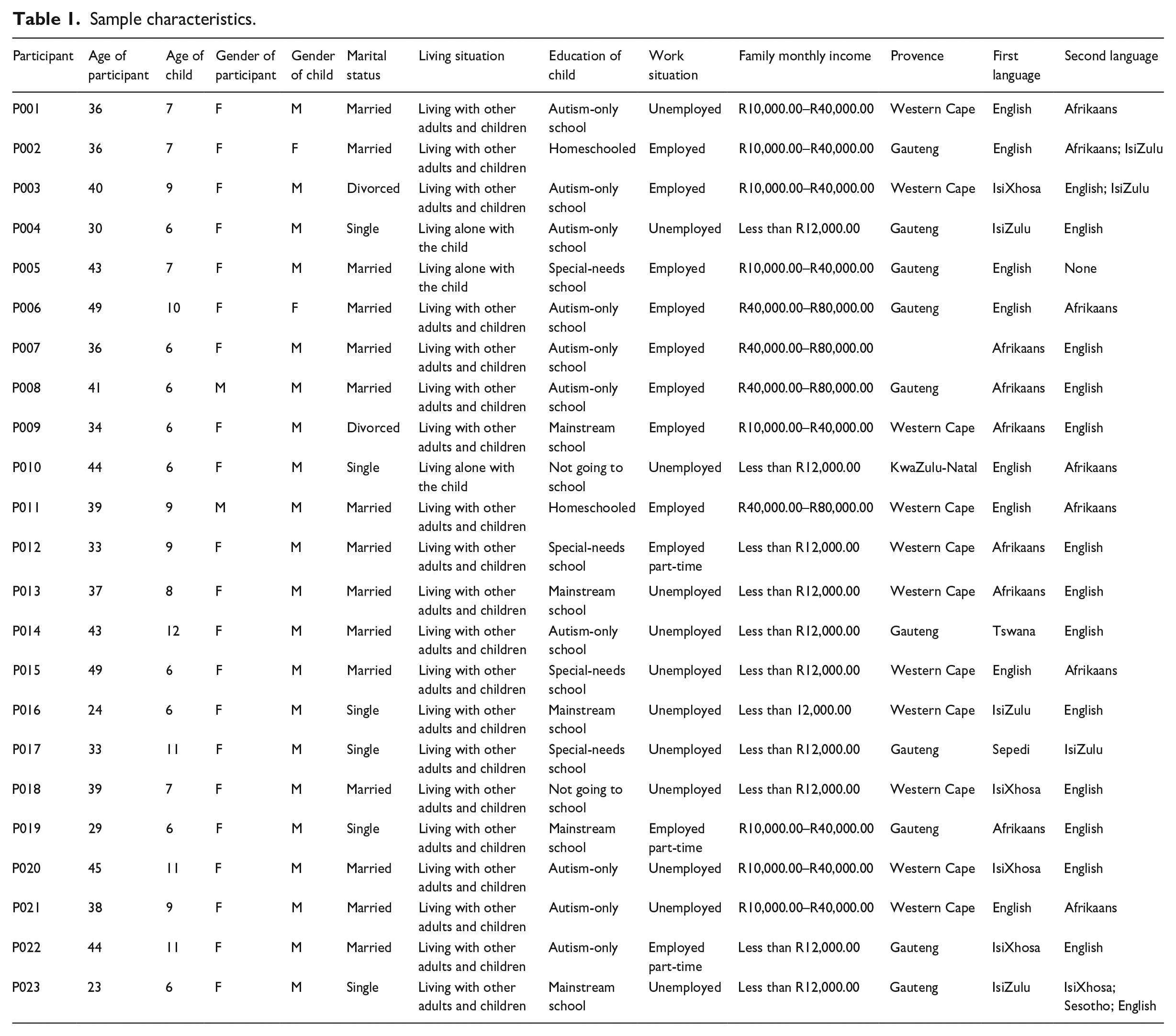
Table 1 shows the demographic characteristics of the parent participants. As can be seen from Table 1, parents’ ages ranged from 23 to 49 years, mean = 37.6, and standard deviation (SD) = 6.9. The majority were identified as female (87%). The ages of the children ranged from 6 to 12 years (mean = 7.8; SD = 2.0). Fifteen parents (65%) reported being married, six (26%) reported being single, and two (9%) reported being divorced.
Sample characteristics.
Findings from the thematic analysis
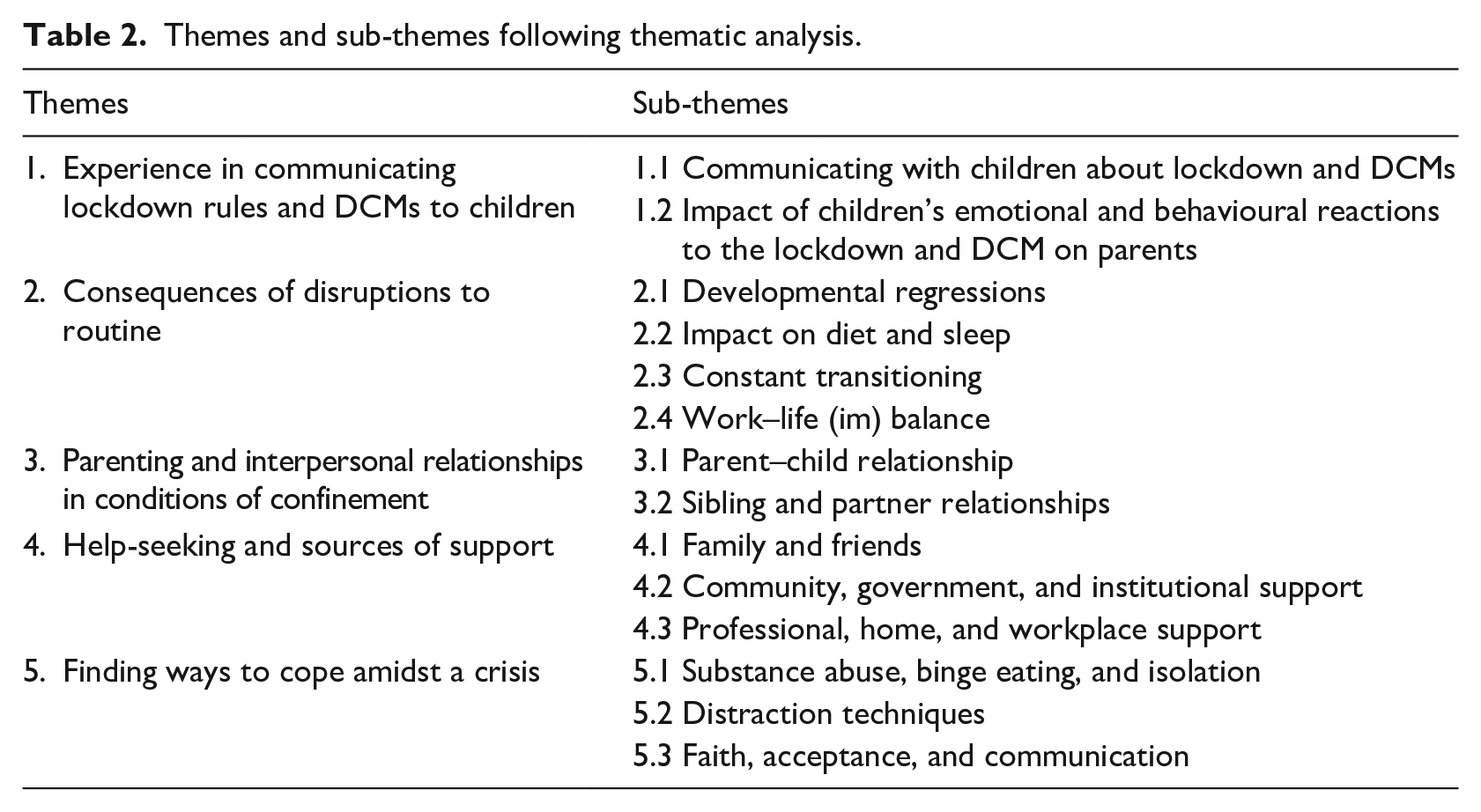
As shown in Table 2, we identified five over-arching themes and 14 sub-themes that provided insight into the parenting experiences of parents with a child with ASD during the lockdown period in South Africa. Each theme is described below with illustrative, anonymised quotes.
Themes and sub-themes following thematic analysis.
Experience in communicating lockdown rules and DCMs to children
This theme captures parents’ experiences of communicating the lockdown rules and regulations to their children, and their children’s reactions to this.
Communicating with children about lockdown and DCMs
Parents reported that in the early days of lockdown they experienced difficulty in communicating to their children what COVID-19 was and why the lockdown and the DCMs were necessary. This left the parents feeling helpless and unable to reassure their children that everything would be OK. As one parent explained,
It was horrible, because I wanted to help and make him understand that everything will be okay even if something is different. I felt helpless because he couldn’t understand and didn’t feel safe. (P009)
One parent seemed to have an easier time helping their child understand what was happening and reported,
I explained to him the virus, he started watching the news and understood that we had to stay home. He accepted it and got used to it. (P003)
In terms of the DCMs, parents reported varying experiences with communicating with their children about mask-wearing, social distancing, and hand sanitising. One parent stated,
He can’t do social distancing so I can’t take him to the shops. People do not understand that he has ASD. I ask my neighbours to help me with groceries shopping. (P010)
The impact of children’s emotional and behavioural reactions to the lockdown and DCMs on parents
Parents reported that the inability to provide their children with explanations about the lockdown that were comprehensible to them meant children experienced serious emotional and behavioural changes (e.g., excessive crying and meltdowns), to the point where some children would attempt to run away or hurt themselves out of sheer frustration. These instances were distressing for parents and required more time for supervision, which was not always possible alongside work and other family and household responsibilities. One parent said,
His behaviour changed completely during the lockdown, he started crying often. When I ask him why he is crying, he says that he doesn’t know. When he had a tantrum, it wasn’t easy to calm him down and I ended up crying myself because I didn’t know what to do. (P009)
For parents with children with co-morbidities like ADHD and Down Syndrome, containing their children’s emotional and behavioural responses seemed to be even more challenging. As one parent reported,
The hardest part is that he also had ADHD with ASD so during the lockdown he would constantly jump and run everywhere in the house shouting and breaking things. (P023)
Consequences of disruptions to routine
This theme captures parents’ account of the consequences of the disruptions to the routine their children experienced. These consequences were developmental regressions, effects on diet and sleep, difficulties with constant transitioning between lockdown levels, and the impact on work.
Developmental regressions
School closures and restrictions on public play areas were major disruptions to routine. Consequently, the lack of educational and play opportunities at school meant that parents experienced their children as regressing developmentally, which concerned them deeply. One parent said,
Not being at school is a negative impact on the learning side. It sets him back. He also had a very bad toilet training regression. COVID-19 impacted my child very negatively because it set back my child’s development. (P009)
Impact on diet and sleep
The lockdown had an effect on children’s diet and sleep routines, which was difficult and stressful for parents to manage. With respect to diet, parents struggled with access to specific foods their children wanted. One parent reported,
He only eats one specific type of yogurt, and if I didn’t buy that specific type of yogurt, he would get a meltdown. (P019)
With respect to sleep, some parents resorted to medications, which seemed to help. One parent said,
Since the lockdown I give him medications to sleep, now he sleeps very nicely at night. (P018)
Constant transitioning
Parents reported that the constant transitioning from one lockdown level to the next was especially difficult to manage and negatively affected their children.
One parent reported,
The transition was horrific. What was worse was that the school would only open three days a week, Monday, Wednesday, and Friday, and that broke his brain because he could not understand that. (P009)
Parents reported that while some children experienced difficulties with the transition from school to home and from one lockdown level to the next, others were better able to adjust to the situation. One parent reported that her son understood the transitions well, which meant he could tolerate the disruptions to routine:
The transition was a bit difficult, but he is very intelligent, he understood and adapted. My son’s autism is very mild, and his IQ level is very high. (P013)
Work–life (im)balance
Working from home was a challenge for parents, as they had to juggle work commitments alongside parenting and schooling responsibilities. One parent whose child has ADHD said,
It was very stressful and there was a lot of hard work. I had to be mom, teacher, cleaner, and a sales manager as I am. I still had to do my own work as well. (P007)
Parents explained that to have time to themselves, they resorted to hiding away, bringing their child into online meetings, working late nights, or taking their full annual leave. One parent explained,
It was really difficult because sometimes when I had an important meeting, I had to go hide in the garage so that he couldn’t get to me. (P007)
Parenting and interpersonal relationships in conditions of confinement
This theme captures the impact of the initial lockdown on relationships within the home. These included the parent–child, sibling, and partner relationships.
Parent–child relationship
While parents mostly reported a good relationship with their children before the pandemic, this relationship often became strained and difficult during lockdown – mostly due to a lack of personal space and minimal time apart from each other. One parent stated,
We used to see each other like five to six hours per day, and now we see each other like 16 hours a day. There is more tension and more anxiety from both sides. We need space from each other. (P011)
The strain on the relationship was emotionally distressing at times. One parent stated,
Covid made my relationship with my daughter much worse. The parent that she related more with was not here, so I was at home with her often. She would get frustrated and violent with me, and I didn’t deal with it in the best possible way. I would also get frustrated, and tensed, I would cry. She is partially verbal, but we got our fights, it got rough, we were frustrated with each other. (P006)
While some parents reported difficult relationships with their children, others had more positive experiences. One parent said,
The lockdown actually helped me a lot to understand him and allowed him to stop taking the medications. I started communicating more with him and understand him better. He is non-verbal, I interacted with him more than before. (P015)
Sibling and partner relationships
Parents reported both positive and negative effects on sibling and partner relationships during the lockdown. On the positive side, parents reported that some sibling relationships improved. One parent said,
His relationship with his brothers improved during the lockdown because they spent more time together as they were locked in the house 24/7. They played a lot more with him during the lockdown, it improved his social skills. (P007)
Parents reported that sibling fights affected them emotionally as it was difficult to manage. One parent described it as follows:
He fought and hurt his baby brother every day during the lockdown because we were confined. These fights were difficult to handle. It made me not want to be a mum anymore because I was forced to stay with my children 24/7. (P021)
Parents also experienced challenging relationships with their partners as they spent more time together and did not have the space they used to have before the lockdown. One parent said,
My relationship with my wife was affected by the Covid, it was a strained relationship. We argued more because we were in each other’s face. You are making me realise that I definitely need a counselling session. I’m about to cry, it is very emotional talking about it because you realise how real it is. (P011)
Others shared positive experiences. For example, one parent said,
It was nice spending more time with my partner. We supported each other and communicated well. We really enjoyed the times that we had together. (P006)
Help-seeking and sources of support
This theme captures the support parents required and had available to them during this time.
Family and friends
Parents reported a range of people on whom they relied for support, including their own parents (child’s grandparents), extended family, siblings of the child with ASD, and their friends. One parent reported,
His brother was very helpful during the lockdown as he didn’t go to school, he would help me and look after him and play with him while I was busy, but not all the time because he still had homework to do. (P007)
For most parents, however, partners in particular were identified as the main sources of support. One parent said,
It was nice spending more time with my partner. We supported each other and communicated well. We really enjoyed the times that we had together. (P006)
Community, government, and institutional support
Parents found support from their community (neighbours, church, and online on the ASD Facebook group) especially helpful during the COVID-19 pandemic. However, parents mentioned that they experienced stigma and a lack of understanding from their neighbours and community during the lockdown. A parent said,
They looked at me funny, especially during the lockdown. He screams at the top of his lungs; other people think I’m hitting him, they don’t understand. (P010)
Several parents (n = 8) received a grant from the government, which helped them financially before and especially during the lockdown. For some parents, the grant was their only source of income during the lockdown, which was not sufficient. One parent said,
I received a monthly grant from the government, it’s R1 200.00 [approximately USD 70.00], but it’s not enough, it’s not even enough to carry his transport fees to the school where he is situated. (P012)
Parents were grateful that child care institutions remained open during the lockdown. These institutions were major sources of support, especially for parents who were at the frontline of the pandemic. One parent explained,
I put him in a full-time institution during the lockdown, I don’t know what I would have done if the government had closed that. (P005)
Professional, home, and workplace support
Parents did not only express the need for mental health intervention and support for their child (which some could access online), but also the need for therapeutic, emotional, and psychoeducational support for themselves (see quote from Participant 11, in the sub-theme on sibling and partner relationships). Another parent explained,
I would have liked mental health care professionals to chat to specifically about my situation at work. (P005)
Furthermore, while some parents benefitted from work support (e.g., working hours and remote working flexibility), which relieved a great amount of parenting stress and eased the difficulties of the pandemic, others lacked this support, which increased their parenting stress. One parent stated,
Members with children who have issues should be given concessions, but the Chief of Defence didn’t give any guidelines as what could have been done about it. She also told me that if I don’t come to work, I will be fired. (P005)
Finding ways to cope amid a crisis
This theme captures the various coping strategies parents used during this time.
Substance abuse, overeating, and isolating
Parents explained that to cope with their mental health challenges and parenting stressors, they turned to substances such as alcohol and cigarettes. Parents explained that before COVID-19, they used to cope by doing outdoor activities, but they now relied on substances to relieve their stress.
One parent stated,
Before the lockdown I would go for a run to relieve my stress but I could not do that during the lockdown so I would drink alcohol every night to relax because I did not know what else to do. It was extremely hard during the lockdown when I could not get alcohol, not that I can make my own. (P011)
While some parents turned to alcohol and cigarettes during the lockdown, others started overeating or/and isolating to relieve their stress and anxiety. One parent explained,
My coping strategy during the pandemic is eating. I eat excessively when I am stressed and that helps. (P009)
Distraction techniques
To deal with their children’s emotional and behavioural difficulties, parents used a range of creative distraction techniques like practical art activities and allowing their children to use digital devices and watch television. One parent said,
I got him colourful things like clothes because I could not get him toys so I would give him different colours of garments. He would then pack them in a row forming different shapes in the yard, it would keep him distracted and calm. (P015)
Faith, acceptance, and communication as coping strategies
Faith was an important coping mechanism, especially during the lockdown, to tolerate children’s behavioural and emotional difficulties and ease other stressors. One parent said,
I am Christian so I would find myself praying more during the pandemic and reading God’s words. I felt lost, neglected and abandoned sometimes and I had all these responsibilities. My husband and I coped by praying because it calmed us and gave us hope that things are going to get better. (P015)
Another parent said,
I just keep on going and praying, that’s the only thing I can do. I try to keep myself as calm as possible because sometimes I would just break down and cry when it becomes frustrating because I don’t know who to turn to to get help or there is no manual for someone with autism as each day is a different day. All I can do is pray and try my best. (P12)
For others, acceptance (which meant tolerance of the child’s uniqueness) and communication were important. One parent said,
It is not easy, it is very difficult, it is terrible and exhausting. I never really accepted the diagnosis, I’m still in denial. I’m going through life, but I have not accepted that he has ASD. (P003)
Discussion
We sought to explore how parents with a child with ASD experienced parenting in the context of COVID-19 in South Africa. Our findings demonstrate that in keeping with the broader literature and transactional theories (Sameroff, 2009), both parent and child factors influenced parenting and parent mental health during this time. We discuss this further in what follows. Our findings may relate to the context of the COVID-19 pandemic specifically, but have wider applicability in the context of future crises and also the demanding and challenging nature of parenting children with neurodevelopmental disorders.
Our study demonstrated that parents felt stressed, frustrated, and helpless in their roles during this time and had limited support. This adds to the broader literature that indicates that even before the pandemic, parents felt ineffectual in responding to the needs of their children with ASD (Crowell et al., 2019). These feelings of ineffectiveness, in turn, affected their own mental health. These findings are important in the South African context, as access to support services and professional interventions remains lacking (Nkonyane et al., 2021; Schlebusch et al., 2017). As such, this study as well as others that have focused on parenting a child with ASD during the COVID-19 period (Chan & Fung, 2022; Lee et al., 2021) highlight the importance of providing parents with tools and strategies (e.g., visual aids to support visual explanations of disease, illness, and emergency containment strategies) to communicate and respond to their children’s needs. These in turn may support parents’ own mental health and support them in managing disruptions to routine and relationships, which can happen even in the absence of a pandemic like COVID-19. Indeed, while the lockdown associated with COVID-19 presented a very context, time, and situation-specific crisis and period of uncertainty that had several parent and child-related consequences, many neurodivergent families face ongoing and difficult situations that affect parenting every day. As such, these findings have much relevance beyond COVID-19 – especially in that they add to the emerging South African literature on autism parenting (Heyworth et al., 2022). Furthermore, it may also be worthwhile to consider the genetic origin of ASD (Folstein & Rutter, 1977) and to ponder whether parents in the study may also have been dealing with their own undiagnosed neurodivergence in addition to having to manage their children’s ASD (Heyworth et al., 2022), which may have exacerbated their experiences. However, we do not know this for sure and did not ask our participants if they had been diagnosed with ASD.
Understanding how parents respond to and cope with change (especially with changes in their children) during conditions of crisis is important, as an inability to respond and cope effectively may affect parent–child relationships and family well-being. According to Lazarus and Folkman’s transactional model of stress and coping (Lazarus & Folkman, 1984b), an individual’s capacity to cope with and adjust to situations appraised as stressful is the result of transactions between person and environment. Primary appraisals can be benign or stressful. Situations appraised as benign require no action, whereas those that are stressful may be deemed challenging or threatening and require coping strategies (secondary appraisals), which can be adaptive or maladaptive, and these coping strategies are continually re-appraised. Our findings showed that the lockdown challenges presented parents with situations appraised as stressful and that coping strategies were mostly maladaptive (turning to substance use and unhealthy eating patterns) as opposed to adaptive. Consequently, these changes disrupt parental mental health and influence their ability to respond sensitively to their children’s, and other family members’ needs. The effect on interpersonal relationships is important, as close family relationships offer an important source of support during difficult and uncertain times. Furthermore, positive parent–child relationships are important for parental mental health and for emotional, cognitive, and social development in children. Adaptive coping strategies were faith, acceptance, communication, and home activities. Similarly to our findings, the literature demonstrated that parents who were able to cope reported more positive experiences (Narzisi, 2020; Tokatly Latzer et al., 2021).
Our findings showed that parents struggled to communicate rules and restrictions, and the uncertainty attached to them. The inability to communicate in ways that were comprehensible to their children left parents feeling worried, frustrated, and helpless. Being able to communicate change clearly to a child, but especially children with neurodevelopmental disorders like ASD, is necessary to help establish (or re-establish) routine (which is important for some, but not necessarily all children with ASD) and manage emotional and behavioural outbursts like meltdowns, which add to parental experiences of distress (Alhuzimi, 2021). The inability to do so effectively meant that, as was seen in our study, parents had to become more vigilant and spend more time supervising their children as some started to hurt themselves and run away from home out of sheer frustration. This constant supervision alongside the many emotional and behavioural difficulties meant parents had little time for their other children and their partners, and struggled to stay focused on their work, all of which contributed to negative and stressful experiences of parenting (Lee et al., 2021; Narzisi, 2020; Tokatly Latzer et al., 2021) and the use of maladaptive coping strategies like substance use and overeating (Fatehi et al., 2023). Previous research has emphasised the negative impact on parents when there are no opportunities for rest and respite, and this adds considerably to strain in not only parent–child relationships but also other significant relationships in the household (Nkonyane et al., 2021).
The importance of structure and routine for some children diagnosed with ASD is well described in the literature. In the absence of structure and routine, some children with ASD may experience emotional dysregulation and behavioural difficulties, which affect parenting (Alhuzimi, 2021; Colizzi et al., 2020; Manning et al., 2021; Tokatly Latzer et al., 2021). In our study and others, it is clear that lockdown severely disrupted family routine, which affected children’s diets and sleep routines, and the lack of educational and play opportunities meant that parents experienced their children as regressing developmentally (Fatehi et al., 2023; Tokatly Latzer et al., 2021). In terms of sleep, it is not surprising that parents reported their children struggling with this as sleep disorders are common in children with ASD (Moore et al., 2017; Sivertsen et al., 2012) and seem to have become more pronounced as a result of the COVID-19 pandemic (Gios et al., 2024; Sharma et al., 2021). While some parents tried to reconstruct a sense of consistency for their children, this remained challenging given the many other responsibilities (such as home-schooling) parents had to take over during this time, as well as the constant transitioning between alert levels. Some of the challenges parents experience may also be attributed to autistic inertia, where individuals with ASD may struggle with initiating, stopping, or changing tasks when routines are disrupted (Buckle et al., 2021). Limited access to play areas during the lockdown meant that children were more sedentary for longer periods, which likely also affected their ability to start or engage in tasks and activities. Constant transitioning between COVID-19 alert levels may be particularly hard for children with ASD, who may struggle with context blindness (i.e., cognitive inflexibility and limitations in seeing the broader context of a situation), which makes it difficult to spontaneously and flexibly accommodate unexpected change (Vermeulen, 2015).
Although many parents explained receiving support from friends, family, siblings, the professional community (i.e., therapists), colleagues at work, and through online support groups (Fatehi et al., 2023; Lee et al., 2021; Tokatly Latzer et al., 2021), some experienced stigma and a lack of understanding from close networks like family and friends. This experience of stigma meant those parents had fewer support resources available to them, even access to health care professionals, which is likely to have added to more negative experiences of parenting during this time (Nkonyane et al., 2021). Furthermore, in instances where sources of support were also sources of conflict (i.e., disrupted sibling and partner relationships), pandemic experiences seemed to be worse. Although a recent study from the United States suggests that mental health and marital functioning did not necessarily improve or worsen during the initial lockdown (Ekas et al., 2024), interventions aimed at addressing uncertainty in everyday situations have shown that parents prefer group-based sessions precisely because they seek support from community and others (Rodgers et al., 2023). As such, future research is necessary to improve awareness and understanding of the emotional and behavioural aspects of ASD in children to minimise stigma experiences among families with children with ASD. Future research is also needed to improve access to professional care and support for children with ASD and their families in South Africa.
Limitations
In the wider South African context, the sample of participants was not representative of all parents of children with ASD in the country. Although generalisability is not an aim of qualitative research, it is prudent to acknowledge the importance of diversity in settings, which were multicultural and multilingual. Given that our participants were recruited via online social media platforms, future studies may broaden recruitment strategies to reach a wider population. Future research might also aim to specifically focus on single-parent and father perspectives and consider recruitment of participants from various socioeconomic backgrounds. Future research might also capture data on children’s severity levels to add more depth and insight into the findings.
Conclusion
The COVID-19 pandemic significantly disrupted life for all. However, even in the absence of a pandemic, parents with children with ASD face significant and varied parenting challenges that can lead to maladaptive coping strategies, affecting their emotional and mental well-being and capacity to parent. Against this backdrop, our findings highlight that these experiences are exacerbated in times of significant life and global events and underscore the urgency with which to provide appropriate and accessible intervention and support to parents with children with ASD, especially in the South African context where both research and professional care and support for ASD are limited. Interventions that are psychoeducational in nature and provide parents with children with ASD with tailored strategies for communicating during stressful times and addressing barriers to help-seeking, such as stigma, are needed.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.