
Abstract
There are inconsistent reports on the impact of the COVID-19 pandemic and its associated social restrictions on mental health, with initial suggestions of an increased prevalence of mental disorders in South Africa. However, the longitudinal trajectories of mental health responses across the COVID-19 pandemic are not clear. The primary aim of this study was to describe the trajectories of self-reported common mental disorders, as determined by repeat administration of clinical screening tools across five consecutive years (from 2019 to 2023). A secondary aim was to consider associations with demographic factors such as gender and age. Point prevalence estimates were obtained from a South African occupational mental health surveillance programme in a stable workplace population. Trajectories of common mental disorders across COVID-19 were determined using the Patient Health Questionnaire-9 and Generalised Anxiety Disorder-7 to identify Major Depressive Disorder and Generalised Anxiety Disorder, respectively. Prevalence estimates for depression and anxiety disorders initially remained stable before increasing towards mid-2021 and returning to pre-COVID-19 estimates by end-2022. Suicidal ideation decreased early into the pandemic but returned to pre-COVID-19 levels by 2021. The study suggests that on a practical level, readily available access to mental health care remains an important mechanism to protect mental health during and after major societal disruptor events. This can further be supported through regular monitoring and through providing high-intensity early intervention for at least 18 to 24 months following such events.
Introduction
COVID-19 represented a major disruption of South African society, alongside reports of increased mental health difficulties. This study examined the trajectories of mental health across the COVID-19 experience in an attempt to provide insights that would support mental health and psychological adaptation during future major disruptor events.
Mental health refers to personal adjustment to life’s demands. Various respected definitions (American Psychological Association, 2018; World Health Organization, 2022) also make reference to relationships, community, and relative freedom from psychopathology. This study focussed on common mental disorders (CMD) – specifically mood and anxiety disorders – representing problematic psychological adaptation that would require clinical attention.
COVID-19 and mental health
The COVID-19 pandemic was associated with severe disruptions in global society, leading to early warnings of an impending mental health pandemic globally (The Lancet Public Health, 2020; Pfefferbaum & North, 2020) and, more specifically, in sub-Saharan Africa (Semo & Frissa, 2020). However, initial reports of the impact of the pandemic on mental health offered inconsistent results. While some studies reported stable rates of CMD during the early pandemic compared to pre-pandemic levels (Knudsen et al., 2021; Van der Velden et al., 2020), others (Daly et al., 2020; Ettman et al., 2020; Pierce et al., 2020; Winkler et al., 2020) reported often dramatic increases. Yet other studies reported that negative affect decreased during lockdown, suggesting a possible differential effect of the pandemic on different population groups (Foa et al., 2020; Fountoulakis et al., 2022; Recchi et al., 2020).
Three risk factors for CMD during COVID-19 were consistently reported (cf. Fountoulakis et al., 2022, for review): being female, being younger, or having a history of previous mental health difficulties. In addition, retrenchment and unemployment were also associated with increased risk for mental distress (Knudsen et al., 2021; Kwong et al., 2022).
Some of the discrepancies in the above reports could be attributed to factors such as timing of data collection, sampling procedures, and measuring tool biases. Levels of mental health appeared to fluctuate depending on whether data were collected during or between COVID-19 waves and lockdown phases. Different levels of depression and anxiety were observed at different time periods during 2020 to 2021, broadly associated with intensifying and easing of lockdown restrictions (Kwong et al., 2022; Van Wijk, 2023), with depressive symptoms significantly increasing during periods of social restrictions while anxiety symptoms did not (Witteveen et al., 2023). Rates of anxiety, depression, and suicidality were also associated with the intensity or severity of individual lockdown periods (Fountoulakis et al., 2022).
Sampling bias further complicated inter-study comparisons due to recruitment strategies as well as differences in online, population-based, or specific subgroup characteristics. Measuring strategies further explain discrepancies between studies (Knudsen et al., 2021; Thombs et al., 2018) and highlight the difficulties posed by comparing studies using different measures. For example, online surveys may have overestimated the increase of CMD, while interview-determined anxiety and depressive disorders reported more stable trends in 2020 (Kessler et al., 2022).
A further reason for the apparent variations in results might lie in how psychological responses to major disruptive events are constructed. Here, it may be helpful to differentiate between mental distress and mental disorders when interpreting psychological responses to disruptive events. Mental distress is viewed as a ‘normal human response, when it both emerges and persists in proportion with external stressful situations; it is not merely a less severe or more transient version of disorder’ (Horwitz, 2007, p. 275). Thus, a sense of decreased emotional wellbeing may be an appropriate response to unusually challenging situations. In contrast, mental disorder refers to dysfunctions in psychological, biological, or developmental processes, typically requiring clinical intervention (American Psychiatric Association, 2013). For example, a South African study by Laher et al. (2021) found little change in clinical mental health but reported poorer outcomes on nonclinical measures of general psychological wellbeing. This suggests that psychological distress may have been elevated without significant increases in clinically diagnosable disorders.
Despite the initial concerns, many individuals and communities demonstrated psychological resilience – adjusting well and coping successfully with challenges (Fancourt et al., 2021). Psychological resilience – the ability to bounce back from adversity or trauma and maintain psychological wellbeing – and recovery are considered model responses to trauma and adversity (Galatzer-Levy et al., 2018). Correspondingly, it was also expected that the COVID-19 pandemic would have long-term resilience as its most common outcome (PeConga et al., 2020).
COVID-19 was unprecedented, due to both the scale and duration of its impact, with no viral pandemic of the same magnitude recorded in recent history. This poses a challenge when seeking to find appropriate reference group(s) against which to compare the COVID-19 pandemic experience. One possible analogue would be to look to other major disasters, whether natural or human-made.
Mental health responses after major disasters
Disasters are severely impacting events that overwhelm the coping resources of local communities, among others, by interrupting the usual functioning of society (Makwana, 2019; Morganstein & Ursano, 2020). Major disasters – that is, large-scale traumatic events – typically share three key characteristics (Goldmann & Galea, 2014): first, disasters threaten harm or death to a large group of people, regardless of the actual numbers of lives ultimately lost; second, they affect social processes, causing disruption of social networks and communal loss of resources; and third, they involve secondary consequences, including identifiable mental and physical health outcomes, among those affected.
COVID-19 represented unchartered terrain. Disasters are typically events that are concentrated in space and/or time, whereafter society can eventually consolidate and rebuild. Unlike other disasters, COVID-19 was a prolonged event that disrupted social life rather than infrastructure. Regulations around physical distancing and restrictions on gatherings deprived communities of the critical coping resource of social support. One such example was the inability to activate communal customs of grieving, leading to disenfranchised grief, expressed in mental distress (Doka, 2002; Fisher & Kirkman, 2020; Fisher et al., 2020; Van Wijk, 2023). COVID-19 further differed in its continuing and long-lasting duration, with waves of increased morbidity and mortality and associated social restrictions, repeated over a lengthy period of time.
Despite such differences, insights from disaster-response literature may still apply. Research shows that most people are resilient to disasters, experiencing distress that peaks within the first year before returning to pre-disaster levels, while others may experience delayed onset or prolonged symptoms (Goldmann & Galea, 2014). On a more granular level, a range of different trajectories (of psychological adaptation) following exposure to severe stress have been described (Norris et al., 2009) and are presented in Table 1.
Trajectories of psychological adaptation following exposure to severe stress.
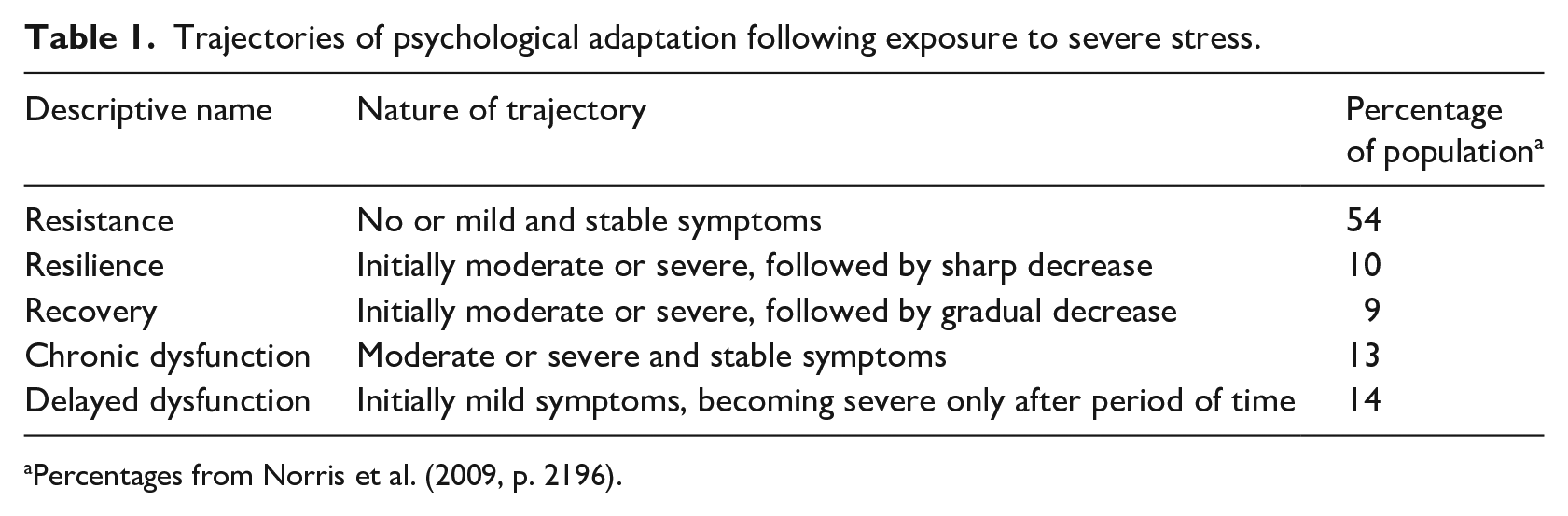
Percentages from Norris et al. (2009, p. 2196).
The prevalence of CMD after disasters depends on factors such as exposure level, post-disaster social support, and pre-disaster mental health (Goldmann & Galea, 2014; Keya et al., 2023). Three key pre-disaster risk factors for post-disaster mental illness have been identified, namely prior mental health difficulties, female gender, and younger age (Goldmann & Galea, 2014). Other risk factors include low socioeconomic status, poor social support, job loss, and/or displacement during or shortly after the disaster (Goldmann & Galea, 2014; Keya et al., 2023). Furthermore, while comorbid mental health disorders often increase after disasters, only a small percentage of individuals with post-disaster distress actively seek treatment (Goldmann & Galea, 2014; Wang et al., 2005).
COVID-19 and the prevalence of CMDs in South Africa
The impact of COVID-19 on mental health in South Africa needs to be viewed against the broader prevalence of CMD locally. The most comprehensive estimates come from the South African Stress and Health study (Herman et al., 2009), which drew on data from 2003 to 2004. It reported, among other findings, the 12-month prevalence of major depressive disorder (MDD) at 4.9% and generalised anxiety disorder (GAD) at 1.4%. Somewhat higher rates have subsequently been reported among student populations (12-month prevalence of MDD at 13.6% and GAD at 20.8%; Bantjes et al., 2019) and general workplace samples (lifetime MDD at 26%; Stander et al., 2016). Yet other workplace samples reported relatively similar figures as Herman et al. (2009), with MDD at ±4% and GAD at ±5% (Peltzer & Phaswana-Mafuya, 2013; Van Wijk et al., 2021). In contrast, two recent studies presented a rather different view, reporting substantially higher estimates: a student sample reported a 30-day prevalence of MDD at 15.4% and GAD at 10.9% (Bantjes et al., 2023), while a national sample reported weighted estimates of probable MDD at 25.7% and GAD at 17.8% (Craig et al., 2022). The data for both studies were collected during COVID-19, but its influence on the findings is unknown.
South African prevalence estimates remain variable across studies, among others due to differences in (1) sample populations accessed (e.g., students vs working adults vs primary health care users vs national surveys); (2) mechanisms of measurement (e.g., self-report tools vs diagnostic interviews); and (3) timing (e.g., before COVID-19 vs during COVID-19). In practice, CMDs appear more prevalent among university students than the general population (Bantjes et al., 2019), self-report screeners tend to elicit reports of more severe symptoms when compared to structured interviews/schedules (Thombs et al., 2018; Van Wijk et al., 2021), and COVID-19 appeared to have worsened the national mental health burden in South Africa (Nguse & Wassenaar, 2021). Being a woman consistently conferred a significant risk for both mood and anxiety disorders (Bantjes et al., 2019; Herman et al., 2009; Van Wijk et al., 2021). Prevalence estimates further differ across provinces, age, and education (Craig et al., 2022; Herman et al., 2009). In particular, being older and retired and only having a primary school education increased the odds of probable MDD or GAD diagnoses in the general population (Craig et al., 2022).
These different methodologies across studies and the inconsistent observations reported complicate attempts to discern the effects of the COVID-19 pandemic on mental health in South Africa. Early studies reported increased self-reports of depression and anxiety among students (Pretorius, 2021; Visser & Law-van Wyk, 2021) and other adults (De Man et al., 2022) during 2020, while others found no significant changes in clinical mental health (Laher et al., 2021). By 2021–2022, some studies indicated a dramatic rise in MDD and GAD among both student and national adult population samples (Bantjes et al., 2023; Craig et al., 2022). The magnitude of increase was of concern, given the challenges to access mental health care in South Africa. Historical inequality, resulting in differential access to public mental health care, as well as social stigma concerning the use of mental health care, has long obstructed optimal mental health care (Sorsdahl et al., 2023).
Trajectories of mental health across COVID-19
South African studies conducted during 2020 and 2021 (Bantjes et al., 2023; Craig et al., 2022) reported higher prevalence estimates than generally observed in pre-COVID-19 studies. However, it remains unclear whether this was sustained during later waves of the pandemic and after COVID-19 had become endemic or whether a return to pre-pandemic levels occurred. A six-wave Argentinian study (López-Morales et al., 2023) reported an increase in anxiety and depression over the first 13 months of the COVID-19 pandemic, whereafter anxiety decreased to initial levels by 24 months. Depression only decreased after 24 months. While international systematic reviews suggested that anxiety and depression returned to pre-COVID-19 levels within 24 months (Robinson et al., 2022; Sun et al., 2023), long-term data from South Africa remain scarce.
To consider local trajectories of mental health, longitudinal data that can reliably compare CMD prevalence estimates from before, during, and after COVID-19 in South Africa are required. Data from an occupational mental health surveillance programme are available for the most recent five consecutive years (2019–2023), which traverses this period.
Context of current study
This study drew on data from the Institute for Maritime Medicine (IMM) in Cape Town, which offers comprehensive primary and occupational health care services to industry. This includes a routine mental health monitoring programme that is conducted using psychometric scales, and employees and their families may voluntarily participate on an annual basis. The programme is managed by a clinical psychologist working in a multidisciplinary team. The current analysis used prevalence data from 2019 to 2023 that were collected as part of the above longitudinal occupational health surveillance programme in a stable workplace population.
Between April 2020 and September 2022, in response to COVID-19, the IMM maintained an intensified mental health service delivery programme, involving three key aspects: (1) frequent community screening of mental distress for early identification and intervention, whereby employees participated in voluntary screening during routine visits to medical clinics, during workplace outreach opportunities, and during vaccination drives; (2) prevention initiatives, including the distribution of brochures and posters in the workplace as well as workgroup briefings on topics associated with stress management and psychological adjustment during COVID-19; and (3) increasing the availability of psychological services, including telephonic consultations, and extending psychologists’ working hours.
Aim
The primary aim of this analysis was to describe the trajectories of self-reported CMD. This was determined by repeat administration of clinical screeners in a carefully delineated population across five consecutive years. The analysis compared reported MDD, GAD, and suicidal ideation before, during, and after the COVID-19 pandemic. The analysis focussed specifically on CMD as a representation of problematic psychological adaptation requiring clinical attention. A secondary aim was to consider associations with gender, age, and psychological resilience.
Methods
Participants and sampling
The analysis employed a longitudinal cohort study design. The populations from which the samples were drawn were accessed through employer-sponsored occupational health care programmes that also included access to mental health care. Participants were distributed across many different fields of work, for example, engineers, technicians, security services, and clerical catering staff. However, they shared one important characteristic, namely their relative protection of income security; throughout the COVID-19 pandemic, there was no imminent threat of termination of employment contracts. All the participants had completed at least secondary education, with further vocational training, and were classified as skilled workers.
The five samples (see Table 2) were deemed comparable. They were drawn from the same community (the same employers), within the same geographical area (Western Cape), and were similar in terms of age, gender, occupational field stratification, and overall health status. As the data were de-identified for inclusion into the analysis, it was unknown how many participants were included in more than one sample. For the same reason, rates of SARS-CoV-2 infection among participants were not known.
Composition of the five samples used for common mental disorder prevalence calculation.
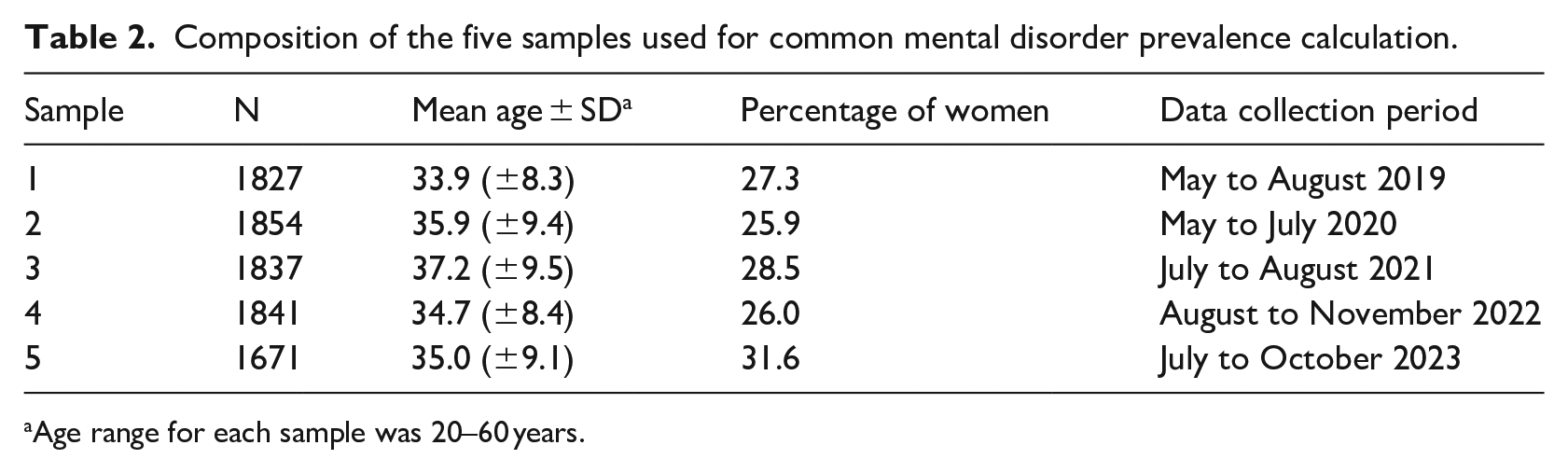
Age range for each sample was 20–60 years.
Measures
The data set included two examples of CMD, namely MDD and GAD. Diagnostic cases were determined through clinical screening tools based on self-reported symptoms, with both screening scales locally validated.
The Patient Health Questionnaire-9 (PHQ-9) assesses the severity of depressive symptoms (Gilbody et al., 2007), with a score of ⩾10 considered a positive screen for depression in low- and middle-income contexts (Akena et al., 2012). In the present analysis, Cronbach’s α = .85.
The Generalised Anxiety Disorder-7 (GAD-7) questionnaire assesses the severity of generalised anxiety symptoms (Löwe et al., 2008) and also of panic disorder, social anxiety disorder, and post-traumatic stress disorder (Kroenke et al., 2007). A score of ⩾10 was considered a positive screen for anxiety disorders (Kroenke et al., 2007; Löwe et al., 2008). In the present analysis, Cronbach’s α = .89.
Suicidal ideation (‘thoughts that would be better off dead, or hurting self in some way’) was determined by coding Item 9 of the PHQ as 0 (not at all) or 1 (several days/nearly every day). Mental health care usage statistics from the IMM were obtained from its annual internal reports, calculated as mean per annum outpatient consultations per clinician. Sample 1 also had data available for the Connor–Davidson Resilience Scale-10 (CD-RISC-10; Campbell-Sills & Stein, 2007), which measures general psychological resilience. In the present analysis, Cronbach’s α = .86.
Data analysis
All statistical analyses were conducted by means of the Statistical Package for Social Sciences (IBM SPSS for Windows, Version 28). Prevalence estimates (Aim 1) were calculated as follows: diagnostic likelihood was determined using total scores that met the established thresholds for each screener and reported here as a percentage of the sample. Furthermore, population estimates, using 95% confidence intervals, were calculated and reported. In support of Aim 2, adjusted odds ratios (ORs) were calculated to examine the contribution of gender, age, and resilience to risk for diagnosis.
Ethical considerations
The study used retrospectively extracted archival data that were de-identified prior to inclusion in the analysis. Institutional Review Board approval for use of the data was obtained.
Results
The prevalence of MDD, GAD, and suicidal ideation across the 5 years is graphically represented in Figure 1, and the details are presented in Table 3. The percentages for MDD and GAD initially remained stable before peaking at about 18 months after the onset of the COVID-19 pandemic and thereafter returning to pre-COVID-19 levels. Suicidal ideation decreased during 2020 but then returned to pre-COVID-19 levels by 2021 and remained stable for the rest of the analysis period.
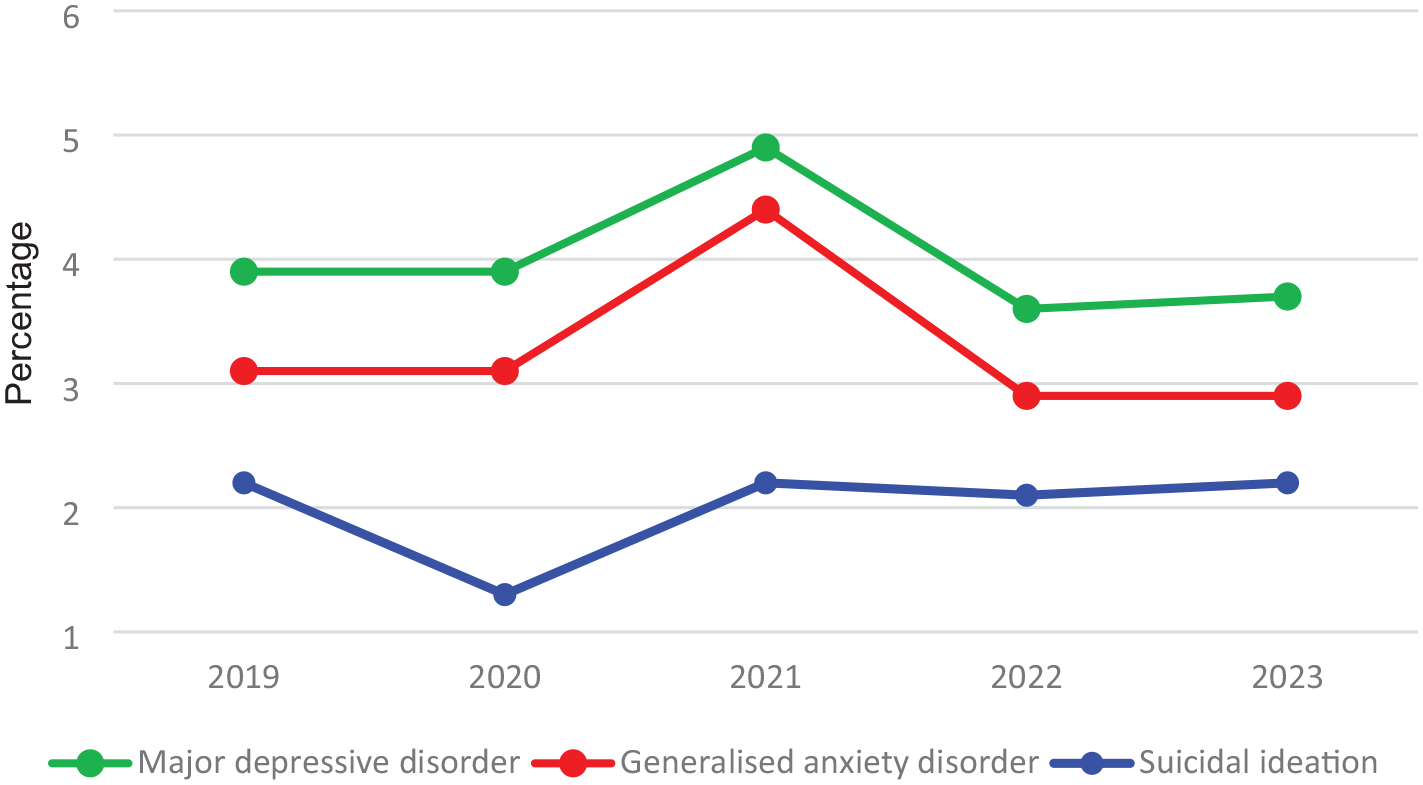
Prevalence of selected common mental disorders across five consecutive years.
Prevalence of common mental disorders across 5 years (2019–2023).
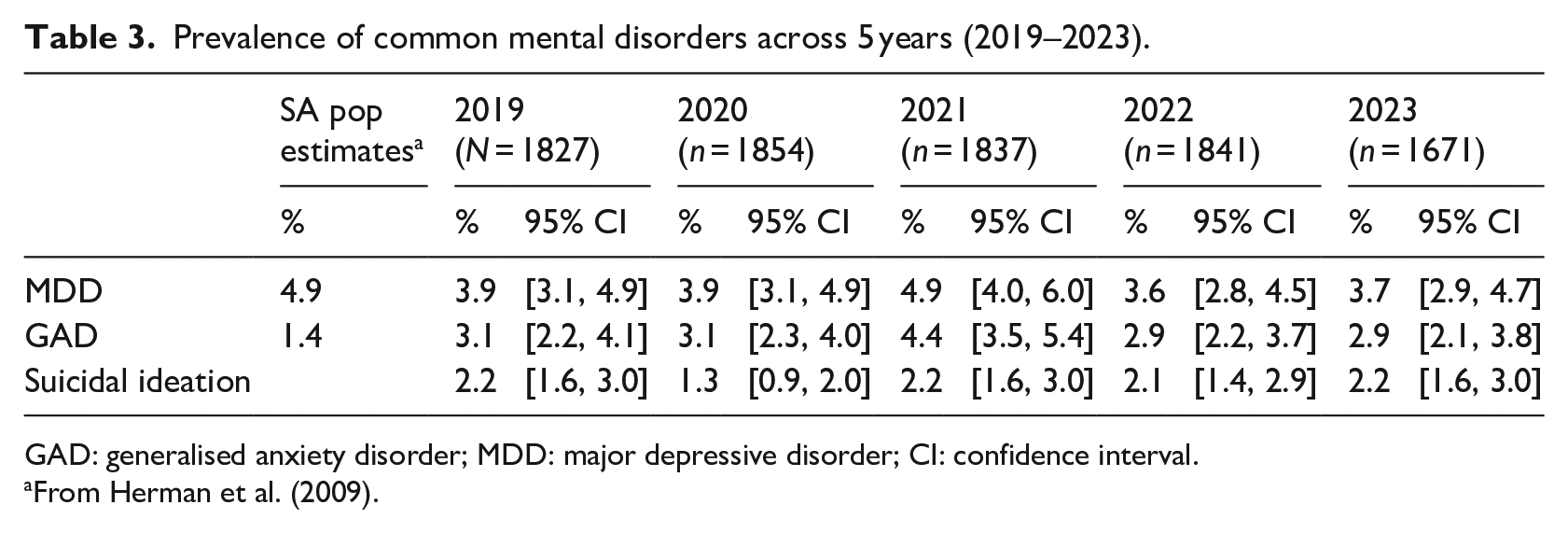
GAD: generalised anxiety disorder; MDD: major depressive disorder; CI: confidence interval.
From Herman et al. (2009).
There was a significant association with gender but not age across the study period. Women were consistently at significantly greater risk for MDD (OR = 2.08) and GAD (OR = 2.44) across the five samples, with minimal year-on-year variability but were not at significantly increased risk for suicidal ideation across the five sample years. In this restricted sample range, age did not significantly differentiate risk for diagnosis. The mean score for the CD-RISC-10 was 32.8 (±5.3), which was significantly higher than that of South African students or original validation samples (namely 26.9 and 27.2, respectively, ps > .01; Pretorius & Padmanabhanunni, 2022). Higher resilience scores were associated with significant but small protection against MDD (OR = 0.77), GAD (OR = 0.79), and suicidal ideation (OR = 0.76) in Sample 1.
The mental health care usage statistics for the IMM have remained stable across the reporting years 2016–2019, with a 70% increase observed from mid-2020 to end 2021, before slightly easing off into 2022.
Discussion
The primary aim of this analysis was to describe the trajectories of self-reported CMD, traversing the period before, during, and after COVID-19. The longitudinal trajectory suggests relatively low prevalence and temporal stability of CMD compared to local (Bantjes et al., 2023; Craig et al., 2022) and international (Daly et al., 2020; Ettman et al., 2020; Pierce et al., 2020; Winkler et al., 2020) studies. The unexpectedly low prevalence of CMD and the specific trajectories of CMD and suicidal thoughts are discussed below.
Prevalence
The CMD prevalence estimates remained low throughout COVID-19 compared to other local studies (cf. Bantjes et al., 2023; Craig et al., 2022). Inherent sampling characteristics may account for some of this. Higher-risk sociodemographic groups (e.g., women, the very young or old, the less educated, and the unemployed) were either underrepresented or excluded from this sample. Furthermore, this analysis only used data relating to CMD and did not include measures of general mental distress, which would more likely reflect increased levels of distress. The samples might not reflect broader South African society.
Possible sampling biases aside, three factors may have mitigated a threatening mental health pandemic in this population. First, the sample population had access to readily available employer-sponsored health care. This included regular monitoring to identify and refer cases of concern, free psychological referral, clinics in close geographical proximity, and time off work to attend them. Furthermore, in contrast to typical post-disaster responses (Goldmann & Galea, 2014), the actual use of mental health services increased substantially during 2020 and 2021. The employee-initiated self-referrals enabled active monitoring, identification, and psychotherapeutic interventions whereby mental health concerns could be addressed. The high-intensity early interventions may have facilitated adaptive coping in this population, potentially preventing CMD escalation.
Second, income security was maintained, and most of the sample population was never under significant threat of unemployment or retrenchment. Employers achieved this through creative scheduling and shift work and using employees in essential-work capacities. This reduced uncertainty and preserved financial security – a critical coping resource.
Third, psychological resilience, known to protect against mental health deterioration during the pandemic (Pretorius & Padmanabhanunni, 2022), may have served a similar role in this population. In Sample 1, resilience was associated with lower levels of MDD and GAD. Resilience, often described as ‘bouncing back from adversity’ could explain the CMD prevalence trends: an initial resistance, then a rise in CMD, followed by a return to pre-pandemic levels. This could be hypothesised to reflect this community’s resilience in recovering from the social and psychological impacts of COVID-19.
Two key constructs that most strongly predict resilience, namely the cultivation of social support and adaptive meaning making, can be learned and acquired (PeConga et al., 2020). Social capital, or the value derived from positive social connections, can enhance resilience to psychopathology by fostering a collective sense of purpose and meaning making during crises (PeConga et al., 2020). Strengthening social capital may be crucial in protecting communities from future large-scale disruptions.
In summary, the relatively low prevalence of clinical maladjustment and the factors facilitating this occurrence in the study population, compared to other communities, may illustrate the ‘differential effects of the pandemic on different population groups’ (cf. Fountoulakis et al., 2022, p. 11).
Trajectory of CMDs
Higher levels of psychiatric symptoms are often reported soon after major natural disasters but also resolve relatively soon thereafter (cf. Goldmann & Galea, 2014, for review). In the current population of employed adults, the prevalence of MDD and GAD remained stable during the early lockdown periods, only increasing about 18 months after the onset of the pandemic before returning to pre-COVID-19 levels by 2022 and maintained through 2023. This observation may reflect the ‘delayed onset trajectory’ seen in mental disorders following major disasters (Norris et al., 2009). Deferred presentation of psychiatric disorders subsequent to disasters, while less common, is well documented (Goldmann & Galea, 2014; Morganstein & Ursano, 2020; Norris et al., 2009). The peak at 18 months aligns with findings from other large-scale disasters (e.g., earthquakes and floods) according to which increases in mental disorder prevalence plateau within 24 months (cf. Morganstein & Ursano, 2020, for review).
However, the ongoing nature of the COVID-19 pandemic complicates the delayed response hypothesis. Rather, the unremitting nature of the pandemic may have led to the cumulative effects of disruptions and their consequences taking their toll on mental health, as the 18-month peak in CMD suggests. Around this time, patients at the clinics expressed increased distress due to increased financial pressures from supporting family members who had lost their jobs and dealing with the loss of family members during COVID-19, amid the unavailability of traditional collective mourning practices due to lockdown restrictions (Fisher & Kirkman, 2020).
The return to pre-COVID-19 levels by 2022 may speak to the personal psychological resilience of this particular South African population to adapt to new situations or to the effectiveness of the mental health interventions provided by the IMM. Adaptation, defined as the process by which individuals or groups make changes (cognitive, behavioural, and affective) in response to new environmental conditions to maintain quality of life (Psychology iResearchNet, 2023), could explain this return to baseline. People are disposed towards stable levels of wellbeing and thus tend to adapt back to baseline levels within a certain period of time after disruptive events (Lucas et al., 2003). Consistent with systematic reviews of global data, the prevalence of anxiety and depression appears to have returned to pre-COVID-19 levels by 24 months after the onset of the pandemic (Robinson et al., 2022; Sun et al., 2023).
Two notes of caution need to be considered when interpreting these results. First, fluctuations in expressions of mental distress were closely associated with COVID-19 waves and troughs and ‘alert levels’ (Kwong et al., 2022; Van Wijk, 2023). In particular, mood response differences between wave peaks and troughs were significant and were temporally associated with periods of increased infections/mortality (and increased government-imposed restrictions) during the waves and with reduced rates of infection (and easing of restrictions) during the between-wave periods (Van Wijk, 2023). Thus, CMD prevalence may have been influenced by the timing of data collection each year.
Second, there are limits to the extent that CMD can be associated with specific events. The aetiology of CMD is located in complex intersections of biological, environmental, social, and psychological factors, and their occurrence cannot always be attributed to specific external events.
Trajectory of reported suicidal ideation
Suicidal ideation decreased during the early lockdown period and returned to pre-COVID-19 levels within 18 months and thereafter remaining stable through to 2023. While the reasons for this remain unclear, two hypotheses may offer some insight.
First, COVID-19 could be viewed as a collective experience that affected the whole of society. Suicide has been associated with subjective feelings of being alone (Calati et al., 2019), and the early collective experience of COVID-19 could have given vulnerable individuals a sense of connection to their larger communities by virtue of the common experience. This could also have given them the opportunity to focus externally on the wider world sharing the same experience rather than on the internal entrapment often associated with suicidal thoughts (Rogers & Joiner, 2017). As COVID-19 progressed and the common experience fractured, the positive impact could not be maintained and suicidal thoughts returned to pre-pandemic levels.
Second, for this specific population, the initial lockdown simplified life by limiting movement, activities, and shopping opportunities. Employees spent time with immediate families, saved on expenses, and so forth. Reduced life stress during the early stages of COVID-19 has been postulated to protect against suicide (Knudsen et al., 2021) and may have served a similar function for the current study population.
Evaluation of study
Few studies have provided data beyond the first 24 months of COVID-19. The current study covered the period from before the COVID-19 pandemic to its endemic phase late in 2022 and used the same delineated population and the same measuring tools throughout. The longitudinal design allowed for consistent comparison across the entire pandemic period and beyond. It also avoided the difficulties associated with comparing studies using different measuring tools. This study corroborated international findings of CMD prevalence returning to pre-COVID-19 levels by 24 months. It further demonstrated that these levels continued to remain stable for at least another year.
The study has certain limitations. The sample comprised employed adults with relative income security, which limits the generalisability of the findings to the broader South African society. In addition, only a narrow range of CMDs were examined. Future studies should include conditions such as adjustment disorders, which are closely linked to stress responses. The use of self-reported symptoms rather than clinical diagnoses may be a limitation, but this was consistent across all samples, minimising concern. Finally, the timing of data collection was not aligned with actual COVID-19 waves in South Africa, which at the time could not have been predicted and which may have influenced the results (Fountoulakis et al., 2022). Future studies in related circumstances could benefit from time series analyses to assess the statistical significance of changes over time.
The analysis of mental health data from the COVID-19 era offers several practical lessons for future major social disruptor events. Early, high-intensity intervention can support individuals in adapting to challenging situations and possibly mitigate mental disorder escalation. This refers to interventions that are active, targeted, potentially complex, and delivered by registered psychologists. The greater challenge might lie in the requirement to maintain the intensity of support for at least 18 to 24 months, which would require careful planning and resourcing. Furthermore, the study highlighted the value of regular, frequent monitoring of mental health to enable informed planning and delivery of appropriate services. Employer efforts to protect job security and offer employees a sense of purpose through essential-work roles may speak to the positive contribution that employers can make to their staff’s mental health during major disruptor events. Finally, developing psychological resilience on a societal scale (PeConga et al., 2020) is essential to mitigate adverse mental health impact, not only for future disasters but also for current psychological wellbeing.
Conclusion
This article described the trajectories of self-reported CMD across five consecutive years, spanning the period before, during, and beyond COVID-19. Relatively low prevalence was reported, among others, due to readily available access to mental health care, income security, and possibly also the resilience of South Africans to adapt to changing life demands. The study further suggested the importance of regular mental health monitoring to provide high-intensity interventions after major societal disruptor events as well as the need to maintain the intensity of support for at least 18 to 24 months.
Footnotes
Acknowledgements
The author(s) wish to recognise Ms Marilize Fourie and Ms Pinky Majola who truly went above and beyond to provide psychotherapeutic services to those in need during COVID-19.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical considerations
The paper used archival data, with ethical oversight for the analysis provided by the Stellenbosch University Health Research Ethics Committee (#N20-07-078).
Disclaimer
The views and opinions expressed in the article are those of the author and do not necessarily reflect an official policy or position of any affiliated agency of the author(s).
Data availability
The data are not publicly available due to privacy and ethical considerations.