
Abstract
Within the South African context, psychoanalysis as praxis and research has not located itself outside of the country’s long, violent, and oppressive socio-political past. A major area in which psychoanalysis continues to demonstrate a deficit is in its lack of attention to race as constitutive of psychological development and a site of intense psychological pain. A further area that is often overlooked in both the theory and praxis of psychoanalysis in South Africa is the diseased body as a site of socio-political violence and oppression, and the subsequent impact of this trauma on intrapsychic development. This situation is particularly applicable in the development of Black children who are vertically infected with HIV. The focus of this article, the fourth in a series of five articles, is on the process of grief and mourning in three vertically infected HIV-positive adolescents. Findings indicate that children who are vertically infected with HIV suffer multiple losses leaving them with intense unprocessed grief despite having access to individual therapy. In addition, their raced subjectivities add to experiences of non-being leading to grief which remains minimised and overlooked within the psychoanalytic canon, keeping the mourning process hidden in historically oppressive systems as melancholia.
Black bodies have been the site of devastation for centuries. We who inhabit and love these bodies live in a state of perpetual mourning. We mourn the disproportionate dying in our families, communities and the dying in the black diaspora.
Decoloniality in both theory and praxis within the South African psychoanalytic field has found strong roots in socio-political debates (Maldonado-Torres et al., 2021; Ratele, 2017). This decolonial stance is entrenched in a strong desire for change in which diversity and multiplicity seek to subvert established authority in the psychoanalytic space that remains entrenched in homogeneous thinking. Fanon (1952) traversing psychoanalysis and phenomenology first raised the direct connection between the political and the practice of psychoanalysis in a racist neocolonial society offering us a theoretical framework to examine historical political contexts within the practice of psychoanalysis. Expanding on Fanon’s work, Maldonado-Torres et al. (2021) articulate the view that to be attentive to the wounds of the post-colonial world, the affect of the oppressed requires a focus as a potential site of healing that can transcend the clinic of psychoanalytic universalism. It is argued that the implied undertaking is not simply a matter of repurposing but to trouble the decolonial attitude from within psychoanalysis (Boutebal, 2020; Maldonado-Torres et al., 2021).
To politicise affect as a feature of lived experiences in relation to oppression requires a movement through historical spaces and subjectivities. This approach will open up a space in psychoanalysis to recreate transformation and move towards radical hope, not just in our interiority but where struggles are located within existing realities of systemic oppression. One significant area that psychoanalytic theory has yet to fully acknowledge and engage with is the process of
In this article, I ask the following questions: Where has the sorrow of the devastation of Black lives in South Africa gone? Does this grief even matter to us as a country? Are psychoanalytically informed psychologists complicit in keeping the grief of millions of Black South Africans out of the national gaze and hidden in the privacy of the clinical rooms in an unprocessed and unthought-of manner? To explore these questions, this article considers the relevance of mourning and melancholia and its intersections with HIV and race. The experiences of three Black adolescents who have been vertically infected (infected at birth or very close to birth) with HIV are presented. The first part of the article engages with the loss, grief, and mourning process of the adolescents, locating this discussion within an object relations reading of Freud’s (1957) work on mourning and melancholia and Kleins’ (1940) work on mourning and its relations to the depressive states. The second part of the article engages with the politics of grieving through the examination of the subjective impact of socio-political conditions that have come to impact deeply on the grieving process of the three participants. The participants’ unfinished process of grieving through their raced and diseased experiences is considered, keeping in mind the implications of these experiences for psychoanalytic theory and practice in relation to the decolonial turn in contemporary South Africa. This focus is of particular significance, as this article allows for the interrogation of how unfinished grieving processes are kept in place by socio-political conditions that have become entrenched in structural ways, and traditional psychoanalysis remains complicit in maintaining this status quo.
Mourning and Melancholia
Within the traditional psychoanalytic canon, loss and grieving are seen as an instrumental process with a return to normalcy that must take place in a timely manner. Freud (1957) gave mourning a central place in psychoanalytic thought. In his article Mourning and Melancholia, Freud (1957) makes an important distinction between the two concepts. Mourning is defined as a natural process of grieving that involves the acknowledgement of the loss, the experience, and the expression of the grief around that loss and letting go of the attachment to the lost object. The ego manages the reality of the loss redirecting the libidinal energy away from the lost object and into a new direction, leading to an eventual resumption of full living. With melancholia the painful loss is not adequately grieved, leading to a more permanent inhibition in the mourner’s capacity to love and relate to the world. There is a component of self-reproach, a turning on the self in internalised anger, harsh criticism, and self-blame. In melancholia, we find a dictatorial superego that rages against the ego with merciless violence. With this anger comes a foreclosure, an incomplete and irresolvable grief, forever trapping one in a pathological state of being.
However, in Klein’s (1940) work, we find the role of reparative love at the core of the superego, the task of mourning, and the development of the ego. What makes possible the attainment of the depressive position (a developmental task in the infant that allows for the coming together of both good and bad through some resolution of feelings of guilt and anxiety) is a process of mourning. Klein moves away from Freud’s consolidation of the ego that has been foreclosed through repressed losses and allows us to engage with the rich internal world of ambivalent objects and the holding together of this ambivalence. In the depressive position, we can come to terms with the ambivalence of our beloved objects. We mourn not only the actual death of our loved ones but also the death in its perfect and idealised forms. In Klein’s work, we see mourning as an important task in the integration of the ego but with a greater synthesis between the internal and external worlds, and a development of the psyche with the whole; ambivalent objects holding both love and hate. By overcoming the melancholic aspects of the paranoid-schizoid position (the earlier developmental process where feelings of persecution predominate through the splitting off of good parts of self), the milder superego appears. This appearance allows for engagement with our external world without the overpowering phantasies of persecutory dread or idealised love. Klein’s work offers an opening into the external world as part of our developmental processes, which gives us a platform to engage with the decolonial turn in psychoanalysis, particularly with raced and diseased subjectivities (Patel & Graham, 2019).
HIV and grief
Grief in the traditional psychoanalytic canon is individualised, severed from its historical context, and mourning is turned into a private affair closed off from public consciousness. Within the South African context, HIV-related deaths are not easily spoken about. The topic remains not only a difficult private conversation but also a deeply uncomfortable public conversation (Posel et al., 2007). HIV-related death has come to be seen as a ‘bad death’ linked to physical illness that is reflective of a society that is ill. Cultural lapses are seen to have caused new patterns of biological death in relation to HIV. A close relationship has been developed between the health of the social body and the health of the individual body (Posel et al., 2007). As such, HIV-related grief has become something that is shameful and hidden away from the public eye. Illness, death, and grieving for those who are HIV-positive have become medicalised, to be defined, understood, and treated through a medical framework. The classification and identification of grief itself have been taken up by the field of psychiatry and psychology (Lund, 2021). Depression, for example, has become contrary to the normative order of society. Those who are depressed must be treated and cured within a set time to satisfy society’s desire for normality (Lund, 2021). Lund (2021) offers the argument that grief is both constitutive of and constituted by society and as such will always remain as a site of trauma for individuals, and attempting to make sense of death and grief then becomes the manifestation of these attempts.
In an attempt to move away from the medicalised discourses around HIV and to reconstitute an African identity that challenged the ravages of colonialism and apartheid, the South African government under the leadership of Mbeki in the 1990s and early 2000s sought a new HIV subjectivity (Nkomo & Long, 2014). There was a drive to move away from Africa as the dangerous other, the diseased other, the primal other, and the other with rampant undesirable desires. Notwithstanding the challenges in this discourse at the time, Nkomo and Long (2014, p. 426) articulate: Within the African renaissance discourse, the subjective and cultural effects of a history of racism and oppression under colonialism (and particularly ‘apartheid’) on African subjectivity demanded a reconstitution of a positive ‘knowledge of the past’ as a significant pre-condition in the constitution of a new African patriot.
The Mbeki administration’s policy on HIV was a terrible failure, prompting HIV-related challenges even further into medicalised outcomes. However, an opportunity was presented for decolonial theorists and practitioners, including those who practice from a psychoanalytic frame, to relook at the ways in which those who struggle with the challenges of being HIV-positive continue to be disenfranchised. This includes the experience of grief, which is a complex historically contingent amalgam of significations located in the dynamic movement of socio-ecological relations (Langstaff, 2016). Nowhere can this impact have more meaning than for those affected or infected with HIV. As an illness that has long been embedded in cultural and socio-political meaning, HIV-related loss is far from an obstacle to overcome, and grieving is an instrumental process to be followed within a time-limited frame.
Method
This research is situated within the philosophical interpretivism paradigm, which includes ontology as reality, reality as subjective; and knowledge as relative and socio-culturally value-bound. Furthermore, use has been made of the hermeneutic cycle as an interpretation of meaning across socio-historical and political terrain. The methodological tension inherent between the phenomenological aspects of the hermeneutic cycle and interpretive aspects of the psychoanalytic framework of knowledge has been traversed by the phenomenological–hermeneutical circle (Cartwright, 2004). This approach remained within the aims of this project, which was to describe in-depth and in detail the deeply embedded elements of HIV and raced experiences and how these elements are taken up in the unconscious of the vertically infected HIV-positive adolescent to elucidate psychodynamic-based sociogenic meaning (Patel & Graham, 2022). In keeping with the phenomenological aspects of this study, only a small sample of participants was required, lending itself to the in-depth, three-session psychoanalytic research study method (Cartwright, 2004). Data from the three participants presented in this article was drawn from a larger data set. The psychoanalytic interview technique was used to elicit data (Cartwright, 2004). Furthermore, to elicit meaningful unconscious material, the projective drawing method was used to get closer to the participants’ intrapsychic world. The drawings were used to elicit the participants’ internalised experiences of themselves in relation to their biological mothers as well as their HIV status and are presented in this article. In addition, the narratives from the interviews are presented as part of the findings. Three interviews were conducted with each of the participants with a week in between each interview, allowing for some transference reactions to develop. The duration of each interview was approximately an hour and a half. The interviews were video recorded allowing for the capturing of verbal as well as non-verbal information. Data analyses were primarily concerned with careful attention to feeling states and corresponding thoughts and perceptions; and the search for core experiences, identifications, and object relations as outlined by Cartwright (2004) and in keeping with the principles of double hermeneutics. All ethical protocols were followed very closely. The following are the projective drawings depicting the participants in relation to their mothers and HIV status.
Nosipho Ntombi Isisa: Pic 1. Isisa: Pic 2.
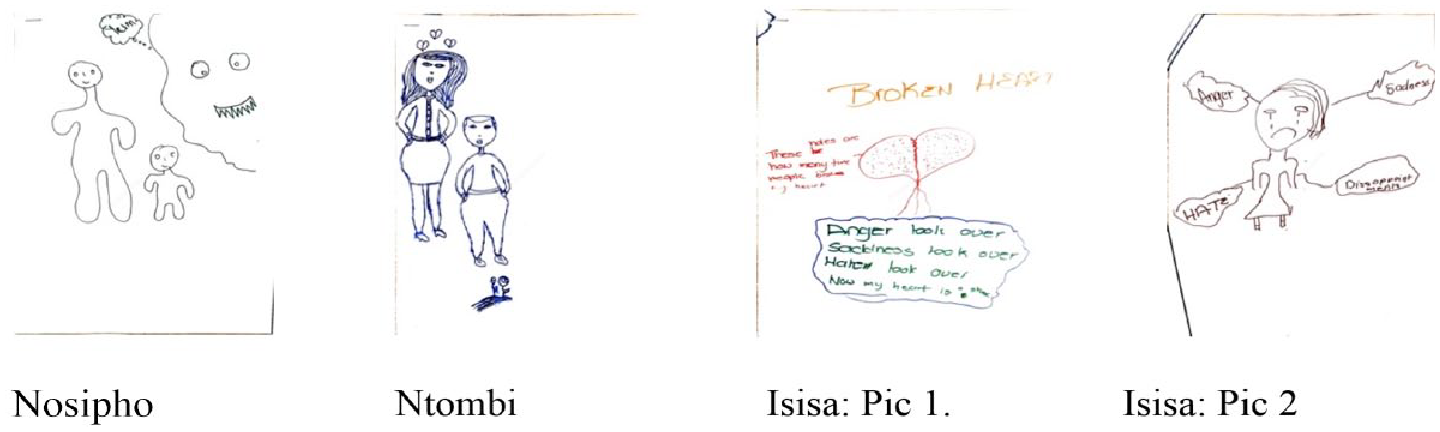
While Nosipho was more engaging with the researcher and expressed her deep grief in talking about her mother, her black subjectivity, and her HIV status, Ntombi and Isisa found it difficult to engage with the researcher. Ntombi was more guarded about hurting the researcher’s feelings and causing an injury, particularly during our conversations about race. Isisa was outwardly rejecting the researcher, expressing her anger and hatred more openly during the interviewing process. Nosipho while being more open in her curiosity about me, expressed her anger in a more passive manner. She questioned my ‘greed’ for not being satisfied with what I have and wanting to pursue a further higher degree. When I responded to her questions about my family, she initially became silent and then responded sadly that my children were lucky to have a mother. My own transference reactions with Nosipho throughout the time I spent with her were steeped in chest-gripping sadness. I wondered where her rage was hiding. Conversely, my time with Isisa was dominated by waves of hate and rage reactions. Throughout this research process and more particularly through the interviews, I was painfully and acutely aware of my own intersectionality. In my own life, and having lived through a period of apartheid as a person of colour, I have worn my skin in various uncomfortable ways. More recently, I have had to sit with the discomfort of the role I play as a middle-class woman of mixed-race heritage in maintaining the status quo of structural privileges. Although all this was unsaid between us during the interviews, the presence of our differing intersectionality danced around us in swirls of sorrow, guilt, hate, and rage.
Findings
Mourning and Melancholia: ‘Zombies walking through life’
Nosipho, Ntombi, and Isisa live at a care-home for children affected and infected with HIV. Living at the care-home was experienced by all three of them as unbearably painful. Isisa was more open and forthcoming in talking about her negative feelings towards living at this institution – ‘the people here will not make you take your medication for a long time, I am very angry. I hate them’. Isisa expressed continued distrust of others throughout the interviews. The hostile feelings were quite powerfully enacted in the transference reactions between Isisa and the interviewer. Yet even as she expressed this deep hatred and anger that she felt towards the outside world, simultaneously, Isisa expressed a deep internal conflict and vulnerability at having to live as an orphan at the care-home and the fear and despair at the thought of having to leave the only place she has known since childhood as soon as she turns 18 years of age. Her painful vulnerability also showed in her deep grief when asked to talk about her mother. She broke into deep sobs and asked to not talk about her mother. Nosipho was already preparing to leave the care-home as she had turned 18. She expressed a deep anxiety at soon having to fend for herself. When talking about her future Nosipho expressed the same despair as Isisa and also deep anger at having no assistance to help her sustain herself in the outside world. I wondered at times during the interviews where Nosipho might be holding a deeper rage at being let down by the people who were supposed to protect and guide her, which Isisa was able to express more freely. The ‘outside world’ was something Nosipho felt unprepared and fearful of. Ntombe, similarly, spoke about living at the care-home as a difficult space to be in – ‘have to put on that mask of a happy person. If you don’t do that you are like disrespectful. You told, you forget where you come from, you think you are better’. All three were constantly reminded of their powerlessness and dependency on the environment of the care-home due to their HIV-positive and orphaned state. Feeling stripped of dignity, none of them had any deep sense of rootedness and belonging, only passing people and superficial friendships within the context of their daily existence.
Outside of the home, neither Nosipho nor Ntombi can return to their fathers. While their fathers are alive, they have largely been absent in their lives with no hope of any reconciliation. Ntombi talked with great depth of sadness about her dad – ‘He is also married. He has kids. He visits my cousins at home but he never bothers to ask about me and my sister. It is very sad (puts her head down and cries)’. Nosipho described herself as an orphan even though her dad is alive – ‘my dad just disappeared into thin air’. Isisa’s dad died when she was twelve years old and describes this time of loss as intensely painful – ‘I wanted to kill myself’. Isisa cried only once during the interviews, her anger being more visible through her glowing eyes when she did talk about her parents. Physically, her body remains stoic, like a massive oak tree rooted deep in the earth, not wanting to show any vulnerability to the world outside of her. There are multiple losses for all three. Isisa said with a resolute toughness, ‘I am having to get used to it because everyone dies in my family. I have experienced a lot of death in my family’. Similarly, for Nosipho and Ntombi, there have been continued multiple deaths in the family. Leaving the care-home hangs over them like a menacing ghost of loss and sorrow filled with the ambivalence of what it means to say goodbye to the place where they spent their childhood and adolescent years and the uncertainty of what is to come after.
Of significant importance for all three and also a major turning point in their lives was the loss of their mothers, their closest and most significant relationship before death. Nosipho was 9, Ntombi was 6, and Isisa was just 3 years old when their mothers died. Now in their later adolescent years, Nosipho (18), Ntombi (17), and Isisa (16), in remembering their mothers, continue to express deeply painful and continued unprocessed grief. The loss of their mothers remains a continued devastation that lingers in endless mourning, surrounded by confusion, sadness, anger, and hate. Ntombi offered these comments when asked to process her drawing of herself with her mother and in relation to HIV:
Can we have a look at your drawing?
That’s for my mom. Like, it [is] a heartbreak for her and for me, it’s flowers.
Can
For me, it was okay because I did not know that she had the virus and for her it was a heartbreak because she knew that. Maybe one day she would [not] make it in life [and] she [would] have to leave me and my sister.
And thinking about it now, what does it feel like to have a mom who had the virus,
long pause
What are you thinking about?
Ntombi at the moment of the long pause was unable to talk about her mother but instead deflected into a long narrative about missing her cousin back home in Kwa Zulu Natal, wanting to reach out to the cousin, being rejected by the family, and their anger at her very existence in their lives. Her mind slipped away from her mother but stayed rooted in feelings of abandonment, rejection, and her mother’s perceived anger towards her. When Ntombi was asked about the time around the death of her mother, she cried silently but deeply expressing a sorrow that remains unfinished, a terrible heartache that seemed to grasp both of us deep within our chests. The pain Nosipho expressed of having lost her mother lingered heavily throughout our interviews. She described herself as ‘a zombie just walking through life’. Nosipho has become relentless in blaming herself for the HIV infection. Here we see how tyrannical and relentless the self-reproachments were, deeply embedded in her unconscious mind:
I feel like I [am] the one who chose it (HIV). I could have been the irresponsible one. I could have been that child who does [not] look after herself or does [not] care about anyone but herself and screws with everybody, does [ not] care for who she infects
Nosipho you were infected with the virus as a baby but you carry the blame for this?
I [have] read about manifesting. So what if I am manifesting all these things that are happening to me
You blame yourself for your mother’s death but also for manifesting HIV as a baby?
Yes
How would you manifest HIV as a baby or cause your mothers infection and death?
(breaks down crying. Sobs for a while). But then if I don’t take the blame, who must take the blame. . .I have lost my mom and when you lose something very important, I do wish something bad would happen to me.
Nosipho will not allow her mind to hold anyone outside of her responsible for being HIV-positive, instead punishing herself relentlessly through self-destructive guilt. Isisa carries her mother around inside of her as a heart full of holes. Her mind will not allow her to even project a human mother, only a damaged heart. Remembering her mother is unbearable.
There is an unyielding, unshakable intensity to the self-blame and guilt expressed by all three of them. Their narratives are littered with strong self-reproachment expressions of unprocessed and unconscious affective states, which they would have initially directed towards their lost loved one, but now turned inwardly, against the self with the intensity expected from unresolved guilt. For both Freud (1957) and Klein (1940), guilt in its unconscious form is key in both the process of mourning and melancholia and takes place solely in one’s internal intrapsychic world of unresolved conflicts. Not only Nosipho, but Ntombi as well as Isisa show an internal state of irresolvable guilt that feels intensely self-destroying. There is a refusal to acknowledge the loss, keeping the lost object psychically alive by introjecting it into the ego. Contradictory ambivalent feelings get turned into relentless punishment. The expectation would be for Nosipho, Ntombi, and Isisa to acknowledge, express, and let go of their attachments to their primary maternal deaths. The multiple other layers of losses – families, homes, schooling, friendships, their bodies as objects of grief, their bodies as objects of illness, safety, security, and belonging – would find a place in the process of grieving. The component of self-reproachment, a turning on the self in internalised anger, harsh criticism, self-blame, and the dictatorial superego that rages against the ego with merciless violence, is the focus of treatment. However, with this focus comes a foreclosure, an incomplete and irresolvable grief, forever trapping one in what psychoanalysts describe as a pathological state of being. It is here that I take a pause to question psychoanalytically informed theory and praxis complicity in keeping the process of mourning outside of structural elements and thereby creating a double foreclosure of grief.
For vertically infected Black HIV-positive children, ambivalence is a far more complex process (Patel, under review). I have argued, that for these children the essence of their diseased self and well as their raced self holds the struggles of a disease of signification as well as intergenerational raced embodiments. For a Black child who is HIV-positive, it is not only diseased bodies that become a site of mourning, but the black condition becomes one of mourning simultaneously (Patel, under review). Letting go of the guilt and self-recriminations would mean having to accept that the black maternal body did in fact pronounce a death sentence, threatening their very daily existence in a world where they as black children continue to suffer immensely. The continued reality of watching daily other losses either through the death of others or through knowing that the lives they so wish for cannot be attained, they are pulled back into a space of hate, rage, anger, aggression, and anxiety, a space that remains pathologised in the therapeutic setting.
McIvor (2012) puts forward a compelling argument that Klein casts a wider lens on mourning and painful unresolved guilt that allows us a space to think about not separating the intrapsychic processes from our political realities. Where Klein (1940) becomes useful is in her argument that the early paranoid-schizoid position is not only a scene of violent aggression and fear but also one of love and desire. The superego in this early paranoid-schizoid position is built up of various phantasies and experiences with the real and imagined object carrying within it the potential for melancholic persecution. In Kleinian terms, this position is not merely a temporary phenomenon to be worked through as a stage but a position that we are continually pulled into throughout our lives. The anxieties that accompany deeply felt losses will continually tug at us and draw us back into the persecution and attack and draw on our defences to fight against these threats. The litany of losses that are scattered across Nosipho, Ntombi, and Isisa’s young lives and the trauma of these experiences with the accompanying intensity of sorrow and sadness will no doubt pull them back into their earlier paranoid-schizoid position with its accompanying melancholia.
Far from this process being a pathology, Klein’s (1940) reading of our identities resulting not from a deferral of the self, but from positive identifications with ambivalent internal and external realities and objects is important for these children. In the more developed depressive position, the experience of loss is managed to make that loss more bearable and continued life possible. The work of mourning succeeds not through disintegration but integration of the subject, which will not eliminate our grief over, or grievances with others, but will make these grievances more realistic and our efforts to address them more reparative. In sum, mourning involves the acceptance of ambivalence through the integration of complex, multi-sided objects into the subject’s identity. For now, this process seems an impossible task for Nosipho, Ntombi, and Isisa as the deep unrelenting grief that they experience is severed from its historical context and mourning is turned into a private affair closed off from public consciousness. In other words, while Klein offers an inroad into the mourning subject as a platform that opens up an understanding of the political life of mourning the external is still kept out very vehemently in therapeutic practice. Here Langstaff (2016, p. 315) makes a compelling argument that, if we understand our lives as a series of social entanglements, death ripples through various networks of sociality and causes pain. Sometimes we are moved on behalf of those we love who mourn more acutely. This entangled network of grief is a stark reminder that we are not singular insular beings despite capitalisms insistence.
Radical politics of loss and grieving: ‘The white world is perfect. That is what we are told from day one’
The distinction between the melancholic internalisation of loss and the externalisation embodied in the process of mourning is significant for the politics of loss and grieving (Lapping, 2019).
Orbeta (2021), using the analogy of the crow arriving at the death scene, writes about the complete desolation, anger, and feelings of abandonment that are brutal as the crow scavenges at the wounds of the dead. But as the internal world becomes dismantled with painful affect, becoming an uncanny experience, it is not only a sensory experience but one of the material worlds (Lapping, 2019). There is no singular loss, every loss contains within it a multiplicity of socio-political formations.
There is a consistency in the complexity of the adolescents’ experiences, not just in the sorrow of losing the loved object but also of the stigma, discrimination, rejection, and abandonment by family and communities who do not have the resources, be it emotional or material, to take care of their affective, emotional, or material needs. Far from being an individualised process, for these young HIV-positive adolescents there is a foreclosure in their morning process that pulls them back into the endless pit of melancholia. There is denial by the mechanisms of culture but also the culture that is situated within the political histories of both HIV and race in the South African context. In the unequal valuing of life and death, mourning is a contested space, Canham (2017) asks if mourning can be conceived of inexhaustive inventory of losses that has travelled through many generations. Nosipho, Ntombi, and Isisa have not only had to endure the suffering of multiple spaces of inexhaustive losses but also the intense marginalisation and dehumanisation that have come from living in black bodies. They also had to endure the violence of poverty, fractured families, desperate competing for resources, violence in their homes, and lack of interpersonal relationships and a preference for self-isolation. Ntombi as a child grew up in an informal settlement where living on the poverty line was a daily experience for her. She had to bear witness to the violence of the structural failures as a daily experience – ‘You know some people end up in jail for many years just because they tried to make a living. It hurts me seeing people on the street, Imagine, it [is] winter, it [is] this virus’. Nosipho feels completely alone. Feeling let down, abandoned, and punished by her family as well as the care-home. This keeps her in a depressive state of mind: If I fuck up with my life there is no one that would catch. Here at this home (care home), they will rip me apart with horrible words if I had to fail at school. . .. Right now, I am in a regretful state of mind. I would have done so much more if I had the right support system. I feel trapped, I am suffering.
Similarly, Isisa has very little support from her family and community. She too has a history of both personal as well as structural violence – ‘My family use to tell me cruel things. First, they hated me for having HIV. They saw me as an outcaste’. Isisa is determined to work towards ending the violence experienced by women, something her mother had to endure in a family she describes as dysfunctional.
The outcome of mourning for all three is highly influenced by and located in the socio-political history of our country. Nosipho, Ntombi, and Isisa are not helped to mourn by the family, the community, and more importantly by closed-off public spaces which will not acknowledge their grief and sorrow. Even the orphanage where they live does not allow for a mourning process that is not isolated from family, wider communities, and the socio-political context. The aftermath of loss takes on a great deal of significance, a powerful reminder of our interconnectedness or disconnectedness (Rosbrow, 2019). There is a fight for survival, there is a fight for who gets to grieve and who does not get to grieve. Nosipho, Ntombi, and Isisa remain dislocated and severed from spaces and places, from a collective consciousness, rendering their mourning invisible and something that does not matter.
Here we come to understand a loss of another kind for Nosipho, Ntombi and Isisa, of racial dehumanisation, where the ghosts of long-ago histories continue to follow and haunt them. The loss of the maternal object overlaps with the sorrow of multiple other historical radical losses spilling into each other, producing an oppressive subjection that prevents mourning. Ntombi and Nosipho lament the disadvantages of living in their black bodies, talking about the power and privilege that come from white subjectivities. Both express a wish to attain some dignity and humanity that can be attained by being a white child which is articulated as being ‘in a perfect world’ (Nosipho). There is also an alienation from the self – ‘like [I] have to be someone [I] am not. I feel like that is what I do here just to fit in. You have to change and be like who you are not’ (Ntombi). Ntombi expresses sadness at having to think about being a black young person.
Butler (1997, 2003) describes this subjectivity as structurally melancholic. In other words, the individual psyche is infused with socially constructed melancholia and the working through of this melancholia gets prohibited and foreclosed through oppressive discourses. While Butler writes predominantly about gender and sexuality, the discourses around HIV and race continue to shape the collective psyche in the South African context threatening the subject with psychic dissolution. For Ntombi, Nosipho and Isisa, the mourning is not only in relation to the self and their primary and other lost objects, but this mourning is also deeply located in their raced experiences, subjectivities and identities. Their experiences allow us to become aware of how the identities of these three young people have been foreclosed in a system that cannot or will not engage in the therapeutic setting with structural melancholia. For Nosipho, Ntombi, and Isisa, their very existence as black children with a political history gets severed and thrown out, annihilated, with no space for private or public recognition through which the multitude of losses can be named and mourned. The prohibition of public mourning doubles the trauma of the loss (Butler, 2003). For now, Nosipho, Ntombi, and Isisa’s pain remains hidden from public eyes, their sorrow shrouded in foreclosed and prohibited silence, forgotten and suppressed, their hate, rage, anger, aggression, and anxiety constructed as melancholia to be treated in personal therapy as an intrapsychic failure.
Yet, the anger and rage are far from being a failure and herein lies the hope of searing ourselves from the depths of our grief. Butler (2003), in her article, violence, mourning and politics, expresses an outrage at the injustice of unbearable loss and the necessity of this outrage in political presence. Although the level of violations and the experiences of vulnerabilities differ across various intersectionality, the recognition of shared vulnerability can forge connections between those who are dehumanised in various ways (Butler, 2003). By protesting actively and publicly the foreclosure of Black rage that is constitutive of Black grief, lives that cannot be mourned fully can find a space for reparative love. Canham (2017, p. 6) makes a compelling argument that one must take into account the legitimacy of the burning rage and it is in the rage that we find both the destructive and liberating power, the ‘potential of Black rage lies in the promise of the expression of self-love – a psychological declaration or gasp of self-worth and defense against oppression’. The lack of rage in Black people is the same as being complicit in the crime of systemic black denigration. For Nosipho, Ntombi, and Isisa, their trauma has a double impetus as it resides and hides in a multitude of different ways through their raced subjectivity as well as HIV diagnosis, their anger visible but turned inwards as self-approachment and rage-hidden. This rage has the potential of healing for them. It has the potential to shield the self from internalising the damaging aspects of being Black children who live with a disease of signification and a journey through a life of raced dehumanisation. Black rage protects and preserves the dignity and self-worth, mitigating the impact of racial trauma (Stoute, 2022). Black rage also contains the superego aspects of what is right and the collective unconscious store of transgenerational traumas. The rage is recruited intrapsychically to counter the devaluing attack from the outside world (Stoute, 2022). There is a protective value of nurturing and mobilising Black rage as an adaptive and dynamic process for intrapsychic success. This offers an opportunity for psychoanalytically informed therapists to step out of the complicity of keeping the grieving processes for those who are marginalised within the boundaries of melancholia only to be treated on the couch. Furthermore, here is an opportunity, a promise of space, within the practice of psychoanalytic work in South Africa and indeed globally, to engage with the invisibility or non-being of children like Nosipho, Ntombi, and Isisa. By refusing to erase the grief, anger, sorrow, and mourning from expression as a public outrage and by refusing to pathologise such public outrage, the lives and experiences of Nosipho, Ntombi, and Isisa will not be obfuscated.
Conclusion
After 30 years of democracy, the discipline of psychoanalysis in South Africa continues to neglect the critical socio-political realities of its people. This neglect renders the discipline ineffective in engaging with the materiality of healing. The more recent turn in engaging with decoloniality in psychoanalysis has offered us a way to think about training, research, and practice of the discipline in new ways that allow for the centring of Black lives in a post-colonial and post-apartheid society. In this article, I have contemplated the question of loss, grief, and mourning through the experiences of three vertically infected HIV-positive adolescents who have all experienced multiple forms of loss throughout their young lives and who are also carriers of intergenerational grief. Keeping the adolescents’ experience of the mourning process within the individual narrative renders their experience of mourning isolating in nature and in a circular process that keeps pulling them back into a state of melancholia. However, this isolating nature of grief that renders it melancholic is far from a pathology in the adolescents but forms part of the dehumanisation process of the black mourning experience. Structural melancholia cannot be foreclosed in our therapeutic encounters if we are to provide a complete healing space that takes the complexity of both raced and diseased subjectivities in Black children who also carry the burden of HIV into account. The delimitation of power in the process of healing has to be revisited in the discipline of psychoanalysis as this process will allow for a greater freedom of expression of Black grief and the accompanying rage. This process will in turn allow for the insurmountable pain to find an expression through rage in a reparative manner. Here lies the potential for radical transformative change in psychoanalytically informed research and practice that can lead to an inclusion of that part of humanity which has been severely amputated by the canon. Psychoanalytic practitioners can no longer hold themselves separate from the socio-political as this holds social asymmetries firmly in place.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.