
Abstract
Although adolescence is a critical period marked by increased vulnerability to trauma, the mechanisms underlying how adolescents cope with such experiences remain underexplored. This study is anchored in Hobfoll’s conservation of resources theory and Porges’ polyvagal theory, which together suggest that emotional intelligence and distress disclosure are critical resources for adolescents coping with trauma and investigated the interplay of distress disclosure in the relationship between emotional intelligence and trauma among secondary school adolescents. A three-wave longitudinal study was conducted with 491 adolescents enrolled in public secondary schools in Enugu State, Nigeria, selected using a two-stage cluster sampling technique. Emotional intelligence, distress disclosure, and trauma symptoms were assessed using the Trait Emotional Intelligence Scale, Distress Disclosure Index, and Trauma Symptom Checklist for Children, respectively. Confirmatory factor analysis, path analysis, and mediation analysis were employed. The results indicated significant negative relationships between emotional intelligence, distress disclosure, and adolescent trauma. Furthermore, the mediation analysis revealed that distress disclosure partially mediated the relationship between the latter two. These findings have practical implications for designing interventions and support systems that foster emotional intelligence and promote distress disclosure among Nigerian adolescents and others exposed to trauma. Future research should explore additional protective factors to enhance the robustness and generalisability of the findings.
Introduction
Adolescent trauma constitutes a significant public health concern and can profoundly impact psychological, emotional, and social development (Seedat et al., 2004; Wekerle et al., 2007). Adolescents’ inability to adapt to overwhelming life events leads to intensely negative psychological and emotional experiences (Hordvik et al., 2019). Ghazali et al. (2014) reported that over 70% of youth in their study had experienced one or more traumatic events in their lifetimes. Unfortunately, many young people do not have access to sustainable behavioural health services (Galagali & Brooks, 2020).
Moses and Villodas (2017) suggested that school engagement could play a significant protective role by boosting adolescents’ emotional adjustment. As a result of the coronavirus disease pandemic (COVID-19), schools closed, although many continued academic activities online. However, supporting young people who rely on schools for behavioural and mental health support was scarcely discussed (Phelps & Sperry, 2020). Prior studies have shown that mental health is often viewed as secondary or unrelated to academic success (Blaustein, 2013; Rawlins, 2019). Nevertheless, the pandemic imparted significant socioemotional and financial stress on several families, making it difficult for children to focus adequately on academic tasks.
Adolescents exposed to traumatic events, such as the global COVID-19 pandemic, are at heightened risk for developing a range of psychopathologies. This vulnerability is not just psychological but deeply neurophysiological, as described by van der Kolk (2014), who highlights the biochemical, physiological, and anatomical effects of trauma that can permanently alter the mind and body. Polyvagal theory, developed by Porges (2003, 2022), provides a crucial framework for understanding these changes. It posits that trauma can profoundly impact the autonomic nervous system, particularly the vagus nerve, which is crucial in regulating emotional and physiological states. This dysregulation can lead to many issues, including difficulties in emotional regulation, social communication, and feelings of safety, which are crucial in adolescent development.
The impact of COVID-19, compounded by other traumas that young people face daily, can leave lasting effects on their neurodevelopment. Trauma during adolescence, a critical period for brain maturation and identity formation, can disrupt key developmental processes (Romeo, 2017). This disruption can impede the formation of healthy relationships, academic achievement, and self-identity. Research indicates that trauma can significantly affect attachment, autonomy, interdependence, achievement, and self-actualisation in individuals (Kira, 2001). In addition, traumatic experiences are linked to higher levels of identity diffusion, which can lead to self-harming behaviours and impact self-identity (Raemen et al., 2021). In terms of academic achievement, trauma has been shown to lower academic self-efficacy and jeopardise students’ well-being, contributing to school failure and problem behaviour (Dods, 2015; Mann, 2013; Ness & Vroman, 2014). These studies underline the multifaceted impact of trauma, extending beyond immediate psychological distress to long-term neurodevelopmental consequences.
Moreover, the neurophysiological changes induced by trauma can manifest in altered stress response systems, such as the hypothalamic–pituitary–adrenal (HPA) axis, leading to increased vulnerability to mental health disorders like anxiety and depression (Lea et al., 2019). The alteration in brain structures and functions, such as the amygdala and prefrontal cortex, can also affect cognitive processes, emotional regulation, and behaviour control (Bennett & Lagopoulos, 2018). This neurobiological perspective is critical in understanding the full spectrum of trauma’s impact, necessitating interventions that address not only the psychological but also the physiological and neurodevelopmental needs of traumatised adolescents.
The relationship between emotional intelligence (EI) and trauma is important, as EI can significantly influence how individuals adjust to, cope with, and recover from traumatic experiences (Sanchez-Ruiz et al., 2021). Higher levels of EI, characterised by the ability to accurately perceive, understand, and regulate emotions in oneself and others, may be a protective factor against the detrimental effects of trauma. Adolescents with well-developed EI are better equipped to process their emotions, maintain resilience in adversity, and seek appropriate support, thereby reducing the risk of developing trauma-related psychopathologies (Llamas-Díaz et al., 2022).
COVID-19 disrupted adolescents’ routines through school closures and online transitions, leading to heightened social isolation and missed milestones (Golberstein et al., 2020). In many African settings, resource constraints and cultural stigma often amplified these challenges. Economic and health-related stress intensified anxiety, and households grappled with escalating domestic tensions. The pandemic magnified pre-existing trauma for many, especially African adolescents (Nchasi et al., 2022).
These circumstances have illuminated the need to grasp factors such as EI that bolster resilience, especially given the specific challenges often faced by African adolescents (e.g., emotional and physical conflicts, infectious diseases, and physical and sexual abuse) that could influence mental health (Dorado Barbé et al., 2021; Kuhlman et al., 2021; Ugwu et al., 2023). Understanding the interplay between EI and trauma offers insights for interventions that enhance resilience and long-term emotional well-being.
However, studies on this relationship among sub-Saharan African adolescents remain limited, particularly in challenging times. Distress disclosure (DD), one’s willingness to share their distress (Keum et al., 2023; Lepore et al., 2004), emerges as a potential mediator. Researchers have noted that DD fosters emotional processing, resilience, and stigma reduction (Kahn & Garrison, 2009). Lepore et al. (2000) highlighted its role in increasing social support, particularly when combined with higher EI. Open dialogue on distressing experiences can dismantle mental health stigma (Corrigan & Watson, 2002), fostering societal understanding and acceptance of emotional challenges. Therefore, exploring the role of DD in EI and trauma dimensions (Briere, 1996) among Nigerian adolescents during the pandemic is imperative.
EI offers adolescents a lens to better understand their emotions, and how trauma affects their well-being. It provides a therapeutic avenue for open emotional communication and DD, fostering a healing environment.
EI and adolescent trauma
The observed relationship between EI and trauma symptoms in adolescents underscores the necessity for more in-depth research on the individual dimensions of trauma. Studies have found that higher EI correlates with improved mental health outcomes, including reduced anxiety, depression, and anger, and better coping strategies and resilience among adolescents (Davis & Humphrey, 2012; Doyle et al., 2021; Foster et al., 2018; Llamas-Díaz et al., 2022). However, the relationship between EI and specific symptoms of trauma, such as dissociation and sexual concerns, remains unclear. Further research is required to develop targeted interventions that foster EI and resilience in trauma-exposed adolescents.
EI and DD
EI is associated with improved mental health and resilience, whereas DD is crucial for effective coping and social support (Lea et al., 2019; Sanchez-Ruiz et al., 2021). Research suggests that higher EI increases DD, contributing to better mental health outcomes (Davis & Humphrey, 2012; Mérida-López et al., 2018). There is limited research on African adolescents whose unique cultural, socioeconomic, and contextual features may influence EI and DD (Straatmann et al., 2019).
DD and trauma symptom
Globally, studies of adolescent DD have yielded mixed results. Some suggest that disclosing trauma can span the spectrum of traumatic symptoms and lead to benefits such as emotional relief, social support, improved coping strategies, and increased resilience (Keum et al., 2023; Kim et al., 2023). However, others highlight that some adolescents regret disclosing abuse, sometimes facing negative repercussions (Jacques-Tiura et al., 2010; Sousa et al., 2023). Few studies on African adolescents show similar associations between DD and reduced trauma symptoms. However, cultural, socioeconomic, and contextual factors may influence African adolescents’ DD and its relationship with trauma symptoms.
DD mediating the relationship between EI and adolescent trauma
This study investigated how openly discussing distress affects the relationship between EI and different dimensions of trauma symptoms in Nigerian adolescents. Research, including in Africa, suggests that adolescents with higher EI are more likely to disclose distress, contributing to reduced trauma symptoms across the Trauma Symptoms Checklist (Pérez et al., 2017; Rayburn et al., 2005).
Hypothesis 1 (H1): EI will negatively predict adolescents’ trauma.
Hypothesis 2 (H2): EI will positively predict DD.
Hypothesis 3 (H3): DD will negatively predict adolescent trauma.
Hypothesis 4 (H4): DD will mediate the relationship between EI and adolescents’ trauma.
In this study
This study examined the complex relationship between EI, DD, and trauma among African adolescents amid the COVID-19 pandemic. Recognising the neurophysiological impact of trauma (van der Kolk, 2014), our study sought to unravel how EI and DD can serve as therapeutic levers. These levers may not only help mitigate the adverse effects of trauma but also foster resilience and emotional well-being, particularly in the unique sociocultural landscape of African adolescents (Betancourt & Khan, 2008). By examining this interplay, we aim to tailor culturally attuned and responsive interventions to adolescents’ specific challenges and experiences (see Figure 1).
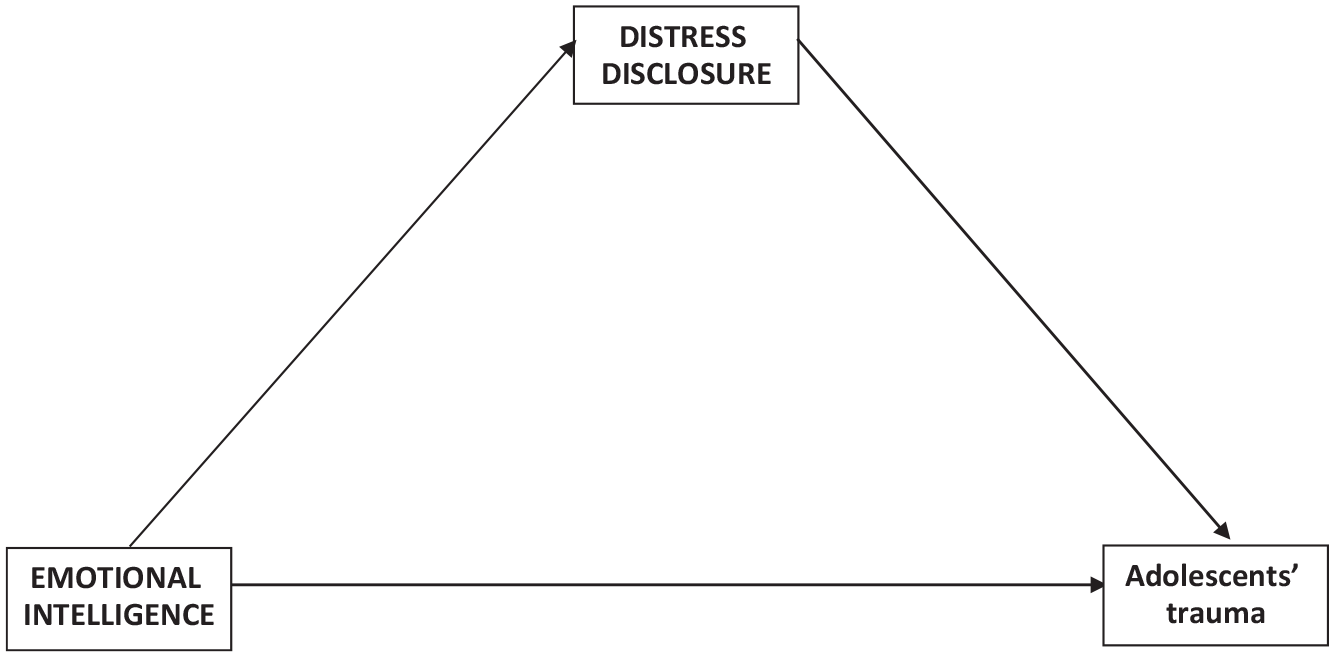
Conceptual framework.
EI, DD, and trauma are crucial in the adolescent journey, which is characterised by evolving relationships and self-discovery. The conservation of resources (COR) and polyvagal theories provide a dual theoretical framework for our exploration. Hobfoll’s (1989) COR theory posits that individuals strive to protect and retain valued resources, conceptualising EI and DD as mechanisms that adolescents employ to shield themselves from the impact of trauma. Concurrently, Porges’ social engagement theory, informed by the polyvagal theory (Porges, 2003, 2022), elucidates how a nurturing environment can activate the social engagement system, encouraging positive social interactions and a sense of safety. Traumatic events, such as rape and those experienced during COVID-19, can disrupt this system, eliciting defensive reactions – fight, flight, or immobilisation – that may manifest as psychological and physical ailments (Greenwald et al., 2023; Leahy & Iglesias, 2022).
Our study posits that well-developed EI can recalibrate the social engagement system in traumatised adolescents, enabling them to engage rather than retreat. Furthermore, when adolescents with high EI engage in DD, facilitating social connection and engagement, they are better equipped to modulate their defensive responses (Porges, 2003). Such activation of the social engagement system through EI and DD is hypothesised to enhance trauma management in adolescents.
Notably, the development of EI is not intrinsic but cultivated through social support and secure attachment experiences in early childhood (Harlow, 2021). This suggests that interventions to foster EI and DD must consider broader influential systems, including parenting styles and community support (Bronfenbrenner, 1979). In addition, there is a pressing need for teacher training that focuses on the impact of trauma on the developing psyche and promotes the development of EI within socio-relational and cultural frameworks (Jennings & Greenberg, 2009).
This study argues that enhancing EI and DD are vital in developing resilience, and inter- and intrapersonal connectedness in adolescents. Our findings can inform therapeutic interventions sensitive to the systemic and cultural dimensions influencing the adolescent experience (Masten & Obradović, 2006).
Method
Participants
This study recruited 491 Level 1 senior secondary school students from public schools in Enugu State, Eastern Nigeria. The sample, comprising 109 boys (22.2%) and 382 girls (77.8%) with a mean age of 14.03 years (SD = 1.20), was selected using a two-stage cluster sampling technique. In the first stage, classes within each school were randomly selected, and second, all students within the selected classes were invited to participate. Participants were informed of the purpose of the study and ethical approval was obtained from the relevant educational authorities (school management) and institutional review boards (RNU202218AR).
Instruments
DD
The Distress Disclosure Index (DDI), comprising 12 items developed by Kahn and Hessling (2001), was employed to evaluate the propensity to divulge personally distressing information. The DDI evaluates both disclosure actions (e.g., ‘When something unpleasant happens to me, I often look for someone to talk to’) and concealment behaviours (e.g., ‘I typically don’t discuss things that upset me’). Participants rated each statement on a scale of 1 (strongly disagree) to 5 (strongly agree). The six concealment items (2, 4, 5, 8, 9, and 10) were reverse scored. Responses were totalled, with higher scores signifying greater inclination to disclose. Given that individuals often engage in both disclosure and concealment of distress (Kahn & Hessling, 2001), the scores from the disclosure subscale and the reversed scores from the concealment subscale were combined for a more comprehensive measure of the DD process. Convergent validity of the DDI has been demonstrated through comparisons with scores of related constructs (e.g., self-concealment and ambivalence overexpression) and further reinforced in a multi-trait multi-method study (Kahn et al., 2001).
EI
The Trait Emotional Intelligence Scale by Austin et al. (2004) measures EI among adolescents using 41 items ranked on a 5-point Likert-type scale (1 = strongly disagree to 5 = strongly agree) categorised in three dimensions: regulation, utilisation, and appraisal of emotions. Austin et al. reported internal consistencies of .78, .68, and .76. A composite score was used in this study.
Adolescents’ trauma
The Trauma Symptom Checklist for Children (TSCC), developed by John Briere (1996), was used to measure adolescent trauma. It is a 54-item self-report scale designed to evaluate post-traumatic stress and related psychological symptomatology in children and adolescents aged 8–16 years who have experienced traumatic events, such as physical or sexual abuse, significant loss, natural disasters, or witnessing violence. TSCC takes approximately 15 min to complete and comprises six primary subscales: anger (ANG; e.g., ‘I want to yell and break things’), anxiety (ANX; e.g., ‘I felt afraid something bad might happen’) depression (DEP; e.g., ‘I want to hurt myself’), post-traumatic stress (PTS; e.g., ‘I have bad dreams or nightmares’), sexual concern (CS; e.g., ‘Thinking about having sex’), and dissociation (DIS; e.g., ‘My mind is empty or blank’), measured on a 4-point Likert-type scale (0 = never to 3 = almost all the time).
Procedure
A three-wave longitudinal study was conducted in public schools to collect data at 2-week intervals using three questionnaires, each focusing on a distinct variable.
A wave study or a longitudinal research design with multiple waves aims to collect data from the same group of participants at different time points (Galbraith et al., 2017), enabling the observation of changes, trends, and relationships among variables over time. The benefits of wave studies include being able to assess changes over time, establish cause-and-effect relationships, reduce bias, examine the influence of earlier experiences, and identify predictors. Wave studies are valuable in various research areas, such as psychology, sociology, economics, education, and public health.
Each student was assigned a unique identification code to label their questionnaires across all three waves, ensuring that responses could be accurately tracked and analysed over time.
In the first week, the students were given Questionnaire 1 (Trait Emotional Intelligence Scale) with clear instructions on completing it, emphasising the importance of providing honest responses. In Week 3, Questionnaire 2 (TSCC) was administered to the same group of students, after they were reminded of the study objectives and need for accurate responses. Finally, in Week 5, Questionnaire 3 (DDI) was administered to the students.
After collecting the questionnaires in all three waves, responses were reviewed for completeness and accuracy. Only complete or consistent data were included in the analysis, resulting in a final sample of 491 completed questionnaires. Data were securely stored to ensure confidentiality using unique identification codes for anonymisation. This study, employing a longitudinal design, successfully gathered in-depth data on adolescent participants from Senior Secondary 1. This approach ensures reliable insights into the targeted demographic over time. The 2-week intervals made it possible to access the students before school obligations (quizzes and examinations) commenced.
Analysis
For statistical analyses, we used IBM SPSS 28.0 and AMOS 28.0. A two-step approach was followed, testing the measurement model, path analysis, and mediation analysis (Anderson & Gerbing, 1988).
We examined the measurement model’s factorial structure and conducted confirmatory factor analysis (CFA) using AMOS. First, model fit was evaluated based on four indices (standardised root mean square residual [SRMR], root mean square error of approximation [RMSEA], comparative fit index [CFI], and Tucker–Lewis index [TLI]). A good fit was defined as SRMR and RMSEA below .07 and CFI and TLI above .90. Second, the structural model was used to confirm the proposed hypotheses. Control variables (gender and age) were based on previous findings that highlighted their significant relationship with trauma (Adewuya & Ologun, 2006; Coles & Cage, 2022; Straatmann et al., 2019; Ugwu et al., 2019).
Results
Measurement model
Validity and reliability were established by examining internal consistency, and discriminant and convergent validity (Table 1). Cronbach’s alphas and composite reliabilities exceeded .7, indicating strong reliability (Hair et al., 2009). Convergent validity was confirmed as factor loadings surpassed .5 (Fornell & Larcker, 1981) and average variance extracted (AVEs) exceeded maximum shared variance (MSV) values (Sarstedt et al., 2011). Discriminant validity was verified by comparing construct correlations with the square root of AVEs (Hair et al., 2009) and the heterotrait-monotrait (HTMT) ratios being below .85 (Table 2; Kline, 2011).
Reliability and validity of constructs.
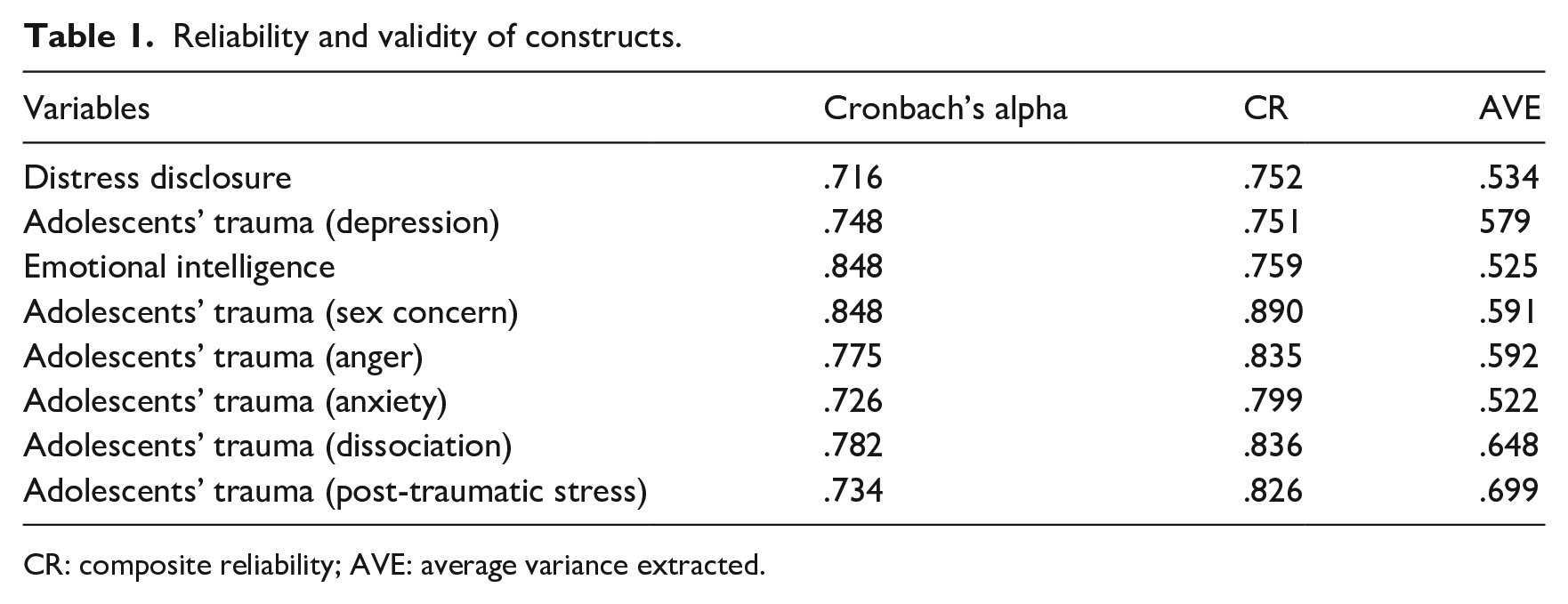
CR: composite reliability; AVE: average variance extracted.
Correlation matrix.
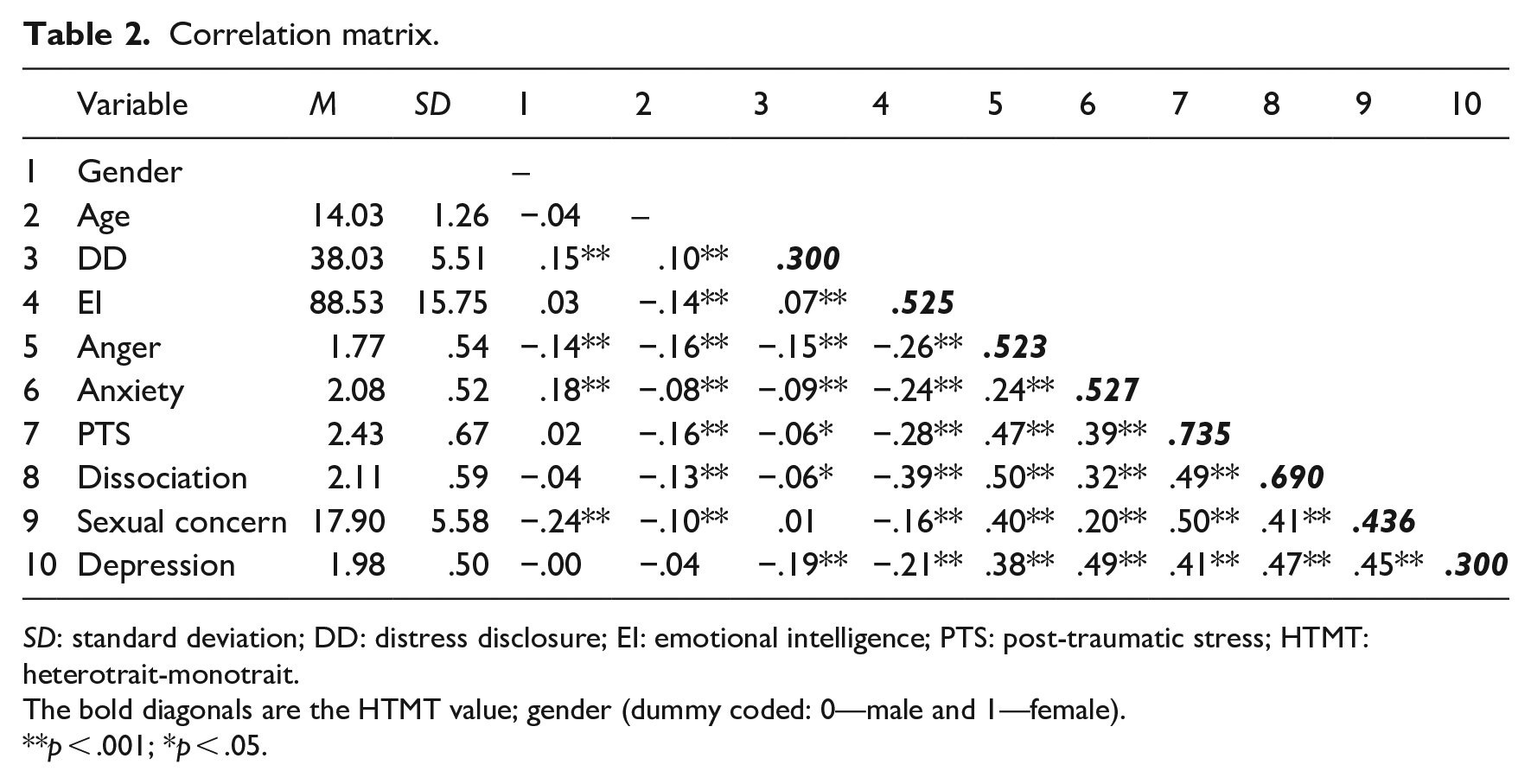
SD: standard deviation; DD: distress disclosure; EI: emotional intelligence; PTS: post-traumatic stress; HTMT: heterotrait-monotrait.
The bold diagonals are the HTMT value; gender (dummy coded: 0—male and 1—female).
p < .001; *p < .05.
Structural model
Using AMOS Version 28, CFA was performed to verify the distinctiveness of the model’s variables. Three models were tested, and the four-factor model showed the best fit (SRMR = .005, CFI = .999, TLI = .994, RMSEA = .018) (Table 3). With established validity, hypothesis testing could proceed.
CFA model fit indices.
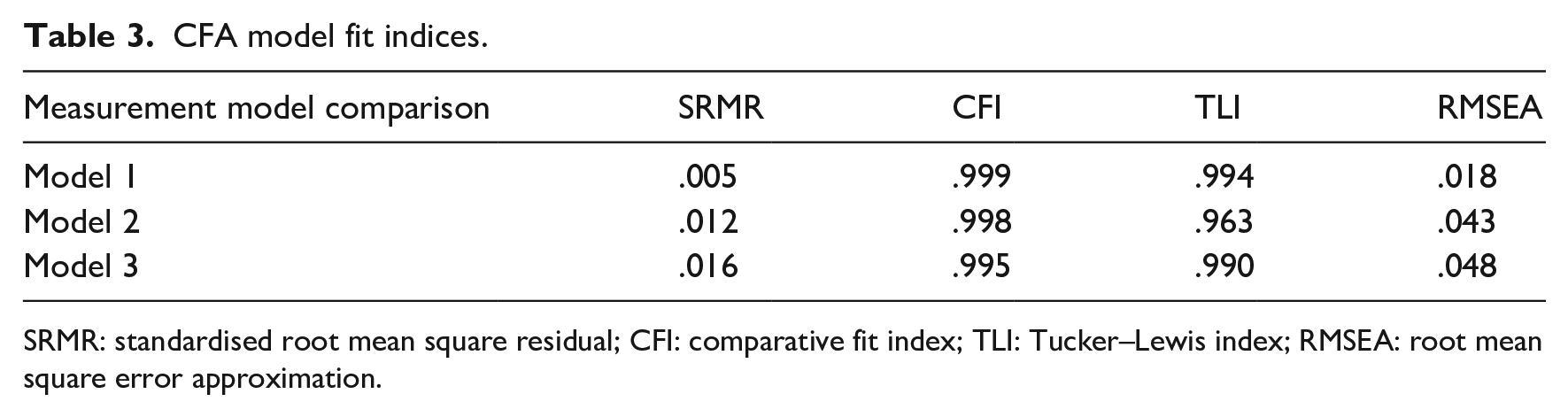
SRMR: standardised root mean square residual; CFI: comparative fit index; TLI: Tucker–Lewis index; RMSEA: root mean square error approximation.
Table 2 presents descriptive statistics and a correlation matrix for the variables. Among the demographic variables, gender (male) was significantly related to anger, anxiety, sexual concerns, and depression but not PTS and dissociation. Males were more positively related to DD than females. Sex was not found to be related to EI.
Age was negatively related to anger, anxiety, PTS, dissociation, and sexual concern but not depression.
DD was negatively related to all dimensions of adolescent trauma except sexual concern. EI was negatively related to all dimensions of adolescent trauma and positively related to DD.
We utilised structured equation modelling path analysis with a 95% bias-corrected bootstrap confidence interval, taking 5000 bootstrap samples to assess both direct and indirect effects. Mediation is considered present if the indirect effects’ 95% confidence interval does not contain zero. Hayes (2018) suggests that the bootstrapping method’s process models offer a more accurate representation of mediation relationships than the Baron and Kenny (1986) and Sobel tests.
The results indicate a significant negative relationship between EI and DD on adolescent trauma (anger, anxiety, post-traumatic stress, dissociation, depression, and sexual concern; Figure 2). This finding supports the first hypothesis. EI was significantly related to DD, supporting the second hypothesis. In addition, DD showed a significant negative relationship with adolescent trauma, supporting the third hypothesis.
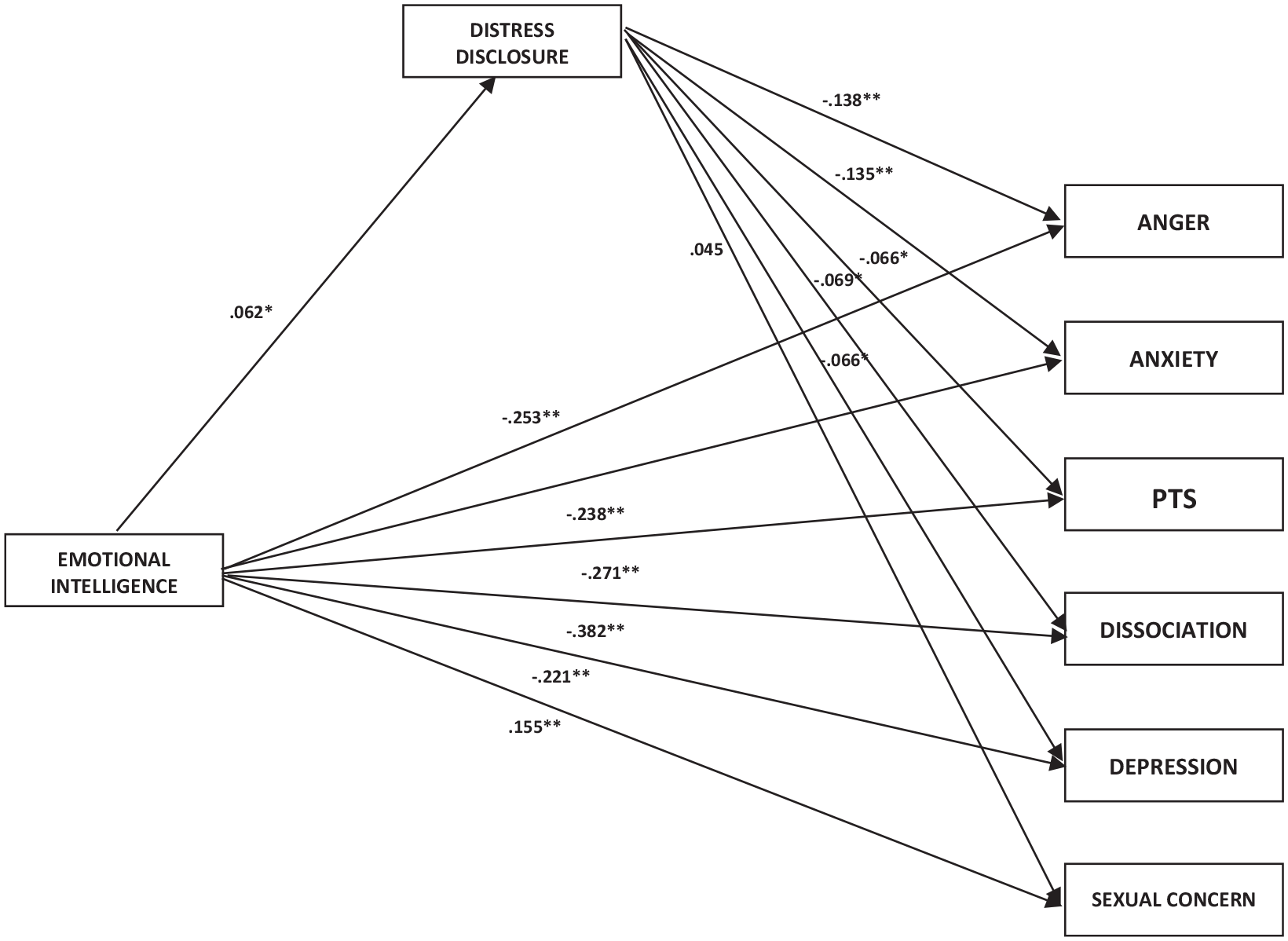
A path analysis of the relationship between emotional intelligence, distress disclosure, and adolescents’ trauma.
Table 4 presents the indirect effects of DD, indicating that the relationship between EI and adolescent trauma is negatively mediated through DD, supporting the fourth hypothesis (partial mediation).
Test of indirect effect.
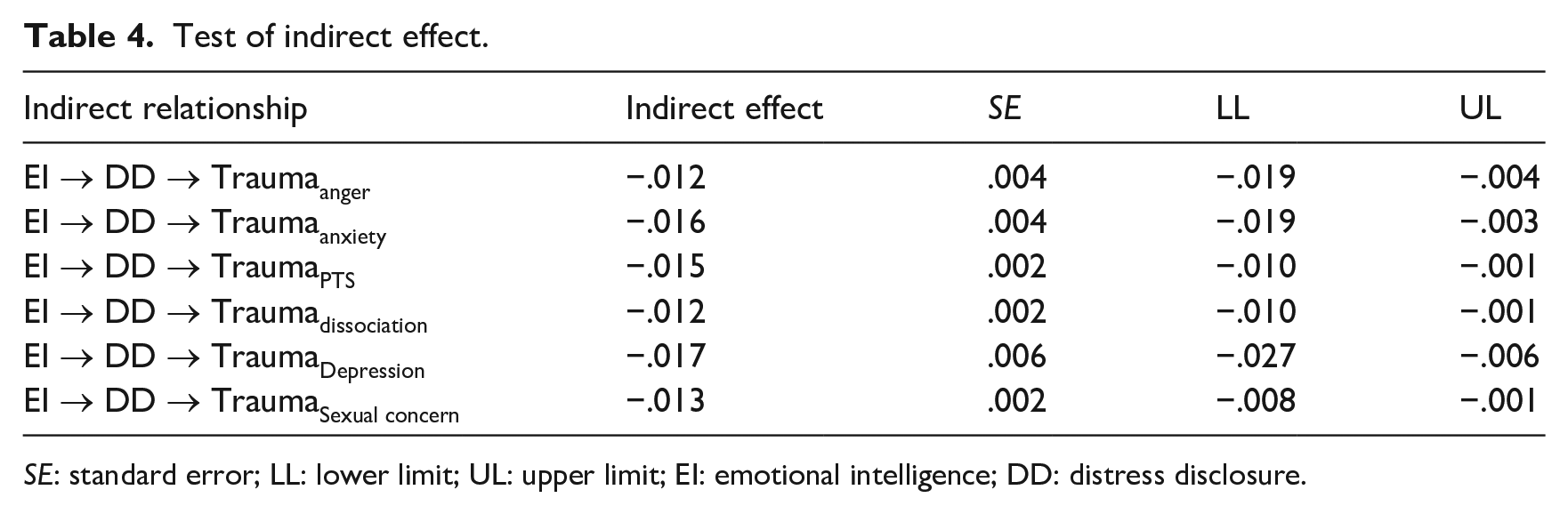
SE: standard error; LL: lower limit; UL: upper limit; EI: emotional intelligence; DD: distress disclosure.
Discussion
This study examined the interplay of DD in the relationship between EI and trauma among Nigerian adolescents in secondary school. Central to this examination were the COR and polyvagal theories, which illuminate the dynamics at play, particularly when viewed through the unique cultural, socioeconomic, and contextual lens of African adolescents.
The results validated our first hypothesis, showing that EI has a notable negative relationship with adolescent trauma. Hobfoll’s (1989) COR theory explains this, suggesting that EI is a valued resource that adolescents use to navigate traumatic encounters. The cultural emphasis on communal living and support in African societies implies that EI, as a tool for understanding and managing emotions, plays a pivotal role in promoting harmonious interpersonal relationships. Furthermore, given the socioeconomic challenges faced by many African adolescents, regulating emotions and maintaining positive relationships becomes critical to their mental and emotional well-being.
The results highlight a significant positive association between EI and DD. DD as a personal resource is particularly relevant in African contexts, wherein oral traditions and storytelling are deeply rooted cultural practices. Sharing experiences, pain, and challenges is not only a way of seeking support but also a means of preserving narratives and drawing strength from shared histories. However, with limited awareness and access to formal mental health services in regions such as Nigeria, the significance of alternative coping mechanisms, such as DD, is heightened. The socioeconomic limitations faced by many adolescents in these regions further emphasise this need.
In line with the third hypothesis, DD demonstrated a significant negative relationship with adolescent trauma. Polyvagal theory, when contextualised within the African setting, suggests that adolescents with heightened EI are more inclined to seek safe social affiliations, which can be achieved through DD. Given the communal nature of African societies, seeking and providing social support are culturally ingrained coping mechanisms. When faced with challenges, including trauma, the community often rallies around its members, offering emotional and tangible support.
With respect to gender, the results indicated that boys were more associated with most trauma domains. In Africa, societal and cultural norms often emphasise fortitude and resilience among men, potentially leading to underreported or unaddressed trauma (Singletary, 2020). In addition, male adolescents may be more exposed to societal conflicts or pressures, accentuating their risk (Amoateng et al., 2014). The stigma associated with mental health support, especially prevalent in African men across cultures, can further compound traumatic effects (Musisi & Kinyanda, 2020).
Finally, the findings indicate that DD partially mediates EI and adolescent trauma, shedding light on the intricate interplay of the three in Nigerian adolescents, especially during the challenges posed by COVID-19. The pandemic further amplified many African communities’ socioeconomic challenges, making this study’s findings even more relevant. Through the combined insights of COR and polyvagal theories, we can better comprehend the resilience mechanisms and coping strategies employed by adolescents in the face of adversity, which are deeply influenced by their environment’s cultural, socioeconomic, and contextual peculiarities.
Our findings on EI resonate with established knowledge, underlining its role in promoting mental well-being, fostering sound interpersonal relationships, and enabling adaptive coping. The importance of social connectivity and support, especially post-trauma, further emphasises the socio-relational and cultural roots of EI.
Practical implication
This study will inform mental health practitioners, educators, and policymakers working with Nigerian adolescents affected by trauma. Emphasising the critical need for interventions aimed at adolescents endeavouring to bolster their EI through the development of ventral vagal connections, as seen in instances of DD, is essential. Enhanced EI is often a product of robust social support and secure attachment experiences during early childhood, which empowers individuals to seek support and share their distress with others. Recognising the complex relationship between trauma, DD, and EI is essential to designing effective interventions. There exists an urgent requirement for education programmes that are informed by an understanding of trauma, specifically tailored for professionals who work closely with adolescents. Establishing environments in educational and community settings that promote open, judgement-free communication is vital. Such environments are instrumental in cultivating a culture where adolescents feel safe and encouraged to share their experiences openly.
EI helps adolescents develop greater awareness of their emotions and the impact of trauma on their mental well-being. This self-awareness allows them to recognise the need for healing and support relevant to the healing process. DD allows adolescents to communicate their emotional struggles openly and honestly. By disclosing their distress, they not only reduce their emotional burden but also enable others to better understand their experiences, which can foster empathy and support. When EI is combined with DD, it facilitates greater empathy and validation. Emotionally intelligent individuals are better equipped to respond compassionately to DDs, creating a safe and nonjudgmental environment for adolescents to share their trauma experiences. These findings also confirm the importance of social connectivity in establishing a sense of safety and support when adolescents experience trauma. EI is developed within a relational space based on secure attachment and needs to be considered from a socio-relational and cultural point of view. Finally, policies that resonate with the unique challenges faced by Nigerian adolescents will ensure that their needs are at the forefront. By adopting these multifaceted approaches, we can collaboratively shepherd Nigerian adolescents towards trauma recovery when required.
Limitations and recommendations
This study has several limitations that should be addressed in future research. The sample, drawn exclusively from secondary school students in Enugu State, Eastern Nigeria, may not reflect the experiences of adolescents from other regions or cultures, potentially limiting the generalisability of the findings. A range of factors prevalent in Nigeria, including socio-political instability, economic challenges, and cultural pressures, uniquely shapes the trauma experienced by this group. These are compounded by the global impact of the COVID-19 pandemic, creating a complex trauma context that is distinct from more stable or resource-rich environments. This specificity in trauma experience, while highlighting the importance of the study, also limits the generalisability of the findings to other settings.
In addition, although self-report measures provide valuable insights, they are subject to biases. Incorporating qualitative methods and innovative approaches such as expressive arts and photo-voice could yield richer, more nuanced data. The longitudinal design, with its 2-week intervals, captures only a snapshot of the dynamic interplay between EI, DD, and trauma and may not reflect long-term outcomes. Extending the duration and intervals between assessments would allow for a more comprehensive understanding. Moreover, the study’s focus on EI and DD leaves other potential protective factors and moderators unexplored. Future research should investigate a broader range of coping strategies and resilience factors for a more holistic view of adolescent trauma recovery.
Conclusion
The findings of this study highlight the complex interplay between EI, DD, and trauma among Nigerian adolescents during the COVID-19 pandemic. They highlight the protective roles of EI and DD in buffering the adverse effects of trauma. They indicate a clear need for culturally sensitive interventions tailored to Nigerian adolescents that incorporate mixed-method approaches to engage adolescents in ways that resonate with their experiences and cultural expressions. High EI is instrumental in enabling individuals to share distressing experiences openly, which fosters coping through emotional processing, social support, and cathartic release. This study advocates integrating EI training into educational curricula, enhancing social support systems, and providing culturally competent care. By establishing a foundation for future research, this study emphasises the critical importance of nurturing EI and DD as strategies for bolstering resilience in traumatised adolescents.
Footnotes
Acknowledgements
The authors wish to acknowledge all the support of Renaissance University, Ugbawka, Enugu State, Nigeria during this study.
Author contributions
The first author (LEU) contributed to the conception and design of the study. LEU helped develop the study measures and data collection. LEU and the fourth author (M-CCO) contributed to the study delivery and interpretation of the data. LEU wrote the manuscript draft, and LEU, the third author, M-CCO, and the second author revised the draft. All authors read the final manuscript and approved its submission.
Data availability
The data sets generated and analysed during the current study are not publicly available due to agreement with the participants and are only available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval and consent to participate
The study has been approved by the Renaissance Faculty Internal Review Board (RNU202218AR). The authors affirm that this study was conducted following the ethical standards of the responsible committee on human experimentation (institutional and national) and the Helsinki Declaration of 1975, as revised in 2013. Informed consent was obtained from all the participants.