
Abstract
Chronic fatigue is a distressing symptom for endometriosis patients but is not widely investigated in the literature. Our aim was to explore patients’ lived experiences of chronic fatigue and how they make meaning of it. We analysed a subset of data from seven severely fatigued endometriosis patients, drawn from a broader qualitative study in South Africa, using an interpretive phenomenological analysis. Three superordinate themes and eight subordinate themes were developed. The three superordinate themes were powerlessness, which was a core aspect of the chronic fatigue experience among participants; struggle and anguish, as their lives had become a daily struggle resulting in feelings of despair and anger; and otherness, as they felt different from their peers due to the fatigue. The findings demonstrate the far-reaching effects that chronic fatigue has in the lives of endometriosis patients, including on their self-perception, and highlights the critical need for fatigue management strategies within treatment protocols.
Keywords
Endometriosis is a complex, poorly understood disease that is estimated to affect between 2% and 10% of women globally (Dunselman et al., 2014). It is defined as the presence of endometrial-like tissue in locations outside the uterus, which results in the development of adhesions, lesions, scar tissue, and cysts (Burney & Giudice, 2012). Common disease symptoms include heavy menstrual bleeding, chronic pelvic pain, and infertility (Dunselman et al., 2014). Endometriosis is a chronic, progressive disease with no known cure and limited treatment options involving surgery or hormonal pharmacotherapy (Bedaiwy et al., 2017). The exact prevalence rates for endometriosis in South Africa are unknown, as are those for sub-Saharan Africa (Menakaya, 2015; Roomaney & Kagee, 2018).
One of the symptoms often overlooked in both the literature and treatment protocols is chronic fatigue, which is significantly more prevalent among endometriosis patients than the general female population (Ramin-Wright et al., 2018). The association between fatigue and endometriosis has been found to persist even after controlling for possible confounding factors such as pain, insomnia, and depression (Ramin-Wright et al., 2018). Chronic fatigue profoundly affects patients’ lives and its impact on their physical, emotional, and psychological wellbeing has been documented in various studies (Álvarez-Salvago et al., 2020; DiBenedetti et al., 2020; Mundo-López et al., 2020). Fatigued patients have higher rates of work absenteeism and lower work ability (Hansen et al., 2013; Soliman et al., 2021). Fatigue also impacts patients’ social activities and relationships, resulting in less time spent with family and a reduction in intimacy with partners (Cole et al., 2020; DiBenedetti et al., 2020). Similar findings have been reported for South African patients (Roomaney & Kagee, 2018).
The impact of fatigue in endometriosis is similar to that reported by people living with other illnesses for which chronic fatigue is a symptom (Bootsma et al., 2020; Hewlett et al., 2005). Endometriosis patients find chronic fatigue distressing; its impact on quality of life and productivity places a great burden on them and their families (DiBenedetti et al., 2020; Mundo-López et al., 2020; Ramin-Wright et al., 2018). However, despite its incapacitating nature, there is a dearth of literature on its pathophysiology and treatment (Ramin-Wright et al., 2018). While it is likely that its aetiology is multidimensional, nonpharmacologic interventions that have been used to treat persistent fatigue in other chronic diseases with some success have yet to be developed for this patient population (Hewlett et al., 2011; van den Akker et al., 2016; Wu et al., 2019). A critical first step in developing such interventions is understanding how endometriosis patients experience and conceptualise fatigue.
To this end, the authors conducted a literature search across various databases (EBSCOhost, ProQuest, PubMed, and ScienceDirect), which revealed no studies focused on these phenomena. To begin to address this gap, the researchers conducted a qualitative study among endometriosis patients to explore their experiences of chronic fatigue. Patients in the study reported a range of functional limitations, highly personalized coping mechanisms, and a lack of available treatment strategies from health care practitioners (Sibande & Roomaney, 2022). For this article, the authors analysed a subset of these data using interpretive phenomenological analysis (IPA) to explore patients’ lived experiences of chronic fatigue and how they made meaning of it.
Methods
Participants
The study formed part of a broader project conceptualised by the third and fourth authors (MEL and RR, respectively) and was undertaken by the second author (ZNS ) under their guidance, while the first author (AS) joined the project after the data had been collected. ZNS used purposive sampling to recruit 25 endometriosis patients who experienced severe fatigue via social media and the Endometriosis clinic at Tygerberg Hospital in Cape Town, South Africa. ZNS visited the clinic weekly and posted a study advert on the Facebook page of two local support groups in order to recruit participants. Eligibility criteria included the following. Participants had to be 18 years or older, formally diagnosed by a gynaecologist, and experiencing fatigue that impaired daily functioning. Fatigue severity was measured by asking participants to rate their fatigue on a scale of 1 to 10, with 1 indicating almost no fatigue and 10 indicating very severe fatigue. Only patients with a rating of 6 or higher were included in the study. This cut-off point was used to distinguish moderate to severe fatigue and was determined based on informal feedback provided by lived experience advisors. Eligible, interested patients provided written informed consent and were interviewed face-to-face. The participants ranged in age from 22 to 45 years (median age: 36 years), with a median duration since diagnosis of 4 years (range: 6 months–21 years).
Instruments
The second, third, and fourth authors developed a semi-structured interview guide to explore the fatigue experiences of participants, including questions about how they described fatigue, the impact it had on their lives, the strategies they employed to manage it, and the support they received from others. ZNS conducted the interviews in English (92%) and Afrikaans (8%) based on respondent preference.
Ethical considerations
Ethical approval for this study was provided by the Health Research Ethics Committee (HREC) at Stellenbosch University as well as the Western Cape Department of Health. Interviews lasted between 30 and 76 min (mean: 40 min). Participants who experienced any distress as a result of the interview could contact the researchers to access counselling services that were made available. The interviews were transcribed verbatim, and transcripts were checked against the audio recordings for accuracy, after which they were loaded into Atlas.ti version 8 for analysis.
Data analysis
Given the exploratory nature of the study, the authors initially analysed the data for breadth to gain better insight into this understudied phenomenon. The full sample of transcripts was analysed utilizing a data-driven, deductive thematic analysis (TA) to focus on the more pragmatic elements of the data (Braun et al., 2015), for which the results are presented elsewhere (Sibande & Roomaney, 2022). While conducting the TA, the authors noted some particularly rich interviews that contained novel insights and interesting self-reflections regarding the experience of chronic fatigue, for which they kept a list of transcripts, and which prompted a subsequent analysis to assess latent meanings within the data.
AS utilized IPA for the subsequent analysis given its wide use in health psychology to explore how participants make sense of their own experiences (Brocki & Wearden, 2006). IPA’s theoretical underpinnings are grounded in phenomenology and hermeneutics, focusing on the meanings that individuals ascribe to events, which are accessible through interpretative activity (Biggerstaff & Thompson, 2008). IPA is a useful methodology for analysing ambiguous, complex, or emotionally laden topics, and involves a two-stage interpretative process, or double hermeneutic, whereby the researcher attempts to make sense of the participants attempting to make sense of their worlds (Smith & Osborn, 2015). While the approach to the exploratory qualitative study was not informed by IPA from the outset, qualitative data tend to be complex, enabling the use of a range of analytical approaches to unpack different possible meanings within it, or what Clark et al. (2015) refer to as analytical pluralism. The breadth and depth of experience shared by study participants using the semi-structured interview schedule meant that the data were suitable for IPA. Furthermore, the exploratory study was phenomenological in that it sought to understand and describe the lived experiences of chronically fatigued endometriosis patients to gain deeper insight into how they understand these experiences.
Of the 11 transcripts containing particularly rich data, a smaller, homogeneous group was identified for the IPA, consisting of seven female patients who were over the age of 25 years, had undergone at least one surgery (and would therefore have expected some relief from the symptoms), and had an advanced stage of the disease.
In undertaking the IPA, AS followed the process outlined by Smith and Osborn (2003), which involved reading the first transcript multiple times and noting interesting or significant aspects in the margin. These were converted into emergent themes at a higher level of abstraction during subsequent readings of the transcript. Connections were subsequently sought between these themes, resulting in a cluster of superordinate and subordinate themes. The same procedure was applied when analysing the remaining transcripts, after which AS, MEL, and RR reviewed the themes to explore convergences and divergences in the data. This informed the development of a master table of superordinate themes, ensuring that they formed a good representation of the transcripts.
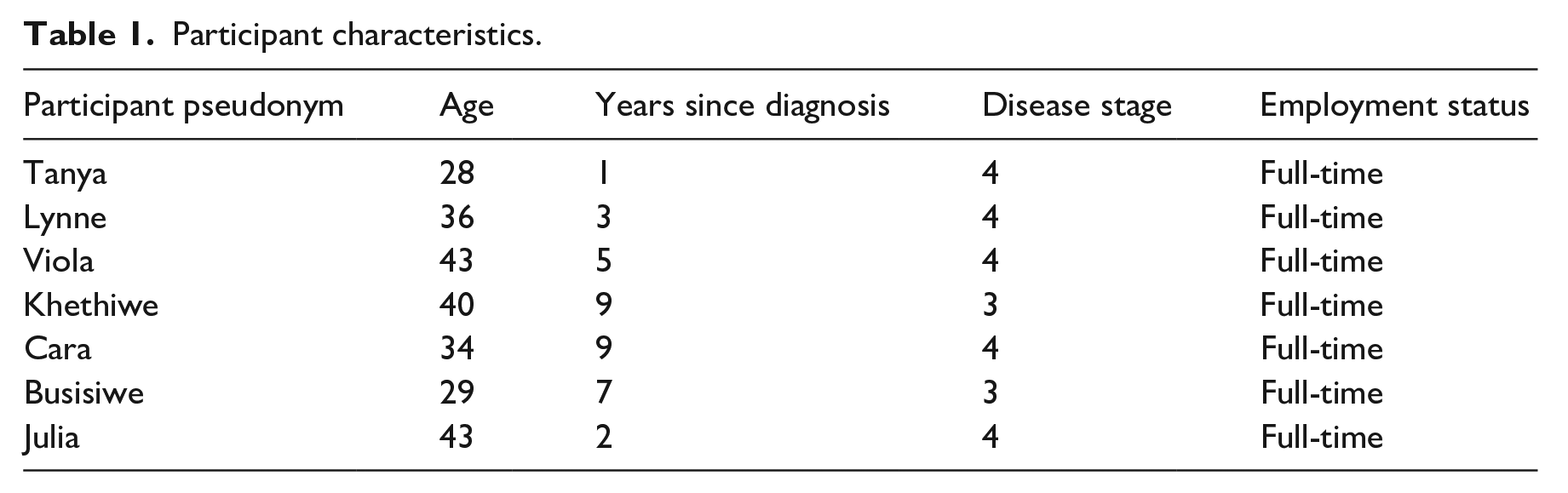
The participants whose transcripts were selected for the analysis using IPA ranged in age from 28 to 43 years and were all employed on a full-time basis (Table 1). Three of the participants were married, three were single, and one was separated. One participant lived alone, four lived with other adults, and two lived with children. Four participants had graduated from university. The names of participants have been changed to protect their identities.
Participant characteristics.
Several strategies were employed to enhance trustworthiness in the data collection and analysis process. The interviews were audio-recorded to ensure that the accuracy of the data contained in the transcripts could be verified. ZNS and RR met on a weekly basis throughout the data collection period to reflect on the data and how future interviews could be improved. Upon joining the project, AS listened to the recordings while reading through the transcripts to ensure that they accurately reflected the discussions. Finally, while undertaking the subsequent analysis, AS shared and discussed the codes with ML and RR who were very familiar with the data.
Results
Three superordinate themes and eight subordinate themes were developed. The three superordinate themes were powerlessness, which was a core aspect of the chronic fatigue experience among participants; struggle and anguish, as their lives had become a daily struggle resulting in feelings of despair and anger; and otherness as they felt different from their peers due to the fatigue.
Powerlessness
The enemy within
Participants described chronic fatigue as a type of ghost that had taken control of their bodies:
It’s like having this monster in your life. It’s like having a ghost. It’s like battling with this ghost that refuses to go away, that does what it wants to do, whenever, however, it wants to do it. Nothing you say, nothing you do, will take this thing away. This monster is saying, ‘when I’m here in your life you just obey . . . you know you just bow down to me and say do what you want to do, allow me, because of regardless if you fight me or not I am here’ . . . (Busisiwe) I don’t know what word I can call it. Evil. I don’t know. Because it’s like such cruelty man. (Tanya)
Busisiwe and Tanya both externalize fatigue as something that is happening to them, over which they have no control. The use of words like ‘ghost’, ‘monster’, and ‘evil’ denote the presence of an external being with malevolent intentions that haunts or torments the women. Tanya’s use of the word ‘cruelty’ suggests fatigue as something sinister that aims to create suffering or punishment. Furthermore, ghosts or monsters are often described as being seen by some people but not others, which implies that fatigue is hidden or invisible to those not affected by it. In the broader qualitative study, many participants spoke about the invisibility of fatigue because they appeared healthy on the outside. In addition, participants described not being able to fight against the fatigue, which has power over them, indicating their vulnerability and their sense of lacking control over their bodies. The repeated use of words like ‘fight’ and ‘battle’ by participants liken having fatigue to being in a war zone, where the women are fighting against the odds.
Being crushed
Most participants also described fatigue as a feeling of physical heaviness, where they felt as though they were being weighed down or crushed. Julia and Khethiwe described a sense of heaviness in their heads when trying to get out of bed in the morning, while Violet likened fatigue to being crushed by an elephant:
I, sometimes in the mornings, feel as if there is a stone in my head. I cannot get up, my head doesn’t want to lift. (Julia) It becomes so much of a struggle to get out of bed. It’s like there’s a magnet between your head and your pillow. (Khethiwe) It feels like you have this elephant sitting on your chest, and it is just pressing you down all the time, so you feel weighed down. Your body feels heavy. (Violet)
The likening of fatigue to a feeling of physical heaviness indicates that the participants experience it as being overpowering and that they do not have the strength to resist it. They felt trapped by the fatigue, which is difficult to ‘carry’ or ‘lift’ and is the opposite to feeling light or free. The women reported having to expend great effort to overcome this weight, which left them feeling weaker, and also required them to expend immense effort to carry out mundane tasks, with which they struggled. This again points to participants’ sense of powerlessness and lack of control that stems from living with chronic fatigue.
Lifelessness
The participants also compared fatigue to being lifeless. In her description, Tanya refers to her blood, which symbolizes vitality and life, draining out of her body, leaving her feeling lifeless and unable to do anything. Some of the participants also referred to death, saying that they were ‘dead tired’ or felt ‘dead inside’. Busisiwe again refers to an external malevolent being, but this time it is one that ‘steals’ her soul. The experience of being alive but feeling ‘dead’ or ‘soulless’ indicates that the participants feel as though they are lacking their inner essence and that they are just hollow shells of themselves. There is no ‘fuel’ left in the tank, with all of it having been taken or having seeped out. There is a sense of doom, with fatigue taking away their vitality and leaving them with nothing:
I just sit and do nothing. At work also, I’ll just sit like this. Just to recuperate, sort of. That’s all I do, there’s nothing else I can do. I usually also tell my mom it feels like all the blood just drained out of my body. (Tanya) But it does, it does kind of hold you back in your life. It’s like somebody robbing you of your soul and expecting you to still live, you know. (Busisiwe)
Struggle and anguish
An everyday struggle
Cara and Khethiwe both reference the immense struggle they face each day in performing regular activities as a result of the fatigue. They were overwhelmed with a sense of exhaustion, even waking up feeling this way in the morning. They experienced an extreme need to sleep or rest but never actually felt rested. The participants reported that they had to ‘push’ themselves to do regular things like get out of bed, which indicates a need for force to be used. The fatigue made it difficult for them to do things, which in turn became things that they did not want to do, resulting in a need for them to go against their natural inclination. There was much internal struggle as participants put up a fight against themselves to get through a regular day and they felt as though life was simply too much to cope with:
When I wake up it’s like a struggle because you wake up and you are like ‘has the alarm already gone off?’ And you are so tired, you don’t want to really get out of bed, but you must push yourself because you need to work. And so I normally feel drained, like someone that has been out all night, you feel like that tired, tired feeling. I’m just permanently tired. It’s like you waking up feeling like you’ve had a hard day already. (Cara) Everything becomes so much of a struggle. Walking from here, going upstairs. They’ll tell you they know when I’m coming up because I’ll be panting and huffing. It’s very difficult. It’s very difficult because the simplest things I’m telling you, standing up from here to there, it can be quite a mission, which it shouldn’t be. These are the simplest things in life. (Khethiwe)
Frustrated outrage
The constant struggle participants were engaged in to ‘get through the day’ resulted in much anger and frustration for them:
You get frustrated in many ways, especially if you’ve got a lot of responsibilities that await you and now you can’t do anything again for another day. You know I have given up when it comes to endometriosis. At some point I felt very angry. (Busisiwe) It is very frustrating, because I want to do more but my body is not allowing me to. (Julia)
Busisiwe and Julia both expressed frustration and anger at the fact that they could not do what they needed or wanted to do as a result of the fatigue. They were incapacitated and felt that they had no control over their lives. Julia said that her body ‘will not allow’ her to do more, which again points to a feeling of not having control or being powerless and trapped. The participants directed this anger towards their own bodies, expressing a sense of betrayal in that their bodies have ‘let them down’. They were disappointed as a result, which also created a sense of failure. In the face of this failure, participants have become angry and resentful, which has led some of them to resign or surrender themselves to the disease as they do not believe it will ever get any better.
Despair
The participants expressed much anguish and sadness as a result of having to live with chronic fatigue. Many participants were visibly distressed during the interviews and cried or became emotional when talking about how it had impacted their lives. They also talked about pervasive sadness:
A lot of times I feel depressed because of how I feel. (Lynne) Waking up tired is not nice. It’s like ‘oh my word another day, the day come so quick, why am I so tired’, like you question yourself. And sometimes you are just so tired and you don’t enjoy things as you used to. It’s like life hasn’t seemed as enjoyable as it used to be. (Cara)
Both Khethiwe and Lynne refer to feelings of depression that emanate from being fatigued. Cara further describes how she had lost any sense of enjoyment in her life as a result of the fatigue. In the quote Cara seemed exasperated about how quickly the days passed and yet how she felt tired on each one of them. The constant fatigue was overwhelming and created much despair among participants, who felt hopeless and doomed to feel this way for the rest of their lives. They also struggled with sadness from not being able to live their lives the way that they want to.
Otherness
Abnormal
The participants described how their energy levels differed from those of others:
I don’t have the energy that you have. I’m not normal as you are, as much as I try to be as functional as everybody in the office or at home does. I’m not normal, I am not like you. (Busisiwe) It’s actually sad, because, why? It’s like you question yourself, ‘why can’t I be like other people? Why can’t I also have that old energy level like other women?’ (Cara)
Both Cara and Busisiwe describe feeling different from other people, who were able to go about their business every day, while they struggled due to the ever-present fatigue, which made it difficult for them to function. This resulted in feelings of abnormality and otherness, where participants felt as though they are separate from the people around them. The participants reported feeling isolated and alone and some expressed feelings of jealousy about how other people had sufficient energy to lead ‘normal’ lives. Participants also felt confused about why they were different and expressed a sense of victimhood as a result, feeling as though they have been singled out in some way for suffering. The participants felt like they were being denied a normal life and did not understand why they had to suffer in this way. They felt that it is unfair and expressed resentment towards being different from others. There was also a sense of loss of normality and functionality as a result of the fatigue, which made participants feel inadequate and less worthy than their peers. The participants problematised their bodies and saw themselves as outsiders as a result of the fatigue.
Old before their time
The participants also referred to feeling aged despite being young. Tanya described how living with persistent fatigue made her feel as though she was much older than her biological age, making her feel old prematurely. The participants spoke about how they ‘should’ feel, namely young and energetic and able to do what ‘young people do’. They felt cheated at lacking youthful energy and vibrance and felt that their bodies had failed to live up to their expectations. There was a sense of inadequacy when comparing themselves to peers their age, referencing how higher energy levels seemed to come naturally to others, about which they felt resentful and disappointed. The participants also expressed nostalgia for the time in their lives before they started struggling with fatigue:
Everything is basically frustrating because I’m like, I’m not even 30 yet, why must I be so tired? And I feel like an old person that just doesn’t have energy levels, and I just don’t feel like doing anything. (Tanya) It makes me feel sad, because then you now sit with ‘Lord, why me?’ type of stuff, because everybody’s young, everybody’s doing what they’re supposed to. (Tanya)
Discussion
The current study explored how women living with endometriosis experience chronic fatigue using IPA, focused on a subset of data from seven participants who took part in a broader qualitative study. The participants in this study described the profound impact that chronic fatigue has on their sense of self. The fatigue experience had become such an integral part of their lives that it forms part of their self-identity and the way that they perceive their lives. This finding is consistent with the literature on chronic illness more generally (Horky et al., 2017; Nettleton, 2021; Oris et al., 2018).
Bury’s (1982) influential concept of chronic illness as a ‘biographical disruption’ is useful for understanding how illness can result in changes to a patient’s identity and consists of three key aspects. First, a patient’s attention is drawn to bodily states that usually go unnoticed, thereby disrupting their ‘taken-for-granted’ assumptions and behaviours. This is followed by more profound disruptions in the way that patients perceive themselves, or a loss of self that forces them to rethink their personal identity, followed by the disruption that ensues in having to cope with their altered situation and reassess their lives (Bury, 1982). In the current study, patients struggled to perform tasks that they used to take for granted and they were so used to feeling fatigued all the time that they struggled to define who they were outside of it, which is consistent with this concept.
The functional limitations that the participants described are intertwined with a sense of uncertainty because their bodies often do not meet their expectations. Carel (2016) argues that individuals care more about what they can do with their bodies than about the body itself and therefore place great value in taking part in activities. Good health brings a sense of control and being able to predict one’s bodily experiences, which creates a sense of certainty. Thus, chronic illness is associated with a sense of uncertainty and has been noted in studies among people living with multiple sclerosis (Alschuler & Beier, 2015; van der Meide et al., 2018). The participants in this study expressed a general lack of control over their bodies due to the fatigue.
Carel (2016) also posits that bodily doubt is a central experience of chronic illness and is involved in the shift from health to illness. Bodily doubt is not exclusively cognitive, but rather experienced as anxiety at a bodily level and involves hesitancy regarding activity. Merleau-Ponty (1996) similarly states that individuals experience the immediate environment through their bodies. When a body operates in accordance with an individual’s expectations, it becomes invisible and is not really appreciated. However, when this is not the case, the focus shifts from the surrounding environment to the body itself. The women in this study described their experience of living with chronic fatigue as being in a body that is strange to them. Their fatigued bodies ruled over them because they had to plan their lives and activities around the fatigue. Their bodies were unpredictable, which had a great impact on their daily functioning. This gave rise to a feeling of being absent, in that they inhabited bodies that no longer supported their participation in everyday life. Participants described feeling imprisoned in a stranger’s body and that life appeared to be passing them by without them being a part of it.
The sense of powerlessness among participants that stemmed from persistent fatigue hugely impacted their quality of life. Strandmark (2004) argues that powerlessness is at the core of illness given the limitations it places on an individual’s autonomy, its threat to their existence, and the feeling of imprisonment it evokes, which causes great anguish. This was seen among the participants, who depicted fatigue as taking on a life of its own, which rendered them powerless and created much anguish and despair. These themes have similarly been identified in studies among patients living with other chronic diseases of which fatigue is a common symptom, such as rheumatoid arthritis (Hewlett et al., 2005).
Finally, the despair expressed by the participants is consistent with depressive symptomatology. Depression and fatigue can be difficult to differentiate since fatigue is often associated with depression and is a key symptom of major depressive disorder (Billones et al., 2020). Diagnoses of depression are common among women living with endometriosis (Young et al., 2015).
Conclusion
To the authors’ knowledge, this is the first study to explore the fatigue experiences of endometriosis patients using IPA. The study contributes to deepening our understanding of endometriosis patients’ experiences of chronic fatigue, highlighting the far-reaching effects that fatigue has in their lives and the critical need for fatigue management strategies within endometriosis treatment protocols. Further research is required to design effective treatment strategies.
While many participants became distressed during their interviews, they expressed gratitude towards the interviewer for the opportunity to speak about their fatigue experiences, with some women having discussed it for the very first time. They also reported gaining a sense of validation from their condition being recognized by the interviewer. Thus, treatment approaches should provide these patients with opportunities to talk about and validate their experiences, alongside providing support and suggestions for effective coping mechanisms and treatment.
Limitations
This study has several limitations. As with any qualitative study, the degree to which the findings may be representative of other endometriosis patients is limited. The self-selected sample of women who had mostly attained tertiary education, were fully employed, and were required to have had a surgical diagnosis likely excludes a reasonable portion of the population living with the disease in South Africa. Differences in the experiences and perceptions of fatigue may exist in other patient sub-populations. The study also relied upon respondents to self-report chronic fatigue, which is both highly subjective and a difficult symptom to understand. Finally, applying IPA at the analytical stage, once data had already been collected, may have limited the interpretive process in terms of understanding the essence of participants’ experiences.
Footnotes
Acknowledgements
We are grateful to the women who volunteered to participate in the study for their invaluable contributions and for sharing private details about their lives.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a National Research Foundation (NRF) Thuthuka grant. The opinions and conclusions of this article are those of the authors and should not be attributed to the NRF. MEL is funded by the National Institute for Health Research (NIHR Advanced Fellowship, 302929). This report is independent research. The views expressed in this publication are those of the authors(s) and not necessarily those of the NHS, NIHR or the Department of Health and Social Care. AS is supported by the National Institute for the Humanities and Social Sciences (NIHSS).