
Abstract
Obstetric research in sub-Saharan Africa largely focuses on the material, physical, and psychosocial aspects of pregnancy and childbirth in relation to mothers. This research aimed to address a research gap in terms of fathers’ experiences of pregnancy and childbirth, particularly in the context of a medically high-risk pregnancy. Specifically, this article focuses on fathers’ interactions with the healthcare system and healthcare professionals throughout the antenatal and neonatal periods. This study was exploratory and qualitative in nature. Eight fathers whose partners had experienced at least one medically high-risk pregnancy participated in semi-structured interviews that were examined using interpretive phenomenological analysis. The findings indicate that fathers’ experiences vacillated between healthcare providers being supportive and informative versus them being uncompassionate and not conveying adequate information. Importantly, the distinctions were largely attributed to the type of healthcare facility (i.e. public or private) that was attended. This research offers recommendations to healthcare workers to enhance fathers’ experiences during pregnancy and childbirth, especially in potentially traumatic situations.
Introduction
Historically, obstetric healthcare was primarily regarded as a feminine matter; however, men’s participation in the gestation and attendance and involvement at the birth of their children has increased steadily (Jackson et al., 2023). Men are often encouraged and expected to be involved throughout their partner’s pregnancy and even more so during birth (Cataudella et al., 2016; Fourie et al., 2018). The expectant father plays a significant role in supporting his partner during pregnancy, with the responsibilities often shared with other family members. In South Africa, these supportive roles often manifest as providing financial support to the mother, assisting in domestic chores, and accompanying their partner to antenatal healthcare appointments (Enderstein & Boonzaier, 2015; Makhanya, 2018; Matseke et al., 2017). Involvement in their child’s gestation and birth is a formative experience, one that can be particularly stressful and traumatic if it is classified as a medically high-risk pregnancy (MHRP) (Elmir & Schmied, 2016; Jackson et al., 2023; Yokote, 2007). An MHRP is characterised by specific attributes that increase the mortality risk of the mother and/or the child(ren). This includes maternal age, the presence of pre-existing medical conditions, the history of gestational complication, the presence of pregnancy-induced medical conditions, multiple pregnancies, and unexpected birth-related complications. When fathers perceive childbirth as negative or traumatic, there is a risk of them developing postpartum mental health problems (Boyce et al., 2007; Jackson et al., 2023). Furthermore, this negative perception may impact the well-being of their partners (Fourie et al., 2018) and may also affect the well-being of the newborn child (Cataudella et al., 2016).
The importance of healthcare providers (HCPs) in relation to the health and well-being of the expectant mother and child has long been established (Fourie et al., 2018). Existing literature demonstrates that father–child attachment commonly develops when the father attends antenatal visits (Poh et al., 2014). Antenatal consultations are important opportunities for fathers to get involved and gain knowledge about pregnancy and childbirth, bond with the foetus, and become actively involved in their child(ren)’s lives (Poh et al., 2014). Therefore, it is important to understand how they experience interactions with HCPs and how antenatal care can promote paternal involvement.
Research on men’s experiences of antenatal visits indicates that fathers often want to be present; this presence was not only verbalised as a demonstration of support for their partner but also because it was regarded as a part of their responsibilities as a father-to-be (Dheensa et al., 2013; Poh et al., 2014). Many fathers reported that although they attended antenatal appointments, they felt that they were inadequately involved in the process and therefore felt excluded (Cosson & Graham, 2012; Jackson et al., 2023; Poh et al., 2014; Steen et al., 2012). In their meta-synthesis, Dheensa et al. (2013) found that men felt ill-informed about the complexities of their partners’ MHRP and, therefore, often sought technical and statistical information, conducting their own research after consulting with HCPs. This empowered fathers and provided a sense of control. South African literature on men’s attendance at antenatal appointments also highlights that men find it increasingly important to support their partner by accompanying them to the antenatal check-ups (Makhanya, 2018); however, in reality, this is often impractical (Drysdale et al., 2021; Matseke et al., 2017). Participants in a South African study conducted by Matseke et al. (2017) shared similar sentiments. For some fathers, attending antenatal appointments was unfeasible due to the queues at the clinic, while others described some clinics as unwelcoming. Furthermore, the presence of mostly female visitors reinforced the unwelcoming clinic settings to expectant fathers (Matseke et al., 2017). As a result, some fathers reported feeling out of place.
Literature pertaining to fathers’ experiences of labour and childbirth suggests that positive interactions with HCPs contribute to a satisfactory birth experience and vice versa (Elmir & Schmied, 2016; Jackson et al., 2023). Many authors found patterns of miscommunication between fathers and HCPs, particularly in the event of emergency birth complications (Jackson et al., 2023; Xue et al., 2018). Findings from a scoping review on fathers’ experiences of MHRP by Jackson et al. (2023) highlight that interactions between fathers and HCPs were often characterised by poor communication. Research demonstrated that fathers who reported poor interactions with HCPs felt more excluded, stressed, frustrated, and less supported and involved in decision-making compared to their counterparts who reported satisfying interactions with HCPs (Boyce et al., 2007; Elmir & Schmied, 2016; Xue et al., 2018). Findings from a study in South Africa showed that many fathers reported negative experiences during the birth of their child(ren), which manifested as nervousness, helplessness, and anxiety due to a lack of information on childbirth (Sengane, 2009). Simultaneously, fathers reported excitement, delight and satisfaction immediately following childbirth (Sengane, 2009), which mirrors international literature on men’s experiences of the birth of their children (Etheridge & Slade, 2017; Hugill et al., 2013; Jackson et al., 2023; Shorey & Wong, 2022).
Overall, fathers expressed a desire for responsive and supportive HCPs, which positively influenced their feelings of involvement and appreciation (Jackson et al., 2023; Sengane & Nolte, 2012). The presence of supportive staff was found to be particularly important in the neonatal intensive care unit (NICU), where parents and staff often had prolonged interactions (Leonard & Mayers, 2008). Overall, the negative impact of poor communication, feelings of exclusion, and unsatisfactory birth experiences impacted the joy that expectant fathers experienced and replaced it with feelings of anxiety, isolation, and concern. This amplifies the need for accurate information and clear communication between HCPs and fathers to curb the negative impact of anxiety on their ability to provide support to their partner and bond with their newborn(s).
Understanding men’s interactions with HCPs also requires consideration of the country’s healthcare system. South Africa follows a two-tiered approach, comprising public and private healthcare (Michel et al., 2020). Around 84% of the population relies on government-funded service provision, which is plagued by a chronic lack of resources and staff, leading to long wait times, brief consultations and reduced quality of services (Maphumulo & Bhengu, 2019; Matlala & Lumadi, 2019; Michel et al., 2020). In contrast, through private healthcare insurance, the remaining 16% have access to private medical facilities. These facilities are characterised by improved quality of care, better hygiene standards, and well-resourced and specialist staffed facilities (Maphumulo & Bhengu, 2019). These significant disparities in resources and expenditure result in vastly different healthcare experiences.
The difference between private and public healthcare is evident in their labour wards. Private facilities typically offer private or semi-private rooms, which provide families with intimacy during childbirth. Expectant couples often maintain long-term relationships with obstetricians and have personalised birth plans tailored to the family’s needs and budget. In contrast, public facilities are typified by shared labour wards, which offer little privacy and the use of midwives or on-duty healthcare professionals. In this setting, research demonstrated a shortage of qualified midwives, with hospitals relying on nurses who were not qualified in midwifery to work in maternity settings (Hastings-Tolsma et al., 2021; Matlala & Lumadi, 2019). Overburdened and under-resourced maternity wards can be traumatising spaces where families report feeling uncared for and alienated (Lappeman & Swartz, 2019; Malatji & Madiba, 2020). This is highlighted in research conducted by Silal et al. (2012), which showed stark inequalities in access to quality obstetric care in South Africa. Participants in that study reported negative patient–provider interactions, which were typified by poor communication patterns, inattentiveness, insensitivity, and patient neglect. These problems are undoubtedly influenced by overburdened obstetric staff who, as reported in a sub-Saharan systematic review, face challenges in providing quality care due to increasing caseloads and resource constraints (Bradley et al., 2019).
Purpose of the study
While women’s experiences of childbirth and support from HCPs during childbirth have been extensively researched in the global North, there remains a paucity in research highlighting these experiences in sub-Saharan Africa. This paucity is striking, especially regarding fathers’ experiences of the ante- and neonatal period and particularly in reference to experiences within the healthcare system and staff. A positive, responsive father’s presence significantly promotes the health and well-being of expecting women and their children (Cataudella et al., 2016). For example, fathers often play an influential role in the home and can encourage their partners to adopt healthy habits and seek ante- and postnatal care (Matseke et al., 2017). Thus, it is important to investigate their experiences of their partner’s pregnancy, especially when it has been characterised as medically high risk. Furthermore, experiences of a partner’s pregnancy and childbirth can be very formative in promoting future paternal involvement in their children’s lives. This is particularly important in South Africa, which has historically been presented as having a high prevalence of fatherlessness (Richter et al., 2010).
Due to their position and expertise, HCPs are key persons in addressing men’s questions and concerns and can promote father involvement in ways that other agents cannot. The exclusion of men’s voices from obstetric research hinders opportunities for improved obstetric care to promote the health and well-being of the mother and child. Therefore, the purpose of this study was to gain an in-depth understanding of fathers’ experiences of their interactions with HCPs in the context of an MHRP in South Africa, given the lack of existing contextual literature on these interactions.
Objectives
The objectives of this study were to:
Explore fathers’ experiences of their interactions with HCPs during the antenatal stage of their partner’s MHRP.
Examine fathers’ appraisal of information and support received from HCPs during an MHRP.
Make recommendations to HCPs and mental health practitioners to enhance fathers’ experiences, increase their involvement during the birthing process, and support them after a potentially traumatic birth experience.
Method
Research design
The research design was exploratory and qualitative, consisting of semi-structured interviews conducted with men whose partner had experienced an MHRP. The data for this article were drawn from a broader study that investigated fathers’ experiences of their partners’ MHRP, focusing on their experiences during the antenatal stage, birth, and neonatal stage. Specifically, the broader project investigated fathers’ emotional experiences, experiences of giving and receiving support, interactions and experiences in the healthcare system, experiences of transitioning to fatherhood, and experiences of early fatherhood.
Participants
Fathers were recruited through a purposive sampling strategy. Only fathers who met the inclusion criteria were invited to participate (Creswell & Creswell, 2018). The criteria for participation included experiencing a minimum of one MHRP with their partner, the ability to provide informed consent, being of legal age, and the ability to communicate effectively in Afrikaans or English. Eight fathers were recruited to participate in individual semi-structured interviews. This sample size was considered appropriate for the scope of this research (Alase, 2017; Morse, 2000; Pietkiewicz et al., 2014). In accordance with the principles of phenomenological research, the intention was to recruit a non-homogeneous sample to capture a wide range of responses representative of multiple lived realities (Pietkiewicz et al., 2014). See Table 1 for participants’ characteristics and a summary of their partner’s pregnancy/ies.
Participant demographics.
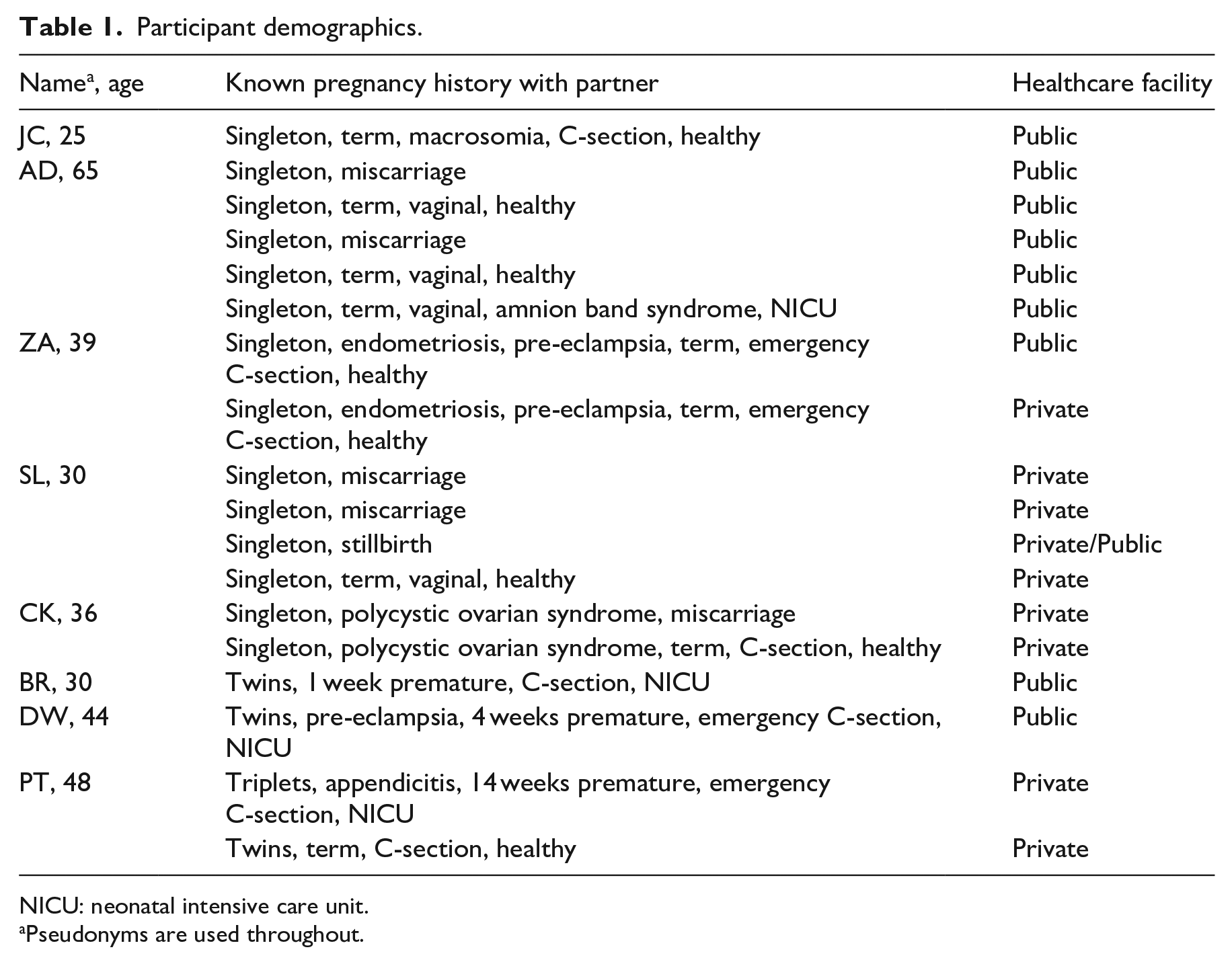
NICU: neonatal intensive care unit.
Pseudonyms are used throughout.
The fathers who participated reflected a range of differences in age, education, occupation, income, and previous pregnancy and birth experiences. All the participants resided in Cape Town; were aged between 25 and 65 years, and had experienced at least one pregnancy with their partner, with the most being five pregnancies. All but one participant was married to their partner at the time of the MHRP. Between the 8 participants recruited, a total of 18 known pregnancies (all of which were classified as medically high risk) were discussed. The pregnancies had resulted in 17 live births (8 singletons, 3 sets of twins and 1 set of triplets; 8 C-sections and 4 vaginal deliveries), 5 miscarriages, 1 stillbirth, 6 neonates admitted to NICU, 1 neonatal death in NICU, and 1 toddler death. Of the 18 pregnancies, 9 were attended to in public healthcare settings and 9 in private settings.
Procedure
Once all the relevant ethical applications were sought and approved, the participants were recruited through online platforms. Various advertisements for the research were distributed across social media platforms and online forums, with posters for the research distributed to local libraries and family-orientated non-profit organisations. Potential participants contacted the authors, and after an initial screening to establish their suitability for participation, those who were eligible were provided with detailed information about the research project and what their participation would entail. The interview dates were arranged with the participants, and they received the information sheet and consent forms by email. On the interview day, the information sheets were outlined again, and the participants were informed of their right to privacy, right to withdraw and access to sources of support.
The interviews were conducted between June 2020 and January 2021. Due to the COVID-19 pandemic restrictions, all the interviews were conducted on a secure video-enabled platform at a time convenient to the participant. The interviews were guided by an interview schedule and each session with opened with ‘Please tell me about your experiences of your partner’s MHRP’, followed by various questions about each phase of the pregnancy, the healthcare system, social support, and experiences of fatherhood. Prompt questions included ‘How did you find out that the pregnancy was high risk?’, ‘How did you experience the support from the healthcare providers?’, ‘What type of information was given to you about your partner’s specific complications?’ and ‘Was your partner hospitalised during the pregnancy?’ The length of the interviews ranged from 27 to 124 minutes, with most interviews lasting approximately one hour. After the interview, the participants were debriefed, asked whether they had any questions and whether they would like to be contacted in future for more information. They were reminded of the free counselling services outlined in the information sheet.
Ethical considerations
The project was registered and received ethics approval at the University of the Western Cape. Permission was obtained from Community Health Science Faculty Research Committee, and the Biomedical Research Ethics Committee (BM20/1/16). We prioritised minimising harm, ensuring anonymity and confidentiality, and safeguarding the integrity of the participants. The participants received verbal explanations of the research and their rights as participants, comprehensive information sheets and consent forms in their preferred language before the interviews. Written consent for audio-recording the interview was obtained.
This research followed guidelines from the seminal work of Lincoln and Guba (1985) in ensuring research trustworthiness. Trustworthiness was promoted by ensuring that the data analysis was credible, dependable, transferable, and confirmable (Anney, 2014). This was done by using interview questions informed by the literature and the aims of this study, having one researcher conduct all the interviews to maintain consistency, providing the participants with feedback and summaries of the researcher’s understanding of their stories throughout the interviews, conducting follow-up interviews where needed, and conducting detailed data analysis that was discussed in depth between the co-authors.
Data analysis
The data were analysed by the first author through a Heideggerian interpretive phenomenological approach. This type of enquiry is hermeneutic, ideographic, contextual, and grounded in social constructivism and interpretivism; therefore, it aims to unpack how individuals interpret their own lives and how meaning is attached to specific life events (Alase, 2017; Pietkiewicz et al., 2014). The interviews were transcribed verbatim and translated where necessary. The data analysis followed guidelines set by experts in the field (Alase, 2017; Pietkiewicz et al., 2014). The iterative analysis process consisted of immersion in the text; coding general units of meaning; clarification and synthesis of codes; labelling themes; compiling analytic summaries; contextualising and comparing interviews, and compiling coherent narratives. In line with the analysis approach, throughout the data analysis process, attention was given to how fathers attributed meaning to their experiences and how their experiences converged with and differed from one another. This process enabled the researchers to unpack the unique, the similar, the represented, the missing, and the meaningful in the participants’ narratives. The findings were discussed with the second author, who provided mentorship throughout the process.
Findings and discussion
From the participants’ descriptions of their interactions with HCPs, the difference between negative and positive experiences became evident. The following section shows how these experiences manifested in fathers’ narratives about the antenatal, birth, and neonatal stages. This section further discusses these findings in relation to existing research. The overarching themes were: (1) a lack of informational and instrumental support, (2) a lack of emotional support and compassion, and (3) HCPs were informative and supportive. Fathers’ satisfaction with the care they received varied greatly, mainly depending on whether they attended private or public healthcare facilities.
A lack of informational and instrumental support
For many fathers, the anxiety resulting from an MHRP was heightened by a lack of realistic information and an inadequate understanding of the pregnancy complications. This highlights the crucial role of HCPs as vital sources of information and support. In this research, three participants (ZA, DW, and JC) who relied on public healthcare facilities articulated dissatisfaction with the quality of care provided by HCPs during the antenatal period. One significant issue raised was the lack of information and resources available to fathers at these facilities. ZA stated, Nothing in-depth, just like a ‘by the way’ . . . With the state facility, it was available to you, but they wouldn’t offer it; it’s basically, ‘There’s all the pamphlets, you can see it, use it, don’t use it, it’s up to you’.
Similarly, DW noted, ‘If it wasn’t for Google, I wouldn’t have known about others’ experiences with twins’. This lack of information was a major cause of stress, mirroring findings from other studies (Cosson & Graham, 2012). Like fathers in the study by Dheensa et al. (2013), DW sought additional information from the internet to supplement his knowledge and understanding of their situation. To learn more about pregnancy and birth expectations, DW and his wife attended free information sessions offered at a local healthcare facility. Despite this, he explained that the content of the sessions did not suit their needs as parents expecting twins, stating, ‘It wasn’t really about if you had two, like we did’, indicating a desire for tailored information. Findings from Sengane and Nolte’s (2012) research closely align with these observations, with fathers consistently expressing their disappointment with the care they had received, as they perceived the information provided by HCPs as insufficient. JC explained, No pamphlets, no extra information really . . . We didn’t really understand what it [high-risk pregnancy] means, so . . . I formulated my own perception . . . and we immediately thought this was something that was going to take my girlfriend as well as my unborn child away, and obviously that thought, that perception, was very, very, anxiety provoking.
JC shared that when he and his partner were informed that their pregnancy was high-risk, the nature and consequences of this classification were not shared with them. Left to form their own opinions, which were based on the little he knew about pregnancy, JC had heightened anxiety. The lack of understanding meant that JC became gravely concerned, ‘The perception of high-risk, to me at the time it was like death’. These sentiments from JC are supported by Jackson et al. (2023), whose scoping review found that fathers indicated that they had a limited understanding of the prognosis related to the high-risk pregnancy and the potential complications. A lack of information and unfamiliarity with hospital policies had negative consequences for JC and his partner during the birth of their baby. Crucial information on labour ward policies was not explained during the antenatal consultation. Instead, as JC explained, [On the morning when she went into labour] I was blocked at . . . the maternity room, which wasn’t very nice. And we weren’t married, and I simply wasn’t allowed inside . . . She was alone. I fantasised months before, you know, what my role would be like in the ward, uhm, to have that uhm, sort of fantasy, that privilege taken away from me . . . I was devastated. I was very, very devastated.
During the antenatal consultations, the couple was not informed that the father would not be permitted in the labour ward due to their unmarried status. JC found this profoundly distressing, as he had envisioned the birth of his son in a very specific way. Having his expectations unmet left him feeling ‘really disappointed in the healthcare system, seriously, I was disappointed in the, in the healthcare system altogether’. These results are consistent with those found elsewhere (Sengane & Nolte, 2012; Xue et al., 2018), where unaccommodating and unapproachable staff left fathers feeling frustrated and excluded from the birth process.
Similarly, ZA noted a lack of information from HCPs at the public hospital they had attended. First-time father-to-be ZA described his interactions with HCPs during his daughter’s birth as follows: And all they told me was, ‘Just come back after four hours’. I’m like, ‘But we driving up and down, it’s frustrating’ . . . It was this way from about 6 pm Friday evening up until it was Sunday evening . . . I told them, ‘Look I’m not leaving here . . . I’m not leaving ‘cause this is now becoming ridiculous’ . . . [They were] not giving us all the information to say, ‘Look here just go lay down, this is what you can do to bring the pregnancy on, assist her in dilating’, any sort of information to that effect, nothing!
Throughout our conversation, ZA often referred to a lack of information and poor communication between the couple and the HCPs. Despite going into prolonged labour, his wife could not be admitted to the public hospital. By the end of the third day, she was admitted for an emergency C-section. ZA experienced his interactions with HCPs during the birth of his firstborn negatively, commenting on the lack of information about how to assist the labour – sentiments shared by fathers in other research in public healthcare settings in South Africa (Sengane & Nolte, 2012). AD and his wife also found themselves without answers following the birth of their third child. He described it as follows: They said, ‘Here comes the baby’. I looked down and then the sister held uhm, this cut-up child and there’s blood everywhere you look. The next moment, they stormed out of the ward with the child, without really communicating what is going on . . . it was terribly frustrating, I cannot describe to you the amount of frustration and anger and, uhm, hopelessness that I had experienced.
AD acknowledged that due to the ‘extensive damage’ caused by what was later diagnosed as amnion band syndrome, the HCPs ‘were shocked witless . . . they were in a panic themselves’. While he understood the reasons for being left in the theatre, this experience was anxiety provoking and left the couple feeling confused and isolated. These findings align with the observations made by Vallin et al. (2019), who found that during birth, as complications surfaced and the number of medical professionals grew, fathers experienced a sense of being overwhelmed and disoriented. Although fathers acknowledged the seriousness of the situation, they often perceived the room as chaotic. Here, the couple had to wait until the following day to see their newborn and receive the ‘devastating’ news about the child’s prognosis.
A lack of emotional support and compassion
The second theme that emerged was that of not receiving support and compassion from HCPs. Again, this theme was most prominent for the participants who were reliant on the public healthcare system. Ensuring effective communication is crucial when offering support during pregnancy, and it is essential to provide information and explanations in a compassionate manner (Jackson et al., 2023). DW felt strongly about this and spoke in depth about his experience with antenatal HCPs, who were perceived as being judgemental and unsupportive when one of the foetuses were underdeveloped. Becoming increasingly agitated as he spoke, he said: At one stage, they went as far as to ask [my wife], ‘Do you smoke, or do you drink?’ . . . And we said that we
DW further explained that later in the pregnancy, they also ‘spoke to other people that had twins, and they said it is always like that with twins, the one is a little bit small and the other big’. His desire was to have received this information from HCPs, instead of feeling held accountable for ‘something that you actually have no control over’. Throughout the pregnancy, he consistently perceived the HCPs as indifferent, unambiguously stating ‘they weren’t supportive’, mirroring the findings of other research (Cosson & Graham, 2012; Matseke et al., 2017; Steen et al., 2012).
JC expressed a similar experience, verbalising that he felt neglected during antenatal consultations. He stated that dissatisfaction was to be expected, as ‘[p]ublic hospitals were very, very inundated with patients, sick people and you know it’s only normal so to say, to sort of just like move through the system very quickly’. This normalisation of subpar care that plagues the resource-constrained environment typify many South African public healthcare facilities. Feeling disregarded by HCPs was also evident in ZA’s depictions of the birth of the couple’s firstborn. He recalled, [The HCPs were] not really helpful and [were] dismissing everything we saying. Yes, we are not clued up about how things work, but end of the day show some compassion . . . I just dislike the way we were treated.
The participants’ narratives highlighted that public healthcare facilities were perceived as overcrowded, leading to a decline in the quality of care provided to each patient. Congruent with the findings of Jackson et al. (2023), fathers wanted to be involved and respected; however, similar to those of Sengane and Nolte (2012) and Lappeman and Swartz (2019), this expectation was often unmet. Several participants commented on the poor communication between the HCPs and the expectant couples. Dealing with an emotionally demanding situation while interacting with a healthcare system that was unfamiliar to them amplified their negative experiences.
HCPs were informative and supportive
In contrast, some fathers had overwhelmingly positive feedback about the care they had received at healthcare facilities. These positive interactions were primarily associated with private healthcare facilities. However, it is worth noting that some fathers expressed satisfaction with public facilities, particularly in relation to support provided by NICU staff.
In contrast to existing South African literature on fathers’ involvement during the antenatal stage (Drysdale et al., 2021; Matseke et al., 2017), all the fathers in this study had played an active part in their partner’s pregnancy or pregnancies and had attended nearly all the antenatal consultations. First-time father-of-twins BR shared a positive experience with his HCPs at the public facility. He explained that their HCP had provided them with thorough, accurate information about what to expect with a twin pregnancy. BR said that the HCP ‘gave us good information about where to go . . . gave [my wife] good information on what to eat, gave us some solutions for the nausea’.
First-time father SL explained that he had attended every antenatal check-up for all his wife’s pregnancies, and he was very satisfied with the quality of care they had received from their private hospital. Following two miscarriages, SL’s wife suffered a pre-term labour while on the highway and the couple raced to the closest healthcare facility, which was a public facility. The couple’s third pregnancy ended in a ‘very traumatic’ stillbirth. Despite the grief of losing another pregnancy, he stated the following about the care received at the public hospital: ‘I think mostly they treated us well, and I don’t think there is anything wrong with our state hospitals and the sisters’.
SL later clarified that despite being satisfied with the public facility, the couple elected to continue receiving care from a private hospital for their fourth pregnancy. He praised their HCPs: ‘They calmed us down, which was very good’. He described giving birth in a COVID-19 ward and stated that the ‘experience was amazing’. Similarly, CK was happy with the quality of care they had received at their private hospital, stating that they had received ‘excellent moral support from the doctors’ and ‘we have a good faith in [the HCPs] and [they] explained everything beforehand’. CK and his wife had a close relationship with their HCP, which made CK comfortable during antenatal consultations. In line with other research findings (Vallin et al., 2019), CK trusted the HCPs, which improved his overall experience because he felt satisfied with the care they were receiving.
ZA’s reflections revealed that after the birth of their first child, he subscribed to private medical aid to avoid reliving the dissatisfactory care they had received at the state hospital. Determined to attend all the antenatal consultations, he stated: ‘That’s a part of
ZA highlighted the contrasting experiences between public and private healthcare as follows: ‘I just feel difference in, let’s call it customer service . . . it was two different experiences’. ZA’s words capture the disparities in experience between the public and private healthcare systems in South Africa. He continued, ‘I felt better . . . It was nice. It was like a hotel compared to the public hospital . . . And I felt like doctors and nurses were a lot more accommodating and compassionate’. The attentive and compassionate approach of the private healthcare professionals made a significant difference, providing a positive and satisfying experience for the couple during their second pregnancy.
Similarly, PT and his wife had attended private facilities when they were expecting triplets. Despite facing multiple challenges, including his wife’s failing health that resulted in frequent hospitalisation and an emergency appendectomy, he, too, reported an overwhelmingly positive experience with their HCPs. A decade later, he vividly recalled the names of many staff members who had worked diligently to resuscitate, incubate and operate on the neonates in the NICU. Overall, PT described the care they had received as ‘fabulous’.
Despite earlier characterisations of antenatal HCPs (at the public facility) being unsupportive, DW noted that the midwives and neonatal nurses had been particularly helpful during what he described as ‘the most traumatic experience I have ever had’. He recalled: ‘The moment they did the C-section, and you see this baby coming out, you know, I’ll never forget, I started crying, no one laughed at me’. The delivery team’s emotional support and efforts to involve DW in the delivery of his children were well received, contrary to his previous interactions with HCPs. He expressed a deep appreciation for nurses in the NICU: ‘They were very nice to the children when they were born, looked after them well, the nurses, uhm, they knitted jerseys for [my daughter], during the time she was in [NICU] for three weeks’. Feeling that the NICU staff genuinely cared was immensely beneficial during their children’s extended stay, as it created a sense of trust and comfort for DW and his partner. This positive experience with caring and compassionate HCPs made a significant difference during this emotionally challenging time. This supports the findings of Leonard and Mayers (2008), who demonstrated that clear information and supportive NICU staff were essential in fostering positive experiences during stressful and potentially traumatic moments.
The impact that the presence of a supportive, available, knowledgeable HCP makes on the father’s experience of the pregnancy is clear. A lack of informative and compassionate interactions with HCPs may contribute to a negative pregnancy experience, even more so in instances of an MHRP. These accounts emphasise the important role that supportive and knowledgeable HCPs can play in the experiences of expectant fathers, especially during complex pregnancies and childbirth.
Recommendations
The findings of this study offer several recommendations for healthcare facilities and HCPs to improve support for expectant fathers. First, facilities should adopt strategies for targeted information dissemination tailored to the needs of fathers. This entails (1) providing consistent, clear, and accessible information about the pregnancy; (2) organising inclusive antenatal classes that involve fathers, and (3) using print media (posters, pamphlets and brochures) to explain various obstetric processes and potential complications. Second, HCPs should actively encourage fathers to participate in antenatal consultations. Finally, healthcare facilities should establish partnerships with external support groups or make referrals to socio-emotional support structures that cater specifically to the needs of fathers.
The insights derived from this research have significant implications for mental health practitioners. It highlights the importance of these professionals being aware of potentially negative experiences that fathers may have during their partners’ pregnancy and childbirth. Notably, these experiences may have a traumatic quality, with the capacity to have enduring effects on fathers’ well-being. Consequently, there arises a necessity to offer customised attention and assistance to address the specific requirements of distressed fathers within this framework. Such targeted support can play a pivotal role in mitigating the impact of these adverse experiences and promoting the mental well-being of fathers.
Based on the findings of this research, there is a need for more empirical evidence to understand how fathers interact with and perceive MHRPs, with the goal of promoting paternal involvement. Recommendations for future research include large-scale quantitative survey research on the prevalence of MHRPs in South Africa, research on fathers’ perceptions of the standard 10-day paternity leave, research on men’s experiences of maternal near-misses, and research on the role that restrictive masculinity norms play in terms of men’s ability to grieve for pregnancy and neonatal loss.
Limitations
As a study grounded in an interpretive phenomenological framework, these findings are time and context-specific and can therefore not be generalised to all fathers in Cape Town or South Africa. In addition, the language criterion (English or Afrikaans) limited the participation of men who had other languages as their mother tongue. The recruitment was done primarily through social media, thus, men who did not have resources or access to the specific recruitment sites were not reached, thereby limiting the heterogeneity of the sample. However, the findings contribute to recommendations to improve clinical practice to better support fathers during an MHRP.
Conclusion
An MHRP can have enduring effects on fathers, hindering their ability to effectively fulfil the multiple roles expected of them in supporting their partner and child(ren). In this research, all the fathers depicted the MHRP as stressful. However, positive and attentive interactions with HCPs who conveyed high-quality information helped to mitigate the stress. There was a notable contrast between the experiences of those who attended private healthcare facilities and those who relied on state facilities. For the latter group, HCPs were described as inundated with patients, resulting in lower quality of care being received. This left fathers confused and frustrated. Conversely, fathers at private facilities appreciated the staff’s attentiveness and the quality of care received. Regardless of the hospital setting, NICU staff received praise for their compassionate, informative, and attentive behaviour. This study highlights the significant impact of accurate information conveyed through respectful and compassionate interactions between HCPs and fathers on their overall experience of their partner’s MHRP and childbirth.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Research Foundation (TTK190405427633).