
Abstract
Religious commitment is a prominent feature in the lives of many students in Africa. The present study investigated the well-being correlates (emotional well-being, social contribution, and depression) of religious commitment, and compared them across sex. A cross-sectional sample of 471 students from South Africa and Kenya (men = 244; women = 227; with an average age of 22.8 years) completed the Religious Commitment Inventory, Patient Health Questionnaire, Social Well-being Scale, and Mental Health Continuum Short-Form. Structural equation modelling in Mplus was used to estimate direct effects of religious commitment on emotional well-being, social contribution and depression, and comparison across sex. The results showed significant direct effects, attesting to the association of religious commitment with higher emotional well-being and social contribution, and lower depression, with no significant sex differences. In addition to insight into positive and negative intra- and interpersonal well-being correlates of religious commitment, the absence of sex differences shows uniformity in how religious commitment is related to well-being for male and female students.
Religiosity, which includes religious commitment, beliefs, and practices, is a prominent feature of the lives of many individuals and communities (Schumann, 2020). African communities are said to be highly religious (Kenzo, 2004; Mbiti, 1991), collectivistic (Wissing & Temane, 2008), and culturally tight (Khumalo et al., 2020). Gelfand (2012, p. 420) describes a culturally tight society as one ‘with strong norms and a low tolerance for deviant behaviour’. Interdependent societies are culturally tight and collective (Carpenter, 2000). African societies are known to draw meaning from religious practices (Wissing et al., 2014; Wissing et al., 2020), find religious beliefs to contribute to their well-being (Nell, 2016; Wilson et al., 2019), and have religiosity as an antidote to ill health (Mpofu, 2018). Although the effects of religiosity on human psychological processes have been examined (e.g., Koenig et al., 2012), the role played by religious commitment in holistic psychological health (see Keyes, 2005, 2013) in African populations remains under-researched (see Mpofu, 2018).
Religious commitment is defined as ‘the degree to which a person adheres to his or her religious values, beliefs, and practices and uses them in daily living’ (Worthington et al., 2003, p. 85). Studies examining religious commitment and well-being dimensions have yielded divergent findings (Koenig, 2012; Paine & Sandage, 2017). While some studies have found positive relationships (Ajibade et al., 2016; Reed & Neville, 2014), others have reported negative associations (Raiya et al., 2010). According to Inzlicht et al. (2011), by providing meaning and understanding, religion offers a worldview through which people make sense of the world, thus buffering against uncertainty and distress. Mechanisms such as self-regulation (McCullough & Willoughby, 2009), spirituality (Ohajunwa & Mji, 2018), and meaning-making (Inzlicht et al., 2011) are said to account for how religious commitment benefits well-being.
The present study maintains that not only is well-being indicated by a positive intrapersonal expression of happiness, but it also includes an interpersonal component of reaching out to others, as well as the absence of or reduced psychological distress (Keyes, 2005, 2013). This comprehensive approach to conceptualising and operationalising well-being is reminiscent of the model of wellness (Hattie et al., 2004) and the general well-being model (Khumalo et al., 2010; Wissing & Temane, 2008). Thus, we are interested in the association between religious commitment and multiple dimensions indicating presence and absence of intra- and interpersonal well-being, namely emotional well-being, social contribution, and depression.
Empirical research findings have shown a positive relationship between religious commitment and emotional well-being (Ajibade et al., 2016; Reed & Neville, 2014). The contribution of religious commitment to life satisfaction has been accounted for by its provision of a sense of structure to the social world, and through alleviating existential concerns (Ajibade et al., 2016; Van Tongeren et al., 2013). Among university students, religious commitment is found to increase with life satisfaction because it enables adaptation and reduces stress associated with the learning environment (Achour et al., 2017; Alaedein-Zawawi, 2015).
Social contribution, which includes altruistic intentions and disposition, appears to be omnipresent in religious practices and doctrines, as many religions encourage generosity and contribution to others among their adherents (Blogowska et al., 2013; Mattis & Grayman-Simpson, 2013). It is likely to ensue from religious commitment as a result of positive social identity linked to the feeling that an individual is connected and valued (Blaine & Crocker, 1995; Valsala & Menon, 2023). Keyes (1998) describes social contribution as the extent to which an individual believes that they have the capacity to help others and contribute to society. Previous research on religious commitment has not been explored in relation to social contribution as defined by Keyes (1998).
Religious commitment has been linked to mental health (Zou et al., 2014), and a decreased risk of depression (Balbuena et al., 2013; Koenig, 2012). At the same time, religious commitment has been found to have an inverse U-shape relationship with depression (Wei & Liu, 2013), showing the need for further exploration. Those who benefit from religion ascribe the positive effect to religion being a multipronged support system (Wang et al., 2016). According to Paine and Sandage (2017), religion offers a refuge from the troubles and hassles of daily life and its practice, belief, and commitment are therapeutic. However, according to Wei and Liu (2013), religious attendance tends to exacerbate the estimated deleterious effects of certain types of stressful life events.
The well-being benefits of social and cultural systems such as religion may be more pronounced in one sex group than another. Owing to societal norms, sex differences in psychological and health outcomes (e.g., Tadi et al., 2022) are often accounted for by the culturally and socially shaped variations (Afifi, 2007), and specifically the way in which African communities determine the social expectations, prescriptions, and prohibitions imposed across gender roles.
Among South African students, Patel et al. (2009) found that an increase in religious commitment was associated with greater psychological well-being. Among Jewish adults the relationship between religious support and well-being was stronger for women (Lazar & Bjorck, 2016).
Given the importance of religion in an African socio-cultural context (see Mbiti, 1991), the present study investigated how religious commitment was associated with emotional well-being, social contribution, and depression. The study’s data were gathered from university students in South Africa and Kenya. Although the two countries are situated in different regions of the African continent, they, together with the rest of sub-Saharan Africa share a common socio-cultural orientation (Møller & Roberts, 2017). The reality of this cultural commonality does not deny nor contradict the multi-ethnic and linguistic nature of the plural societies of sub-Saharan Africa (Adams et al., 2016). It is in the context of this common orientation of shared collectivism (Adams et al., 2016; Møller & Roberts, 2017) that the students in this study are situated. While student populations are known to be an important but vulnerable group, there remains a gap in empirically sound research aimed at determining well-being antecedents and their causal mechanisms (Dar & Iqbal, 2019).
Access to university provides the needed social mobility for young people (Walker, 2020). A few studies concerned with the psychological functioning of university students have taken a pathogenic view (e.g., Tadi et al., 2022). In those where a well-being perspective is taken (e.g., Mason, 2019; Walker, 2020), the question of religiosity does not feature significantly. This research gap exists despite religiosity being central to human development and its importance tends to remain stable during student years (Gilbertson et al., 2022).
Method
Participants
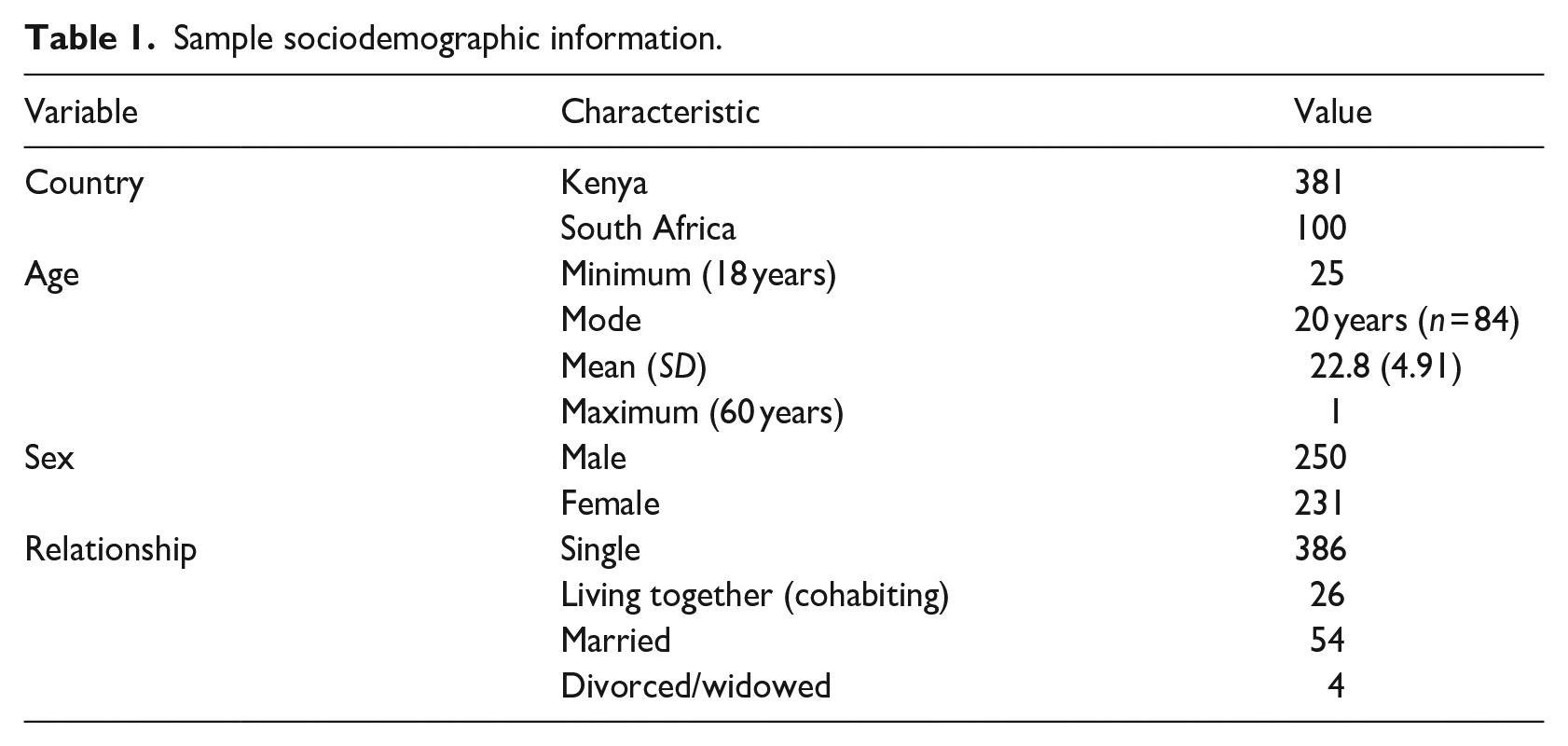
The group of participants (N = 471) consisted of students from Kenya (n = 373) and South Africa (n = 98). There were 244 men and 227 women students, with a mean age of 22.81 (SD = 4.92); 18 participants did not disclose their age. While the students from Kenya were based at a university in a rural setting in the West of the country, South African students came from a university situated in an urban centre. All participants were registered students and not necessarily psychology students. The participants completed the English version of the questionnaires. From the initial 490 students considered, 7 were excluded on the basis of missing sex identifying information, and the remaining cases were excluded on the basis of them having not completed more than half of the items of the target measuring instruments. Sociodemographic variables and frequencies are displyed in Table 1.
Sample sociodemographic information.
Instruments
The Religious Commitment Inventory (RCI-10; Worthington et al., 2003) was used to assess the levels of religious commitment. It consists of 10 items scored on a 5-point agreement Likert-type scale. The scale has two dimensions: intra-personal religious activities (6 items) and interpersonal religious activities (4 items). However, Worthington et al. (2003) observed that the two dimensions tended to be highly correlated, rendering the RCI-10 unidimensional. The reliability indices for the RCI-10 range between .87 and .93 (Worthington et al., 2003). The present study applied the unidimensional model and obtained an omega reliability index of .91.
The Patient Health Questionnaire (PHQ-9 Kroenke et al., 2001; Kroenke & Spitzer, 2002) was used to measure the prevalence of self-reported symptoms of depression. The PHQ-9 is a nine-item screening tool scored on a 4-point frequency Likert-type scale. It has been applied in sub-Saharan Africa with evidence of good psychometric properties, including to people living with HIV/AIDS in western Kenya, where Monahan et al. (2007) reported a Cronbach’s alpha of .78. The unidimensional PHQ-9 obtained an omega reliability index of .89 in the present study.
The Mental Health Continuum Short-Form (Keyes, 2006; Keyes et al., 2008) subscale for Emotional Well-Being (EWB) consisting of three items. The participants completed the whole MHC-SF, which consists of 14 items. Joshanloo et al. (2013) found a Cronbach’s alpha of .77 in the South African sample. The present sample obtained an omega reliability index of .79.
The Social Well-Being Scale (SWBS-SF; Keyes, 1998) subscale for social contribution comprising three items was used to measure individual social contribution. The SWBS-SF (total of 15 items) is scored on a 6-point agreement Likert-type scale, and has five subscales comprising three items each: social coherence, social contribution, social actualisation, social integration, and social acceptance. Although the participants completed the whole SWBS-SF, only the social contribution subscale was included in the analysis. Keyes (1998) found Cronbach’s alpha coefficients of .75 for a Dane County sample, and .66 for a national US sample. The present study obtained an omega reliability index of .72.
Procedure
Data were collected in 2017 by means of English-version questionnaires completed by students who were recruited by means of classroom announcements and pamphlets placed on their university campuses. Without coercion or compensation, volunteering participants completed the questionnaires in their spare time, after signing informed consent letters. Data were captured and checked for accuracy by postgraduate psychology students under the supervision of the first author.
Ethical considerations
Recruitment, obtaining participant consent, and the distribution of questionnaires were facilitated by trained student assistants at both universities. Students were assured of confidentiality. The study was part of a multi-country research project titled ‘Measuring and exploring the contextual manifestation of well-being: A cross-cultural African study’. Ethical clearance (NWU-HS-2015-0126) was awarded by the Ethics Review Board at North-West University in South Africa, which is governed by the guidelines of the South African Department of Health (2015) and adheres to Helsinki Declaration (World Medical Association, 2013).
Statistical analysis
Statistical analysis, conducted using structural equation modelling (SEM) (Byrne, 2012; Kline, 2011) in Mplus, version 8.1 (Muthén & Muthén, 1998–2017) followed four steps. The measuring instruments were first examined for reliability using the guidelines of McNeish (2017). In the first step, the measurement model demonstrating the distinction and independence and intervariable relationships among the four latent variables was tested. The following criteria for model fit index cut-off points indicating excellent fit, as recommended by Hu and Bentler (1999) and applied by Byrne (2012), were used: smaller and insignificant χ2, root mean square error of approximation (RMSEA), and standardised root mean square residual (SRMR) of less than .06; comparative fit index (CFI) of more than .95; and Tucker–Lewis index (TLI) of more than .95. However, good and acceptable fit can be indicated by CFI and TLI of >.90 (Kline, 2011). In fact, according to Kline (2011, p.197), ‘Hu and Bentler (1999) never intended their rules of thumb for approximate fit indexes to be treated as anything other than just that’.
The second step was concerned with testing the direct effect of religious commitment on three dependent latent variables: depression, emotional well-being, and social contribution. The strength and significance of direct effects were tested on the basis of their direction, size, probability, and confidence intervals. Third, as a precursor to multi-group sex comparison, the measurement invariance of the latent variables was examined (see Strasheim, 2014; Van de Schoot et al., 2012). The chi-square difference and the change in CFI were used for model comparison across configural, metric, and scalar models (Van de Schoot et al., 2012). Fourth, the direct effect models were estimated for the two groups, and the strength of the significant standardised direct effects was compared using the Wald test statistic. This method is referred to as multi-group moderation analysis (Strasheim, 2014). In all the analyses, all variables were treated as categorical, and the mean- and variance-adjusted weighted least squares (WLSMV) estimator was used (see Byrne, 2012; Muthén & Muthén, 1998–2017). WLSMV is a robust weighted least squares estimator, and uses a diagonal weight matrix (Muthén & Muthén, 1998–2017). Variables measured on shorter range Likert-type scales are considered categorical (Byrne, 2012).
Results
Measurement models
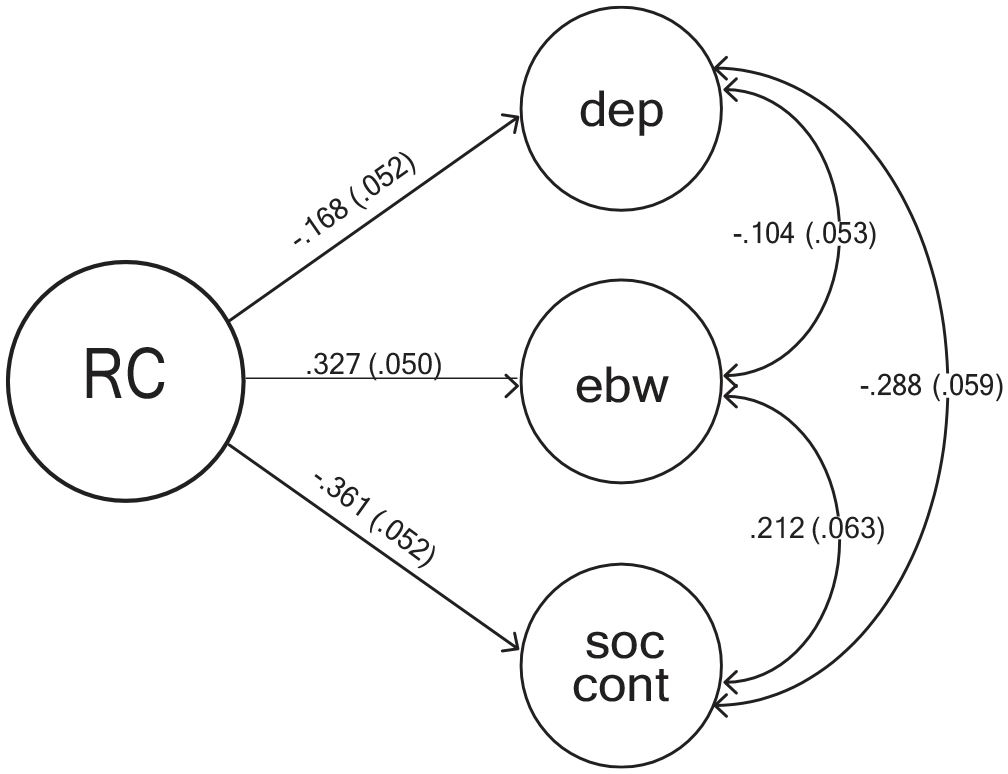
Model fit indices for the confirmatory factor analysis (CFA) measurement models are presented in Table 2. As shown in Figure 1, the theoretically intended measurement model with four latent variables, namely religious commitment, social contribution, emotional well-being, and depression, was estimated. This four-factor model, with correlated latent variables, had good fit in the whole sample: CFI = .958, TLI = .953; CFI = .965, TLI = .961 for males (n = 244), and CFI = .934, TLI = .927 for females (n = 227).
Fit indices of the theoretically intended four-factor measurement model across samples.
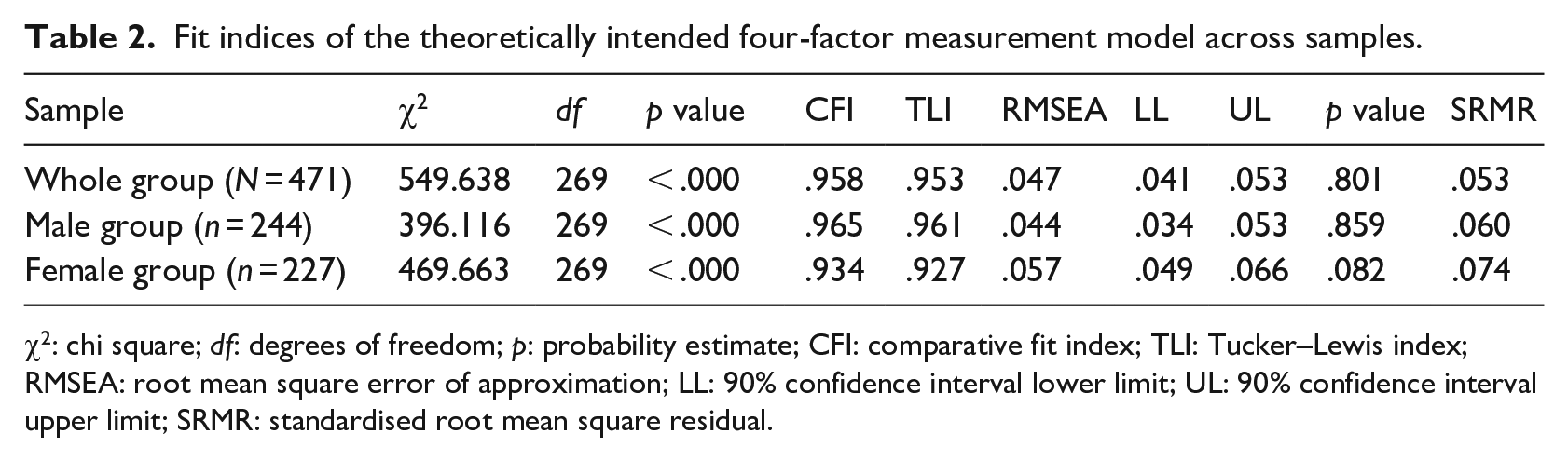
χ2: chi square; df: degrees of freedom; p: probability estimate; CFI: comparative fit index; TLI: Tucker–Lewis index; RMSEA: root mean square error of approximation; LL: 90% confidence interval lower limit; UL: 90% confidence interval upper limit; SRMR: standardised root mean square residual.
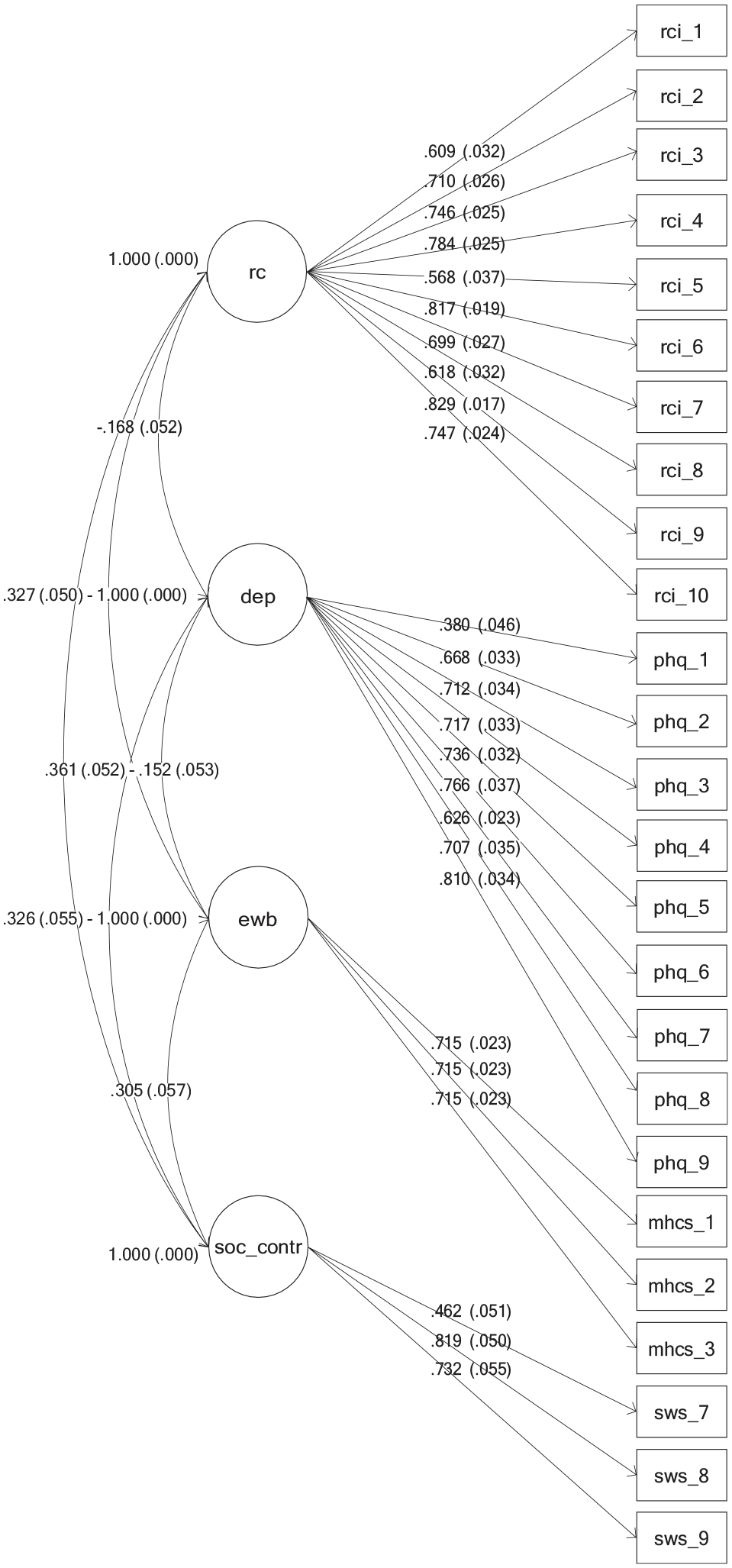
The measurement model showing the four latent variables.
Measurement invariance
Based on baseline models, the four-factor measurement model was tested for measurement invariance across the two sex groups (see Table 3). A good fit was obtained from the baseline model, thus indicating configural invariance. The model with equality constraints on the factor loadings showed good fit, and its CFI difference (.003) against the configural model was not large enough to warrant a rejection, showing metric invariance. Scalar invariance was tested by fitting a model with equality constraints on the items’ intercepts and comparing its CFI with that of the configural model. A CFI difference of .004 demonstrated scalar invariance.
Measurement invariance testing across gender (male = 244; female = 227) for the four-factor measurement model.
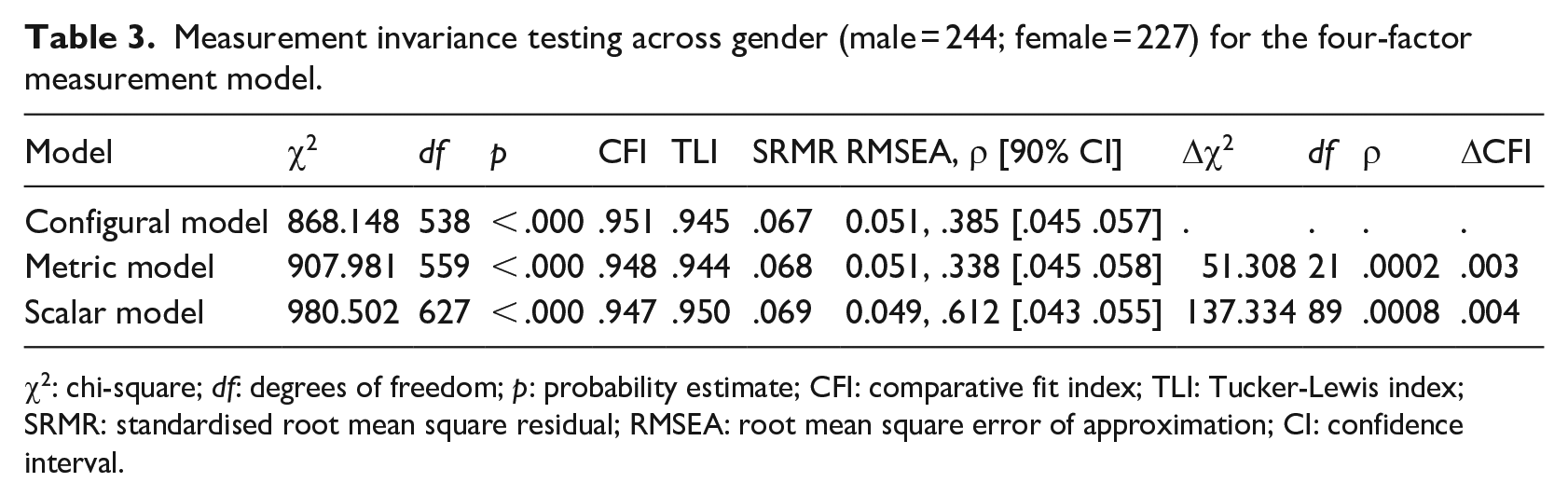
χ2: chi-square; df: degrees of freedom; p: probability estimate; CFI: comparative fit index; TLI: Tucker-Lewis index; SRMR: standardised root mean square residual; RMSEA: root mean square error of approximation; CI: confidence interval.
Inter-variate correlations
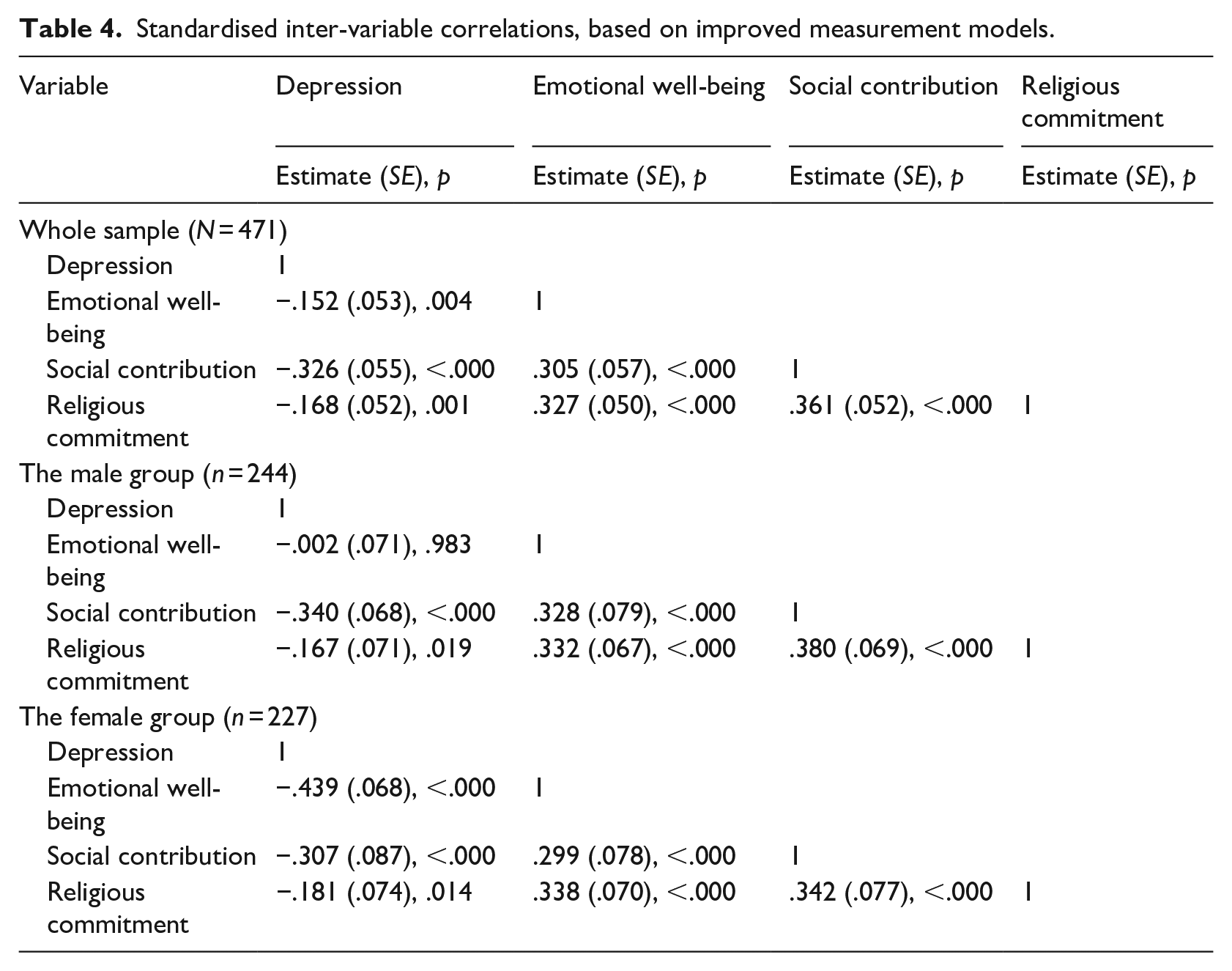
Bivariate correlations investigating the associations among religious commitment, depression, emotional well-being, and social contribution were observed in the whole sample, and in the male and female groups (Table 4). In all instances, except for the relationship between depression and emotional well-being amongst males, the correlations were significant. Religious commitment was consistently positively correlated with emotional well-being and social contribution, and negatively with depression.
Standardised inter-variable correlations, based on improved measurement models.
Direct effects
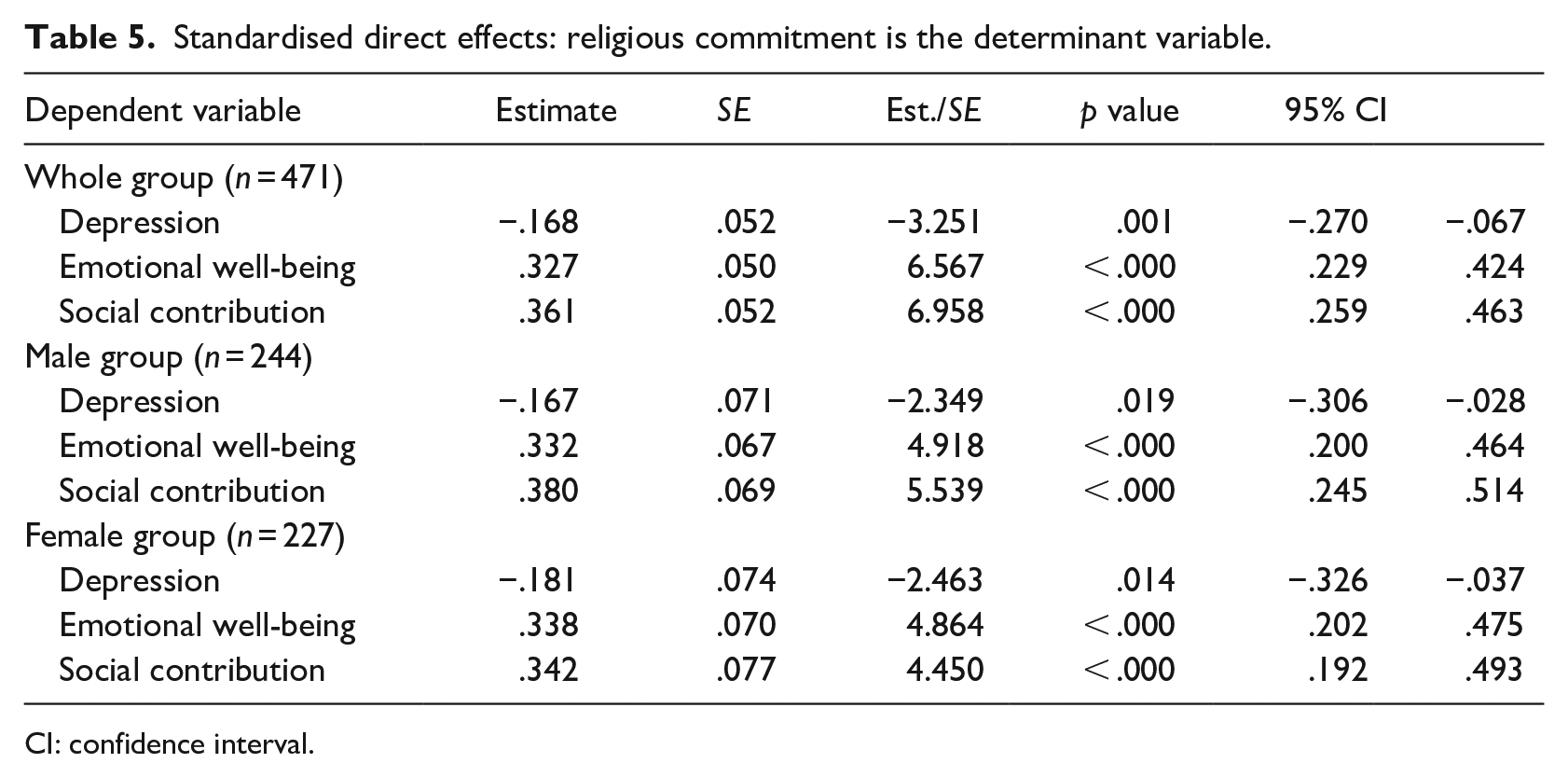
The direct effects model, in which religious commitment is estimated as a determinant for three outcomes is shown in Figure 2. As seen in Table 5, all three direct effects were significant for the whole group, as well as for the separate male and female groups. Hence, religious commitment significantly predicted lower levels of depression and higher levels of emotional well-being and social contribution. Comparing these direct effects between males and females showed no differences: religious commitment to Depression: Wald (1) = .151, ρ = .697; religious commitment to Emotional well-being: Wald (1) = .89, ρ = 765; and religious commitment to Social contribution: Wald (1) = .144, ρ = 704.
The structural model showing the direct effects.
Standardised direct effects: religious commitment is the determinant variable.
CI: confidence interval.
Discussion
The purpose of the present study was to investigate the relationship of religious commitment with emotional well-being, social contribution, and depression, and compared across sex. We found that religious commitment was associated with higher emotional well-being, higher social contribution, and lower levels of depression. No difference between male and female students was found.
The finding that for this group of Kenyan and South African students, religious commitment was associated with emotional well-being, is similar to reports from other samples elsewhere in the world. For example, among Muslims in Turkey, Aydogdu et al. (2021) found that religious identification and practice were associated with happiness and life satisfaction. Similarly, in Poland, those who attended religious services more frequently reported higher emotional well-being (Pawlikowski et al., 2019). In Ghana, orphans placed in an orphanage ascribed their happiness to ‘having God’ (Salifu Yendork & Somhlaba, 2017).
Regarding religious commitment and social contribution, although Pazhoohi et al. (2017) noted that research in this area is inconclusive, our study lends support for the relationship between religious commitment and social contribution. Religion fosters transcendental values of connectedness with a bigger realm (Wissing et al., 2020), which in turn encourages individuals to actively engage in adding value to their community. It inspires selfless giving and contributing to the well-being of others, as individuals commit themselves to the teachings, doctrines, and values of their religious organisation. In addition, commitment to religious ideals that support other-directedness and self-effacement might spur individuals to volunteer, and be more creative and helpful (Schumann, 2020). Religion primes its adherents towards protecting and enhancing well-being and prosocial behaviour (Preston & Ritter, 2013). In addition, religious people tend to exhibit an agreeable personality that encourages selfless concerns for others, as well as trusting and generous attitudes (Blogowska & Saroglou, 2011).
Religious commitment functions through a number of mechanisms to reduce depression (Epstein-Ngo et al., 2013). Practices associated with religious commitment, including prayer and meditation, offer themselves as tools for dealing with incomprehensible, difficult life situations (Cole-Lewis et al., 2016). Religious teachings tend to proffer solutions and explanations that result in meaning-making, consequently mitigating depressive symptoms. Within most African settings, doctrinal messages are infused with the omnipotence of a Supreme Being who is able to either solve or provide explanations for the difficult questions of an individual’s existence (Cole-Lewis et al., 2016).
No sex differences were found in the relationship between religious commitment and indicators of mental health. The findings also do not indicate that religious commitment protects the one sex better than the other. Yet, various studies have suggested that there is a significant and consistent sex difference in religiosity itself (Bergan & McConatha, 2001; Collett & Lizardo, 2009) and in most variables of mental health, especially depression (Afifi, 2007; Wilson & Somhlaba, 2018). The finding of measurement invariance for the measures of religious commitment, depression, emotional well-being, and social contribution across gender, is important as it shows that the male and female participants in this study interpret the indicators of these constructs in the same fashion.
Despite the contributions of the present study, it is not without its limitations. As with all cross-sectional data, conclusions of causality cannot be made. Beyond university students, future studies may wish to focus on more representative adult and clinical populations. Although the present study did not seek this information, it may be important to know the religious affiliation of the participating individuals. In addition to exploring emotional well-being and social contribution, future studies could test a structural model where the relationship between religious commitment and other dimensions of positive mental health (i.e., flourishing; Keyes, 2002) are determined.
There are a variety of reasons and mechanisms through which the link between religious commitment and well-being can be explained. Among them are that, religion is a form of culture (Cohen, 2009), an external expression of inner spirituality (Pawlikowski et al., 2019), and a source of meaning and motivation (Inzlicht et al., 2011). Although the mechanisms through which this link is made was not the focus of this study, such knowledge is important and future studies in the African context may wish to investigate this.
Finally, it would have been useful for this study to have controlled for possible confounding variables, including religious affiliation, age, and socio-economic status of the participants.
Conclusion
Our findings provide further support for the association between religious commitment and well-being. The comprehensive study by Inzlicht et al. (2011) provides a neuropsychological explanation and argues for the psychological pathways of meaning and motivation for the effects of religious belief and practice. Therefore, it is plausible that to promote positive psychological functioning and protect against mental illness, religious beliefs and practices may be an important component to consider. While recognising that there have been numerous studies addressing the link between religious commitment and psychological functioning, the present study’s contribution is important for a few reasons. However modest, and notwithstanding the conception and operationalisation of well-being as multidimensional (see Keyes, 2002, 2005), the present study’s contribution is anchored in its novel context of interest. Not only is Africa considered as collectivistic in cultural orientation, there is high social norm regulation in this region (see Carpenter, 2000). Implications for well-being-promoting interventions could be grounded in fostering religious commitment among people of faith and promoting other self-transcendental values among those who do not have a preference for religious practices.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.