
Abstract
Identifying the factors that contribute to differential vulnerability in the face of adversity is key to psychology fulfilling its mandate as a helping profession. One such factor, fortitude, which is described as the psychological strength to manage adversity and to stay well, has consistently been linked to psychological well-being. The objective of the research was to statistically integrate studies examining the relationship between fortitude and the indices of psychological well-being by using a meta-analysis. We used a random-effects model for the meta-analysis. In addition to the overall effect size, we examined publication bias and the moderating role of age and methodological quality. We also performed a subgroup analysis to compare between studies with positive and negative indicators of psychological well-being. In addition, we used robust variance estimation to account for effect-size dependencies, as some studies have reported more than one correlation coefficient. A total of 13 studies reporting 35 correlation coefficients pertaining to the relationship between fortitude and the indices of psychological well-being were extracted. The meta-analysis revealed a significant overall effect (r = .44, p < .001). The results also indicated that age and methodological quality did not influence the effect size. Subgroup analysis indicated that the overall effect size for studies that used positive indicators (r = .49, p < .001) was higher than that for studies that used negative indicators (r = .36, p < .001). In addition, no visual or statistical evidence of publication bias was observed. The robust variance estimation results also confirmed that the effect-size dependencies did not influence the overall effect size. The study results provide strong evidence regarding the association between fortitude and psychological well-being. This finding has several implications for promoting mental health and suggests that interventions aimed at building fortitude can be leveraged to mitigate psychological distress.
Experiencing hardships and distress is an intrinsic part of life (Lahti, 2019). Therefore, focusing on the factors and processes that help overcome these hardships is imperative (Adler et al., 2017; Hamid & Singaram, 2016). Although eradicating stressors and challenges from an individual’s environment is considered an unrealistic goal (He et al., 2018), studies have often focused on identifying and understanding the factors that enhance psychological well-being (PWB). In doing so, individuals can effectively navigate challenges while maintaining their sense of PWB. Generally, PWB describes not only the absence of mental ill-health but also the presence of positive factors, such as positive emotions and self-concept, self-actualisation, and supportive relationships (Adler et al., 2017), in other words, an individual who manages to flourish in several areas of their life (He et al., 2018). Research has also identified various factors that contribute to PWB, such as autonomy, self-acceptance (Ryff, 2014), familial and social support, mindfulness (He et al., 2018), resilience (De Kock et al., 2021), and fortitude (Lahti, 2019; Roothman et al., 2003). High levels of well-being enhance both psychological and physical health and, through various pathways, are even associated with longer life expectancy (Diener et al., 2010; He et al., 2018; Vázquez et al., 2009). However, some adversities often surpass an individual’s ability to overcome their challenges.
Recently, COVID-19 precipitated a global public health crisis. The measures implemented to curb the spread of infection (e.g., national lockdowns, closure of educational institutions and nonessential services, social-distancing policies, and work-from-home mandates) led to unprecedented disruptions in daily routines, schooling, employment, mobility, and social connectedness.
Since the onset of the pandemic, several nationwide studies on the mental health status of the general population have consistently reported decreased levels of PWB and increased negative mental health outcomes (Chen et al., 2021; Fond et al., 2021). For example, a nationally representative survey conducted in the United States (Ettman et al., 2020) reported a threefold increase in depression early on during the pandemic. Similarly, in the United Kingdom, a nationally representative survey (Fujiwara et al., 2020) indicated substantially elevated levels of anxiety during the initial stages of the pandemic compared with previous years. Other representative population-based studies from China (Wang et al., 2020) have also reported moderate-to-severe symptoms of anxiety and depression in the months following the outbreak.
Similar studies in low-to-middle-income countries, such as in South Africa (Pretorius & Padmanabhanunni, 2021a), Brazil (Goularte et al., 2021), Bangladesh (Banna et al., 2022), and India (Venugopal et al., 2022), have reported elevated levels of depression, anxiety, loneliness, and posttraumatic stress disorder among the general population. Although the levels of psychological distress clearly increased at the beginning of the pandemic, the mean levels of distress declined or returned to the prepandemic levels over time. This notion was observed in various longitudinal studies (Bendau et al., 2021; O’Connor et al., 2021). Furthermore, the current data suggest that certain groups of people were at a greater risk of adverse mental health outcomes, whereas others were largely unaffected. These heterogeneous trajectories and mental health outcomes associated with the same stressor highlight the influence of risk factors and protective mechanisms. Among the factors that are typically associated with greater vulnerability to negative mental health outcomes are younger age, living alone, financial insecurity, unemployment, limited access to social support resources, and preexisting physical or psychiatric illness (Ahrens et al., 2021). Several studies (Agha, 2021; Zhou et al., 2020) have also investigated the relationship between stressors and protective factors (e.g., social support, active problem-solving, and positive cognitive reappraisal) and their effect on mental health. In stress research, these protective factors are said to operate through certain pathways, namely a health-sustaining, stress-reducing, or mediating pathway (Pretorius, 2020). For example, the health-sustaining pathway suggests that the effect of a protective factor (e.g., social support or problem-solving ability) on mental health is independent of the level of the stressor. By contrast, the stress-reducing pathway suggests that protective resources reduce or buffer the impact of stressors on PWB. Finally, the mediating pathway suggests that protective factors are a mechanism through which the stressor influences the mental or physical health outcome (Pretorius, 2020).
In this study, we focused on the construct of fortitude, which is defined as the psychological strength required to manage adversity and to stay well and is derived from positive or fortigenic appraisals of self, family, and supportive others (Pretorius & Heyns, 1998). To assess the levels of fortitude, a questionnaire called the Fortitude Questionnaire (FORQ; Pretorius & Heyns, 1998) was developed. Since its development, mounting evidence has been reported regarding the role of fortitude as a protective resource among diverse population groups facing a range of stressors, including adolescents living in contexts of adversity (Pretorius et al., 2016), young college students exposed to traumatic events (Padmanabhanunni & Wiid, 2022), and health care workers caring for patients with Alzheimer’s disease (Heyns et al., 2003). In a recent systematic review (Pretorius & Padmanabhanunni, 2021b) assessing 20 years of empirical research on the FORQ, a consistent relationship was identified between fortitude and the indices of PWB. In the present study, our goal was to extend this effort by using a meta-analytic approach to statistically integrate existing studies assessing the relationship between fortitude and PWB.
Method
We conducted our meta-analysis in terms of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Moher et al., 2009). However, no protocol was registered because a systematic review has already been published (Pretorius & Padmanabhanunni, 2021b).
Search strategy
We focused on a quantitative synthesis of the results of published studies regarding the relationship between fortitude and PWB. To identify suitable studies for the period between January 1999 and May 2022, we used Google Scholar, PubMed, Academic Search Premier, Sabinet African Journals, EBSCO Open Access Medical and Health Collection, Academic Search Complete, and UKWAZI (the local library search engine). The review period was selected due to the FORQ having been developed in 1998 and the first published use of the instrument was reported in 1999. Given our previous experience, we limited the search terms to ‘fortitude questionnaire’, ‘fortitude scale’, and ‘FORQ’, because using the term ‘fortitude’ resulted in studies from a wide variety of disciplines.
Eligibility criteria and screening process
The abstracts of the articles were independently examined by all three authors to identify the articles eligible for inclusion. An article was deemed eligible for inclusion if it was published in either English or Afrikaans, involved the FORQ as a total scale and not as a selected subscale, and reported on the relationship between fortitude and the indices of PWB. Full-text articles were obtained if the abstract indicated that the article in question met the inclusion criteria. If any doubts were raised, the full-text article was also obtained to verify whether the article met the eligibility criteria. Snowballing (i.e., searching the reference lists of the selected articles) was also used.
Assessment of methodological quality
All of the extracted studies were independently assessed for methodological quality by the three authors. The following criteria, obtained from the Observational Study Quality Evaluation (Drukker et al., 2021) tool, were used: random sampling, a sample size greater than 85, assessment of the independent variable, assessment of the dependent variable, an explicit statement regarding the treatment of missing data, and a description of the statistical analysis. Generally, a sample size greater than 85 ensures 80% power for detecting a medium effect size at an alpha level of .05 (Cohen, 1992). Here, a study was allocated a score of 1 if random sampling was used, if the sample size was greater than 85, if the study reported on the treatment of missing data, and if the statistical analysis was fully described. Regarding the assessment of the dependent and independent variables, a study was allocated a score between 1 and 3 if standardised instruments were used, if the reliability of the instrument was reported, and if the reliability was at a satisfactory level (α > .70). Thus, the ratings ranged between 0 and 10. After we provided the independent ratings, we discussed and resolved the rating differences between us.
Statistical analysis
The meta-analysis was conducted using the packages ‘metafor’ (Viechtbauer, 2010) and ‘robumeta’ (Fisher & Tipton, 2015) in R software (R Development Core Team, 2015). A random-effects model was used for the analysis. The heterogeneity of the effect sizes was examined using the Q-statistic, I2 statistic, and τ2 (tau squared). The correlation coefficients reported in the studies were converted into Fisher’s Z, and a forest plot was used to visually present the effect sizes. Publication bias was visually examined using a funnel plot and Egger’s regression test (Egger et al., 1997). However, Quintana (2015) suggested that the funnel plot and Egger’s regression test are tests of small study bias, which may include publication bias. He instead suggested that weighting studies in terms of their likelihood of being published is an alternative way of testing for publication bias. This was therefore performed using the weight function in R software. The potential moderating role of age and methodological quality was also examined through the use of regression plots of the relationship between the moderators and the correlation coefficients. In addition, the statistical test, model sum of squares (QM), was used to evaluate if the regression coefficient was statistically significant. Several studies have reported more than one correlation coefficient. Hence, robust variance estimation (RVE) was used to account for effect-size dependencies (Hedges et al., 2010). Because both positive and negative indicators of PWB have been reported, a subgroup analysis was performed to examine whether a difference existed in the effect between studies using positive and negative indicators. This subgroup analysis was performed using Meta-Essentials version 1.3 (Suurmond et al., 2017). Moderator plots (Figure 4) were also generated using Meta-Essentials.
Results
Studies extracted
Our search yielded an initial pool of 190 articles. In total, 104 articles were found to be duplicated across the databases, 12 articles were dissertations published in journals (i.e., also duplicates), 15 articles referenced the FORQ only, 37 articles did not focus on PWB, and 9 articles used only the subscales of the FORQ. The PRISMA flow diagram detailing the search process is presented in Figure 1.
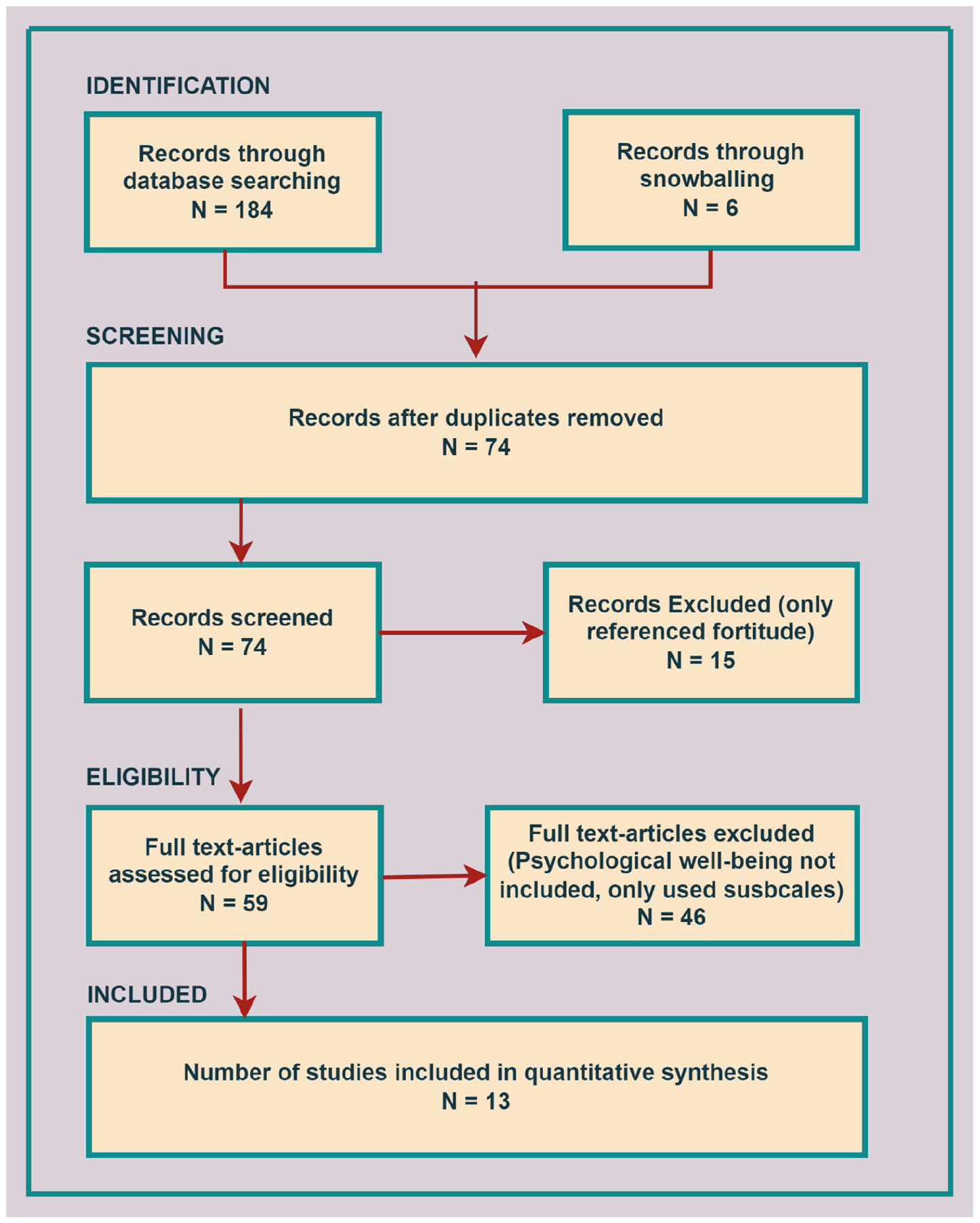
PRISMA flow diagram of the extracted studies.
The characteristics of the studies extracted and used in the meta-analysis are reported in Table 1. As shown in the table, 13 studies reporting 35 correlation coefficients between fortitude and the indices of psychological distress were included in the meta-analysis. The mean age across the 13 studies was 26.56 (SD = 8.89, range: 15.10–44). The median sample size was 263 (range: 26–1480). In total, 15 effect sizes (42.9%) were related to negative indicators of PWB, whereas 20 effect sizes (57.9%) were related to positive indicators.
Studies extracted for the meta-analysis.
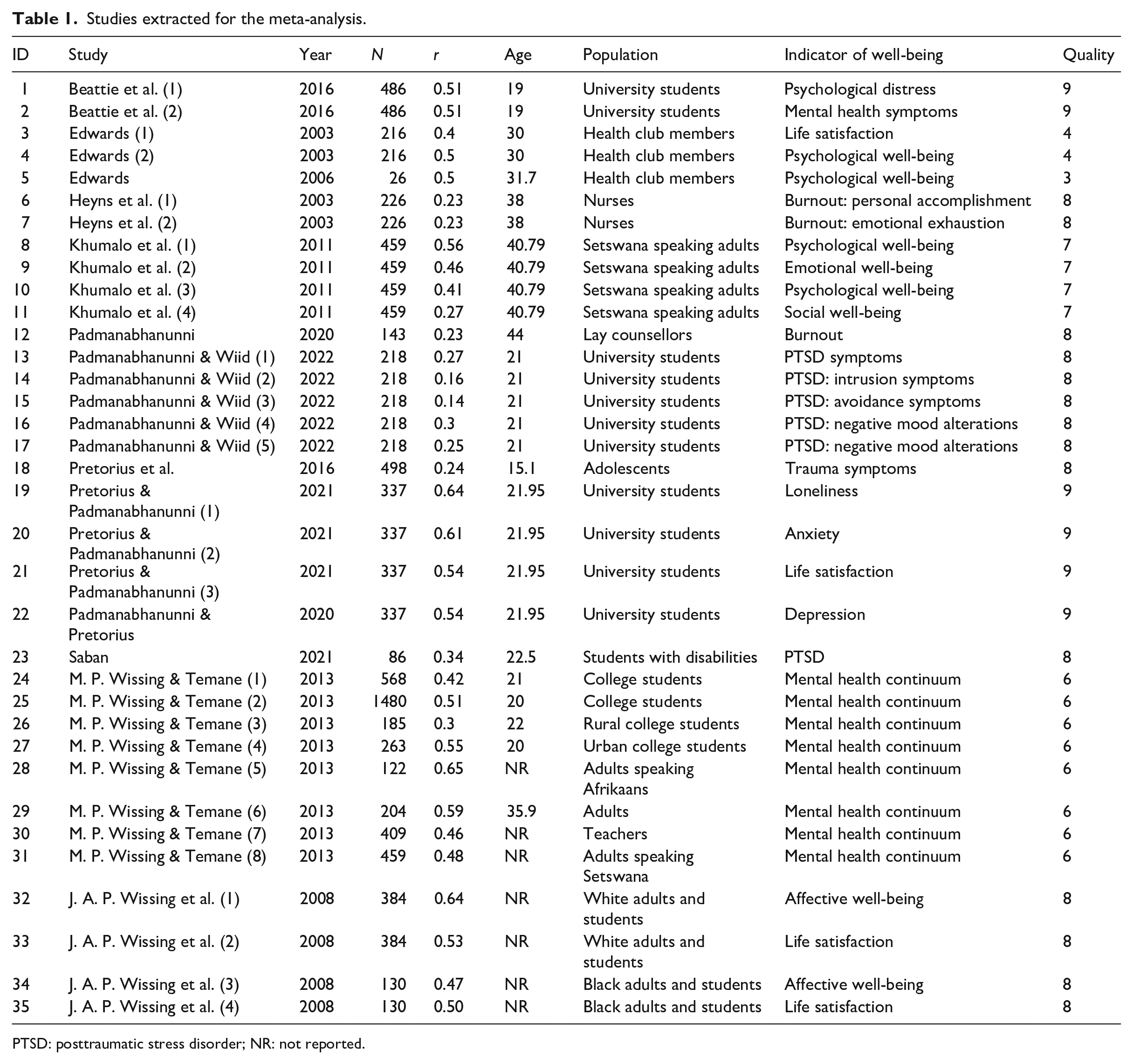
PTSD: posttraumatic stress disorder; NR: not reported.
Heterogeneity of effect sizes
The heterogeneity indices indicated a large heterogeneity in the effect sizes (Cochrane’s Q = 303.71, p < .001). Because the Q-statistic is sensitive to the sample size (Higgins et al., 2003), the I2 statistic and τ2 were also considered. Hence, both I2 = 90.31%, 95% confidence interval (CI) [84.81, 94.40] and τ2 = .029, 95% CI = [.017, .052] provided evidence of heterogeneity. Regarding I2, the literature suggests that an I2 value greater than 75% is an indicator of high variance (Higgins et al., 2003). To determine which studies contributed most to heterogeneity, the Baujat plot (Baujat et al., 2002) shown in Figure 2 was used.

Baujat plot indicating studies that contributed to heterogeneity.
Each study was identified by its identification number in the Baujat plot, and the effect sizes that contributed most to heterogeneity were located in the upper-right corner of the plot. Here, effect sizes 14 and 15 (Padmanabhanunni & Wiid, 2022), effect size 32 (J. A. P. Wissing et al., 2008), effect size 19 (Pretorius & Padmanabhanunni, 2021a), and effect size 28 (M. P. Wissing & Temane, 2013) contributed most to the heterogeneity of the effect sizes. The package ‘metafor’ also provided an indication of whether any study disproportionally influenced the overall effect size. None of the studies was identified as a significant influencer, and the study weights ranged between 1.21% and 3.28%.
Combined effect size
A forest plot of the various effect sizes is presented in Figure 3. This plot visually confirms the study heterogeneity, as indicated by the heterogeneity statistics. The overall effect size resulting from the random effects is also represented by a polygon at the bottom of the forest plot (r = .44, 95% CI = [.39, .4], p < .001). The sizes of the squares of the various effect sizes indicate the contribution of each effect size to the combined effect size.
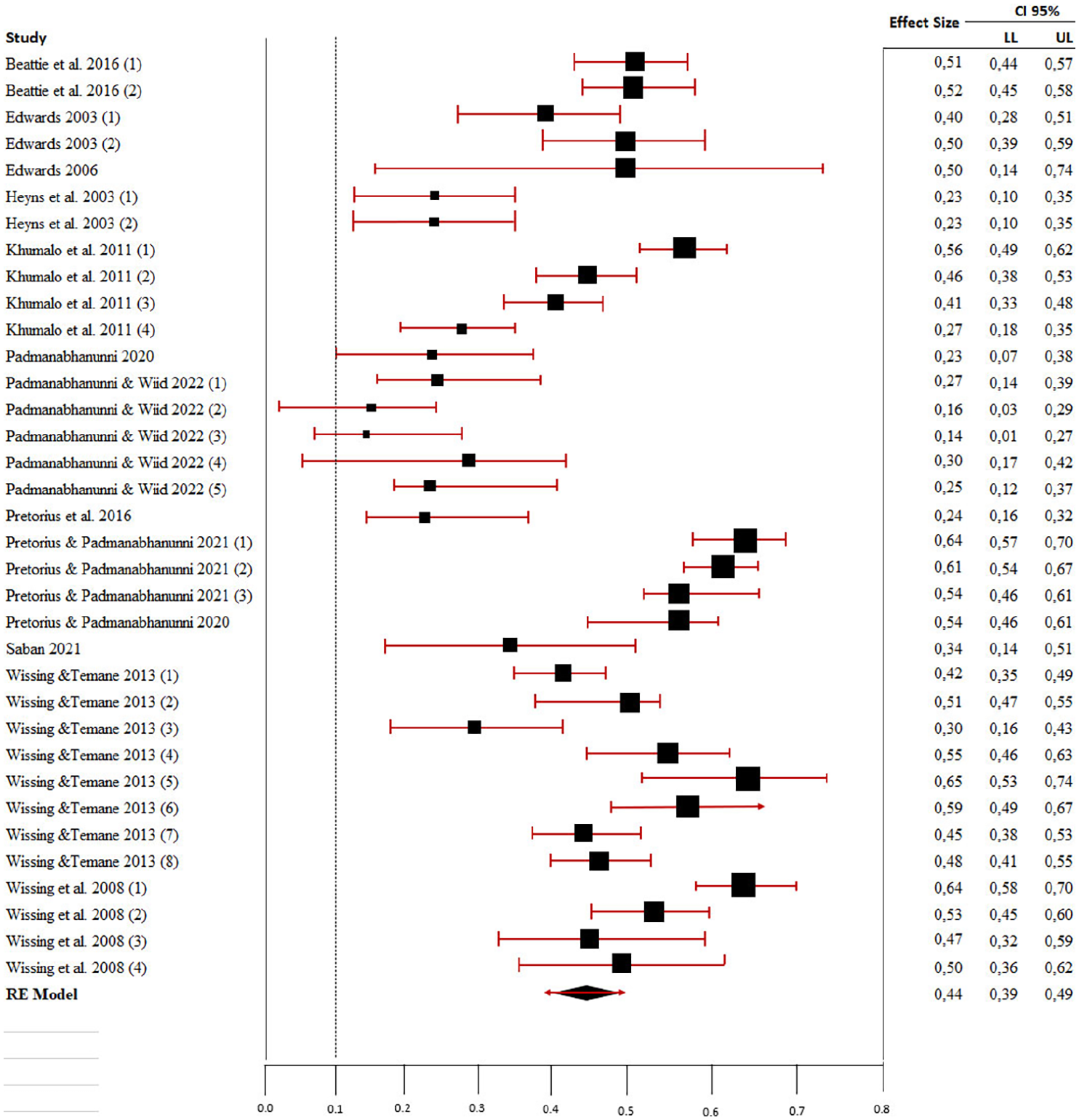
Forest plot of the relationship between fortitude and the indices of psychological well-being.
The role of potential moderator variables
To examine the potential effect of age and methodological quality on the dataset, a moderator analysis was performed. The regression plots of age and methodological quality as moderators are presented in Figure 4(a) and (b), respectively.
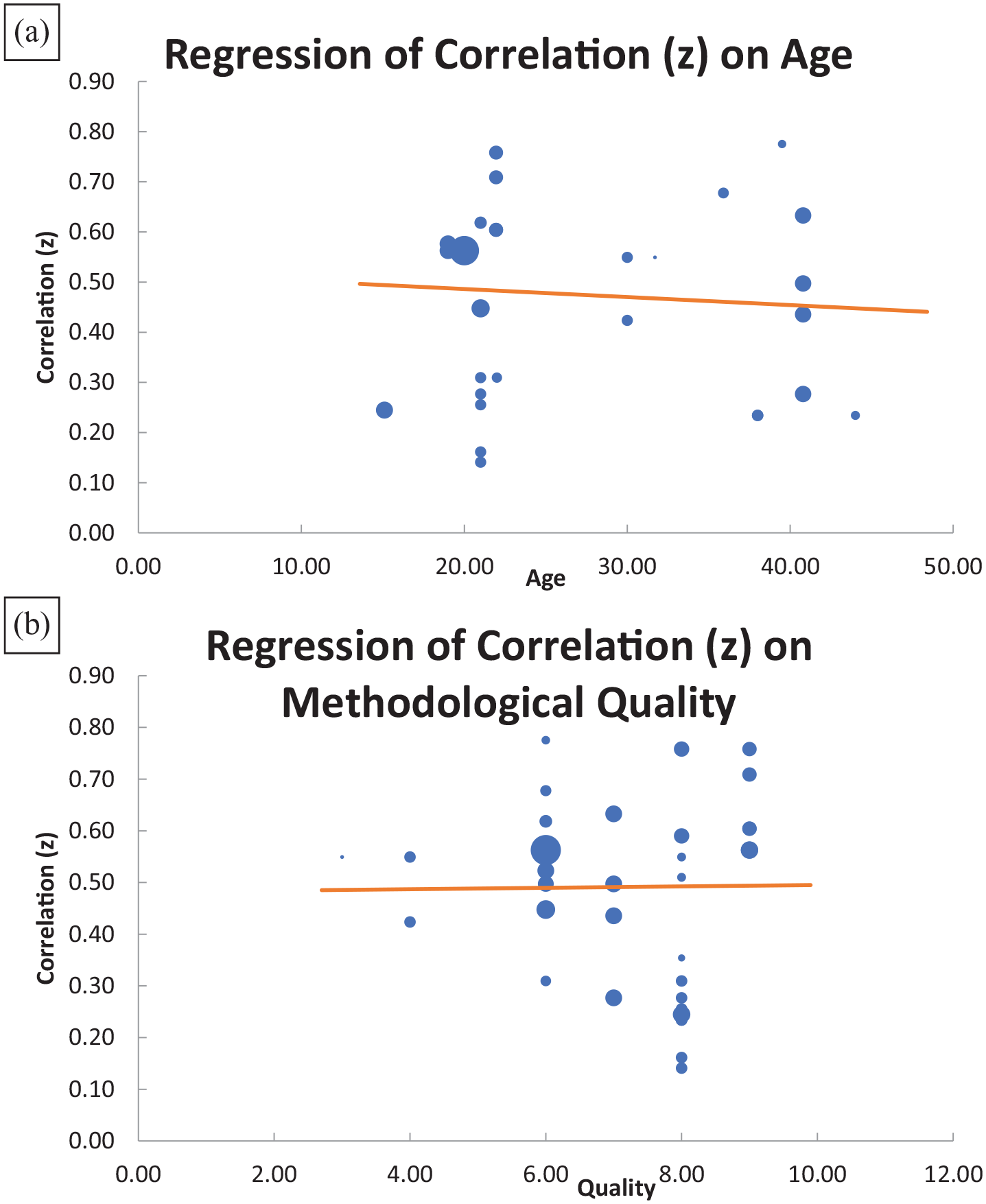
Plot of age and methodological quality as moderator variables.
Visual inspection of the regression plots suggested that neither age nor methodological quality had an effect on the effect sizes. This was confirmed by statistical tests of significance: age, QM = .163, p = .69; methodological quality, QM = .101, p = .75.
Subgroup analysis
We hypothesised that two distinct subgroups existed in the 35 effect sizes, namely those reported in relation to positive and negative indicators of well-being. A forest plot of the two subgroups is presented in Figure 5.
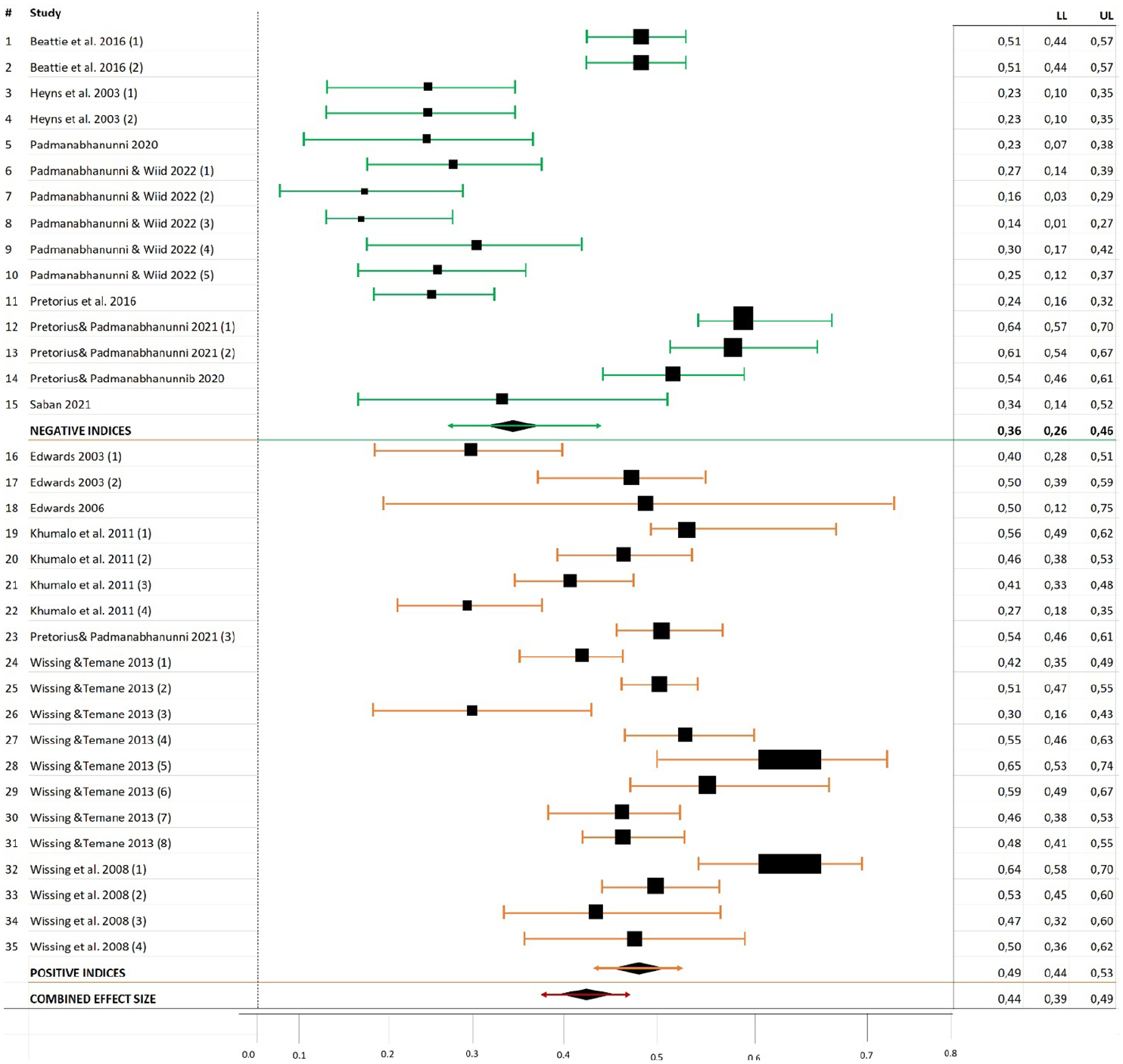
Forest plot of subgroups: positive and negative indicators of well-being.
As shown in Figure 4, the combined effect size for positive indicators (r = .49, 95% CI = [.44, .53]) was higher than that for negative indicators (r = .36, 95% CI = [.26, .46]). In addition, the heterogeneity statistics indicated heterogeneity in both subgroups: positive indicators, Q = 92.49, p < .001, I2 = 79.46%, τ2 = .01; negative indicators, Q = 176.85, p < .001, I2 = 92.08%, τ2 = .04.
Assessing publication bias
We examined publication bias visually with a funnel plot and statistically with Egger’s regression test and weighting studies. The funnel plot is presented in Figure 6.
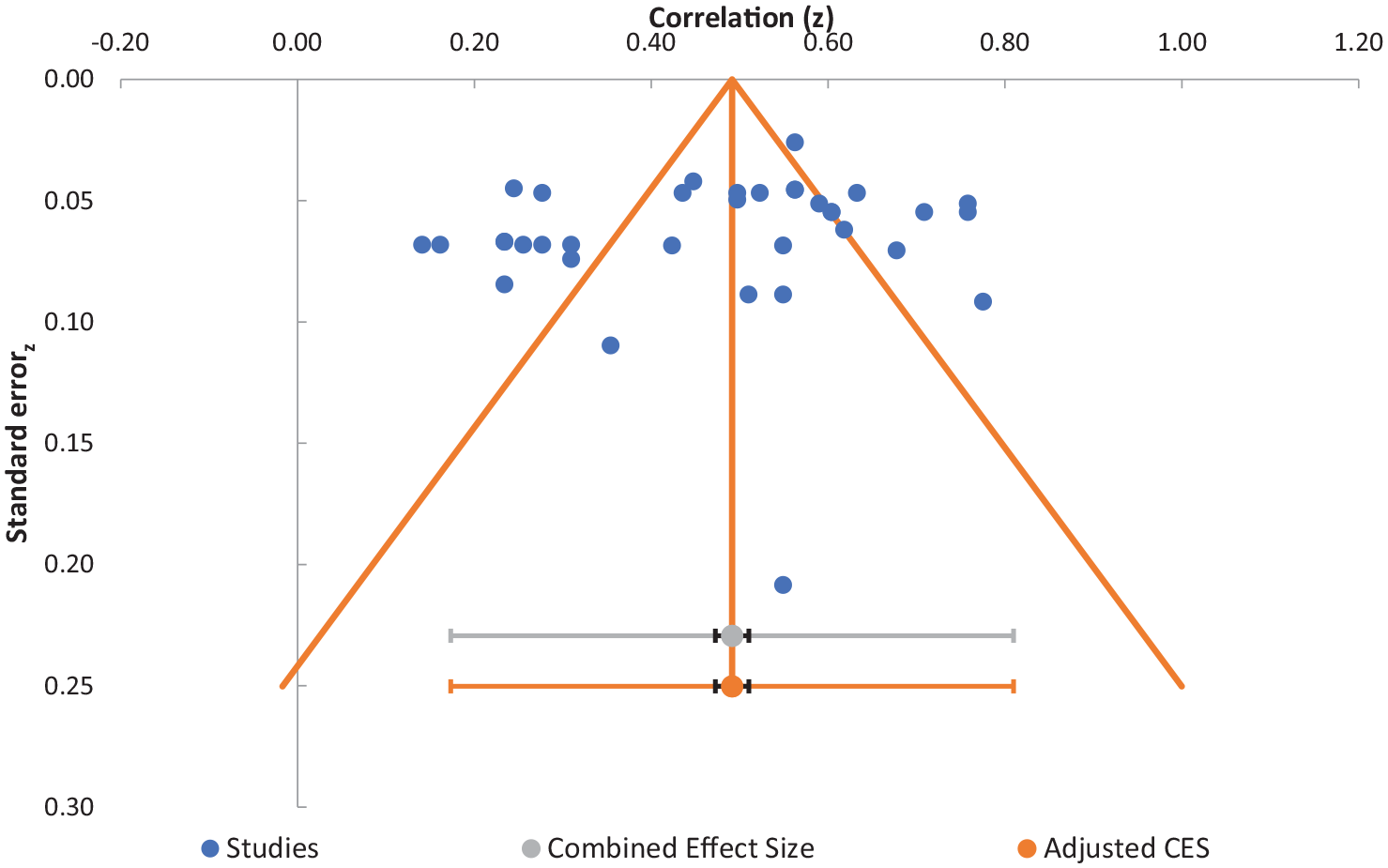
Funnel plot of the assessment of symmetry and publication bias.
Visual inspection of the funnel plot provided evidence of symmetry, because the 35 effect sizes were almost equally spread around the combined effect size, denoted by the vertical line. The evidence of symmetry was confirmed by Egger’s regression test, which was not significant (z = −.660, p = .51). The weighting of the studies also did not significantly affect the point estimate. The estimates were .471 (95% CI = [.410, .531]) in the unadjusted model (in which the studies were not weighted) and .446 (95% CI = [.392, .499]) in the weighted model.
Effect size dependencies
As indicated in Table 1, the 35 effect sizes were reported in 13 different studies. To account for the dependencies of effect sizes, RVE was used with a correction for small sample sizes, which resulted in a slight increase in the overall effect size (.508, 95% CI = [.425, .592]).
Discussion
In a scoping review of 20 years of empirical research on the FORQ, Pretorius and Padmanabhanunni (2021b) concluded that the FORQ is a versatile measure that has been applied in different cultural contexts and among a wide range of population groups and has demonstrated sound reliability. In the present study, our goal was to extend this work by using a meta-analytic approach to statistically integrate existing studies assessing the relationship between fortitude and PWB.
Fortitude has been identified as a salient aspect of mental health and well-being, and a large number of studies have confirmed that the presence of fortitude is associated with positive mental and physical health outcomes (for an overview, please refer to Pretorius & Padmanabhanunni, 2021b). Despite the growing body of research investigating fortitude and various indices of PWB, to the best of our knowledge, no meta-analytical studies have yet provided an overall mean estimate of the relationship or quantified effect size variance to explain differences in effects across studies. This type of research is considered critical in gaining broader insights into the strength of the relationship between fortitude and PWB and understanding the factors that underlie the differences in the direction and magnitude of effects within and across studies of these variables (Noble et al., 2022).
The current meta-analysis yielded a medium effect size, and the effect sizes were larger for positive than for negative indicators of well-being. This agrees with the conceptualisation of fortitude as a fortigenic construct (Pretorius & Heyns, 1998). The medium effect size observed may be due to the methodological differences in studies including small sample sizes, which may have contributed to some bias in the interpretation of the findings. Our results indicated a large heterogeneity in the reported effect sizes. In addition, neither age nor methodological quality affected the observed effect size, and no evidence of publication bias was observed.
Overall, the results of the meta-analysis regarding fortitude and PWB can be considered in relation to its current implications for intervention. Globally, people continue to grapple with the impact of COVID-19 (Şimşir et al., 2022). Although successive waves of the pandemic have been associated with increased access to vaccination and personal protective equipment and a greater knowledge of how to treat this disease, a large percentage of people continue to experience adverse mental health outcomes because of the prolonged social isolation, economic restrictions, continued fear of COVID-19, unresolved grief, and difficulties in accessing mental health care (Padmanabhanunni et al., 2022; Pretorius & Padmanabhanunni, 2021a; Veer et al., 2020). Numerous empirical studies (e.g., Aknin et al., 2022) have documented heightened levels of anxiety, depression, loneliness, and posttraumatic stress reactions among the general population. Other studies have also documented increases in psychosocial challenges, such as gender-based violence and substance abuse (Usher et al., 2021). Therefore, identifying the factors that can protect people against adverse mental health outcomes is urgently required.
Fortitude represents a salient protective factor in mitigating psychological distress. The construct of fortitude is grounded in the theory of cognitive appraisal, and several studies conducted during the pandemic have underscored the salience of cognitive factors in promoting adaptation. For example, Veer et al. (2020) indicated that a positive appraisal style is a strong predictor of coping and resilience. Hence, a potentially effective approach for promoting adaptation is to alter potentially unhelpful patterns of appraisal, which represents a central component of evidence-based mental health interventions, such as cognitive behavioural therapy. Growing evidence has been reported regarding the accessibility and usability of digital cognitive behavioural mental health interventions, particularly those delivered via mobile phone applications (Jarvis et al., 2019). These interventions can be adapted to focus on amplifying fortigenic appraisals and thereby promote adaptation and coping. Brief digital cognitive behavioural therapy interventions have been found to be effective in improving coping and resilience in highly stressful situations (Ang et al., 2022; Weiner et al., 2020). These interventions have also been found to inhibit the emergence of psychological disorders, including depression and anxiety (Weiner et al., 2020). Within the context of the pandemic, digitally delivered interventions have the advantage of circumventing challenges in access to mental health care, which arise because of the social-distancing mandates, quarantine requirements, and stay-at-home orders.
Although the present study provided strong evidence regarding the association between fortitude and PWB, some limitation should be noted. Although no signs of publication bias were observed in the studies included in the analysis, some studies may have not been included because they were not listed in the databases selected. These incomplete data may have led to an overestimation of the effect size.
Conclusion
The current meta-analysis provides robust evidence regarding the association between fortitude and PWB. This has implications for promoting mental health in light of COVID-19 and suggests that interventions aimed at building fortitude can be leveraged to mitigate psychological distress.
Footnotes
Acknowledgements
The authors thank John Thwaits, a graphic designer, for helping with the graphs.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.