
Abstract
National strategies to manage COVID-19, including lockdown, have caused significant disruption to student learning and to the ways that students engage with staff and peers. The transition to online learning, alongside common anxieties associated with the disease itself, was likely to have affected student mental health. This study explored psychology student mental health experiences during Lockdown Phase 3 at the University of the Witwatersrand. A convenience sample of 160 first- and second-year psychology students completed a questionnaire consisting of the General Mental Health Scale, the Hospital Anxiety and Depression Scale, the Burnout Measure, the Brief Coping Orientation to Problems Experienced, the Connor–Davidson Resilience Scale, and the Generalised Self Efficacy Scale. In addition, six open-ended questions asking students about their experiences and support during this time were included. Descriptive statistics were used to analyse quantitative data, whereas content and thematic analysis was used for the open-ended responses. Results indicated that students’ scores were not elevated on the mental health scales. However, the thematic analysis of responses revealed significant concerns with regard to psychological wellbeing, online learning, and home dynamics. These are discussed with a view to providing recommendations for supporting students in circumstances that may require emergency remote teaching.
Introduction
Mental disorders constitute the highest burden of disease among young people worldwide; depression, in particular, is identified as the largest single contributor to the burden of disease globally (World Health Organization [WHO], 2001, 2004). There is also growing international concern about the reported poor mental health of university students (Cvetkovski et al., 2019), especially because university students may have to leave home to study away, experience new social environments, are subjected to increased academic pressure, and may feel extreme financial pressure (Bantjes et al., 2019). Also, the transition from high school to university may place students under stress, as they need to learn how to study in a new academic environment that usually necessitates more independence than was required in high school (Parker et al., 2004). Research is consistently finding that approximately one third of students report a mental disorder in the preceding 12 months (Alonso et al., 2018; Auerbach et al., 2016).
South African student samples reveal similar rates, with depressive and anxiety disorders most commonly reported (Bantjes et al., 2019). At higher risk are female students, students who are not heteronormative, and those with a disability (Bantjes et al., 2019), a finding echoed among psychology students (Lipson et al., 2016). Mental illness significantly impedes social adjustment to university and academic attainment and is linked to increased suicidality (McLafferty et al., 2017; Mortier et al., 2015).
Undergraduate humanities students, and in particular students of psychology, are reported to experience higher levels of anxiety, depression, and suicidal ideation (Lipson et al., 2016). While many psychology students report previous personal mental health problems or mental health problems in family members as motivators for studying psychology, some also find the content and delivery of taught psychology courses to exacerbate pre-existing symptoms and induce concerns about treatments (Woof et al., 2019). In the South African context, students are already navigating multiple challenges such as difficulties with concentration, finances, depression, sleeping, family and personal relationship problems, anxiety, and stress around exams (Schreiber, 2007). This appears to be exacerbated by ‘high crime rates, widespread poverty and illness, with abuse and unemployment’ (Schreiber, 2007, p. 553). This aforementioned context may contribute to findings that the prevalence rates for mental illness among South African students may be higher than their peers in other countries (Bantjes et al., 2019). Moreover, particular student stressors include concerns around academic performance, pressure to succeed, and postgraduation plans (Beiter et al., 2015) as well as reduced academic performance, impaired memory, low self-esteem, exhaustion, and intention to terminate their studies (Jacobs & Dodd, 2003). Socioeconomic status has been associated with increased risk for depressive symptoms (Othieno et al., 2015), and higher stress levels have been associated with more substance use (Oduaran & Akanni, 2019). Poor mental health literacy and high levels of stigma appear to exacerbate the situation (Kutcher et al., 2019). For students of psychology, this stigma may be exacerbated because they may worry that they will be perceived as potentially impaired future providers of psychological services (Rummel, 2015) and fear professional isolation as well as stigma around help-seeking behaviour (El-Ghoroury, Galper, Sawaqdeh & Bufka, 2012). However, Mostert and Pienaar (2020) report that social support from parents and significant others may mitigate some of the burnout effects and possible risk of students abandoning their studies. University students are shown to be at risk particularly around times of transition, and student mental health is shown to decrease significantly around times of major transition in their student careers (Cvetkovski et al., 2019).
National strategies to manage COVID-19, including lockdown, have caused significant disruption to the way people were used to living their lives and the resultant restrictions, especially in the stricter lockdown levels, which were characterised by people being required to learn and work from home and to limit social activities. These restrictions were disruptive to student learning and to the ways that students engage with staff and peers. There has been a notable loss of contact learning and social aspects of university life. Rapid adaptation to the temporary use of distance or online learning platforms has been required. The transition to emergency remote teaching, alongside common anxieties and fears associated with the disease itself, is likely to have affected student mental health. This viral pandemic has potentially added a further dimension to students’ experiences and mental health.
This offers a unique context to investigate pertinent issues regarding psychology student health experiences. Thus, this study aimed to investigate the mental health of students as well as self efficacy, resilience, and coping strategies using appropriate scales. Five open-ended questions were incorporated, asking students about their experiences during the pandemic and lockdown, their experiences of working on university work at home since the COVID outbreak started in South Africa, their support mechanisms, challenges they were experiencing, and their suggestions for the university that would improve working from home.
Research questions
(a) What are the levels of physical and psychological health, resilience, and coping among psychology students at the University of the Witwatersrand (Wits) during the COVID-19 pandemic?
(b) What are the health and study experiences of students during COVID-19?
Method
Research design
A nonexperimental, cross-sectional design was used for this study where students completed an online questionnaire on the SurveyMonkey platform. Data collection commenced on 1 June 2020 and closed on 30 June 2020. Hence, data were collected during Lockdown Phase 3 in South Africa. At this time, the university had already been just over 1 month into emergency remote teaching. Students were completing or had just completed their first semester examinations when they responded.
Lockdown Level 3 (1 June 2020 to 17 August 2020) saw the easing of restrictions to allow for the opening of the economy. All high-risk economic activities such as entertainment, sports, conferences, and events were prohibited. Individuals were required to wear a face mask in public spaces, allowed to travel to and from work, and attend funerals and places of worship, provided strict health protocols were adhered to and capacity was limited to 50 individuals. Exercise was permitted between 6:00 a.m. and 6:00 p.m., provided that it was not done in groups. This was different to Lockdown Level 4 (1 to 31 May 2020) where movement was more restricted. Only certain industries were allowed to reopen, funerals could only be attended by immediate relatives, places of worship were closed, and exercise was only allowed between 6:00 a.m. and 9:00 a.m. It was also very different to Lockdown Level 5, the strictest Lockdown to date, which started on 26 March 2020 and ended on 30 April 2020. In Level 5, all South Africans were required to stay at home unless they worked in an essential service sector, were purchasing essential goods, seeking medical services, or collecting a social grant (South African Government, 2020).
Participants
All first- and second-year students in the psychology department received the invitation to participate. Participation was voluntary and students remained anonymous unless they chose to provide their details for further interviews. Hence, a nonprobability convenience sample of 112 first-year and 48 second-year students completed the questionnaire. This was a low response rate (12.8%) as there are 691 registered first-year students and 551 registered second-year students. Nonetheless, the feedback provided has been very useful in terms of understanding student experiences and mental health during COVID-19. Before combining these two groups for analyses, a one-way analysis of variance (ANOVA) was run across the year of study for all the variables concerned and there were no significant differences between the two groups on the variables studied. Students in their final year and postgraduate studies were not included in this study as there were significant differences between the groups, which were beyond the scope of this article.
The demographic characteristics of the sample appear in Table 1. The majority of participants in the sample primarily identified as female (n = 142, 88.8%), Black African (n = 84, 52.5%), Christian (n = 102, 65.0%), and spoke an African language (n = 79, 49.38%) or English (n = 74, 47.4%) as their home language. Most of the participants reported experiencing financial worry some of the time (n = 66, 41.5%), were not married (n = 159, 99.4%), were not in a relationship (n = 126, 78.8%), lived with immediate family (n = 122, 77.71%), had no children (n = 153, 97.5%), and reported having not been diagnosed with a chronic condition (n = 115, 72.8%). Participants were aged between 18 and 22 (M = 19.12, SD = 1.036) years.
Demographic information for participants.
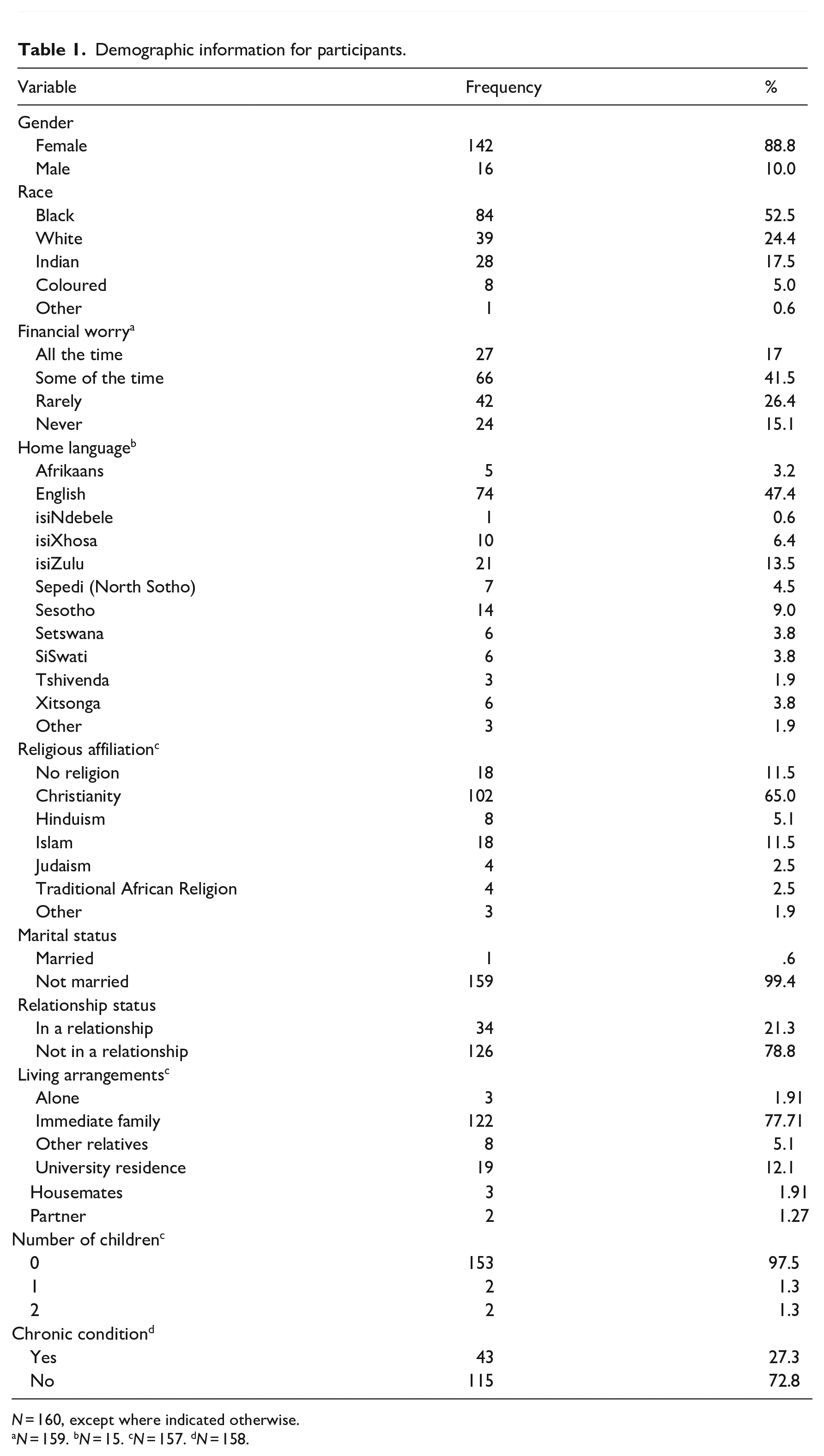
N = 160, except where indicated otherwise.
N = 159. bN = 15. cN = 157. dN = 158.
Instruments
A questionnaire consisting of a demographic section, several mental health screening instruments, and five open-ended questions was used. The instruments chosen for the study are screening assessments and were not used diagnostically. The demographics section requested information on gender, age, race, socioeconomic status (more specifically – level of financial concern/worry), year of study, family and other support structures, and whether the student suffered from a health condition prior to COVID.
General mental health
The Global Mental Health Scale (GMH-4) of the PROMIS Global Health Instrument (v 1.2) was used to assess overall mental health (Hays et al., 2017). All four items in the GMH-4 scale have a 5-point response format: Items 1 to 3 have the same anchors (excellent to poor) and Item 4 has a unique anchor (never to always). The GMH-4 has been shown to be reliable (Hays et al., 2017) and valid (Katzan & Lapin, 2018). The GMH-4 evidenced a .75 internal consistency reliability coefficient for this study.
Hospital Anxiety and Depression Scale (HADS)
The HADS was used as a measure of depression and anxiety. Although it was initially developed for use with patients in hospital settings, it has been validated in community settings (Snaith, 2003). The scale comprises two subscales, one assessing anxiety and one assessing depression. Each subscale consists of seven items that are rated on a 4-point scale (0–3), with unique anchors for each item. The HADS has been validated across multiple languages and settings (Bjelland et al., 2002; Herrman, 1997), including with patients diagnosed with HIV/AIDS in South Africa (Wouters et al., 2012). An internal consistency reliability coefficient of .79 was found for the depression subscale and .83 for the anxiety subscale.
Burnout
The Burnout Measure–Short Version (BMS) was used to assess burnout in participants. The BMS measure is a shortened version of the Burnout Measure by Pines and Aronson (1988). This scale contains 10 items addressing the frequency of experiencing symptoms of emotional, mental, and physical exhaustion. Participants indicated the extent to which the items (e.g., tired, trapped, helpless) corresponded to how they felt about their work/studies, rated on a 7-point Likert-type scale (1 = never, 7 = always). The measure has been found to be reliable and has been successfully used in the South African context with a coefficient alpha of .82 (Fatoki, 2019). In this study, a Cronbach’s alpha coefficient of .89 was obtained for the BMS.
Coping skills
The Brief Coping Orientation to Problems Experienced (COPE) Inventory was used to assess coping skills. The inventory consists of 28 statements, with two items each making up one of 14 scales of coping, namely, self-distraction, active coping, denial, substance use, use of emotional support, use of instrumental support, behavioural disengagement, venting, positive reframing, planning, humour, acceptance, religion, and self-blame. Participants are asked to rate the degree to which they use each coping strategy to deal with a particular stressful event. Participants using the inventory, score themselves on a 4-point Likert-type scale (1 = I haven’t been doing this at all, 4 = I’ve been doing this a lot). For the purposes of the proposed study, Item 19, that is, ‘going to the movies’ as an example of coping was removed as it was not applicable in Lockdown Level 4. The scale has been used in South Africa with good internal consistency reliability (Kotzé et al., 2013). Cronbach’s alpha coefficients ranged between .62 and .89 for the coping subscales, except for the venting (α = .15), self-distraction (α = .32), and active coping (α = .57) subscales.
Resilience
The Connor–Davidson Resilience Scale (CD-RISC) is a test that measures resilience or how well one is equipped to bounce back after stressful events, tragedy, or trauma (Conor & Davidson, 2003). The CD-RISC-10 (Campbell-Sills & Stein, 2007) was used for this study (Vaishnavi et al., 2007). Items are answered on a Likert-type scale of 0 to 4: not true at all (0) to true nearly all of the time (4) with scores ranging from 0 to 40. The measure has adequate test–retest and internal consistency reliability as well as good construct validity evidence (Vaishnavi et al., 2007). Previous studies in Nigerian student and South African adolescent populations have found reliability coefficients of .81 and .93, respectively (Aloba et al., 2016; Jørgensen & Seedat, 2008). In this study, a Cronbach’s alpha coefficient of .90 was found for the resilience scale.
Self-efficacy
The Generalised Self-Efficacy Scale (Jerusalem & Schwarzer, 1995) assesses individuals’ beliefs in their own abilities to respond to novel or difficult situations. Items are answered on a 4-point Likert-type scale (1 = not at all true, 4 = exactly true). Items include statements such as ‘When I am confronted with a problem, I usually find several solutions’. This scale demonstrates satisfactory internal consistency of .86 and test–retest reliability of .75 after 12 months (Wu et al., 2004). Internal consistency reliability for this study was good with a Cronbach’s alpha coefficient of .90.
Self-report, open-ended questions
Five open-ended questions about an individual’s experience of COVID-19 were asked at the end of the questionnaire. These focused on students’ experiences, particularly their mental health experiences, during the lockdown; their experiences of working on university work at home; their support structures at home; the challenges experienced; and their needs in terms of support from the university.
Procedure
Students received notification about the study via an announcement using the Wits e-learning management system. The announcement included the link to the questionnaire on SurveyMonkey. Completion of the survey required minimal data and all students had received 10GB of daytime data and 20GB of night-time data from the university.
Ethical considerations
Ethical clearance was obtained from the Human Research Ethics Committee at the University of the Witwatersrand (Protocol No. H20/03/33). Students were informed about the aims of the study and the conditions of their participation by means of an information sheet. Students remained anonymous unless they provided details to be interviewed later. Students were provided with details for the free online and telephonic counselling services offered by the university and encouraged to use these if they felt overwhelmed.
Data analysis
Analysis was conducted on SPSS Version 26 (IBM Corporation, 2017). Descriptive statistics were used for demographic information and to determine levels of mental health, coping, and resilience in the sample. Open-ended questions were analysed using content and thematic analysis (Braun et al., 2019).
Results
What are the levels of mental health, resilience, and coping among Wits psychology students during the COVID-19 pandemic?
From Table 2, it is evident that there were no elevations on any of the mental health scales. All the scales were within the expected ranges and normally distributed. Students made use of primarily approach rather than avoidant coping strategies, except for the self-distraction coping strategy that was the second most dominant coping strategy used by students. Resilience and self efficacy scores were also within the expected ranges and normally distributed.
Descriptive statistics.
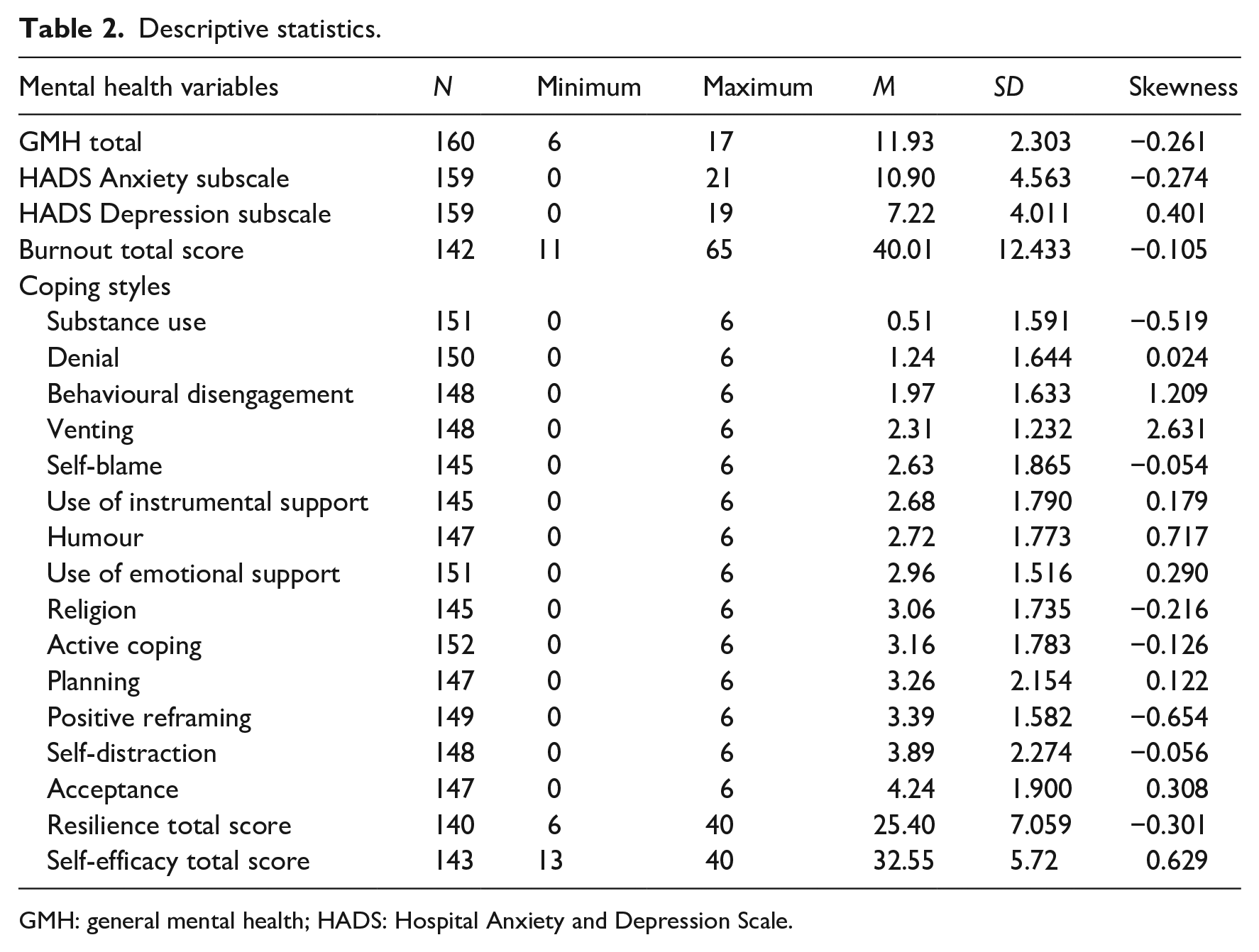
GMH: general mental health; HADS: Hospital Anxiety and Depression Scale.
What are the health and study experiences of students during COVID-19?
While a minority of students reported no impact or certain positive impacts, such as the slower pace of lockdown, increased time to reflect, and the opportunities for closeness with family, the vast majority reported experiencing some challenges. Broadly, these were best represented by three themes: (1) psychological well-being; (2) challenges linked to online learning; and (3) home dynamics.
Psychological well-being
Emotional symptoms
Anxiety and fear emerged clearly. Students worried about the virus and becoming infected, their academic performance, and they particularly feared losing loved ones to the virus. Many students reported feelings of sadness and emotional exhaustion: Irritability was a fairly common response, linked to a tendency to withdraw socially. Many described feelings of numbness. This extended to their interpersonal relationships where many reported feeling detached. Some attributed their detachment to a lack of motivation to connect interpersonally and to a sense of apathy.
Many reported that increased time alone at home had resulted in ‘overthinking’ and excessive rumination about themselves and their histories. Over-eating, gaining weight, and a general unhappiness about this was also reported. Some students attributed their weight gain to a lack of exercise as a result of the national lockdown: This lack of exercise, in turn, appeared to contribute to more negative emotional states. Sleep disturbances also featured among the student responses. A number of somatic complaints were reported that were often linked to feeling stressed, anxious, and depressed like ‘Back pain, eye strain . . .’; ‘. . . my migraines [have] increase[d] in both frequency and intensity’; ‘. . . I have been having stomach cramps’; ‘I get headaches often and I feel tired most of the time’.
Feeling trapped
The words ‘trapped’, ‘stuck’, and ‘claustrophobic’ emerged as a significant theme in the student narratives. In some instances, this was related to the physical restrictions on movement associated with the national lockdown. In other responses, the ‘trappedness’ appeared related to a broader sense of helplessness, feeling overwhelmed, and lack of control over their own lives. A great deal of uncertainty about the future was expressed. This uncertainty about the future left some students feeling despondent and even hopeless.
Isolation
Many students struggled with the isolation that the national lockdown entailed, reporting feelings of loneliness. Students linked this lack of social contact to their negative emotional states. Some felt that the lockdown denied them access to social support. For some of the first-year students specifically, the loss of social experiences meant the loss of the much anticipated ‘first-year experience’: ‘My first-year experience has been cut short, I was unable to make friends on campus’.
Challenges of online learning
Responses to online learning were emotionally laden with the following words reflecting the difficulty that they experienced: stressful, strain, numbing, frustrating, heart-breaking, exhausting, mentally draining, burnout, fearful, trapped, madness, panicked, demotivated, overwhelmed, and discouraged. This difficulty seemed at times insurmountable: ‘I can’t do it. I can’t focus. I don’t feel like I’m learning anything. I feel overwhelmed. My mind feels full of thoughts of anything other than school. I really can’t do this’ (Participant 43). In addition to the impacts of emotional overwhelm on learning, a number of practical difficulties also emerged.
Difficulties understanding course material due to an absence of interaction
Some students experienced the lack of in-person learning as difficult. An absence of interaction with lecturers and other students was perceived as making understanding the course content more difficult, and some found it harder to ask questions via email and felt that this made grasping concepts much harder. This difficulty appeared exacerbated in first-year students who felt that the transition to online learning had impeded their adjustment from high school.
Time management challenges
The majority of students experienced difficulty managing their time: I have felt pushed to my absolute limit and then some more . . . I’m mostly falling behind and am unable to learn my work until it is assessment time because of the workload of subjects combined. I always feel like I’m neglecting at least one subject at a time. (Participant 115)
This struggle with time management was attributed to an increased workload, difficulties structuring the day, and multiple responsibilities as a result of being back home. The lack of structure associated with in-person classes appeared to contribute to this. The lack of structure was also perceived to exacerbate procrastination, the tendency to become distracted, and concentration difficulties.
Home dynamics
While some students experienced home as a supportive space, many experienced home as not conducive to study for a variety of reasons.
Multiple responsibilities
A portion of the responses indicated that students’ stress levels were exacerbated by increased exposure to their homes and family distress: ‘It has affected me emotionally because I’ve been experiencing a lot of tension between my parents’ (Participant 1). In addition to challenging interpersonal dynamics, sometimes the practicalities of home life presented challenges, such as a lack of space: ‘It’s hard to work at home because there is no study room or a quiet room where I can study and work whenever I want’ (Participant 144). Some students reported experiencing difficulty balancing studies and home responsibilities, which included helping younger siblings with online schooling: ‘It was a nightmare. I live in a household of 20 people I can’t really get a chance to touch my books. I try to wake up and do the work, but I will be tired because of chores and babysitting’ (Participant 82). Students found this continuous balancing exhausting and found their motivation and concentration to be adversely affected.
Infrastructural considerations
Limitations to infrastructure compounded the difficulty of working from home. There was reference to loadshedding (power cuts in South Africa by the national electricity supplier as a controlled option to respond to unplanned events to protect the electricity power system from a total blackout, Eskom, 2020), regular power cuts (over and above loadshedding), and internet connectivity issues: ‘I’ve had trouble with internet connection . . . Sometimes I breakdown because of inability to connect to the internet, which results to me being behind with so much work’ (Participant 158). Many areas outside of cities in South Africa still do have adequate infrastructure for students to access the internet even if students have access to data to connect. Insufficient funds to buy data to access online platforms for university work were also cited as a problem.
Support mechanisms
Support from close others (e.g., a parent, partner, friends) was the most frequently identified source of support. Most participants indicated that they received support from their immediate and/or extended family. However, some students reported having little or no support at all.
With regard to support from the university, a portion of the students experienced the university as supportive with regard to the provision of data, counselling services, and the overall support offered by lecturers and tutors. Students had some recommendations with regard to what the university could do to provide increased support. The majority of the students requested flexibility, largely with regard to deadlines for assessments; some desired more understanding from the university regarding challenges being experienced. Some students expressed a need for more data, more consistently, and some requested more access to lecturers and tutors. Some students indicated that the workload should be reduced for students. More access to counselling services and self-help material was recommended. A few students expressed a need to be back at the university residences.
Discussion
The results demonstrated differences between results obtained on the quantitative measures and on the qualitative responses. From the scales, it is possible to conclude that students self-reported as mentally healthy were using largely positive coping strategies and demonstrated adequate resilience and self efficacy. An examination of the qualitative responses particularly with regard to the emotional well-being theme indicated that there was a percentage of students experiencing symptoms of depression, anxiety, and burnout. However, this may have been missed in the quantitative analyses, more so due to the small sample size. Alternatively, the discrepancy in findings may indicate subclinical levels of emotional distress, perhaps appropriate to the encountered stress, but not tapped by the quantitative instruments. The qualitative experiences of mental health are congruent with those found in the literature with regard to depression, anxiety, and burnout as well as overall mental health (Bantjes et al., 2019; Cvetkovski et al., 2019; Rummel, 2015). During times of transition like COVID-19 and the lockdown, mental health challenges are exacerbated.
Aside from students’ own coping styles, resilience, and self efficacy, a few positive steps taken by the university and department may have resulted in fewer students expressing mental health stressors. Student familiarity with the online learning system prior to COVID-19 could have made the online transition easier. The Wits psychology department had been using it to provide PowerPoints of lectures, readings, online assignment submission, plagiarism checking, and online tests since the #FeesMustFall protests of 2015 and 2016 when the university embarked on emergency remote learning for a short while in each year. Some lecturers were also using the system before #FeesMustFall. The university’s early continuation of classes, immediately after initial lockdown restrictions, meant that students did not miss as much as students from other institutions who started later. The laptops provided by the university together with free data made it easier for students to partake in the online environment. The accessibility of staff across platforms from telephonic and mobile access through to consultations on Whatsapp and Microsoft Teams assisted students. As yet, there is no publicly available data on the uptake of free telephonic counselling services at the university, the option to access this could also have reduced the intensity of symptoms such that there were no elevations on the quantitative scales. Certainly, these were among the factors cited by students as support received from the university and the Psychology department.
Contact tertiary education institutions across the world have been debating the merits and demerits of going online (Bowen et al., 2014; Mpungose, 2020; Wong et al., 2018). The responses from students are providing support that contact sessions do have a value pedagogically in terms of enhancing the learning experience for students, improving understanding and uptake of material, and assisting students with workload and time management. The feedback shared with regard to home dynamics, such as limited finances, poverty, overcrowding in small houses, and limited internet connectivity in rural communities, further strengthens the case for contact institutions continuing with face-to-face campus tuition and explains why students needed to come back despite the Lockdown. It also makes a strong argument for why institutions should use blended learning and not online learning going forward.
All of these responses, including the requests for flexibility, reduced workload, more structured lessons, access to counselling and self-help and more understanding, were conveyed to the module co-ordinators with staff working on implementing this for the second semester.
While this study was very useful in gaining insight into psychology students’ experiences during COVID 19, it must be acknowledged that this was a small sample, which consisted of first- and second-year students only. It is possible that those who were in greater distress may not have responded and vice versa. Hence, these data only represent a snapshot of the student experience at a particular time – Lockdown Level 3. Further follow up research is necessary.
Conclusion
While the self-reported experiences of undergraduate psychology students during COVID-19 and the national Lockdown revealed evidence of emotional distress, the levels of this distress when measured did not reach elevations to warrant clinical concern. It is likely that the emotional responses were appropriate to the situation, which entailed sudden shifts in day-to-day life, such as limited opportunities for social interaction and changed requirements for academic engagement and performance. While a number of challenges were experienced with regard to emergency remote teaching, students appear to have exhibited some resilience within their distress, with support from family, where possible, and the university. Going forward, lessons learnt with emergency remote learning have been useful in terms of facilitating blended learning for psychology undergraduate students. Lessons learnt can assist in improving access to content for students, but most importantly, the lessons learnt can be used to facilitate student mental health and stress in the post-COVID period or in other times of transition.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.