
Abstract
Palliative care staff are exposed to a plethora of work-related stressors that negatively affect their psychological well-being and work engagement. Using qualitative interviews, this study sought to explore the experiences of work-related stress and coping among a multidisciplinary group of 12 palliative care staff employed by a non-governmental hospice in South Africa. Data were analysed using the principles of thematic analysis. Four domains of stressors were implicated in the experience of work-related stress: stressors accruing from the nature of work and were specific to palliative care; stressors relating to working in the community; those deriving from certain encounters with patients and families; and organisational stressors. Broader structural factors pertinent to the socio-political and economic context in South Africa and the perception of palliative care were interwoven with the experience of work-related stress. Receiving social support from co-workers, professionals, and family and friends; accepting limits; setting work–life boundaries; relying on personal resources and reconstructing the hospice in positive ways were coping strategies deployed by staff to manage stress. Arguably much of the experience of work-related stress and coping among palliative care staff in South Africa is similar to that reported in resource-rich contexts. However, the particularities of the broader socio-political and economic environment and its subsequent impact on palliative care organisations appear to augment and expand work-related stress for these practitioners. Deployment of intra-individual and interpersonal coping resources could be supplemented with efforts to address structural factors contributing to the subjective experience of stress.
Constituting a landmark in the development of palliative care in sub-Saharan Africa, the 2002 Cape Town Declaration asserted that pain relief is a human right for everyone with a life-limiting disease (Grant et al., 2011; Mpanga Sebuyira et al., 2003). Despite progress since then, limited population coverage (Grant et al., 2011), late patient presentation, limited availability of pain control drugs (Grant et al., 2011; Harding & Higginson, 2005), poverty (Gysels et al., 2011), and a growing burden from non-communicable diseases (Powell et al., 2017) are common challenges for palliative care provision in sub-Saharan Africa.
In South Africa, palliative care provision has achieved some degree of integration with mainstream health services (Wright et al., 2008); there are currently eight hospital palliative care services and 150 hospices, with a few initiatives focusing on paediatric palliative care (Downing et al., 2013; Drenth et al., 2018). Most palliative care in South Africa is provided by non-governmental organisations (NGOs) in the community and at patients’ homes. Estimates suggest that 0.52% of the population need palliative care in any year (Drenth et al., 2018). Although South Africa has led palliative care developments on the continent, limited funding and people’s negative perception of palliative care remain the key challenges (Drenth et al., 2018).
Work-related stress and coping in palliative care staff
Healthcare staff experience high levels of work-related stress (Johnson et al., 2005), which is associated with increased prevalence of psychological distress (Weinberg & Creed, 2000) and burnout (Felton, 1998). Palliative care staff also face an increased risk of burnout and compassion fatigue (Kearney et al., 2009). A UK survey among cancer clinicians (Ramirez et al., 1995) showed that 28% were probable cases for minor psychiatric disorder and more than a quarter manifested signs of burnout. Research with palliative care clinicians in the United States (Kamal et al., 2016) indicated that 62% experienced at least one symptom of burnout: emotional exhaustion or depersonalisation. Support from family and friends, recreational activities, physical well-being, taking vacations, setting boundaries, and realistic expectations were important strategies to manage burnout (Kamal et al., 2016).
Qualitative studies have sought to provide an in-depth understanding of the subjective experience of workplace stressors and coping mechanisms employed by palliative care practitioners to manage stress (Ablett & Jones, 2007; DiTullio & MacDonald, 1999; Kavalieratos et al., 2017; Perez et al., 2015; Swetz et al., 2009; Zambrano et al., 2014). Positive, sometimes transformative (Mota Vargas et al., 2016), experiences are reported by palliative care staff such as compassion satisfaction, an enhanced sense of spirituality, opportunity to live at present and be able to deeply reflect on the meaning and continuity of life (Sinclair, 2011). However, frequent exposure to suffering, death and dying, the complexity of caregiving activities at the end of life (Lindqvist et al., 2012), and the high levels of emotional labour involved in working with the dying (Funk et al., 2017; Rokach, 2015) constitute significant challenges.
Organisational factors are a primary source of stress for palliative care staff (Vachon, 1995). Limited resources and shortage of staff, increased workload and work complexity, competing role demands, unpredictable schedules, conflicting expectations, inadequate communication, organisational change, and lack of organisational support contribute to staff strain (Ablett & Jones, 2007; DiTullio & MacDonald, 1999; Kavalieratos et al., 2017; Perez et al., 2015). Stress further derives from interactions with patients and families. For instance, the intensity of cases or encountering cases with which staff identify and managing patient and family communication and expectations are important sources of stress (Ablett & Jones, 2007; Perez et al., 2015). Finally, individual factors, such as difficulty in setting work–life boundaries and embracing limits, also play a part in experiences of work-related stress (Perez et al., 2015).
To manage stress, palliative care staff rely on a series of intrinsic and extrinsic resources (Zheng et al., 2018). Engagement with self-care, leisure activities, and daily routines; reflection and increased self-awareness; maintaining a healthy work–life balance; and emotional and physical distancing have been found to be beneficial (Ablett & Jones, 2007; Perez et al., 2015; Swetz et al., 2009; Zheng et al., 2018). The availability of supportive relationships and social networks in and out of work, the use of humour, participation in religious communities or spiritual practices, and the availability of regular debriefing within organisations help palliative care practitioners cope with stress (Ablett & Jones, 2007; Perez et al., 2015; Swetz et al., 2009; Zheng et al., 2018).
Despite a growing number of qualitative studies in European and North American countries (Ablett & Jones, 2007; DiTullio & MacDonald, 1999; Funk et al., 2017; Kavalieratos et al., 2017; Perez et al., 2015; Sinclair, 2011; Swetz et al., 2009; Zambrano et al., 2014), there is limited research in sub-Saharan Africa. This hinders a full understanding of the perspectives of palliative care staff within this resource-limited context. As a result of the HIV epidemic in South Africa, existing research in the country has mainly focused on professionals working with HIV/AIDS terminally-ill patients (Bam & Naidoo, 2014; Demmer, 2006; Smit, 2005; Valjee & Van Dyk, 2014). Little is still known about the experiences of palliative care staff who work in a hospice setting and provide care primarily to cancer patients. This study, thus, sought to provide insights into the subjective experience of work-related stress and coping mechanisms among a multidisciplinary team of hospice staff.
Method
Participants
A qualitative, cross-sectional study was designed using in-depth, semi-structured interviews. The research took place at a non-profit hospice organisation, located in the Western Cape, South Africa. The organisation consisted of a 10-bed, in-patient unit, which admits patients for up to 2 weeks, and community hospices that provide day-centre facilities and home-based care and support for patients and their families. After hours and on weekends, community services are covered through telephonic support. In total, over 700 patients are served every month. Palliative care personnel include nurses, doctors, social workers, spiritual counsellors, and community health workers who are assisted by volunteers drawn from the local communities. Currently (as of 31 August 2018), there are 169 staff and approximately 600 volunteers. The hospice offers a range of services from nursing support, physical, emotional, psychosocial and spiritual care to bereavement support.
Access to the organisation was sought by A.K., and following discussion, the current study was developed. The study was advertised to potential staff participants through the organisational management structure. The dates for the interviews were set to coincide with a visit from P.S. The study utilised an opportunistic purposive sample which included a range of palliative care practitioners.
In total, 12 palliative care staff took part in interviews (11 women and 1 man). Participants’ age ranged from their late 20s to 65 and worked across the full range of palliative care specialties. Eight participants were working in the in-patient unit and the remaining four were based in the community. Participants’ work experience in the hospice varied from a few months to 28 years. To avoid breaching confidentiality and ensure participant anonymity, we refrained from providing any further participant information. Interview extracts in the results were only identified by whether the person was a community or an in-patient unit staff and their unique identification code.
Interview guide
An interview protocol consisting of 12 open-ended questions were developed to guide the semi-structured interviews. Interview questions and related prompts explored participants’ experiences of working at the hospice, their sense of well-being and how they cope working in the end of life care, any current or future concerns they might have, and their needs for help and support. The interview protocol was initially developed by A.K. and P.S. based on researchers’ prior experience of conducting similar projects. The protocol was then discussed with the Director of Education in the hospice whose feedback informed further development and refinement of the questions.
Procedure
P.S., an experienced qualitative researcher, carried out one-to-one interviews in 2016. Interviews took place at the hospice, at a time convenient to participants and lasted between 39 and 69 min (average length 51 min). All interviews were conducted in English, audio-recorded and transcribed verbatim.
Ethical considerations
The research received ethical approval from the University of Bath (Ref SU-HSD-003055) and Hospice Palliative Care Association South Africa (Ref 03/16). All participants gave written informed consent before the interview.
Data analysis
An inductive thematic analysis (Braun & Clarke, 2006) was performed on the transcribed interviews. Transcripts were initially read repeatedly, and summaries were developed. Preliminary analysts’ thoughts were noted down at this stage and first impressions of the data were discussed among researchers. Assisted by software programme (NVivo), data were then organised into initial codes. Themes and subthemes were developed by aggregating relevant coded segments under broader categories. A preliminary analytic report was produced and discussed with a view to revising and refining the emerging themes. After ensuring that the themes were exhaustive and reflective of the data, the final analytic report was generated.
Results
The results are divided into two sections: (a) the experience of work-related stress and (b) coping with stress. Figure 1 presents the themes and subthemes identified for each section of the analytic focus.
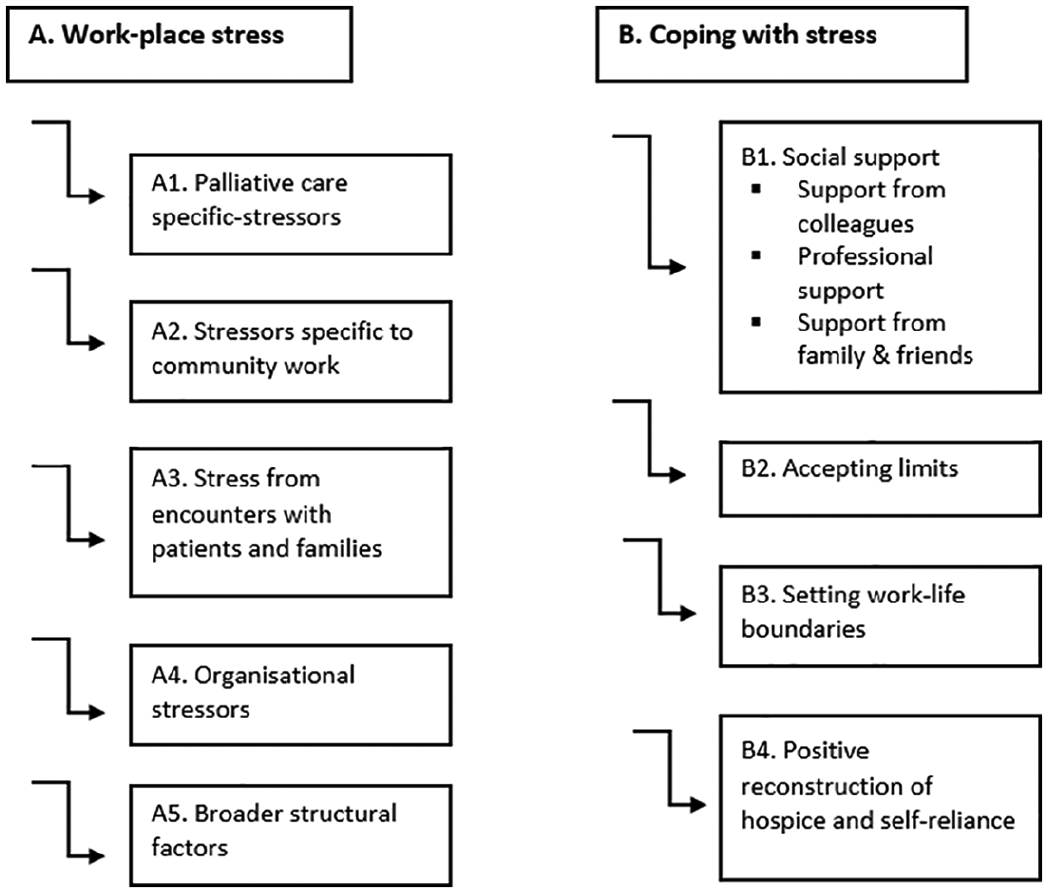
Themes and subthemes of work-related stress and coping.
Experience of work-related stress
Palliative care–specific stressors
Staff reported that confronting death on a regular basis was stressful and emotionally draining, especially for those who had routine contact with patients and developed connections with them. Patients’ death functioned as a reminder of staff’s own losses and brought to the surface existential worries and questions around the meaning of life. Certain patient cases – primarily young deaths – provoked intense emotional responses as staff tended to psychologically identify with them (e.g., as parents of that young person). Rumination was a risk for some who found hard to disassociate their thoughts and feelings from these patient cases: There are people that die almost every day and there are children who are young and you think if it was my child what was going to happen. You don’t just let it go, you always think about it. (P2: In-patient unit staff)
Concealing their own difficult emotions (e.g., sadness, frustration) in front of patients and families was another challenge especially when staff thought that patients were able to discern their emotional state. Feelings of inadequacy to improve the patients’ medical situation, particularly among staff from a curative healthcare background, and intervene with their broader life situation added to staff strain: But I think the biggest thing I struggle with is the feeling of ‘I can’t fix this’. (P7: In-patient unit staff)
Stressors specific to community work
Participants reported that providing palliative care in the community presented difficulties that were linked to the lone and mobile character of work. Community workers were required to make their own decisions without direct supervision. Sometimes they also had to handle situations that might fall outside their remit or comfort zone. Work in the community was difficult to organise and predict, with staff needing to be flexible and prepared to respond to patients and families’ needs as they arose in the field. Community staff might end up spending more time in certain home visits or do a different job than what they had planned. The unpredictability of encounters in the community, sometimes combined with traffic delays while travelling from site to site, resulted is a less structured and more haphazard work day than that experienced by in-patient unit staff: I could go in with a plan, this is what we need to talk about but then they don’t want to talk about it or they are not ready to talk about it. (P5: Community staff)
Stress deriving from certain encounters with patients and families
Interactions with patients and families were clearly a major source of job satisfaction when the caring staff’s work was recognised and appreciated. However, certain encounters caused considerable stress and frustration. Such a situation arose when staff managed ‘difficult’ patients, that is, patients who were demanding, did not cooperate and might become frustrated, accusatory, or depressed. Handling patients’ own stress every time they became aware of someone else’s death and trying to address practical aspects (e.g., will) with patients who were in denial of death were further stressful interactions: They do get frustrated and they will accuse you of anything, you didn’t treat him or her right and all those things. (P6: In-patient unit staff)
Encounters with family dynamics characterised by confrontation and dysfunctional communication was another source of stress. Interviewees expressed frustration and sadness when patients and families were unwilling to resolve their conflicts and restore their relationship nearer the death. Equally, participants stated that they felt frustrated when families were unable to take care of their loved one with the latter feeling rejected, isolated, and lonely. Managing families’ own concerns about the patient’s condition and unrealistic expectations about what could be offered and achieved further contributed to staff stress: And sometimes they also have unrealistic expectations and you have to sort of break the news gently to them, what we can do and what we can’t do. (P5: Community staff)
Organisational stressors
At the time of the study, the hospice was undergoing major changes which seemed to have unsettled established work routines and affected relationships, practices, and structures within the organisation. Against this background, interviewees described challenges relating to the impact of those changes on the caring team. Specifically, participants felt that new structures, changes, and decisions were sometimes imposed on staff without the latter being consulted and listened to; that the core function of the organisation – palliative care provision – had been affected negatively over the years; that there was a lack of understanding and appreciation of the nuances and subtlety of the caring staff’s work; an increasing focus on quantitative indicators and metrics; and that leadership did not always succeed to smooth out tensions and manage power dynamics and politics. Diminished trust, deficient communication, and lack of organisational transparency were highlighted. Within this context, feeling unsupported by senior management was an important source of stress at times: (there is) a feeling the caregiving team does not feel supported and it’s a major problem. It really does add to staff stress. (P1: In-patient unit staff)
Due to financial constraints, the number of in-patient nursing staff was reduced over the years, which impacted on workload and the perceived quality of care provision. The low salaries for non-professional nursing staff and long work hours (e.g., 12-hr shifts) were also referred to as important issues. Although community staff had shorter shifts, maintaining work–life balance was practically and psychologically challenging. As there was only telephonic coverage during out of hours and over the weekends, in emergencies, staff had to visit patients’ home outside their work days/hours. As a participant said (P9: Community staff), ‘we work from 8 till 4 but it’s a 24 hr job’. Moreover, staff had to negotiate competing demands; on the one hand, they had to prioritise self-care by having time off work, and on the other, they had to find the courage to refuse requests to colleagues; to be able to trust colleagues who covered them that they will provide an equally good service to their patients; and to manage uneasy feelings arising from staff’s unavailability on occasions their patients might be most in need: Sometimes people don’t realise that you are not just being difficult but there’s a practical reason behind saying ‘no’ . . . if I am overtired or over-exhausted or the workload is just heavy then I am like ‘oh how am I going to cope?’ (P5: Community staff)
Finally, increasing organisational bureaucracy and concerns relating to health and safety at work were further factors causing stress.
Broader structural factors interwoven with work stress
Elements of the broader socio-political and economic context in South Africa were brought into narratives of work-related stress. The dangers from criminality, problems with transportation to and from work, and the challenges accruing from working with racially, religiously, and linguistically diverse communities were interwoven with workplace stress: Some people travel quite a bit and of course they all have to use public transport and there’s dangers and they work nursing hours that are not very sociable and in winter they come in the dark, leave in the dark. (P1: In-patient unit staff)
The interface of palliative care with the medical world and society at large also created challenges. Community staff described how the fact that palliative care is not massively recognised or well understood by other healthcare professionals (e.g., GPs) and healthcare organisations obstructed smooth collaboration and integration of services for the patient’s benefit. But staff also faced the public stereotype of hospice care as being inherently linked to death and dying. This made patients and families occasionally reluctant to receive the service: We are invited into the patient’s house but sometimes you also get that resistance. People will think hospice is not welcome. Hospice is all about death and dying. We are not allowing you in the house. (P10: Community staff)
Coping with work-related stress
Social support
Support from colleagues
Interactions with colleagues, in the same profession and across disciplines, was a significant source of support. This took the form of unstructured, informal exchanges or more formal, regular meetings. Support from colleagues was valued, partly because co-workers could genuinely understand work-related problems and concerns. Formal and informal interactions among staff served several functions: facilitated job-related problem-solving, information sharing, and instrumental aid; provided a space for expressing concerns, sharing emotional difficulties and frustrations, and being listened to; created connectedness that alleviated a sense of aloneness under difficult work circumstances; and enabled validation of work: I think sometimes when we’ve had a really bad day we would like get it out there and talk to one another and say ‘yeah I had this day’ and I think that also kind of helps just to get the weight off. (P10: Community staff)
Professional support
Although co-worker support was invariably valued, interviewees recognised limits relating to time constraints and people’s willingness to share personal concerns and emotions with people in the same work environment. As a result, staff stated that they often used professional counselling services to cope primarily with emotional distress. The counselling services were either provided by the organisation or sought by interviewees outside the organisation on their own initiative: Then I have taken it upon myself to see somebody outside of the organisation, she is just a counsellor and. . .we deal with personal stuff and work stuff and that works really well for me. (P7: In-patient unit staff)
Support from family and friends
Social circles outside work was a further source of support. A sense of comfort and relaxation was achieved through routine and everyday interactions at home, spending time with friends, and the use of humour that helped participants unwind from work stress. Interestingly, participants avoided discussing details of their work with family and friends in an effort to protect them from becoming upset and emotionally involved: There are things that you can tell them but there are things that you feel no, it will worry them. (P6: In-patient unit staff)
Accepting limits: ‘it is what it is’
Coming to terms with limits was an important coping strategy. These limits concerned staff’s professional knowledge and ability to exert control and bring change over the patient situation. For some participants, acknowledging and accepting inadequacy was transformed into a source of strength that helped them continue working in this field and manage frustrations. Interviewees further recognised that they were not responsible for, ‘fixing things’. Instead, they ascribed value to, and derived job satisfaction from, aspects of their work that they could control. For instance, the medical staff highlighted how impactful their mere presence was on patients even though they could not cure them: I think a lot of doctors will struggle with that, that you can’t do anything! I always emphasize that you are doing a huge amount and it’s really just to your presence that matters most. (P1: In-patient unit staff)
For community staff who came into close contact with family dynamics, it was important to embrace families’ pace. This meant that staff respected their decisions even if they contradicted staff’s advice and viewed families’ responses as a way of retaining control over their life. Finally, approaching death as an unavoidable part of life, even if this entailed some degree of fatalism and intellectualisation, and being able to let go of patients who died were important coping mechanisms. Saying goodbye to patients was facilitated by rituals, for example, attending memorial services organised by the hospice.
Setting work–life boundaries
Achieving a healthy work–life balance was of paramount importance both for participants’ perceived well-being and the quality of their interactions with patients and their relationship with family and friends. More experienced staff highlighted to newcomers the value of securing ‘me time’ and several had managed to set satisfactory work–life boundaries over the years. For example, they tried to address work problems at the work environment and not carry them at home; they avoided working longer hours, had regular breaks, weekends away and took their leave; concerning the community staff, they took precautionary measures so that the likelihood of having to visit patients during weekends was minimised. Staff were acutely aware of the risk of burnout and drawing that line essentially reflected their effort to preserve a space for self-care. Listening to music, walking, doing meditation or exercise, and engaging with community activities were pleasurable activities participants engaged with to de-stress and mentally disassociate from work.
I mean one must look after oneself. If you don’t, you are not going to be of any use to your patient or anybody else. (P4: In-patient unit staff)
Positive reconstruction of hospice and self-reliance
To manage uncomfortable discussions about hospice and palliative care with people outside work, a few participants tried to deflect negative associations of hospice with death and dying. The latter was achieved by highlighting that humour was often present at the hospice. They also stressed that time nearer death can be constructive and transformative for patients, a potentiality particularly rewarding for staff: We use a lot of humour so they’re always coming with funny stories or things that made them laugh when they weren’t allowed to laugh in the moment. So there’s a lot of humour and that’s a big coping strategy. (P7: In-patient unit staff)
Finally, relying on personal resources, such as the ability to reflect on things, put them into perspective and reframe them; being able to recognise, express, and stay with emotions; and draw on belief and value systems (e.g., religion) to derive strength and make sense of adversity were useful resources for managing stress.
Discussion
The present qualitative study sought to provide an in-depth understanding of the experiences of work-related stress and coping strategies used by palliative care staff who work in a hospice in South Africa. In line with previous research (DiTullio & MacDonald, 1999; Vachon, 1995), our findings indicate that experiences of work-related stress were commonly attributed to organisational aspects. Organisational change and decision-making were often felt to be imposed on staff and disturbed established relationships and work routines, partly due to staff turnover. These changes were also viewed to undermine the quality of the core function of the organisation, that is, holistic palliative care provision. Deficient flow of intra-organisational communication – both horizontally and vertically – staff shortage, increased workload, long work hours, dissatisfaction with economic rewards, increasing organisational bureaucracy, and at times, unsatisfactory management of health and safety at work were all reported to contribute to staff stress and compromise quality care for patients and their families (Ablett & Jones, 2007; DiTullio & MacDonald, 1999; Kavalieratos et al., 2017; Perez et al., 2015). Supporting existing research (Ablett & Jones, 2007; Perez et al., 2015), exposure to death and dying, psychological identification with patient cases, engagement with ‘difficult’ patients, and interactions with dysfunctional families were further sources of stress that were emotionally draining and existentially challenging.
Moreover, our findings uncovered broader socio-political and economic factors that further compounded the experience of work-related stress. High rates of criminality in South Africa, inadequate transportation, limited financial resources, and unstable funding for palliative care organisations were interwoven with staff stress. Furthermore, racial, linguistic, and religious patient and community diversity, a lack of recognition and integration of palliative care into the broader healthcare system, and negative public perceptions of hospice (Drenth et al., 2018) also contributed to workplace stress.
Finally, our results demonstrated that both extrinsic and intrinsic resources were deployed by staff to cope with workplace stress (Zheng et al., 2018). Receiving social and professional support; embracing limits; maintaining a healthy work–life balance; actively prioritising self-care; and positive reconstruction of hospice (Ablett & Jones, 2007; Kamal et al., 2016; Koh et al., 2015; Perez et al., 2015; Swetz et al., 2009; Zheng et al., 2018) were important coping strategies. Although staff utilised formal organisational support (i.e., counselling, bereavement, and wellness services), co-worker informal support was among the most valued coping resources.
The findings of this study should be considered within the context of the study limitations. First, although sampling was designed to be purposeful so that information-rich cases are attracted and interviewed, termination of participant recruitment was dictated by pragmatic considerations. These related to project resource constraints, rather than data saturation, the point at which no new information is generated by adding further interviewees. Nevertheless, the interviews produced adequately rich data which allowed us to provide a comprehensive cross-participant account of stress and coping. Moreover, due to our sample heterogeneity in terms of their profession (i.e., medical, nursing, allied health professionals), the possibility that additional nuances relating to specific occupations would be detected, should more interviews have been carried out with particular occupational sub-groups, cannot be precluded. Finally, this study took place within a non-governmental palliative care organisation. To ascertain to what extent these findings might be relevant and transferable to palliative care staff working in different palliative care settings (e.g., hospital palliative care units; community-based models), further research is required in these other palliative care environments to determine commonalities and differences.
Conclusion
Much of the experience of work-related stress and coping among palliative care staff in South Africa resembles that reported by practitioners in resource-rich countries in Europe and North America. For example, stressors specific to end-of-life care or those accruing from challenging encounters with patients and families are commonly encountered. Nevertheless, broader socio-political and economic circumstances in South Africa seem to augment workplace stress either directly or through more indirect ways. For instance, the health and safety of staff who commute to and from work or work in the community are often at risk due to the high rates of criminality in the country. The tight financial climate and the operation of many hospices under unstable (i.e., non-governmental) funding is likely to enforce these organisations to frequent or unanticipated change and adaptation which in turn might impact on employee outcomes negatively. Insufficient integration of palliative care within the broader healthcare system, limited recognition by healthcare professionals, and stereotypic conceptions held by the public at large further complicate the everyday work experience of these practitioners. This study suggests that staff rely on a series of individual and interpersonal resources to cope with work-related stress. Yet, any effort to intervene holistically with work-related stress should also address structural barriers.
Footnotes
Acknowledgements
We are very grateful to the palliative care practitioners and the organisation for taking part in our study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported financially by funding from the British Academy, Newton Mobility Grant, and the University of Bath. The funding body had no role in the design of the study and collection, analysis, and interpretation of data and in writing the manuscript.