
Abstract
In this report we describe the implementation of a new electricity supply system at Mulanje Mission Hospital, Malawi, which integrates the use of grid electricity, solar-generated electricity and battery back-up. To realize the system, suppliers from several countries had to be used and external expertise and funding were vital. The completed system provides reliable and good quality electricity to all departments in the hospital, prioritizing essential equipment when needed. Implementation of the system has reduced cost of electricity bills by 60%, ended black-outs and extended longevity of electrical equipment. We describe our approach, the materials used and results with challenges and recommendations to governments, donors interested in hospital infrastructure and other health facilities operating in similar circumstances. Others in similar settings can benefit from the experiences documented.
Introduction
Mulanje Mission Hospital (MMH) is a 237-bed secondary healthcare facility in south Malawi providing a range of in- and outpatient care as well as community outreach and public health programmes. Reliable infrastructure including electricity supply is a critical requirement for the provision of safe patient care.
However, grid electricity outages due to insufficient supply, natural disasters and poor infrastructure are common in Malawi, for example during a recent tropical cyclone. 1 These outages have a negative effect on quality of care. 2 Over- and under-voltages (brown-outs) are common too, leading to early failure of electrical equipment.
A 2017 survey across Malawi in 44 health facilities found that all of them experienced interruptions in power supply in the past six months and that these interruptions were unpredictable and lasted on average eleven hours. In the survey, 25% of facilities were found to use some form of solar photovoltaic energy, but 67% of the solar-powered back-up systems were described as non-functional. Only 15% of back-up energy sources could cover all required appliances. 2 To our knowledge, prior to our work there was no hospital in Malawi primarily and reliably electrified by solar energy.
Methods
Preparation
In 2021, MMH embarked on a project to renovate and reinstall the solar power system and upgrade the general electrical system at the hospital. This had become a priority for several reasons:
The hospital faced increasing utility bills; at the same time prior investments in solar energy did not bring significant cost reductions; The general electrical system had been evolving over many decades3 and was not well organized, making fault-finding difficult and compromising safety; overhead cables suffered regular lightning strikes causing loss of electrical equipment such as medical monitors, computers, pumps and air-conditioning; A central distribution board in the hospital was absent, making fault-finding and management difficult.
At the start, an energy audit was carried out in all departments together with consumption readings, which allowed us to gain insight and map all electricity consumers. A scope of work was then developed in cooperation with technicians from overseas and from within Malawi. We decided to pursue a system that would lead to significant cost savings and a situation whereby the entire hospital could be provided with a reliable electricity supply without destructive surges and brown-outs. We decided that the commonly implemented emergency systems in which one or several departments are connected to a battery back-up without integration with the rest of the electrical network would not provide the desired outcome. The resulting scope of work was shared with four local companies. None tendered an acceptable proposal – for example, one proposed to discard all existing solar panels and batteries, making the project unnecessarily expensive, and another presented a technical design that would not work. Therefore, MMH decided to execute the project in-house with the help of overseas volunteers supported by local technicians. Learning and capacity-building was an important and integral part of our approach. A system was designed utilizing high-quality solar and battery inverters and reuse of still functioning materials from the existing system.
Implementation
Some system components were sourced locally but most were imported from South Africa and the Netherlands. These were duty-free under Malawi's tax-code. Even cable and good quality common electrical components such as circuit breakers had to be imported. MMH technicians and a volunteer solar technician installed the equipment and the required cabling (Table 1). From the previous malfunctioning solar installation 28 4800Wh li-ion batteries, some cabling and the majority of solar panels were reused; 30 kWp existing solar panels were removed, cleaned and re-installed whilst adding new panels, bringing the total to 128 kWp installed. Orientation was both North and East/West to gain the optimal supply of solar electricity throughout the day. Since grid feed-in is not allowed in Malawi, our aim was not peak production but maximizing the number of hours that solar energy is available. The system started to be used in January 2022 and was subsequently increased in size and completed in June 2022.
Materials used for upgrading the electrical system at MMH.
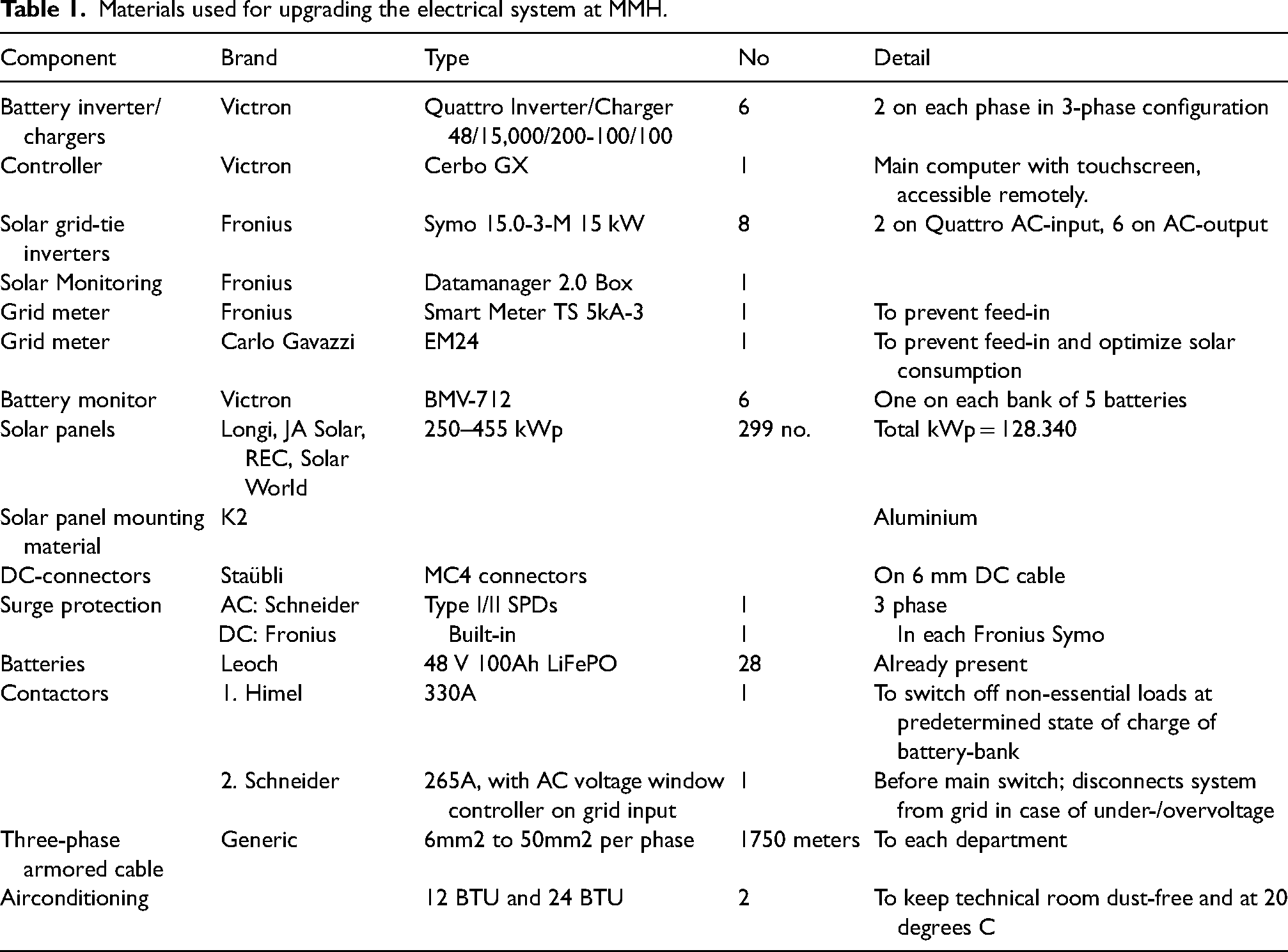
Several general improvements were also implemented as part of the work: all single-phase and overhead cables were replaced with three-phase underground cables of adequate size, a new central distribution board was installed, and the transformer connection was upgraded with a new incoming cable, reducing energy losses and disturbances. A contactor (automatic switch) was placed to allow loads to be reduced after a certain time of grid-loss and a set battery ‘state of charge’, so that battery energy is conserved for essential equipment. Each department is now provided with three phase power with always one of the phases (alternating per department for reasons of balancing) having guaranteed uninterrupted power supply (UPS) for essential needs.
Results
MMH now has a 3-phase grid-coupled solar electricity system. Battery cycling allows MMH to use each night excessive solar power. The system can be controlled via a mobile app by the maintenance supervisor. This is useful, for example when bad weather or grid outages are expected, in which case the batteries can be kept fully charged throughout the night.
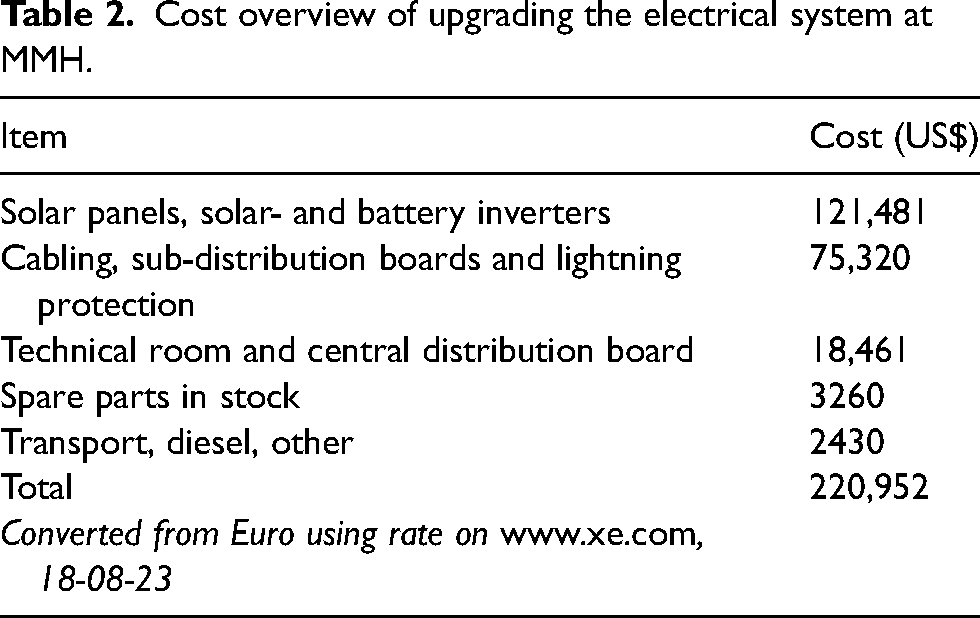
A total investment of US$ 220,952 was made. See Table 2. Due to unstable exchange rates, exact figures may be slightly different. In addition, foreign volunteers gave their time. Cost savings are being made in several categories: (1) electricity bills have been reduced by 60.6% in the period prior to installation compared to after completion (Table 3), which provides an average saving of US$ 1585,00 per month (electricity price and exchange rate as of 01-01-2022). At this rate the investment will repay itself in 11 to 12 years; (2) diesel for the generator is very rarely required now except during extremely prolonged outages combined with rain, such as during the cyclone in March 2023, and (3) replacement and repair costs for electrical equipment is much reduced and the water supply has improved as power for borehole pumping is now constantly available.
Cost overview of upgrading the electrical system at MMH.
Grid electricity consumption and cost savings over one year at Mulanje Mission Hospital.
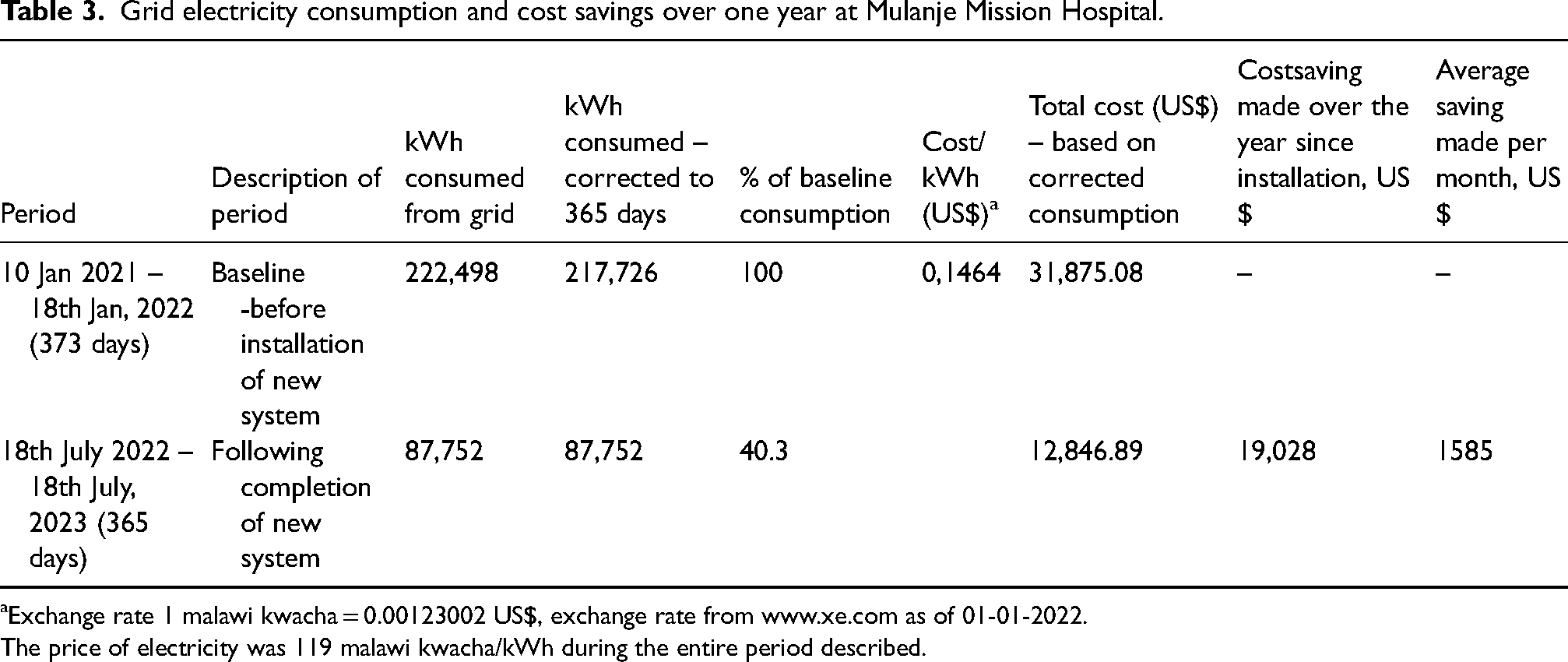
Exchange rate 1 malawi kwacha = 0.00123002 US$, exchange rate from www.xe.com as of 01-01-2022.
The price of electricity was 119 malawi kwacha/kWh during the entire period described.
Additional benefits include reduced greenhouse gas emissions, a stable working environment for healthcare workers enabling them to focus on patient care, more electricity available to other consumers in Malawi and setting a positive example of what can be achieved in a difficult environment.
Discussion
Despite an ultimately successful implementation, serious challenges were encountered.
A major challenge to a system like this is that feed-in to the grid is not allowed in Malawi. This leads to more complex system design and loss of efficiency as solar power throttling is needed. For optimum use of solar inverters, more expensive batteries are needed.
The extremely poor quality of electricity supply is a challenge too. Not only are there frequent black-outs, but also when power is available it cannot always be accepted by the inverters due to under- or over-voltage, phase rotation problems and frequencies exceeding safe limits. This is especially a problem during the rainy season, although has improved after the upgrade of our transformer connection.
Previous solar and other electrical connections done at MMH were of poor quality, reflecting the generally poor standards of electrical work in the country. Even when we undertook new work, the work needed continuous oversight and frequent correction.
While solar generating power and battery backup are visible and easily understandable, technical upgrades that attract ample attention from donors, they may prove to be of little use and limited longevity if at the same time there is not a substantial investment done in the basic local electricity infrastructure. Good electrical cabling and connections and a well organized and secure power distribution network are indispensible for all other technical advancements. Yet, it is hard to secure funding for these improvements alone even though the investments can last decades, demand little to no maintenance and hold their value (copper doesn’t age).
It was a logistical puzzle to get all parts into Malawi in time, especially as not all funding was secured from the start of the project. Basic electrical parts, cables and pieces of equipment are extremely hard to find locally; most must come from abroad. It proved challenging to obtain a distribution board of the required standard.
Others may consider the use of DC MPPT chargers instead of some of the solar AC inverters as we have done, as this requires less AC-DC conversion, which takes a strain on the inverters and results in energy losses. Looking towards the future, maintenance and cleaning are done regularly, and repairs will be done locally if possible. To this end a local solar energy company has been engaged early-on during the implementation phase. Spare parts will likely have to come from abroad if not in stock already.
We plan to add 16 more 4800Wh Li-ion batteries in future to use even more solar generated electricity in order to further reduce costs.
Recommendations
We advise donors interested in solar to invest in independent, adequate technical knowledge and supervision so that installations are done with acceptable quality materials and workmanship. Donors should demand inclusion of maintenance contracts of at least five years when commissioning contracts in order to ensure a good quality level of material and workmanship. Also, donors should consider investment in less visible crucial infrastructure improvements as part of their strategy.
The Malawian Government and other governments in the region should consider to allow feed-in to the grid to make solar energy more economically feasible and increase supply to the national grid.
Other health facilities with interest in solar power should plan carefully what the aim of solar investments would be – for example only emergency supply or also cost-savings. This decision needs to be made at the start of system design and careful consumption readings are essential to dimension the system adequately.
Conclusion
An investment in solar energy in a Malawian hospital can pay off in terms of improved reliability of electricity supply, improved longevity of equipment and reduced costs with good return on investment. This investment has filled a basic prerequisite for safe patient care and provides a basis for improving patient outcomes. A project like this requires intensive senior staff involvement, significant fundraising efforts and technically competent advisers and contractors.
Footnotes
Acknowledgements
We would like to acknowledge collaboration with EMMS International, and donations from Action Renewables, the Flow Traders Foundation, the Belvedere Trust, Ansbach für Malawi and Stichting Steun Malawi. Wilson Kachikuwa, Pearson Soka, Jan Pieter van Driel, Gerwin Habermehl and David Zijderveld all contributed to the installation at the hospital.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.