
Abstract
Open tibia fractures are devastating, life changing injuries, with infection associated with substantial morbidity to the patient. Reducing infection is a research priority, but before interventional studies can be designed, the incidence of infection following this injury needs to be better defined. Our aim was to estimate the global incidence of infection following an open tibia fracture. A systematic review was performed of MEDLINE, EMBASE, Central Register of Controlled Trials (CENTRAL), Web of Science and Global Index Medicus. We included randomised controlled trials with more than ten participants which reported infections after open diaphyseal or distal fractures (AO 42 or 43). Primary outcome was deep infection according to the Centres for Disease Control and Prevention criteria. Secondary outcome included causative micro-organisms. A meta-analysis using a random effects model to assess incidence and between-treatment effects was performed. Thirteen studies including 1463 adults from seven middle-income countries, seven high-income countries and one low-income country were included. The incidence of infection was 12.12 person-years (95% CI 7.95–18.47). A subgroup analysis compared external fixation and intramedullary nailing showed no difference between infection rates. There were limited data on organisms, but Staphylococcus aureus was the most commonly identified. There are limited to no data on antimicrobial resistance.
Introduction
Following trauma, the tibia is one of the most common sites of lower extremity fractures. 1 Moreover, owing to the superficial position of the tibia, with minimal soft tissue coverage, one in four results in an open fracture.1–3 These have a bimodal distribution of presentation in high-income countries with the first peak amongst males in their twenties (3.71 per 100,000 person-years) and a second peak mostly in females aged 90 and over (9.91 per 100,000 person-years). 4 Infection is an important complication that can substantially increase morbidity and is associated with mal- and non-union, re-operation and even loss of limb or life. 5 Furthermore, open tibia fractures have a large economic burden on society, with only 20% of victims working at 1-year post-injury in low-income countries and substantial initial hospital costs.6,7
Therefore, understanding the incidence of infection in terms of patient, injury and treatment characteristics is important to reduce patient complications and the societal economic effects after injury.
Open tibia fractures follow a standardised treatment which includes early intravenous antibiotics, definitive fixation (internal or external fixation) and soft tissue coverage. 8 However, several factors, including delayed treatment and inadequate antibiotic prophylaxis, have led to the emergence of bacterial antibiotic resistance which is a global concern.9,10 Therefore, there is a need to understand the causative pathogens of infection in patients with open tibia fractures and their antimicrobial resistance profiles to target appropriate antibiotics and improve targeted treatment. 11
Understanding and improving the treatment of infection in trauma is a priority set by multiple stakeholder groups. The James Lind Alliance priority setting process is a UK-based stakeholder group which has identified infection as the leading priority in complex fractures. 12 Similarly, an international stakeholder group, consisting of trauma and general surgeons, identified infection associated with trauma as a top 10 priority. 13 A modified Delphi technique of surgeons in sub-Saharan Africa identified infection as a priority, and identifying the organisms and which antibiotics should be used to treat them. 14 Therefore, infection in open tibia fractures has been prioritised both in high-income countries and low-income countries, which may have different incidences and different pathogens. Despite numerous international groups identifying infection as a topic needing further investigation, the incidence of infection and causative organisms remain unknown.
Methods
We conducted a systematic review of the relevant literature currently available. Research studies included were critically assessed following pre-determined criteria according to a pre-registered protocol (https://www.crd.york.ac.uk/prospero/CRD42022371375). This review adheres to the guidelines published in the Preferred Reporting Items for Systematic Reviews and Meta-analysis 15 and in the Cochrane Handbook for Systematic Reviews of Interventions. 16
We reviewed randomised controlled trials (RCTs) with >10 participants. Studies in the English or French language reporting on: infections following open diaphyseal or open distal fractures (AO 42 or 43) 17 in adult civilians and the organisms causing them, were included. We included only RCTs as they represent studies with purposeful and well-defined follow-up points. Observational studies are likely to introduce bias into by under-, or over-estimating incidence as they often have poor follow-up rates, and so were excluded. 18
We also excluded case reports, cohort studies, case-control studies, case series, systematic reviews and expert opinions. Studies reporting on open tibial fractures sustained and treated in war were excluded, as military treatment resources and outcomes are not representative or generalisable to civilian populations. When there was a population with mixed fracture type, the studies were excluded if they did not report infection rates per fracture site (e.g. reporting pooled infection and not specifically for open tibia fractures).
A systematic search of the MEDLINE, EMBASE, Central Register of Controlled Trials (CENTRAL), Web of Science and Global Index Medicus was conducted) on 27 October 2022.
The search strategy was determined and refined with assistance of a medical librarian. Search terms including ‘tibia’, ‘open fracture’, ‘infection’, ‘surgical site infection’, ‘osteomyelitis’ and ‘microbiology’ were used. The search was limited to publications in the English or French languages.
Titles and abstracts were screened and included when they followed the inclusion criteria by the reviewer (DC & AR). Any discrepancies were solved through discussions with the senior authors (FD &CK). Data were extracted from included studies into pre-formatted Excel spreadsheets by two authors (DC & AR).
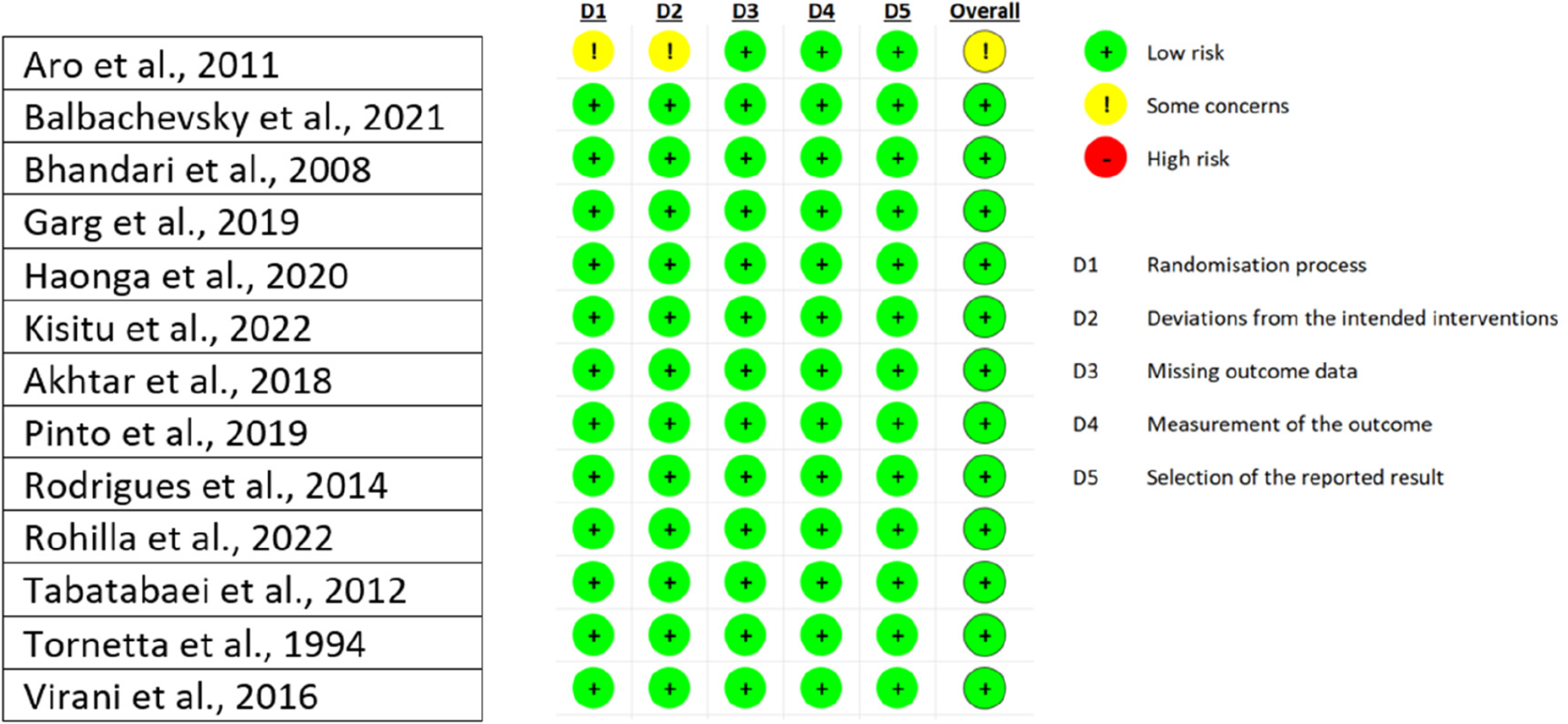
The primary outcome of this review was to establish the incidence of infections after an open tibia fracture, as defined by the Center for Disease Control criteria of bone and/or joint infections. 19 To assess the risk of bias, the Cochrane Risk of Bias tool for randomised trials (RoB 2) 20 was used.
A subgroup analysis to define infection based on income status of the country as high-, middle- and low-income countries as defined by the World Bank 21 , as well as a further subgroup analysis based on treatment type (Internal fixation, external fixation, plaster, non-operative treatment) will be carried out.
The secondary outcomes were to identify the most common organisms responsible for the infections and report their antibiotic resistance profile.
A meta-analysis with a random effects model was performed in R with the ‘meta’ package,22,23 to calculate the incidence of deep infections in person-years. Person-years is an appropriate measure of observation when incidence rates in the reported literature are reported with varying lengths of follow-up to estimate an incidence. 24 A sensitivity analysis was performed based on removing studies with short follow-up periods (<3 months). To assess the heterogeneity of the studies, the I2 statistic was used. It quantifies the amount of variation in outcomes due to differences between the groups rather than sampling error. 16
Results
The literature search yielded 3256 citations. After the removal of duplicates (n = 1162), the titles and abstracts of 2094 studies were screened. This led to the full-text retrieval of 94 studies. Of these 94, 19 reports were not published. Finally, 75 full texts were assessed for eligibility. Out of these, 63 were excluded, the reasons being listed in Figure 1. Reference review generated an additional study. Eventually, 13 studies from 15 countries were included for narrative synthesis and incidence calculation. Two studies were conducted in high-income countries (Canada, USA and the Netherlands).25,26 One study had data collected from multiple high and middle-income countries (Finland, South Africa, UK, France, Spain, Romania and USA). 27 Nine studies were carried out in middle-income countries (Brazil, India, Pakistan, Iran and Tanzania).28–36 Finally, one study collected data in a low-income country (Uganda). 37
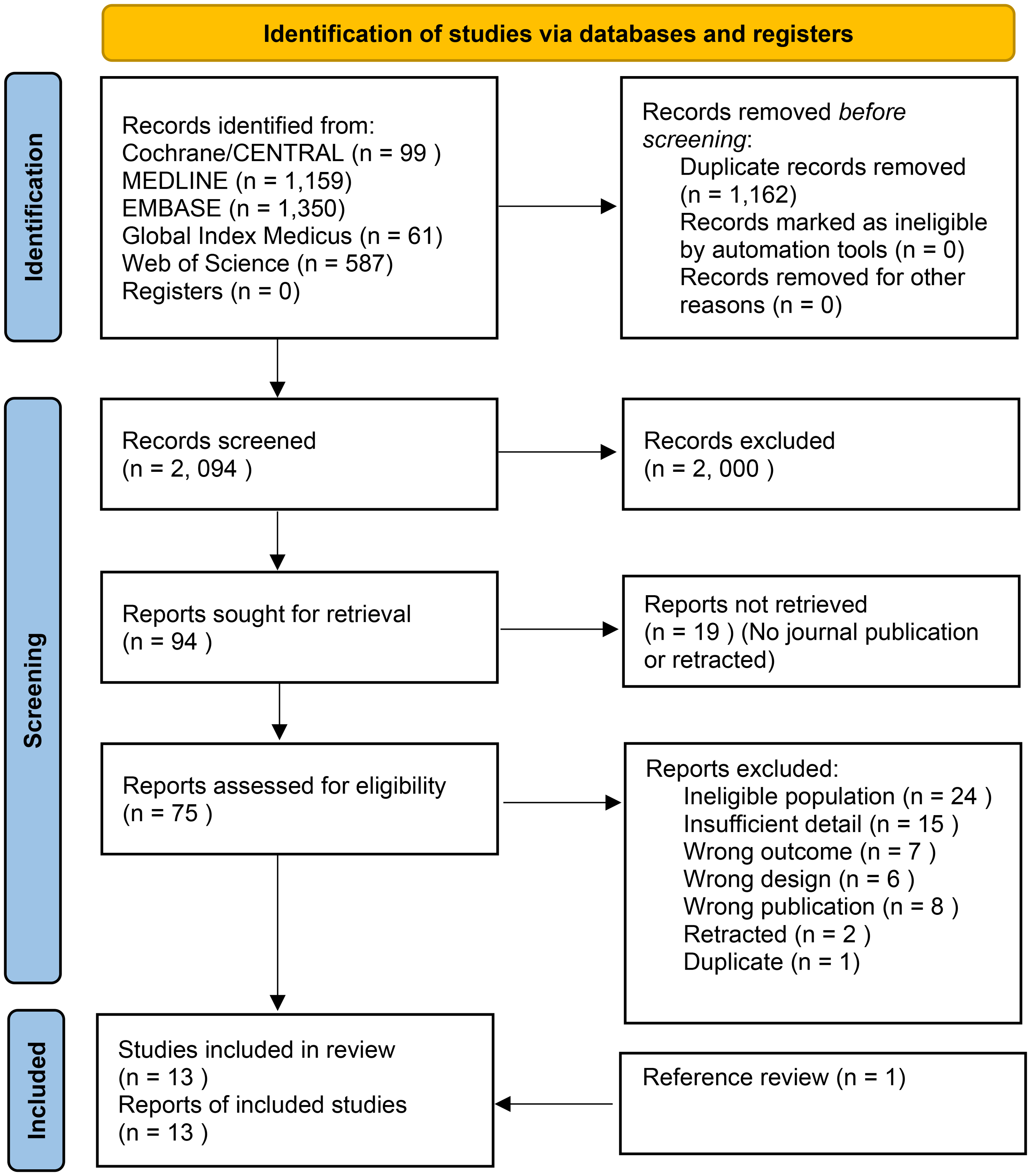
PRISMA flow diagram of the study selection process. PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-analysis.
These trials mainly aimed to compare different surgical interventions to fix open tibia fractures. However, one study was comparing different types of postoperative dressings. 35 The population sizes differed across the studies, ranging from 28 to 400 participants, representing 1463 adults in total. The mean number of participants in the studies was 113. The mean age of the participants was 34.7 years. One study 30 was not included in the mean age calculation as only ranges of the participants’ ages were available. Two studies could not be included to calculate the sex of participants: one had a mixed population (open or closed fractures) 25 and did not give the patients demographics per fracture type. The other study did not report the sex of the participants. 31 They were 428 participants in total in these two studies. In the remaining studies, 80.7% of the participants were male. Overall, the mean follow-up time for the included studies was 49.2 weeks. One study followed the patients up until completion of union. 34
The demographic findings for each study can be found in Table 1. The injuries reported were all diaphyseal or distal open tibia fractures.
Demographic characteristics of the participants in the included studies.
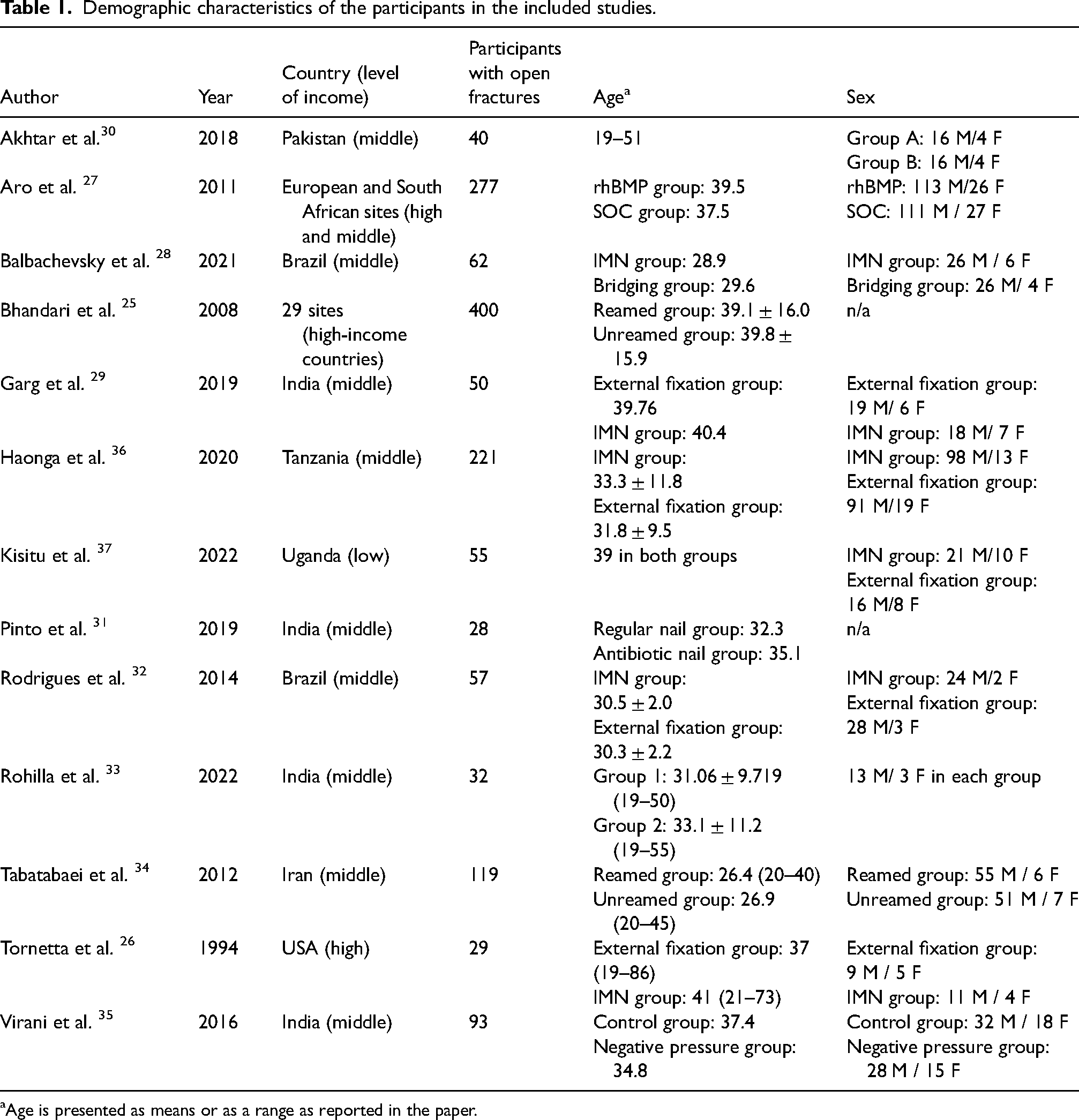
Age is presented as means or as a range as reported in the paper.
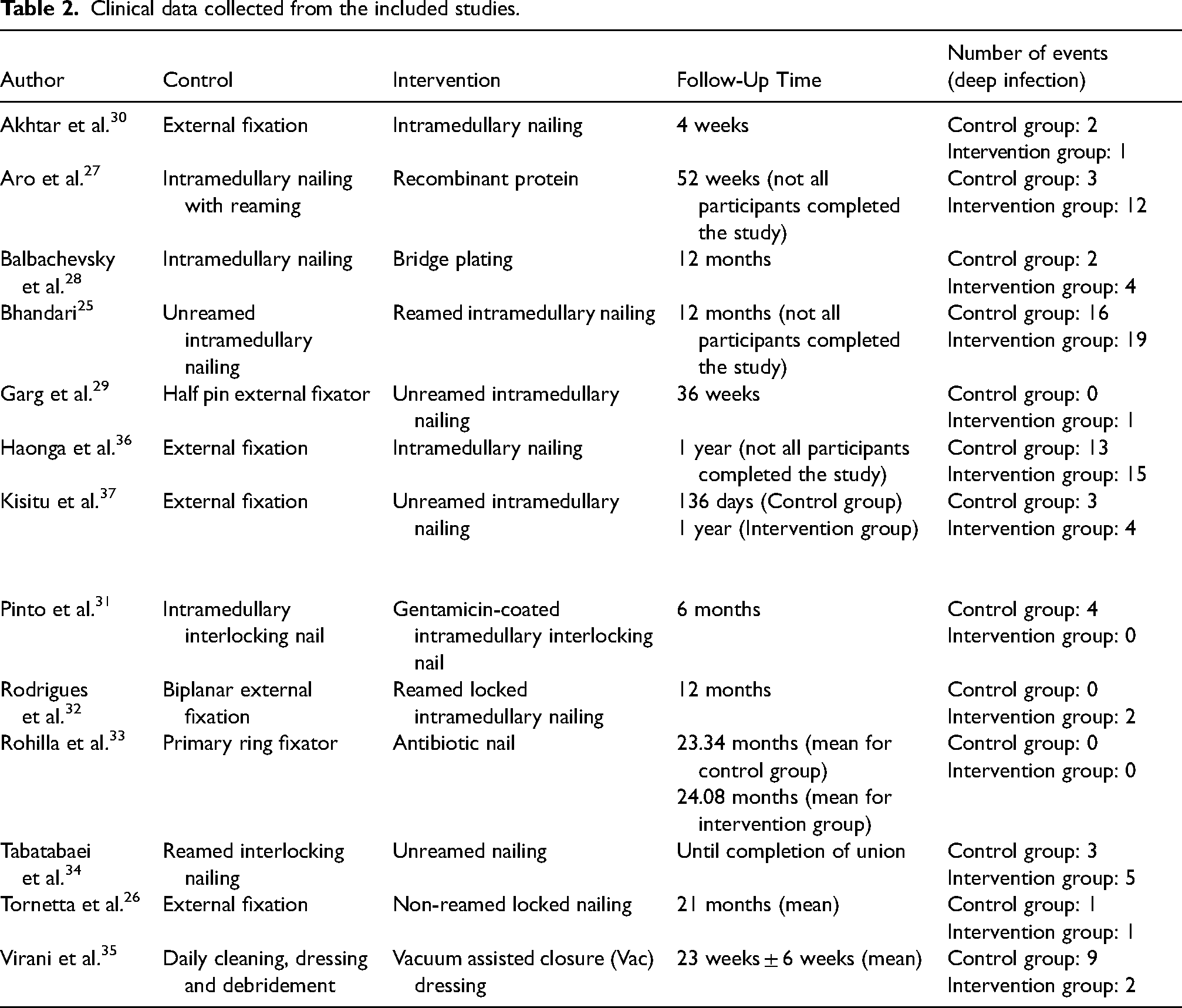
The data from all 13 studies were suitable to be pooled in order to conduct a meta-analysis. Data about the number of deep infections following open tibia fractures were collected for each trial and can be found in Table 2.
Clinical data collected from the included studies.
The first analysis aimed to give an estimate of the overall incidence rate of deep infections following open tibia fractures (Fig. 2) and included all 13 studies. The three others were subgroup analyses, one giving an estimate of the incidence of deep infection depending on the type of fixation used, another one giving an incidence depending on level of income of the countries. The last one excluded outliers from the analysis if they had a short follow-up period (<3 months). As a result, three studies were excluded from this analysis.
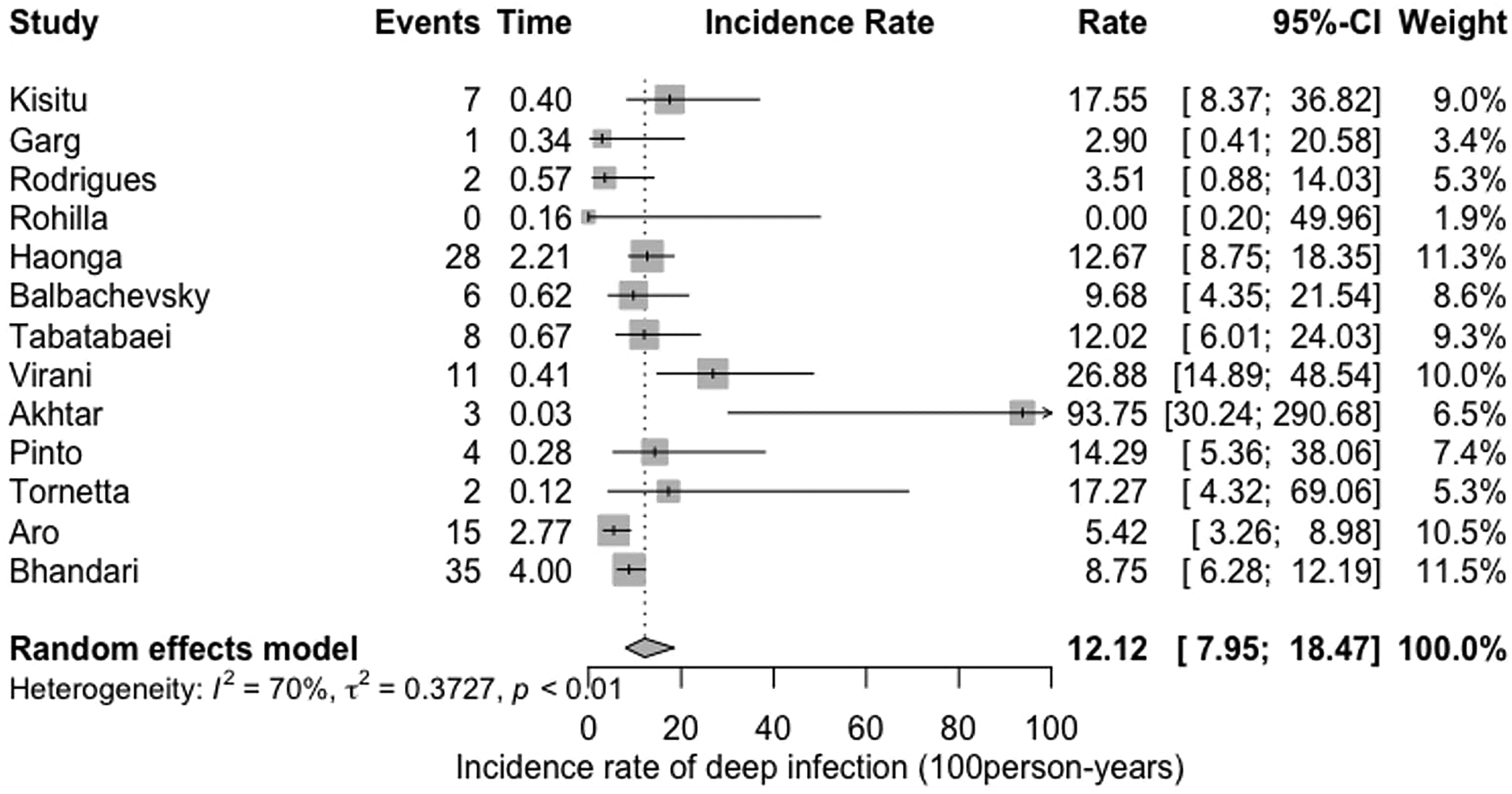
Overall incidence rate of deep infection after open tibia fracture.
Figure 2 shows the overall incidence rate of deep infection (given in 100 person-years) calculated based on the 13 trials: 12.12 (95% CI [6.28 to 18.47]). In this first random effect model meta-analysis, heterogeneity among the included studies was assessed using the I2 statistic. Its value of 70% indicates substantial heterogeneity.
Amongst the 13 studies, two were from high-income countries, one was from high- and middle-income countries, nine were conducted in middle-income countries and one was from a low-income country, 37 which was comparing intramedullary nailing to external fixation. This trial reported 4 (12.9%) deep infections in the intramedullary nailing group and 3 (12.5%) in the external fixation group. The fractures included were ranging from 42-A to 42-C according to the Müller AO classification of fractures. 17 In Figure 3, the incidence of infection was analysed and subdivided by country. The effect measure in this forest plot is the risk ratio with a random effect model. This model accounts for both within-study and between-study variability, providing a more conservative estimate of the overall effect.
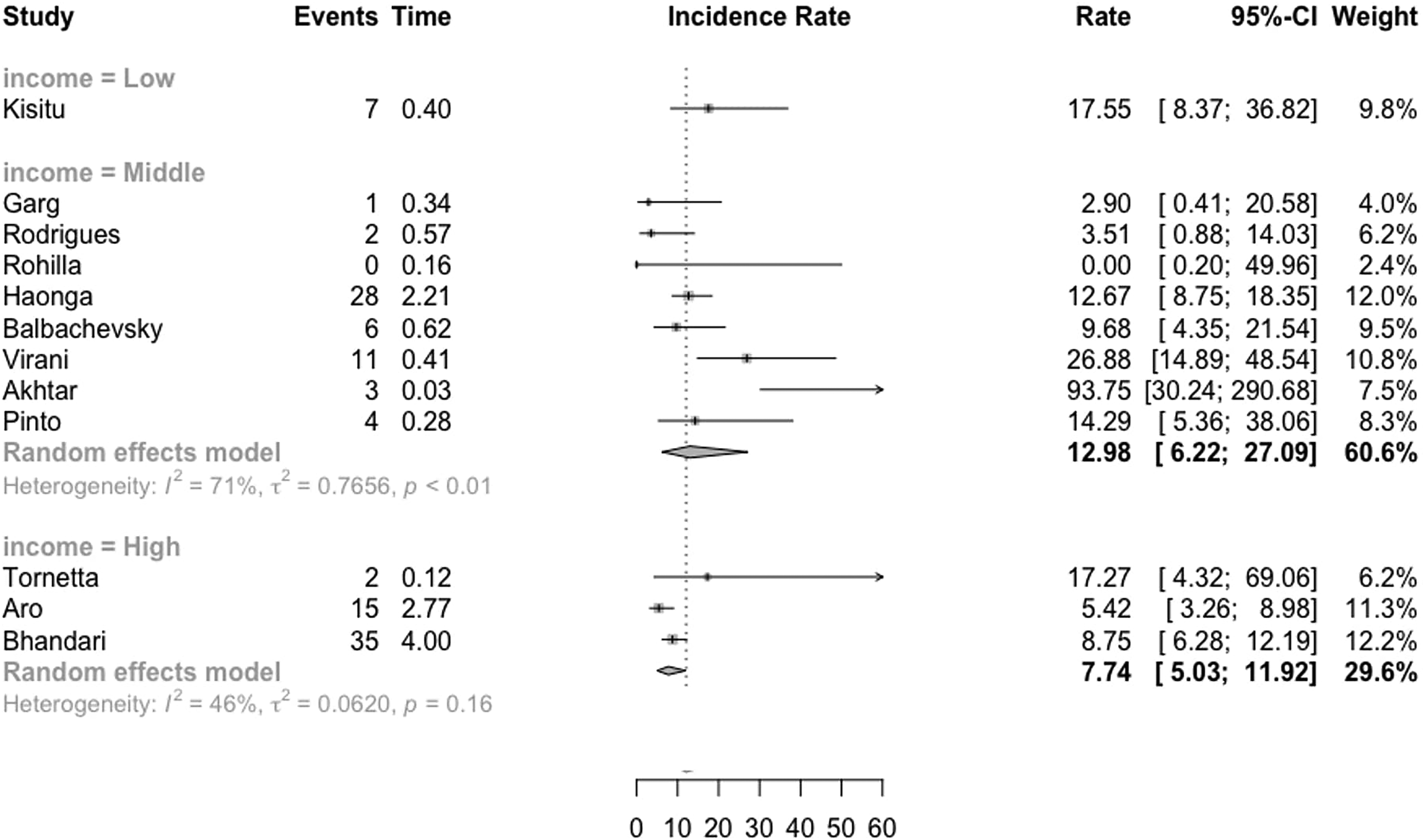
Overall incidence rate of deep infection after open tibia fracture subdivided by country income group.
The subgroup analysis by fixation type demonstrated an Incidence Rate Difference of 0.03 [−0.03; 0.09] (Fig. 4) of deep infections following open tibia fractures. The two types of fixation compared were intramedullary nails and external fixation. A sensitivity analysis, with outliers excluded, was also performed and demonstrated a pooled incidence rate of 13.91 (8.47; 22.84) (Fig. 5).
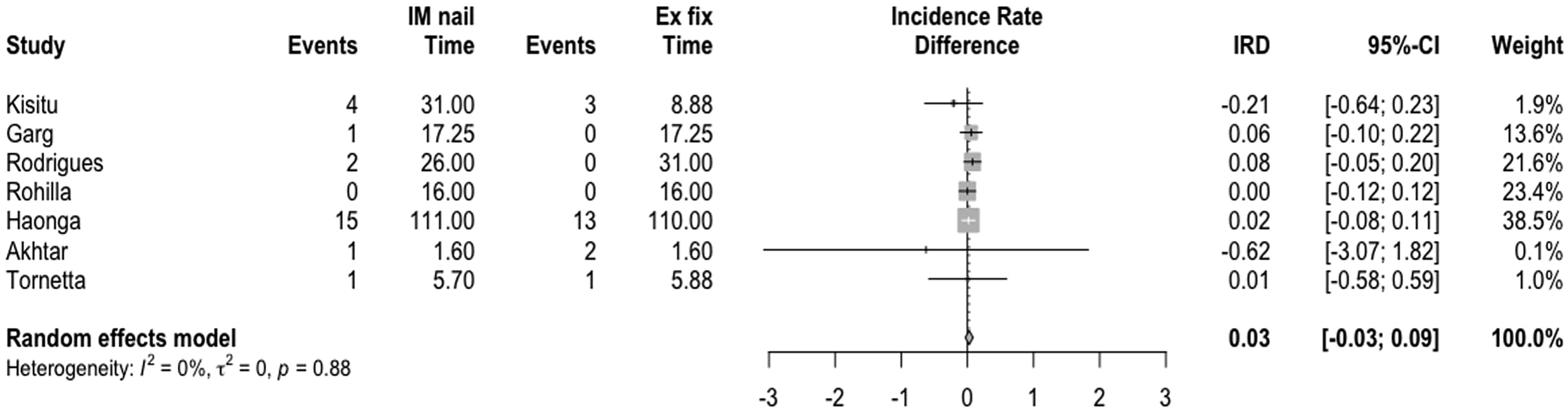
Subgroup analysis looking at the difference in the incidence rate of infection by fixation type.
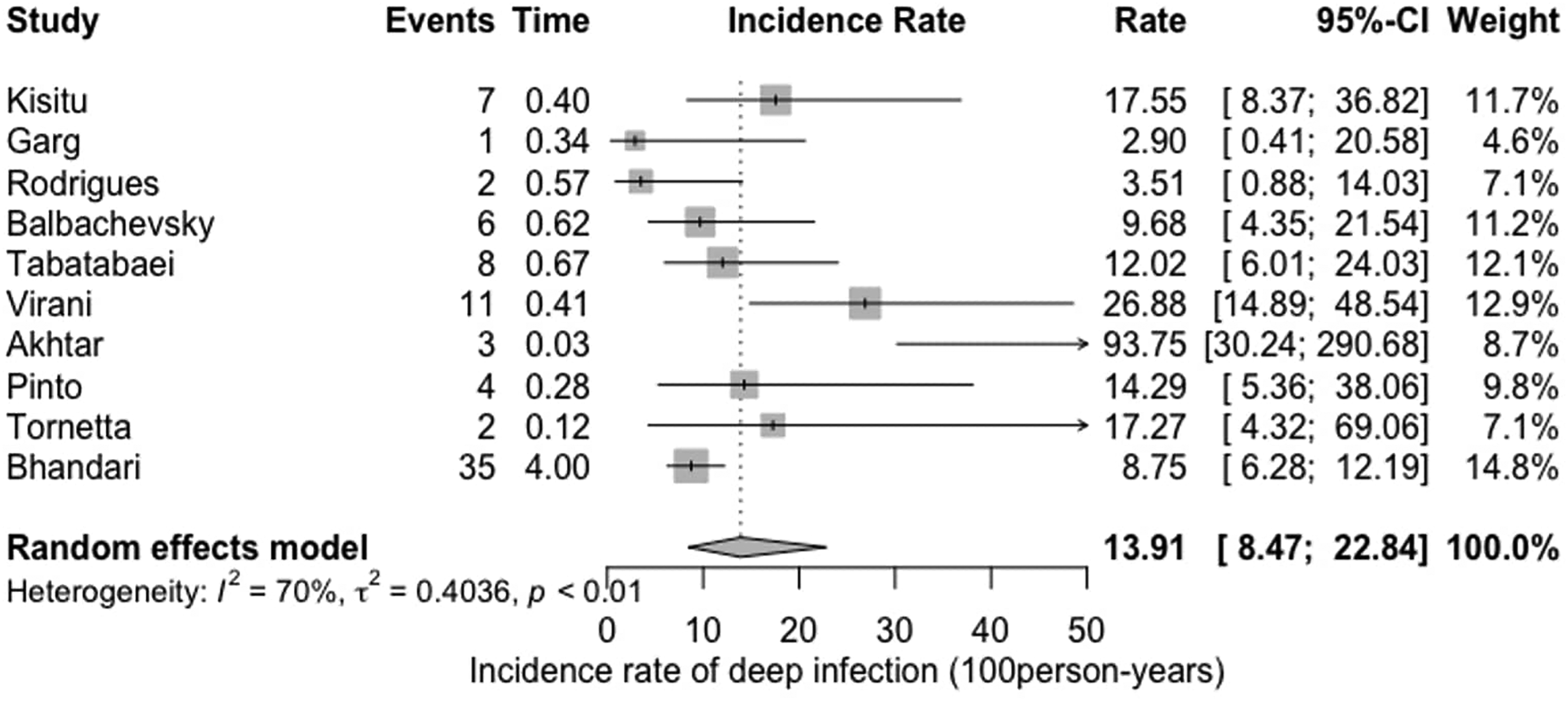
Sensitivity analysis with outliers excluded.
Only two studies reported limited microbiology data,29,35 the former reporting that Staphylococcus aureus was the causative organism of all infected cases. In the second trial, 35 out of the five patients who developed osteomyelitis, there were three methicillin-resistant Staphylococcus aureus (MRSA), one Pseudomonas aeruginosa and one mixed Escherichia coli and Acinetobacter. The only information about antibiotic resistance was the MRSA cases mentioned. 29 No other study included in this review provided data about antibiotic resistance.
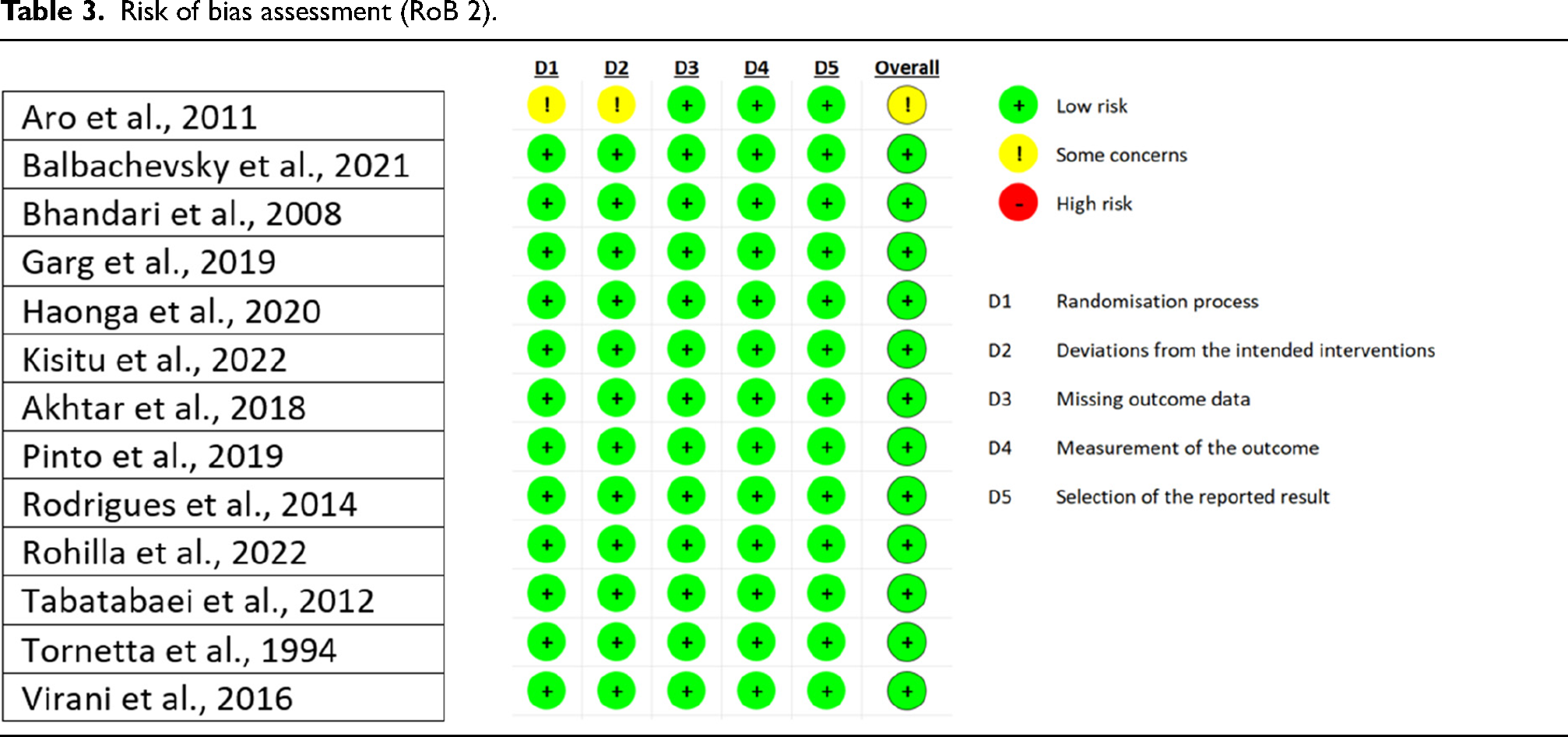
The results from the answers given in the RoB 2 Assessment Form Excel spreadsheet can be seen in Table 3.
Risk of bias assessment (RoB 2).
Discussion
The meta-analysis of 13 suitable randomised trials found an overall incidence of 12.2 infections per 100 person-years after open tibia fractures. This can be interpreted as that if 100 open tibia fractures are followed up for one year, 12 deep infections would be expected. This data can be used in the design of future interventional studies to inform power calculations. Our study shows no difference in the rates of infection between two interventions (external fixation and intramedullary nail), which further improves its generalisability when considering sample size. Further analysis by country income level provides estimates specific to different settings, but is limited to high- and low-income countries.
The highest incidence of infection amongst these trials was conducted in Uganda 37 which included a higher rate of patients with Gustilo Anderson III fractures, which are known to be associated with higher rates of infection.38,39 Large prospective observational studies in LMICs have shown a low rate of infection following operative management of people with fractures. 18 The high incidence of infection reported in our one selected article may be due to the increasing incidence of severe fractures, delays in operative management or availability of plastic surgeons.40,41 Future studies from LMICs need to explore patient, injury and treatment characteristics and delays in open tibia fracture treatment that are associated with higher infection.
Owing to studies investigating different open tibia fracture treatment such as type and timing of definitive fixation and type and timing of soft tissue coverage, there was substantial uncertainty in the incidence of infection according to treatment. A systematic review of randomised control trials comparing timing of different long bone open fracture interventions also found significant uncertainty in 2020. 42 Despite multiple further trials included in this meta-analysis, uncertainty in terms of incidence of infection remained possibly due to differences in Gustilo grade of injuries, patient co-morbidity, associated injuries and treatment settings. Future studies and reviews that investigate infection following open tibia fractures will need to stratify across Gustilo grading and treatment to reduce uncertainty in infection.
Furthermore, very little information was provided about the microbiology of the infections reported and the methods to assess this. Microbiology services are very limited in LMICs with a survey indicating only one microbiologist per million population being available in Sub-Saharan Africa 43 This meta-analysis was not able to draw any conclusions on differences in pathogens across different settings and injuries. Very little data exist (and are predominantly from HICs) to guide open fracture antibiotics but would suggest a 24 h course of a first-generation cephalosporin to reduce the risk of infection in open fractures as reasonable. 44 The culture, microbiology and sensitivity of deep samples following infected open tibia fractures is key to guide antibiotics, especially in settings where the micrology might be different. Effective antibiotics are important not only to prevent infection, but treat established infection using antibiotic coated nails, beads or masquelet technique 45 Future international surveys could investigate reported pathogens in different countries, although this might be limited by availability and reliability of microbiology testing in LICs.
Our systematic review only included RCTs. Since the follow-up time of these is pre-set in their protocols, this allows a thorough reporting of results, helping to reduce the risk of bias that could be seen in a cohort study where participants lost to follow-up can influence the final results.
We aimed to discuss results of trials without discriminating countries by level of income. However, it was clear that there is a lack of research in LICs, with only one trial from such. 46 RCTs may not routinely report antibiotic resistance. Microbiology information may therefore be better gained from reviews of cohort studies.
Another limitation to our study stems from the definition of infection. The same definitions may not be used, causing disparities in reporting and results between studies. Consideration of adopting consensus-driven definition, which are specific to orthopaedics, such as fracture-related infection, may reduce heterogeneity in definition and therefore in results of studies. 47 The definition of fracture-related infection has been shown to be relevant to LMIC settings, but there might be challenges in terms of guiding the treatment of infection owing to different availability of resources. 48 Our results suggesting a link between the severity of the fracture and the odds to develop an infection correlate with the previous literature. 49 As our population was mainly composed of younger males, however, results may not be generalisable to older adults. Our study was however unique in attempting to calculate an overall incidence.
Footnotes
Acknowledgements
Not applicable.
Authors’ contributions
DC and AR performed the initial searches and extraction of data; AS and CK designed the work; FD, CK and AS performed the statistical analysis and interpretation of data. All authors contributed to the initial drafting and subsequent revision of the article.
Availability of data and materials
Not applicable.
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.