
Abstract
Acute toxic leukoencephalopathy and serotonin syndrome are rare neurological complications associated with various drugs and toxins, some of which overlap. However, the co-occurrence of these conditions is poorly documented. We present the case of a 14-year-old boy who suddenly developed altered consciousness and autonomic dysfunction after consuming excessive quantities of cough remedies containing dextromethorphan, chlorphenamine, dichlorobenzyl alcohol, and amylmetacreson. Magnetic resonance imaging of the brain revealed distinct white matter lesions. With supportive care, the patient rapidly improved, and the magnetic resonance imaging abnormalities disappeared. The swift resolution, typical magnetic resonance imaging findings, and a history of exposure to drugs affecting the central nervous system's serotonergic system suggested concurrent acute toxic leukoencephalopathy and serotonin syndrome. The components of cough medications can be hazardous in overdose due to their potential to enhance serotonin toxicity and cause direct or indirect central nervous system white matter damage. Early recognition and appropriate treatment are essential for recovery.
Keywords
Case report
A 14-year-old boy was brought as an emergency with a one-day history of fever, frequent vomiting, loose stools, altered behaviour, and generalised seizures. He had an upper respiratory tract infection for three days (prior to the COVID-19 pandemic), following which he consumed OTC cough syrup arbitrarily and excessively.
Clinical examination revealed pyrexia (38.2 °C), excessive sweating, tachypnoea, and tachycardia. He had impaired consciousness, intermittent agitation, mydriasis, spontaneous clonus, brisk deep tendon reflexes, and an extensor plantar response.
He was transferred to the intensive care unit and required mechanical ventilation.
Laboratory parameters including serum electrolytes, kidney and liver functions, serum ammonia, and lactate were normal. A magnetic resonance imaging (MRI) brain showed patchy ill-marginated areas of T2/FLAIR hyperintensity in the lobar white matter (Fig. 1). Evaluation for systemic and cerebral infection, including cerebrospinal fluid (CSF) study, were normal. CSF pan-viral PCR (herpes simplex virus 1, 2 and human herpes virus 6, Japanese encephalitis, cytomegalovirus, enterovirus, and varicella zoster) were negative. Serum and CSF autoimmune antibodies (anti-NMDA, anti-LGI-1, anti-AMPA 1 & 2, anti-CASPR, and anti-GABA-B receptor antibodies) were likewise negative. Toxicology screening of blood and urine tested negative for opiates, benzodiazepines, and amphetamines. An electroencephalogram showed mild diffuse slowing without epileptic activity.
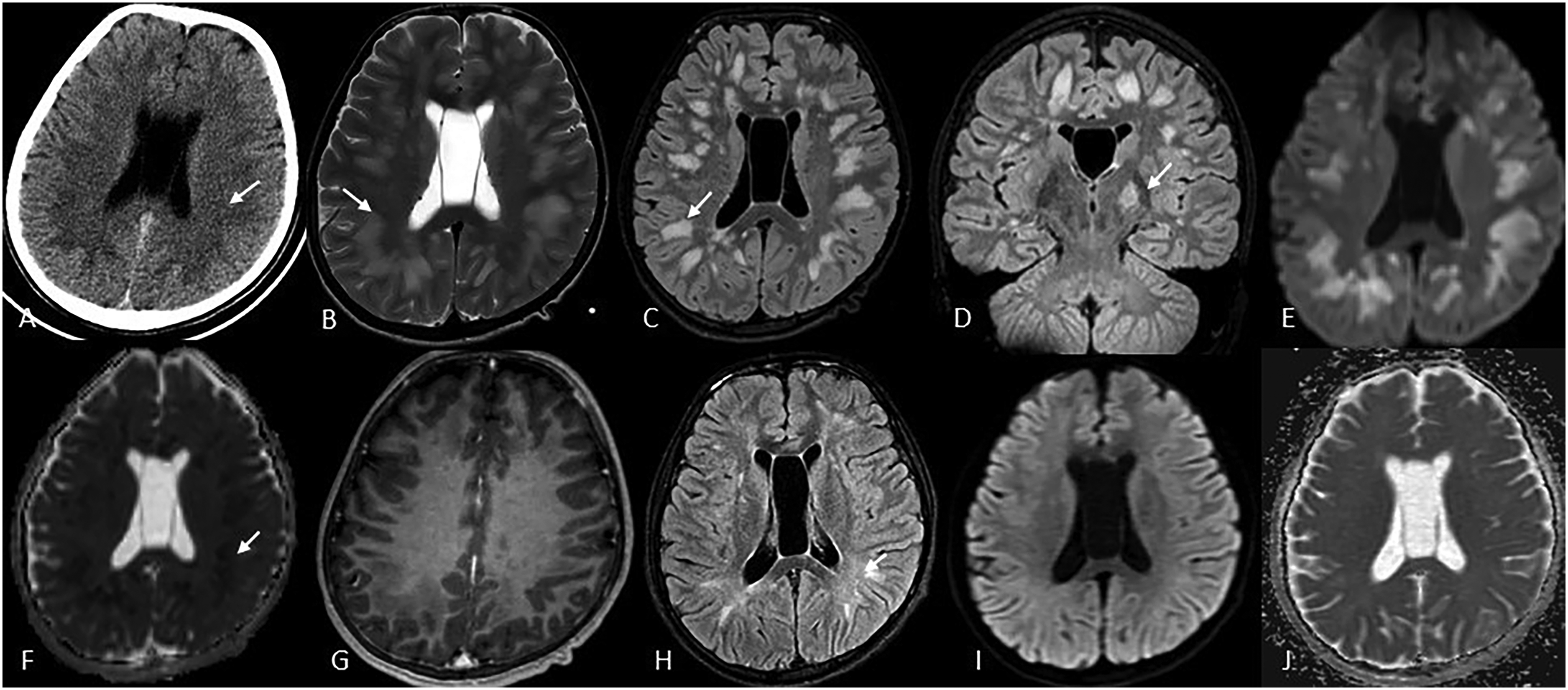
Brain CT reveals symmetrical confluent hypodensities involving deep WM of bilateral fronto-parietal lobes (A). MR imaging (day 2) demonstrates T2/FLAIR hyperintensities involving subcortical and deep WM of bilateral cerebral hemispheres (B, C) with additional involvement of left PLIC (D). Corresponding lesions show restricted diffusion on DWI (E) and the corresponding ADC map (E) without evidence of postcontrast enhancement (G). A follow-up scan (day 51) later demonstrates significant resolution of the T2-FLAIR hyperintensity (H) with normalisation on diffusion-weighted images (l, J).
Treatment with intravenous methylprednisolone for five days was commenced. Levetiracetam was used for seizure control. Clinical improvement by the fifth day of admission was seen and discharge possible after two weeks with no neurological deficit.
At one month follow-up, he was asymptomatic and a repeat MRI showed improvement. He remained asymptomatic at the most recent follow-up two years after the event.
Discussion
Acute toxic leuco-encephalopathy (ATLE) is a rare clinicoradiologic syndrome that preferentially involves brain white matter of various causes.1,2 Serotonin syndrome (SS) is characterised clinically by a triad of autonomic instability, neuromuscular hyperactivity, and altered mental state. Previously, components of cough medications such as codeine, dextromethorphan, and chlorphenamine have been implicated separately in SS and ATLE. Though simultaneous SS and ATLE have been reported with recreational drug abuse, this has not been associated with cough medication.
Our patient fulfilled the diagnostic criteria for SS. 3 The pharmacist who had dispensed his medication confirmed that he was given cough syrup containing a combination of dextromethorphan and chlorphenamine, and cough lozenges containing 2,4-dichlorobenzyl alcohol and Amylmetacreson. Considering the close temporal relationship, acute onset, and quick resolution of symptoms, the possibility of these drugs triggering a combination of SS and ATLE is most likely. Based on the Naranjo adverse drug reaction scale, the level of causal association in our patient could be categorised as ‘probable’. 4 Mimics of ATLE such as extra-pontine myelinolysis, hyperammonemia encephalopathy, as well as sepsis-related ADEM and mitochondrial disorders (normal serum and CSF lactate) were ruled out in our case.2,5 We considered a variant of posterior reversible encephalopathy syndrome (PRES), in view of the reversible nature of the MRI changes. While PRES has been described in the context of SS, the diffusion restriction and the lobar (rather than a subcortical) distribution made the diagnosis less likely.
Whether any individual component or the combination of dextromethorphan, chlorphenamine, 2,4-dichlorobenzyl alcohol, and amylmetacreson is responsible in our patient is unclear. However, whilst the mechanism is unclear, a potential connection between systemic serotonin imbalance and brain serotonin neurotoxicity may involve leucotoxic serotonergic damage, oxidative stress, or cerebrovascular tone disruption. 6
Toxic leuco-encephalopathy can present with a spectrum of neurological findings. The severity is best correlated with the extent of white matter involvement on MRI. 2 Early recognition is crucial in preventing complications.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.